Embed Size (px)
Citation preview

Hearing impairment Hearing impairment and rehabilitationand rehabilitation
OUTLINEOUTLINE
Types of hearing loss
Classification of hearing loss Diagnosing and managing different kinds of hearing loss; e.g
congenital hearing loss otosclerosis, presbyacusis, noise Induced Hearing Loss ,Meniers disease ,ototoxicity
Performing and interpreting various subjective and objective hearing tests
Tuning fork test
Pure Tone Audiometry
Impedance Audiometry
Brain Stem Evoked Response Audiometry
HEARING IMPAIRMENTHEARING IMPAIRMENT
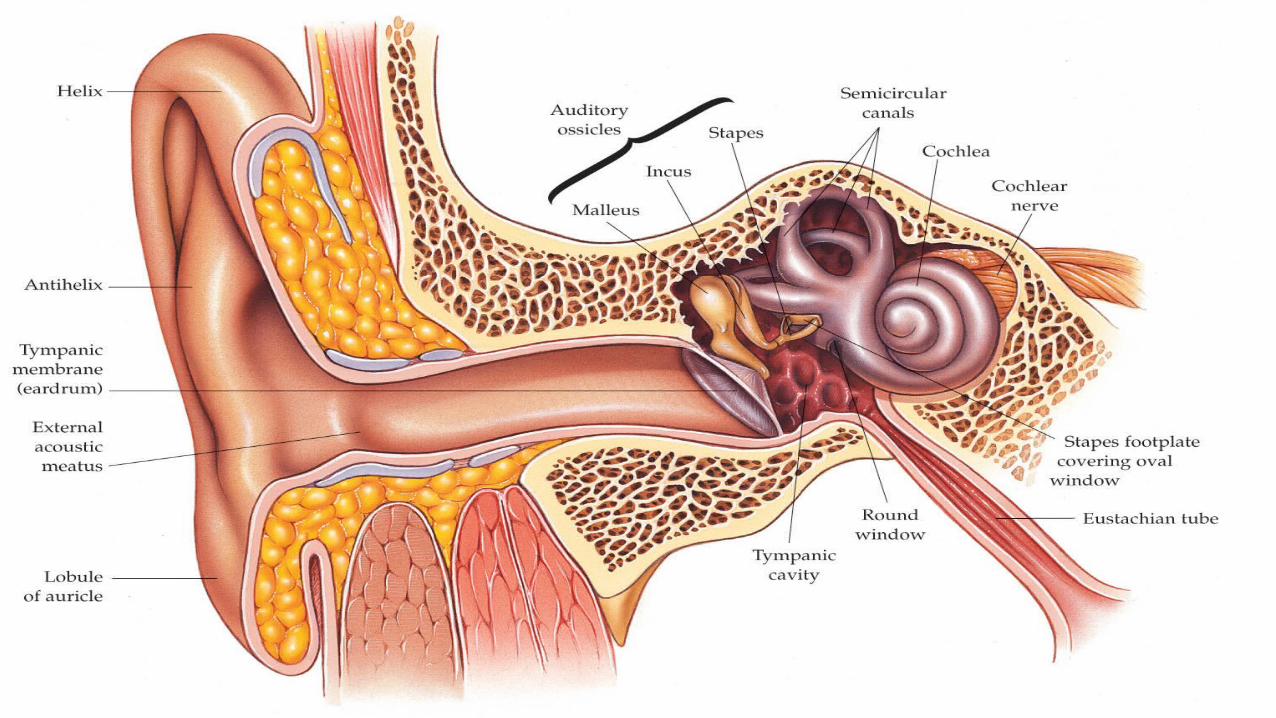
Hearing impairment, also called deafness or hearing loss, occurs when there’s a problem with or damage to one or more parts of the ear.
