Embed Size (px)
Citation preview

Hand TraumaHand Trauma
Prepared by:Dr. Ahmed Mirza Shammasi
2031040009Surgical Intern - KFU – Saudi Arabia
1

OutlinesOutlinesIntroductionMechanisms of InjuryApproach to hand trauma patientStructural Injuries:◦Cutaneous Injuries◦Tendon Injuries◦Nerve Injuries◦Bone Injuries
Amputation and Replantation
AnatomyPresentation
andManagement
2

IntroductionIntroduction The hand is a very vital part of the human body
4 requirements for a functioning hand:◦ Supple (moving with ease)◦ Sensate
Account for 5-10 % of hospital ER visits.
Great potential for serious handicap
Good understanding of hand anatomy and function, good physical examination skills, and knowledge of indications for treatment.
Proper Initial diagnosis and timely appropriate treatment would reduce morbidity.
◦ Pain free◦ Coordinated
3

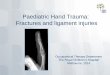
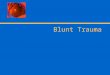
Mechanisms of InjuryMechanisms of InjuryBlunt trauma◦Most common type◦Crush injuries, contusions, abrasions
Laceration or punctureAvulsion with or without soft tissue
deficit ◦Form of amputation where digit is pulled off
rather than cut off.Ring avulsion
4

Approach to Hand TraumaApproach to Hand Trauma1. History: General
◦ Age◦ Hand dominance◦ Occupation/hobbies◦ History of previous hand problems
When and where did this injury take place? ◦ Determine the likelihood of severe injury and probability of
contamination with foreign matter. How was the trauma sustained?
◦ This gives clues to the most likely injury. What was the posture of the hand at the time of the injury?
◦ Structures in the hand slide with movement. The tissue under a bruise or laceration may not be the same tissue that was present when the injury was sustained
Past history of treatment or surgery in the hand
5

Approach to Hand TraumaApproach to Hand Trauma2. Physical examination
◦ Entire upper limb should be exposed and carefully inspected (Muscle wasting, colour change, Asymmetry, fixed abnormal posture etc.)
◦ Extrinsic flexor and extensor muscles and their tendons’ injuries.
◦ Intrinsic muscles (Thenar, lumbricals, interossei, and hypothenar muscles).
◦ Joints’ pain and stability.
◦ Sensory examination.
◦ Circulation for colour change, Allen test.
6

Approach to Hand TraumaApproach to Hand Trauma3. Imaging Studies
Radiography◦ Plain-films of the hand or wrist should be obtained when a
patient presents with a soft tissue injury suggestive of fracture or an occult foreign body.
US◦ Has a growing role in locating foreign bodies and in evaluating
soft tissues◦ Can detect ruptured tendons and assess dynamic function of
tendons non-invasively. MRI
◦ Highly sensitive in detecting ruptured tendons. ◦ However, it does not have a role in emergent management of
hand wounds.
7

8

9

CUTANEOUS INJURIESCUTANEOUS INJURIES
•Anatomy•Presentation•Management
10

AnatomyAnatomy Dorsum surface
◦ Thin and pliable. ◦ Attached to the hand's skeleton only by loose areolar tissue,
where lymphatics and veins course.◦ Edema of the hand is manifested predominantly at the
dorsum◦ Loose attachment makes it more vulnerable to skin avulsion
injuries.
Palmar surface◦ Thick and glabrous and not as pliable as the dorsal skin◦ Strongly attached to the underlying fascia by numerous
vertical fibers◦ Most firmly anchored to the deep structures at the palmar
creases◦ Contains a high concentration of sensory nerve endings
essential to the hand's normal function
11

PresentationPresentationCutaneous injuries are very common
injury.Two Types◦Open: Incised, laceration, punctured (bites),
penetration, abrasion.◦Closed: Contusions, Hematomas
Vary in depth from superficial to very deep involving underlying structures.
Explore for underlying structural Injuries.
12

