Embed Size (px)
Citation preview

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
1
GRAFT VERSUS HOST DISEASE
Presenter – Dr. Deepak R. ChinagiGuide – Dr. L. S. Patil
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
2
• Greetings• At the end of this topic, we will understand:– Define GVHD and its mechanism,– How is it different from graft rejection,– Identifying GVHD and differentials.– How to treat and how to prevent.– Future perspectives.

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
3
Introduction• Graft versus host disease (GVHD) is an immune mediated disease
due to complex interaction between donor (lymphoid tissue) and recipient’s immunity occurring after transplantation.
• Two types– Acute (less than 100 days)– Chronic (more than 100 days)
• It occurs when immunologically competent T cells or their precursors are transplanted into recipients who are immunologically compromised.
• Incidence - 1-2 %• Mortality - up to 75%
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
4
Procedures with risk of GVH disease
• Allogenic HSC Transplantation (hematopoietic stem cell transplantation)– Bone marrow transplantation.– Umbilical cord blood.– PBSC (peripheral blood stem cell) transplantation.
• Solid organ transplantation (esp. organs containing rich lymphoid tissue)– Kidney transplantation.(rare)– Liver transplantation. ()– Heart transplantation
• Transfusion of unirradiated blood products.• It can also be caused by whole blood transfusion in patients with
severe combined immunodeficiency.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
5
Pathophysiology of GVHD
• Immune-competent T cells transplanted into immune-compromised host.
• Host cannot reject the graft due to decreased immunity. But graft T cells perceive the recipients tissue as foreign and react against it.
• This leads to activation of CD4 and CD8 T cells ultimately causing inflammation and killing of host cells.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
6
Pathophysiology of GVHD (Future Scope)
• GVHD can be minimized but cannot be eliminated – HLA typing is useful– Donor T cell suppression before transplant – mixed
blessing– Multi-functional T cells not only mediate GVHD but are
also required for efficient engraftment of transplanted HSC s and elimination of leukemic cells
• The disease is less understood due to its complex mechanism. It is known to occur in autologus form also. Usually after PBSC transplantation.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
7
• Effector cells(Donor T cells)
• Proinflammatory Cytokines(IL1, IL2, TNF, IFN)
• Target Host tissues (Skin, Liver, Intestines)
• Allogenic recognition &• Autologous dysrecognition

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
8
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
9
Clinical Features
• Types of manifestations– Hyperacute– Acute– Chronic
• Severity of GVHD depends on the degree of HLA disparity and other factors like…– Cryopreservation of BMT and Cord blood are known for lower
incidence of GVHD.– Allogenic PBSC has high incidence of chronic GVHD– Post-transplanational prophylaxis (immuno-supression)
decrease the incidence of GVHD

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
10
Hyperacute Form - GVHD
• Usually develops after 7-14 days after transplantation
• Symptoms are …. Fever, generalized erythroderma, desquamation may occur.
• Later follows a similar course as acute form.

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
11
Acute GVHD
• Triad of dermatitis, hepatitis and enteritis.• Skin Manifestations- ( onset 5-50 d, M=19 d)– Pruritic and Painful rash– Red to Violet lesions, first appear on palms and soles, cheeks,
neck, ear, trunk.– In severe cases, bullae and vesicles may form.
• In cases of chronic GVHD, – Lichenoid lesions or sclerodermatous thickening can be seen.– Contractures can occur,– Joints get restricted mobility.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
12
• Hepatic Manifestations-– Jaundice– Pruritis– Skin excoriations due to scratching– Rare manifestations are cirrhosis, portal
hypertension, hepatic coma and death.– Raised serum bilirubin, ALT, AST, ALP