U.S. population 270+ million2 million Deaf 26 million Hard of Hearing
1 of every 10 people has a hearing loss Over age 65, 1 in every 3 persons has some degree of hearing loss 80% of hearing people are in denial
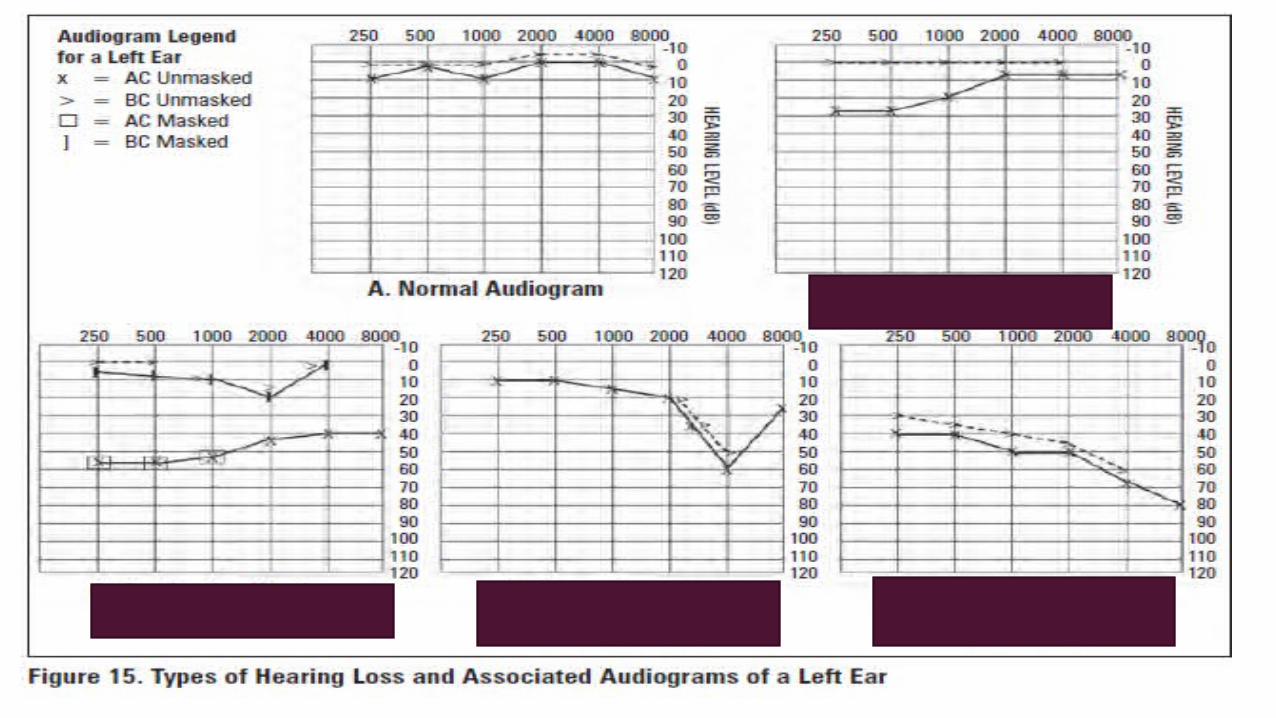
TYPES OF HEARING LOSSTYPES OF HEARING LOSS
1. Conductive Hearing Loss (CHL)
• the conduction of sound to the cochlea is impaired
• can be caused by external and middle ear disease
2. Sensorineural Hearing Loss (SNHL)
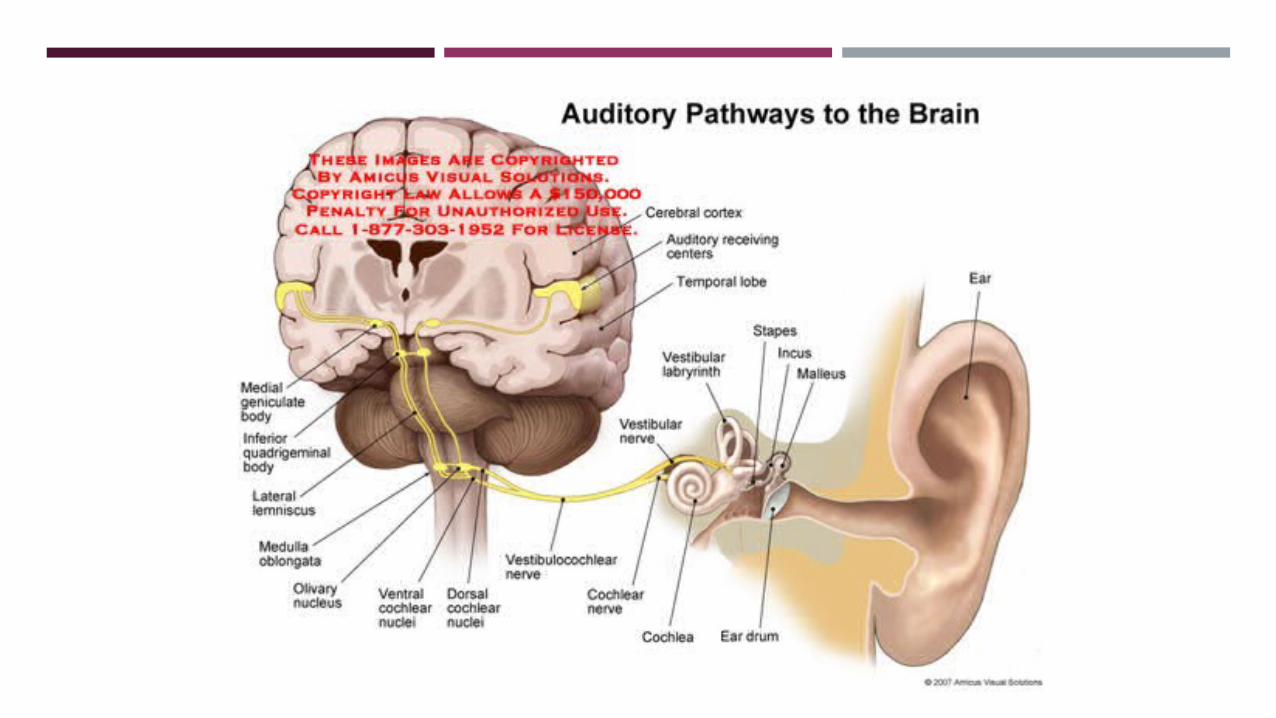
