Embed Size (px)
Citation preview

“A ‘wheelie’ interesting case”
Interactive E-Learning Case
- Emergency Medicine -

Module Information
Author: Terasa Broom
SpR Emergency Medicine
Yorkshire Deanery Rotation
Module reviewer: Dr Taj Hassan
Consultant in EM, Leeds
Date of submission: July 2007
Date of review: July 2008

Pre-Alert
• You are the Emergency Department SpR
• 00:30 Thursday night
• Red call from ambulance service:– 41yr old female
– Fall one day ago
– Altered conscious level
– Bleeding from left ear
– ETA 5 minutes

Pre-Arrival Actions
• Organize team to await her arrival in resus (including SHO and senior nurse)
• Prepare resus room
• Organise equipment (including intravenous access and airway tools)
• Ambulance arrives……

Ambulance Handover
• 42 year old female
• Fall from ‘wheelie’ bin 27 hours previously onto concrete
• No loss of consciousness or vomiting reported
• Headache since event, getting worse
• Bleeding noted from left ear
• Altered conscious level
• Perseveration
• Haemodynamically stable

Primary Survey
A: Patent, talking intermittently
B: RR 16/min, SaO2 100% (room air)
Good and equal air entry
C: Pulse 56/min regularBP 180/90 mmHg
Cap refill <2 sec
D: GCS - E3 M6 V4 Intermittent periods of lucidity
E: Bleeding from left ear Boggy haematoma left parietal region of skull

Q1. Immediate Actions
What are the most important immediate actions in managing this patient (choose four options)?
1. Call an anaesthetist 2. Endotracheal intubation
3. Oro-pharyngeal airway 4. Oxygen therapy
5. IV access/bloods 6. Analgesia
7. Catheterisation 8. Organise CT scan
9. ENT opinion 10. Measure BM

Q1. AnswerALWAYS follow the ABC rules:
• A: patent and currently ‘safe’ - GCS 13 [airway deemed to be ‘safe’ if GCS > 8]
• B: breathing normally, but still requires O2 therapy A. 4
• C: obtain IV access and routine bloods A. 5[coagulation screen and G+S particularly important if head injury present]
• D: Never forget to check the glucose! A. 10[low BMs are a frequently missed cause of altered consciousness]
NB always attempt to make the patient as comfortable as possible - simple analgesia will not affect the conscious level and will make further investigation and management easier. Additionally, it should be remembered that pain causes an increase in ICP A. 6

Secondary Survey
• IV access is achieved and analgesia and slow IV fluids started
• The patient, although intermittently confused, complies with examination
• Apart form the scalp haematoma and the bleeding from the left ear no other injuries are identified
• It is noted that the right pupil is dilated and unresponsive to light stimulus

Q2. Choice of Imaging
What type of imaging should be requested to help with your assessment of this patient’s injuries (choose one answer)?
1. Plain skull x-ray
2. MRI Head
3. CT Head
4. No immediate imaging required

Q2. Answer3. CT Head
According to the NICE head injury guidelines an immediate CT should be organised in any of the following circumstances:
– GCS<13 at any time since injury
– GCS 13-14 at 2 hrs post injury
– Focal neurological deficit
– Suspected open or depressed skull fracture
– Any sign of basal skull fracture
– Post-traumatic seizure
– >1 episode of vomiting (in adult)

CT Head

Q3. Interpretation of CT Head
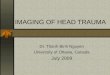
What are the two most obvious findings on the CT scan of this patient’s head?
1. _ _ _ _ _ _ _ _ _ _ _ _
2. _ _ _ _ _ _ _ _ _ _ _ _

Q3. Answer1.The CT shows an acute right sided biconvex sub-dural haematoma.
2.There is also associated mid-line shift towards the left
subdural
midline shift

Further CT Scan

Q4. Interpretation of CT Head
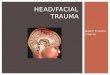
What four things do you notice on this further CT?
1. _ _ _ _ _ _ _ _ _ _ _ _
2. _ _ _ _ _ _ _ _ _ _ _ _
3. _ _ _ _ _ _ _ _ _ _ _ _
4. _ _ _ _ _ _ _ _ _ _ _ _

Q4. Answerright fronto-parietal craniotomy with
soft tissue swelling and flecks of gas extracranially adjacent to the
site (consistant with recent surgery)

Q4. Answer cont.
evacuated sub-dural

Q4. Answer cont.
small focus of evolving haematoma
within the right temporal lobe

Q4. Answer cont.
some midline shift

Potential Problems
• Postoperative complications:
– Elevated ICP
– Brain oedema
– New or recurrent bleeding/haematoma
– Infection
– Seizures
• Prognosis: – Definitive prognosis often is not possible at the time of
emergency department evaluation– Ultimate prognosis is related to the amount of associated direct
brain damage and the damage resulting from the mass effect of the SDH

Learning Points• Always follow the ATLS approach
• Be aware that GCS can change/fluctuate and so frequent re-examination and assessment is necessary (particular attention needs paid to the patient’s airway). Make sure to document the timing and each component of the GCS clearly to judge any deterioration
• Make sure to have instituted all possible neuro-protective measures in patients who have a high likelihood of intra-cranial pathology (oxygen, adequate ventilation to main normocapnia, adequate fluid resuscitation, slight head up tilt to help control ICP, temperature control and glycaemic control
• Organise definitive investigations and referral to the specialty team but make sure to document a clear management plan
[view e-learning tutorial on sub-dural haematomas]