Embed Size (px)
DESCRIPTION
2011 National HIV Prevention Conference. Plenaries. Wednesday.
Citation preview

Tiffany LaDanaWest, MPH, MSPHBureau Chief, Strategic Information BureauDistrict of Columbia, Department of Health
Uses of Strategic Information to Assess Health Equity

Health Inequities in US Gender, Race and Socioeconomic Factors that drive health inequities
in US
Heavily Influence by Environment Disease Syndemics Access to Prevention, Care and Treatment Services
Influence Individual Behavior Risk Behaviors in social and sexual networks Health Seeking Behavior Utilization of Prevention, Care and Treatment Services
Triangulate Syndemic, Behavioral, Service to assess Health Inequities to target policies and programs populations at greatest need
Greater Focus on Health Outcomes where inequities exist

Cumulative and Annual Diagnosed Number of AIDS Cases, By Race/Ethnicity and Year, United States, 1989-2008
Cumulative_v_Dx_with_trails_wmv.wmv

Cumulative and Annual Diagnosed Number of AIDS Cases, By Transmission Category and Year, United States, 1989-2008
MOT_no_total_wmv.wmv

Annually Diagnosed AIDS Cases, by Sex and Year, United States, 1989-2008

Percent Below the Federal Poverty Line, By Race/Ethnicity and Year, United States, 1989-2008

HIV Infection Among Heterosexuals in Urban Areas, by Socio-Economic Indicators, 2006-2007, N=14,837
National HIV Behavioral Surveillance (NHBS) Heterosexuals at High Risk for HIVAreas of High Rates of HIV/AIDS and Poverty
Approximately 2.0% HIV Prevalence 2.1% Women and 1.9% Men 4.2% 40-50 year olds, 2.2% 30-39 year olds, 0.6%, 18-29 year
olds 3.1% Northeast, 2.7% South, Midwest, South, Territories
<1%
*CDC. Characteristics Associated with HIV Infection Among Heterosexuals in Urban Areas with High AIDS Prevalence --- 24 Cities, United States, 2006--2007. MMWR 2011;60:1045-1049.

HIV Infection Among Heterosexuals in Urban Areas, by Socio-Economic Indicators, 2006-2007, N=14,837-Structural/Environmental
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
HIV
Pre
vale
nce
*CDC. Characteristics Associated with HIV Infection Among Heterosexuals in Urban Areas with High AIDS Prevalence --- 24 Cities, United States, 2006--2007. MMWR 2011;60:1045-1049.

HIV Infection Among Heterosexuals in Urban Areas, by HIV Risk Factor, 2006-2007, N=14,837-Behavioral
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
Used crack cocaine Did not Exchanged sex for money or drugs
Did not Received an STD diagnosis
Had not
HIV
Pre
vale
nce
*CDC. Characteristics Associated with HIV Infection Among Heterosexuals in Urban Areas with High AIDS Prevalence --- 24 Cities, United States, 2006--2007. MMWR 2011;60:1045-1049.

Estimated Number of New HIV Infections among Men who have Sex with Men, By Age
Estimated Number of New HIV Infections among Men who have Sex with Men (MSM), 2009,By Race/Ethnicity and Age
* Estimates of New HIV Infections in the United States, 2006–2009, The Center for Disease Control and Prevention Fact Sheet, August 2011

Estimated Number of New HIV Infections among Men who have Sex with Men, By Race
Estimated Number of New HIV Infections among Men who have Sex with Men (MSM), Ages 13-29, 2006-2009, By Race/Ethnicity and Age
* Estimates of New HIV Infections in the United States, 2006–2009, The Center for Disease Control and Prevention Fact Sheet, August 2011

Washington DC

14
• 16,721 reported living with HIV/AIDS in the District at the end of 2009• 5,505 new HIV cases reported between 2005 and 2009• 3.2% of the District’s population diagnosed with HIV/AIDS• one-third to one-half of people (locally) may be unaware of their HIV status. (Source: DC NHBS data)
Prevalence of HIV/AIDS in the District of Columbia, 2009
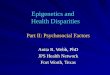
DC Resident Living with HIV/AIDS as of 2009, by Gender and Race/Ethnicity
Black Hispanic White Other Total
Male 8,325 756 2,620 350 12,051
Female 4,256 156 141 117 4,670
Total 12,581 912 2,761 467 16,721
DC% 75.2% 5.5% 16.5% 2.8% 100.0%
US% (2008) 49.3% 20.0% 27.8% 2.9% 100.0%
Overview: HIV/AIDS in District of Columbia

HIV Prevalence among High Risk Population, District of Columbia
7.1%
4.7%
3.4%
2.9% 2.8%
2.1%1.8%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
Black Males
All Blacks Hispanic Males
White Males
Black Females
All Hispanics
All Whites
25.0%
7.7%
13.0%
3.9%
6.3%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Black MSM White MSM IDU Male Heterosexuals
Female Hterosexuals
HIV Prevalence among Study PopulationsHIV Prevalence by Sex and Race/Ethnicity

Syndemics and Service Delivery High rates of STDs among
youth High rates of Syphilis,
chronic Hepatitis B and HIV among MSM and High rates of co-infection
High rates of chronic Hepatitis C among IDU and Heterosexuals
Sub-optimal health outcomes
Approximately 91% Health Care Coverage
Generous prevention, care and treatment programs
No ADAP Waiting List Extensive ADAP formulary Generous coverage on local
public health insurance programs
Poor Healthcare Utlization

Mean Community Viral Load among Whites and Blacks Living with HIV/AIDS in DC, 2008
18,283
39,173
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
White Black
Mea
n C
omm
unit
y V
iral
Loa
d (c
opie
s/m
L)
N=762 N=3,395

Linkage to Care among Newly Diagnosed Cases in DC, by Race/Ethnicity, 2005-2009
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
< 3 months 3-6 months 6-12 months > 1 year
Prop
orti
on e
nter
ing
care
White
Black
*Entry into care was determine by the date of the first CD4 count or percentage test or viral load test reported to the DCDOH.