• due to a defect in the conversion of sound into neural signals or in the transmission of those signals to the cortex
• can be caused by disease of the cochlea, acoustic nerve ( CN Vlll), brainstem, or cortex
TYPES OF HEARING LOSSTYPES OF HEARING LOSS
3. Mixed Hearing Loss
• the conduction of sound to the cochlea is impaired, as well as transmission through the cochlea to the cortex
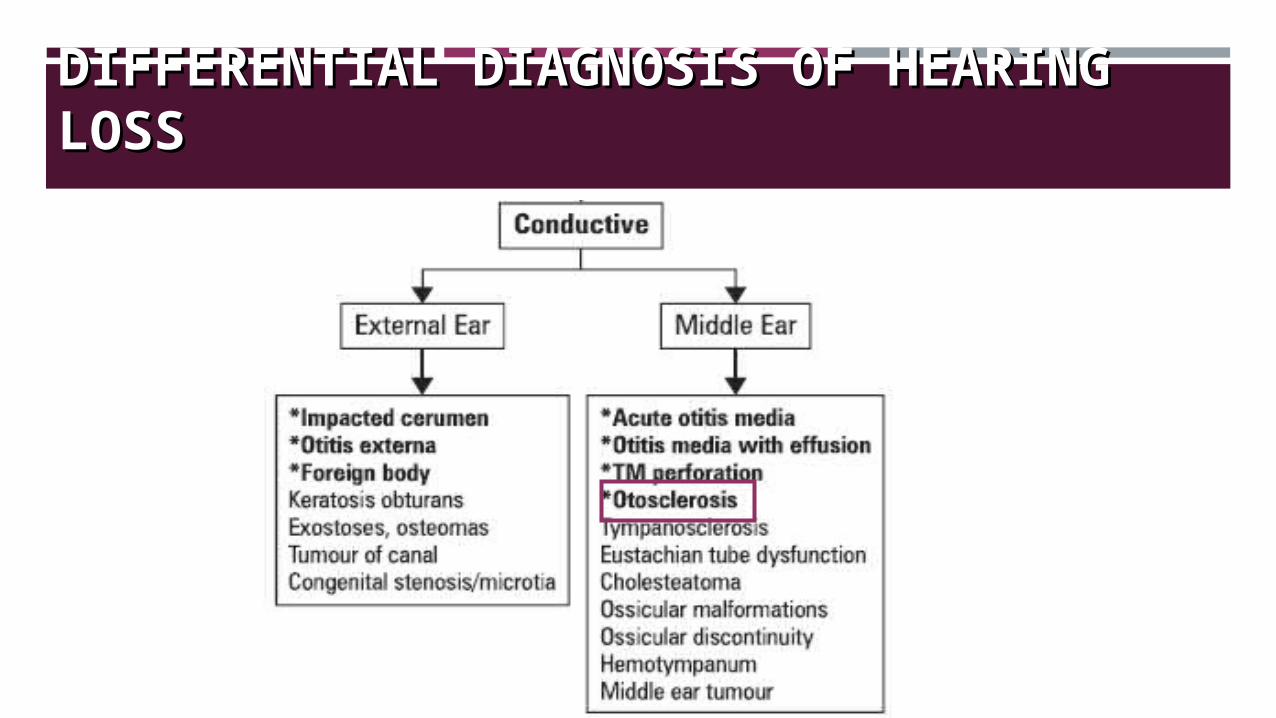
DIFFERENTIAL DIAGNOSIS OF HEARING DIFFERENTIAL DIAGNOSIS OF HEARING LOSSLOSS
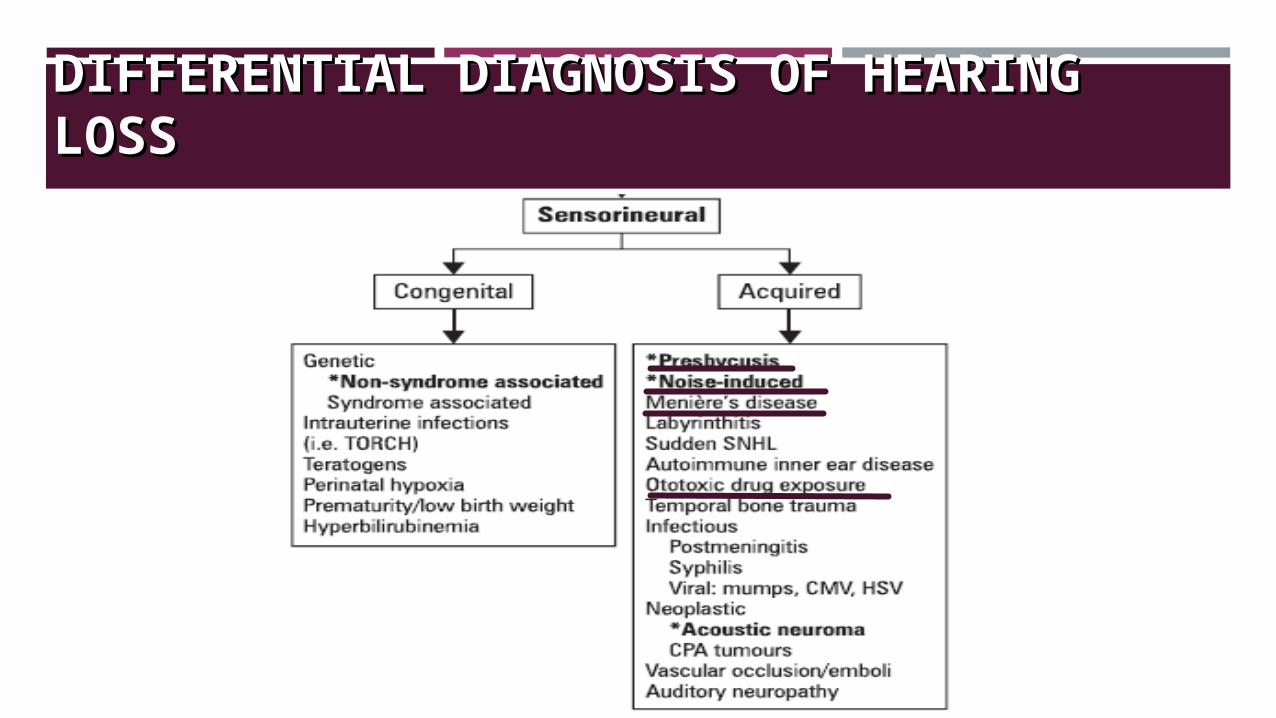
DIFFERENTIAL DIAGNOSIS OF HEARING DIFFERENTIAL DIAGNOSIS OF HEARING LOSSLOSS