13

ManagementManagementSkin Laceration:◦Small: Rinse and cover.◦Large:
Infiltrate with Lidocaine Irrigate wound profusely with betadine or sterile
water Drape and explore (underlying injuries and
foreign bodies) Close the skin wound with simple sutures. Wounds older than 6-8 hours should not be
closed primarily because of an increased likelihood of infections.
Irrigate, explore then apply sterile dressing. Re-check after 4 days for skin infection. Delayed primary closure at 4 days.
Update Tetanus vaccination.14

ManagementManagementBites:◦ Should not be closed primarily but should be given
serial wound checks with delayed closure at 4 days if needed
◦ Antibiotic prophylaxis is indicated in human (including fight-bites) and cat bites and may be of benefit in dog bites as well.
Contusions:◦ Cold packs with pressure for 30 to 60 min. several
times daily for 2 days.◦ Two days after the injury, use warm compresses for 20
minutes at a time.◦ Rest the bruised area and raise it above the level of
the heart◦ Do not bandage a bruise.
15

ManagementManagementAbrasions:◦Superficial:
Rinse and cover. Prophylactic antibiotic ointment
◦Deep: Rinse with antiseptic or warm normal saline.
Scrub gently with gauze if necessary. Dress with semi-permeable dressing
(Tegaderm, Bioclusive). Changed every few days.
Keep wound moist. Enhance healing process.
16

TENDON INJURIESTENDON INJURIES
•Anatomy•Presentation•Management
17

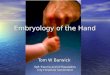
AnatomyAnatomyMuscles of the hand are divided into
two main groups:◦Extrinsic group
Extrinsic extensors Extrinsic flexors
◦Intrinsic group: Thenar complex lumbricals Interosseous Hypothenar complex
Extensor FunctionInterphalangeal
joints
18

19

20

21

22

23

PresentationPresentation Extensor injuryExtensor injury
Extensors Injury:◦Divided into
Zones according to anatomical location of injury
24

PresentationPresentation Extensor injuryExtensor injury
25

26

ManagementManagementZone Presentation Management
I Mallet’s Deformity
•Closed: splinting 6-8 weeks•Open: suture repair for fixation. Soft tissue reconstruction
IIIBoutonniere’s
Deformity
•Closed: splinting MCP and PIP in hyperextension for 6 weeks•Open: suture repair (figure of 8 suture)
VFixed flexion of
MCP
•Closed: splinting ,45 extension at wrist and 20 flexion at MCP•Open: suture repair.
VIIFixed flexion of
MCP•Suture repair followed by post-op splinting
27

28

PresentationPresentation Flexor injuryFlexor injury
Flexors Injury:◦Divided into
Zones according to anatomical location of injury
29

30

31

PresentationPresentation Flexor injuryFlexor injury
Zone Presentation Management
I
Loss of active flexion at DIP joint
Hyperextension of DIP joint
•Primary or Secondary tendon repair•Careful suturing prevent post-op adhesions.
IILoss of active flexion at MCP
joint
•Skin closure then secondary repair by tendon grafting•Primary repair performed by skilled hand surgeon to minimize post-op adhesions.
III, IVThumb
Same
•Primary or secondary tendon repair•Examine carefully for thenar muscle injury and recurrent branches of median nerve.
32

PresentationPresentation Flexor injuryFlexor injury
Zone Presentation Management
VPalm
UncommonLie deep and
protected by palmar fascia
Same presentation
•Superior to Tendon division: repair is unnecessary.•Both muscles’ tendon division: primary repair
VI, VIIWrist
Multiple flexor tendon injury
Impaired active flexion of multiple digits
•Primary tendon suturing further proximal in the forearm to prevent post-op cross-adherence.•Injuries to muscles in forearm require primary repair•Post-op splinting of wrist in flexion position and elevation for 4 weeks.
33