Retention in Care and Not in Care among Newly Diagnosed Cases in DC, by Race/Ethnicity 2005-2009
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
White Black
Retained in care
No care
Not in care: absence of any HIV-related laboratory tests indicative of receipt of HIV primary care within the study period•Continuously in care (retained in care): presence of at least 2 HIV-related laboratory tests within 12 months of the initial linkage laboratory test date, each 10 to 14 weeks apart (modified HRSA definition)

National HIV Behavioral Surveillance Project (NHBS) Men who have Sex with Men, 2008
Unprotected Receptive Anal Intercourse, By Race, N=422
Unprotected Insertive Anal Intercourse, By Race, N=422
56.7%
25.3%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
White MSM Black MSM
51.0%
29.0%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
White MSM Black MSM

7.9%
26.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
White MSM Black MSM
National HIV Behavioral Surveillance Project (NHBS) Men who Have Sex with Men, 2008
HIV Prevalence among Study Participants, by Race, N=422

Mean Community Viral Load among White and Black MSM with HIV/AIDS in DC, 2008
N=645 N=901
19,732
31,404
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
White MSM Black MSM
Mea
n C
omm
unit
y V
iral
Loa
d (c
opie
s/m
L)

Linkage to Care among Newly Diagnosed White and Black MSM in DC, 2005-2009
Linkage to care was determine by the date of the first CD4 count or percentage test or viral load test reported to the DCDOH.
Pearson’s Chi-square p value, p=0.0006
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
< 3 months 3-6 months 6-12 months > 1 year
White MSM
Black MSM

Retention in HIV Care among Newly Diagnosed White and Black MSM in DC, 2005-2009
Pearson’s Chi-square p-value, p=0.0020
Continuous care is defined as having evidence (e.g. HIV-related lab test) of at least 2 visits to an HIV medical provider 10-14 weeks apart. Sporadic care is defined as having only one visit to a provider or 2 visits but more than 14 weeks apart.
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Retained in Care Sporadic Care No Care
Prop
orti
on o
f MSM
Cas
es
White MSM
Black MSM

Social Determinants of Health

Social Determinants of Health (2)

Social Determinants of Health (3)

Targeted Messaging

Targeted Services Finding Action
General Populations • High burden of disease (HIV, STD, HepC)
• Opt out routine screening in emergency departments
• Routine GC/CT screening in women and girls of childbearing age
• Health Behavior and Risk Reduction• Municipal Condom Distribution:
online, venues, schools• Increased HIV/STD partner services
MSM • Co morbidities: HIV/Syphilis• High Rates HIV• High rates of high risk behaviors
• Engage w/providers who serve MSM• Encourage routine HIV and syphilis
screening• Bi-Annual HIV and STD testing• Messages developed to reduce stigma• Increase HIV/STD partner services• Hepatitis A/B Screening/Vaccination
Heterosexuals • High rates HIV, STDs• High rates of high risk behaviors• Low risk perception
• (General Population Strategies)• Social Marketing/harm Reduction• Integrated Partner Services (PCRS)
29

Condom Distribution Locations

Geographic Distribution of Substance Abuse Needle Exchange Programs Overlay - Heroin Arrests in the District of Columbia, 2008
Heroin Arrests
Substance Abuse Needle Exchange Programs

Preview
Dir
Preview
DC GOVTLeadership,
Coordination, $$$NGOs, CBOs:
program, pops
Fed Gov: $$$, TA, Guidelines
DC Planning Councils:Priorities, $
direction/advice
Medical Establishment: services, pops
FBOs: leaders, stigma, support, services
Involvement in the HIV response
Academia: TA, Research, Services
Media: info, ads
Families, Social Networks, Individuals:change
•Priorities•Experiences & Approaches•Reality & Implementation•Best Practices•Gaps in Service, Effect and
Intention•Cost-efficiency, ResourcesEVENTUAL IMPACT
Private/Businessinsurance, social resp
prevention

Conclusions: Health Inequalities are associated with both environmental and
social and sexual networks Role of Public Health System is to ensure targeted, evidence
scalable strategies that influence positive health outcomes Targeted, Integrated Messages and Service Delivery Monitoring Evaluation of Health Outcomes to influence Change

Special Thank You ONAP-LA Mario Perez
George Washington University School of Public Health Alan Greenberg, Amanda Castel, Manya Magnus, Irene Kuo
Emory University CFAR Patrick Sullivan, Jeb Jones
HAHSTA-DC Angelique Griffin, Jen Opoku, Sarah Willis, Rowena Samala
CDC Irene Hall, Amy Lansky
Dad, Mom, Tony-For Believing in Me