APPROACH
HISTOHISTORYRY
HPI:
Onset (sudden or gradual)
Duration
Unilateral/ bilateral
Continuous / Intermittent
HISTOHISTORYRY
HPI:
Exposure- noise, drugs, viral illness
History of ear of head trauma
History of surgeries
Associated symptoms- pain, discharge, tinnitus, vertigo
HISTORYHISTORY
PMH: Chronic illness: DM, HTN, Hypothyroidism Previous surgeries
Rx: Ototoxic drugs
Amino glycosides, diuretics, quinine, aspirin
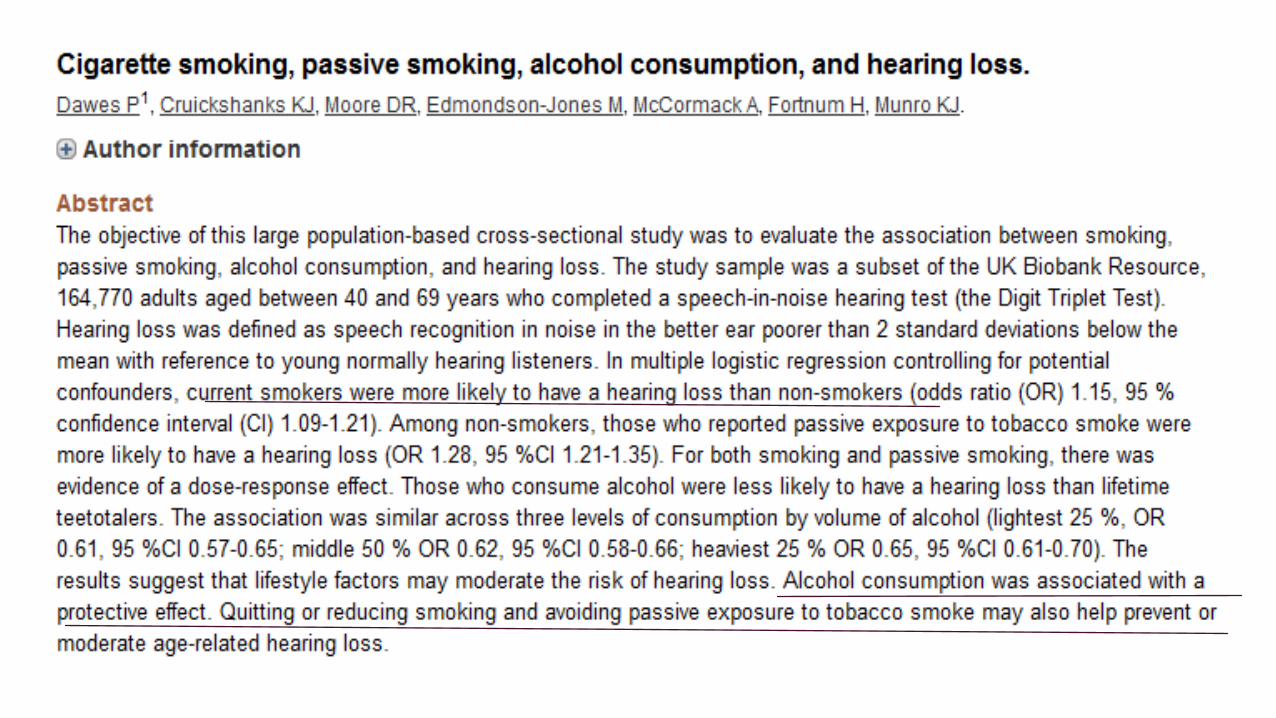
Social history: Occupation Tobacco Alcohol Cocaine Marijuana
PHYSICAL PHYSICAL EXAMINATIONEXAMINATION