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
13
• Gastrointestinal Manifestations-– Upper GI Symptoms- • Anorexia , • Dyspepsia
– Lower GI Symptoms-• Diarrohea, Intestinal Bleeding, Cramping Abdominal
Pain and Ileus.• Diarrohea is usually described as voluminous, secretory,
green, mucoid, watery, associated with exfoliated cells
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
14
• Pulmonary Manifestations-– Pneumonia – infectious and noninfectious.– Pleural Effusions – usually sterile.
• Other Manifestations- – Hemorraghic cystitis– Thrombocytopenia– Anemia– Hemolytic Uremic syn.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
15
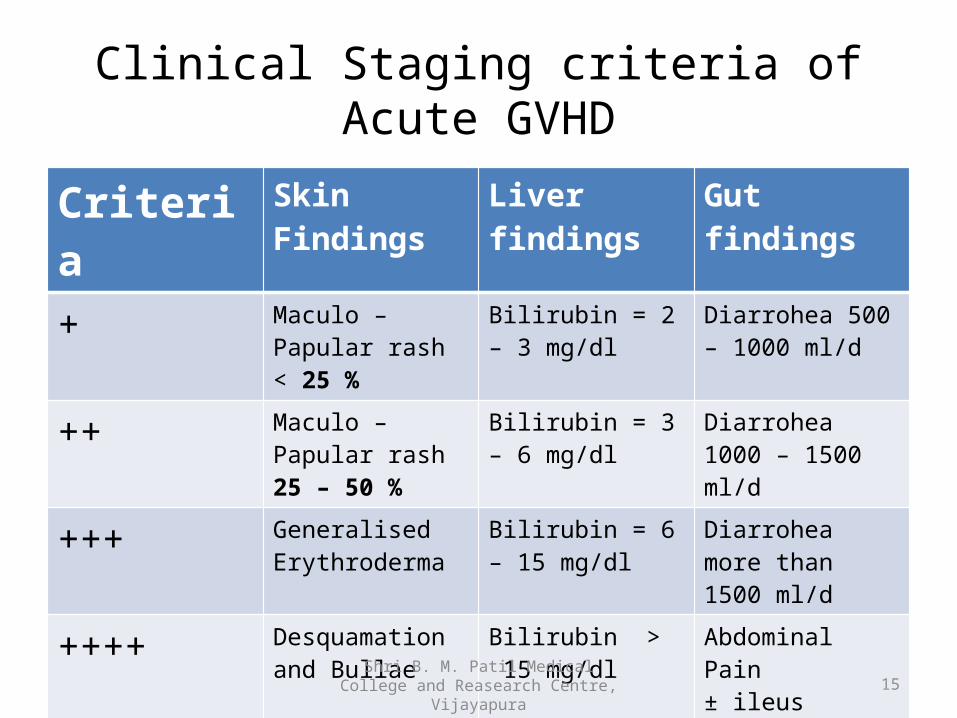
Clinical Staging criteria of Acute GVHD
Criteria Skin Findings Liver findings Gut findings
+ Maculo –Papular rash < 25 %
Bilirubin = 2 – 3 mg/dl
Diarrohea 500 – 1000 ml/d
++ Maculo –Papular rash 25 – 50 %
Bilirubin = 3 – 6 mg/dl
Diarrohea 1000 – 1500 ml/d
+++ Generalised Erythroderma
Bilirubin = 6 – 15 mg/dl
Diarrohea more than 1500 ml/d
++++ Desquamation and Bullae
Bilirubin > 15 mg/dl
Abdominal Pain ± ileus

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
16
Clinical Staging of Acute GVHDGrade Skin Liver Gut Functional
impairment0 (None) 0 0 0 0
1 (Mild) +/++ 0 0 0
2 (Moderate) +/+++ + + +
3 (Severe) ++/+++ ++/+++ ++/+++ ++
4 (Life-Threatening)
++/++++ ++/++++ ++/++++ +++

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
17
Chronic GVHD• May occur as extension of already existing disease or de
novo. Usually it emerges after an interval after acute GVHD.• Skin Manifestations-
– Lichenoid lesions, sclerodermatous thickening, contractures of skin and restricted joint mobility.
• Ocular Manifestations-– Burning sensation of eyes, irritation, photophobia, pain, dryness
of eyes.– Hemorrhagic conjunctivitis, pseudo membrane formation,
lagophthalmos, keratoconjunctivitis sicca, punctate keratopathy, corneal erosions.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
18
• Oral Manifestations-– Dryness of mouth, atrophy of mucosa, dysphagia,
odynophagia, weight loss• Pulmonary Manifestations-– Wheeze, dyspnea, chronic cough.– Bronchiolitis obliterans.
• Neuromuscular manifestations-– Weakness , neuropathic pain and muscle cramps.

Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
19
Differentials
• Chronic GVHD has similar manifestations as that of systemic sclerosis, SLE, lichen planus, sjogrens syn., eosinophilic fasciitis, rheumatoid arthritis, primary biliary cirrhosis.
• Erythema Multiforme(SJS)• Viral Hepatitis• Malabsorption• Mixed Connective Tissue Disease
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
20
Investigations• CBC• LFT• Serum Electrolytes• USG Abdomen- liver and gall bladder• Barium swallow• Schirmer test – ocular manifestations• PFT , ABG• Biomarkers
– IL2 receptor α– TNF receptor 1– IL8– Hepatocyte growth factor
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
21
Investigations
• Skin Punch Biopsy• UGI endoscopy• Sigmoidoscopy/Colonoscopy• Liver Biopsy
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
22
Treatment
• Primary prophylaxis– CSP A /Tacrolimus for 6 mths and short course
MTX and added with prednisolone.– ATG decerases severity but doesn’t alter survival– ECP – 8methoxy-psoralen . After UV light , cell
undergoes apoptosis.
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
23
Treatment• Primary therapy
– Topical steroids / continue immunosupressive prophylaxis.– ATG , CSP alone , Mycophenolate Mofetil
• Secondary therapy steroid refractory cases– ATG / multiple pulses of methylprednisolone– Mycophenolate mofetil 2g/d– Muromomab– Anti IL2 receptor– PUVA– Tacrolimus, Visilizumab, Daclizumab, Infliximab,– TNF α inhibitor (etanercept)
Shri B. M. Patil Medical College and Reasearch Centre, Vijayapura
24
Treatment
• Chronic GVHD– Prednisolone 1mg/kg ± Azathioprine.– TNF modulator- Thalidomide
– Steroid refractory cases –• Azathioprine , CSP / prednisolone, thalidomide• Clofazimine• PUVA / ECP