34

NERVE INJURIESNERVE INJURIES
•Anatomy•Presentation•Management
35

AnatomyAnatomy
36

AnatomyAnatomy
37

PresentationPresentationMechanisms of injury:◦Traction: force is longitudinal to nerve axon◦Compression: force is cross-sectional to nerve
axon.◦Laceration: sharp object injury.
Blunt trauma delivers forces that stretch and compress nerves. Nerve my undergo total disruption or avulsion. Less favorable outcome.
Sharp laceration can cause complete transection of nerve but it is associated with best prognosis
38

PresentationPresentationEffect of injury: “Seddon’s Classification”
◦Neuropraxia: Disruption of Schwann cell sheath but no loss of
continuity.
◦Axonotmesis: Injury to both Schwann sheath and axon. Distal part undergoes Wallerian degeneration. Stimulation of nerve 72 hours after injury does not
elicit response. Regeneration occurs with the average rate of 1-2
mm/day. Regeneration is supported and guided by the
surrounding endoneurium.
39

PresentationPresentation
◦Neorutmesis: Injury to all anatomical components, myelin
sheath, axons and the surrounding connective tissue.
This total nerve disruption makes regeneration impossible.
Surgical intervention is necessary.
◦Examine carefully to document any sensory or motor injury and for follow up.
40

PresentationPresentation
41

PresentationPresentation
42

ManagementManagementNeurolysis:◦Removal of any scar or tethering attachments to
surroundings that obstruct nerve ability to glide.Neurorrhaphy:◦End-to-end repair.◦Resection of the proximal and distal nerve stumps
and then approximation.Autologus Nerve grafting:◦Gold standard for clinical treatment of large lesion
gaps.◦Nerve segments taken from another parts of the
body.◦Provide endoneural tubes to guide regeneration.◦ Two types: Allograft, Xenograft.
43

44

BONE INJURIESBONE INJURIES
•Anatomy•Presentation•Management
45

46

PresentationPresentation Key to diagnosis is careful History and Physical
Examination, supported by radiographic studies. History:
◦ Handedness◦ Occupation◦ Mechanism of injury◦ Time since injury “golden period”◦ Place of injury
Physical Examination:◦ Inspection for open fractures, swelling◦ Deformities (angulation, rotation, shortening)◦ Alignment.◦ Range of motion (active and passive)◦ Neurovascular status
Radiographic studies:◦ 3 planes: AP, Lateral and Oblique
47

Carpal FracturesCarpal FracturesScaphoid fractures:◦Most common carpal fracture◦Results from force applied on distal end with
wrist hyper extended.◦Common in young adults.◦Unless treated effectively it would result in mal-
union and permanent weakness and pain in the wrist. With subsequent osteoarthritis.
◦ If blood supply is confined to distal end, proximal end will undergo avascular necrosis.
◦Deep tenderness in anatomical snuffbox is felt.◦Treatment:
Stable: Cast for 12 weeks Unstable or non-union: open reduction and internal
fixation.48

49

Carpal FracturesCarpal FracturesTriquetral fracture:◦ 2nd most common carpal fracture◦Results from direct blow to the dorsum of the hand
or extreme dorsiflexion.◦On clinical examination, palpation of the triquetrum
is facilitated by radial deviation of the hand.◦Point tenderness is usually elicited directly over the
triquetrum.◦Treatment:
Chip fracture: symptomatic with 2-3 weeks immobilization. ROM
exercise once symptoms decrease. Body fracture:
Minimally displaced: cast immobilization for 4-6 weeks + ROM exercise
Displaced: Closed reduction and pinning or Open reduction and fixation
50

51

Metacarpal FracturesMetacarpal FracturesRelatively common. 30-40% of hand fracturesResult from direct or indirect trauma. Direct
trauma commonly results in transverse fracture, usually midshaft.
Most fractures are easily reducible, stable and managed non-operatively. Immobilization or controlled mobilization.
Indications of surgical intervention:◦ Intra-articular fractures, ◦Displaced and angulated fractures, ◦Unstable fracture patterns, ◦Combined or open injuries, ◦ Irreducible and unstable dislocations
52