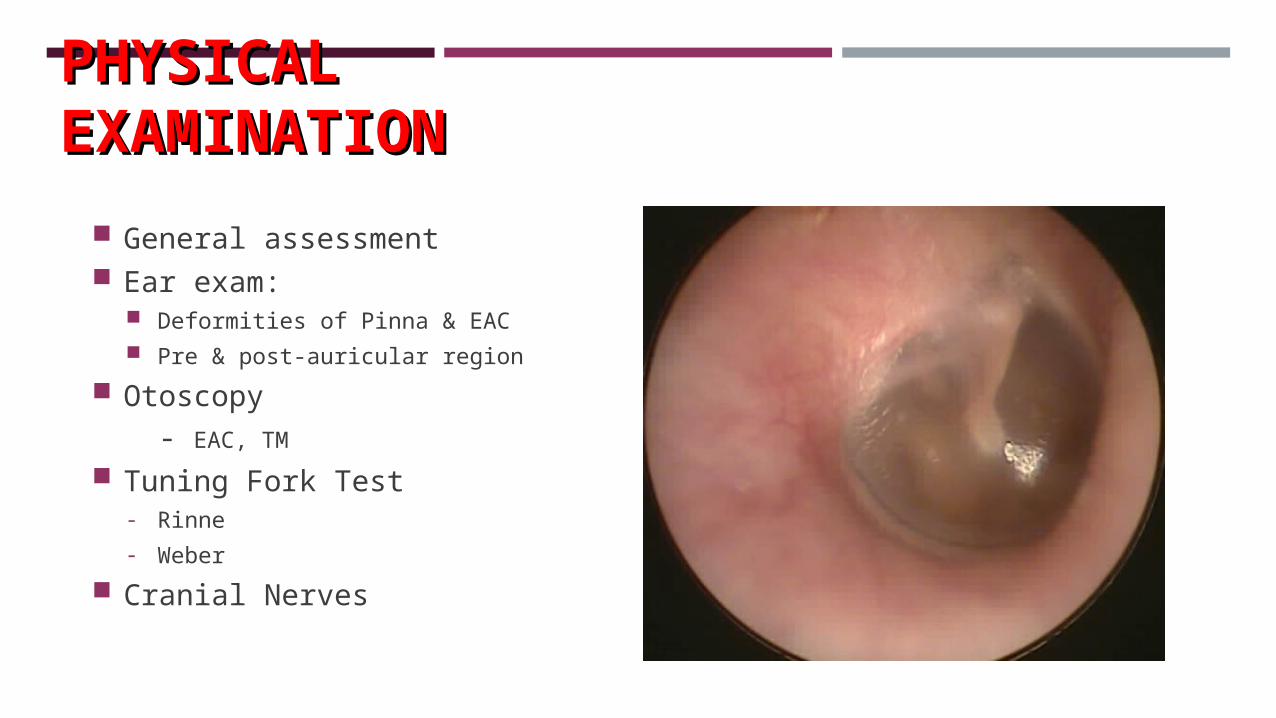
General assessment Ear exam:
Deformities of Pinna & EAC Pre & post-auricular region
Otoscopy - EAC, TM
Tuning Fork Test- Rinne
- Weber
Cranial Nerves
INVESTIGATIONSINVESTIGATIONS
Specific hearing tests
Tuning Fork Tests
Pure tone audiometry
Impedance audiometry
Brain stem evoked response audiometry
Radiology
- CT & MRI of skull & temporal bones
HEARING TESTSHEARING TESTS
Subjective Tonic Fork test
Pure tone audiometry (PTA)
Objective Tympanometry (impedance audiometry)
Electric response audiometry (ERA).
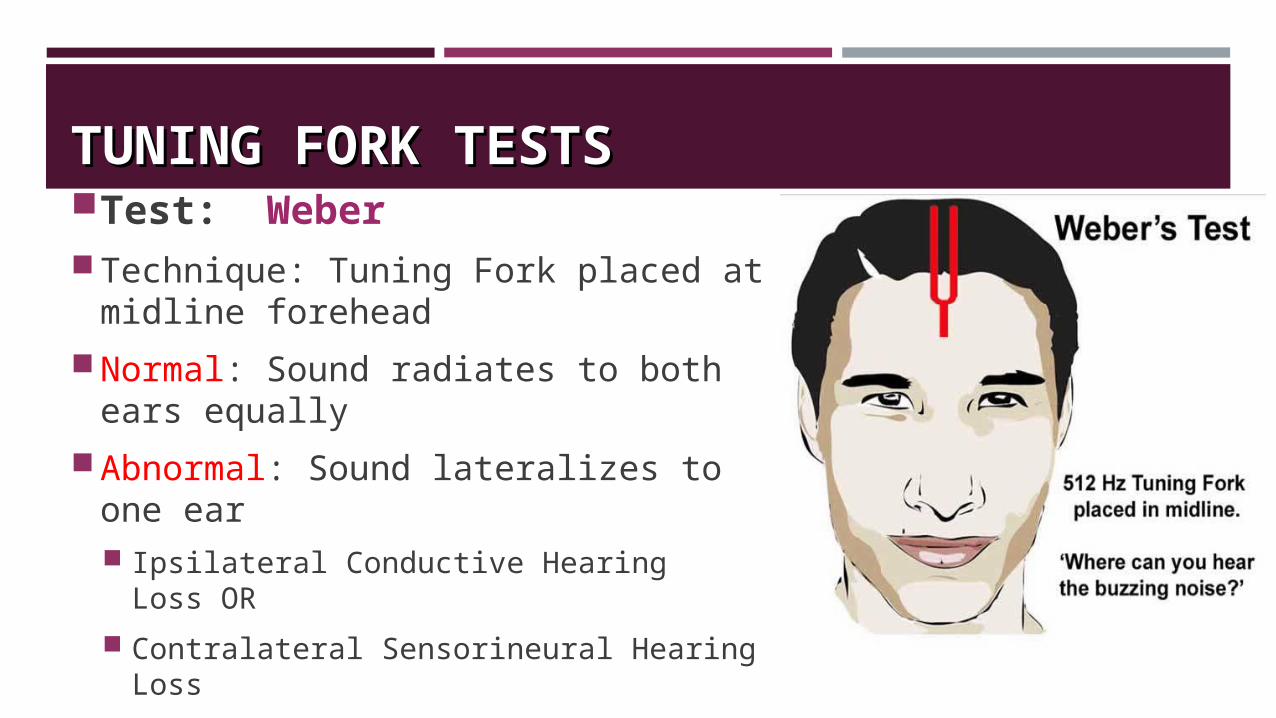
TUNING FORK TESTSTUNING FORK TESTSTest: Weber Technique: Tuning Fork placed at
midline forehead
Normal: Sound radiates to both ears equally
Abnormal: Sound lateralizes to one ear Ipsilateral Conductive Hearing Loss OR
Contralateral Sensorineural Hearing Loss
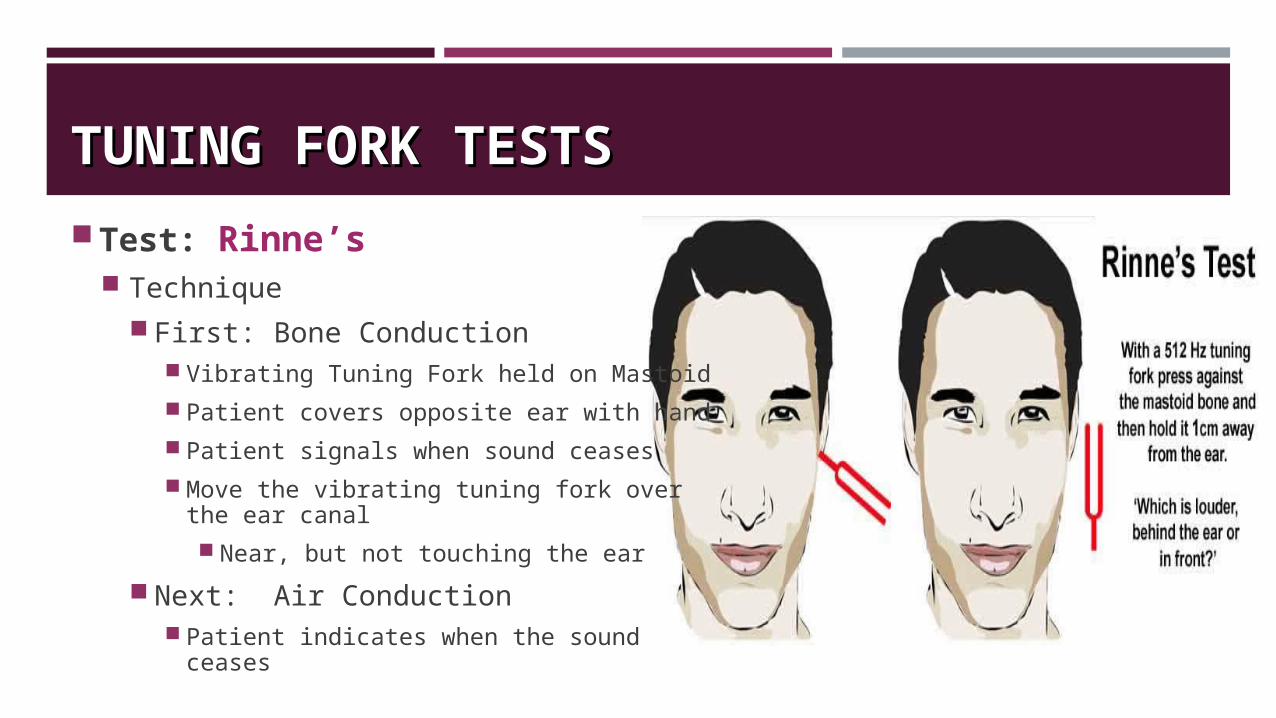
TUNING FORK TESTSTUNING FORK TESTSTest: Rinne’s
TechniqueFirst: Bone Conduction
Vibrating Tuning Fork held on Mastoid
Patient covers opposite ear with hand
Patient signals when sound ceases
Move the vibrating tuning fork over the ear canal
Near, but not touching the ear
Next: Air Conduction Patient indicates when the sound
ceases
TUNING FORK TESTSTUNING FORK TESTS
Test: Rinne’s Normal: Air Conduction is better than Bone Conduction
Air conduction usually persists twice as long as bone