53

Thumb FracturesThumb FracturesBennett’s fracture:◦ Fracture at the base of
the 1st Metacarpal.◦ Intra-articular fracture
subluxation: unstable arthritic joint with secondary loss of motion and pain.
◦ Swelling and pain at the thumb base
◦ Closed reduction and immobilization with thumb spica splint
◦ Open reduction and internal fixation.
Rolando’s fracture:◦ Comminuted (displaced)
thumb base fracture.◦ Improper healing would
lead to restriction of motion around Carpometacarpal joint.
◦ Swollen, tender thumb base. If significant varus has developed, a clinically visible deformity may be present.
◦ Swelling can mask a surprising amount of angulation.
◦ Open reduction and internal fixation.
54

Bennett’s Rolando’s55

56

Phalangeal FracturesPhalangeal FracturesDistal Phalanx:◦Extra-articular fractures are common, associated
with significant soft tissue injury.◦Crush injuries from a perpendicular force (injuries
from a car door or hammer)◦ Intra-articular fractures are associated with
extensor tendon avulsion (Mallet’s finger), flexor profundus tendon avulsion (Jersey finger).
◦Examination: Inspection: attitude of the injured finger, and localization of
any swelling. Neurovascular status should be examined as well as color, capillary refill, and digital temperature.
Palpation is done for tenderness.
◦Closed treatment is recommended with splinting and if necessary closed reduction
57

Phalangeal FracturesPhalangeal FracturesMiddle Phalanx:◦Blunt or crush force perpendicular to the long axis
of the bone.◦Angulation and rotation are two features of
instability that must be examined.◦Rotational deformities are serious injuries and are
detected clinically.◦Examination:
Inspection: for dislocations and sublaxations. Ask patient to fully flex the phalanx to examine alignment of digits.
Palpation: swelling and tenderness
◦ Treatment: Nondisplaced without impaction: require only dynamic
splinting for 2-3 weeks. Angulation and rotation require closed reduction and
splinting to restore finger alignment. 58

Phalangeal FracturesPhalangeal FracturesProximal Phalanx:◦More common than middle phalanx fractures.◦May result in a great deal of disability.◦Direct perpendicular force, a rotary force, or
hyperextension of the finger.◦Dorsal or palmar angulation may occur with these
fractures.◦Examination:
Inspection: attitude of the injured finger, and localization of any swelling. Neurovascular status (color, capillary refill, and digital temperature).
Palpation is done for tenderness.◦ Treatment:
Nondisplaced fractures: usually stable and treated by closed reduction and dynamic splinting.
Angulation or unstable fractures may require internal or external fixation.
59

60

AMPUTATION ANDAMPUTATION ANDREPLANTATIONREPLANTATION
61

IntroductionIntroductionReplantation: reattachment of a severed digit of
extremity.Not all patients with amputation are candidates
for replantationDecision is based on: Importance of the part,
level of injury, mechanism of injury and expected return of function.
Because hand function is severely compromised if the thumb or multiple fingers are not present to oppose each other, thumb and multiple-finger replants should be attempted.
Mechanism of injury may be the most predictive variable for successful replantation.
62

IntroductionIntroductionRecommended ischemia times for
reliable success:◦Digit: 12 hours for warm ischemia and 24
hours for cold ischemia.◦Major replant: 6 hours of warm and 12
hours of cold ischemia.Preoperative preparation: radiography
of both amputated and stump parts to determine the level of injury and suitability for replantation
63

64

OutcomeOutcomeOverall success rates for replantation
approach 80%.Better outcome with Guillotine (sharp)
amputation (77%) compared to severely crushed and mangled body parts(49%).
Studies have demonstrated that patients can expect to achieve 50% function and 50% sensation of the replanted part.
65

66

ReferencesReferencesPlastic Surgery, Goldwyn and Cohen,
3rd edition.Plastic Surgery, Grabb and Smith, 3rd
edition.Clinical Anatomy, Richard Snell, 6th
edition.Macleod’s Clinical Examination, 11th
edition.www.emedicine.com
67