Referred to as "positive test"
Abnormal: Bone conduction better than air conduction
Suggests Conductive Hearing Loss
Referred to as "negative test"
PURE TONE AUDIOMETRY (PTA)PURE TONE AUDIOMETRY (PTA)
PTA is the key hearing test used to identify hearing threshold level of an individual, enabling determination of the degree, types and configuration of hearing loss.
Provides the basis for diagnosis and management.
The symbols used on most audiograms are: x - left, air conduction
o - right, air conduction
] - left, bone conduction
[ - right, bone conduction
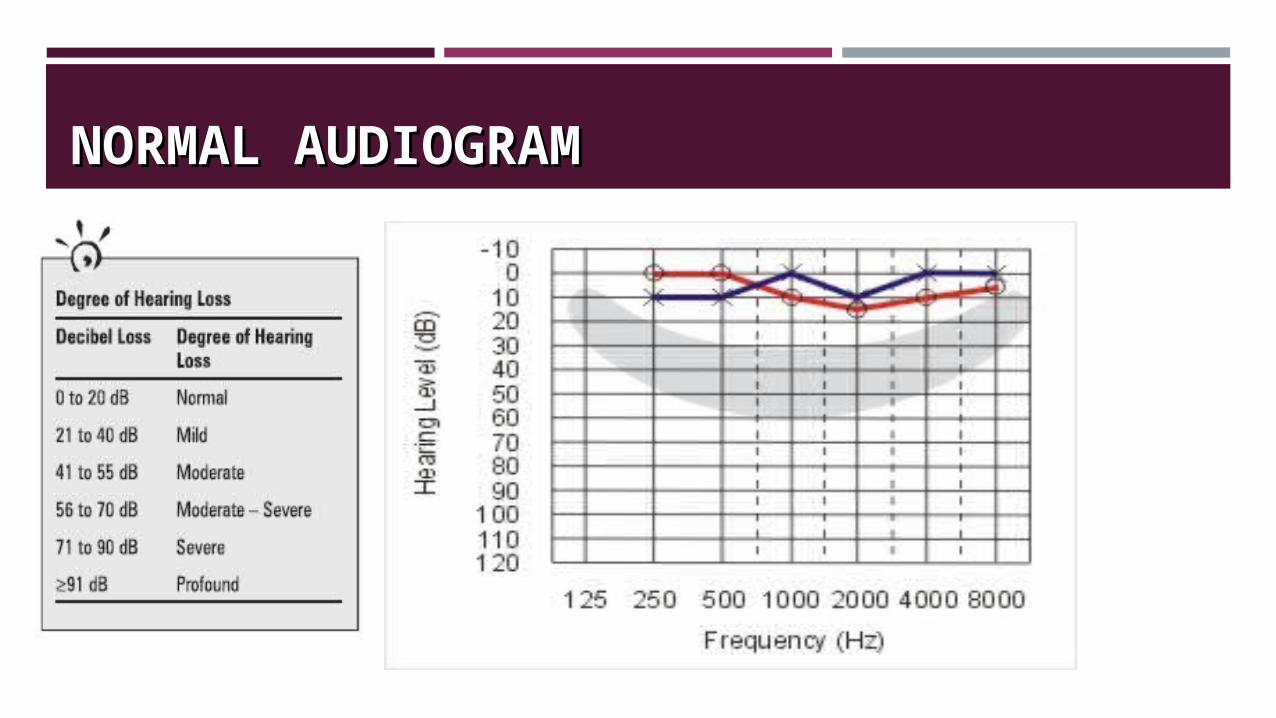
NORMAL AUDIOGRAMNORMAL AUDIOGRAM
TYMPANOMETRY (IMPEDANCE TYMPANOMETRY (IMPEDANCE AUDIOMETRY)AUDIOMETRY)
Assess the function of middle ear and Eustachian function of middle ear and Eustachian tube.tube.
Very useful when screeningscreening for middle ear effusion.
It is not a hearing testnot a hearing test, but rather a measure of energy transmission through the middle ear.
It can also assess the integrity of stapedius refluxstapedius reflux. .
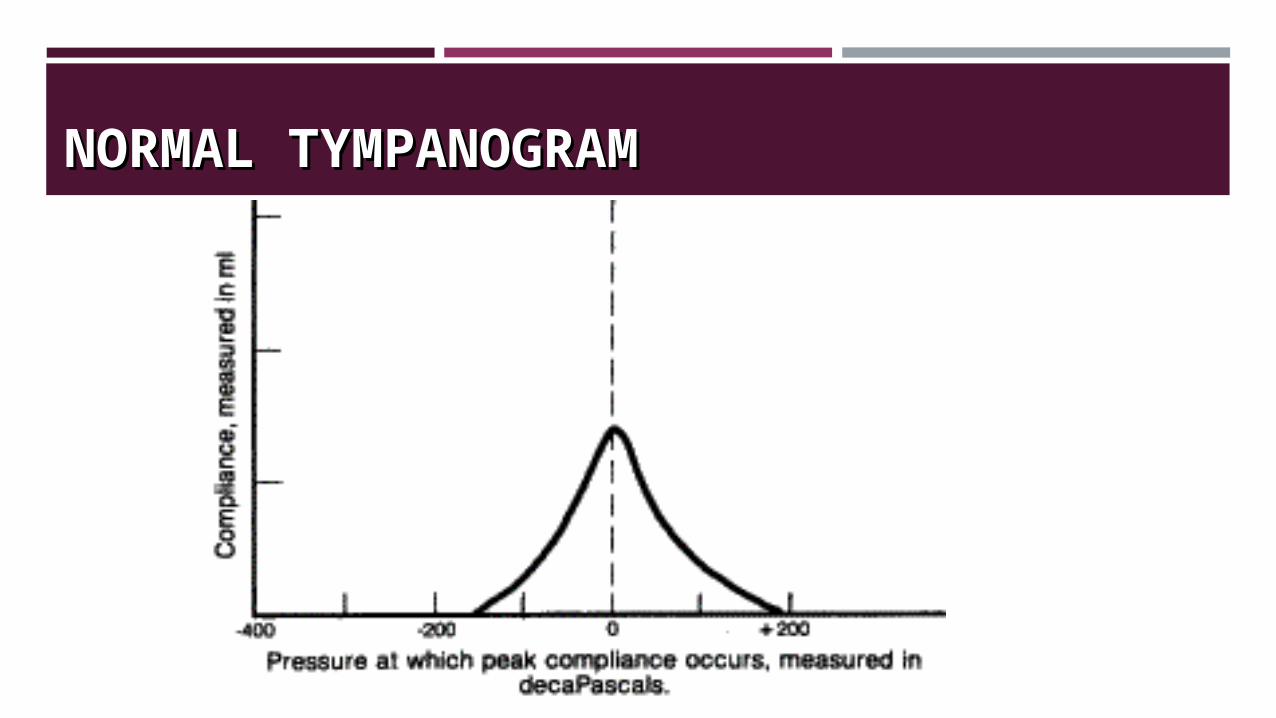
NORMAL TYMPANOGRAMNORMAL TYMPANOGRAM
AUDITORY BRAINSTEM RESPONSE (ABR) AUDITORY BRAINSTEM RESPONSE (ABR) AUDIOMETRYAUDIOMETRY
An objective neurologic test of auditory brainstem function in response to auditory (click) stimuli.
Procedure: The stimulus either in the form of click or tone pip is transmitted to the ear via a transducer placed in the insert ear phone or head phone. The wave froms of impulses generated at the level of brain stem are recorded by the placement of electrodes over the scalp.
AUDITORY BRAINSTEM RESPONSE (ABR) AUDITORY BRAINSTEM RESPONSE (ABR) AUDIOMETRYAUDIOMETRY
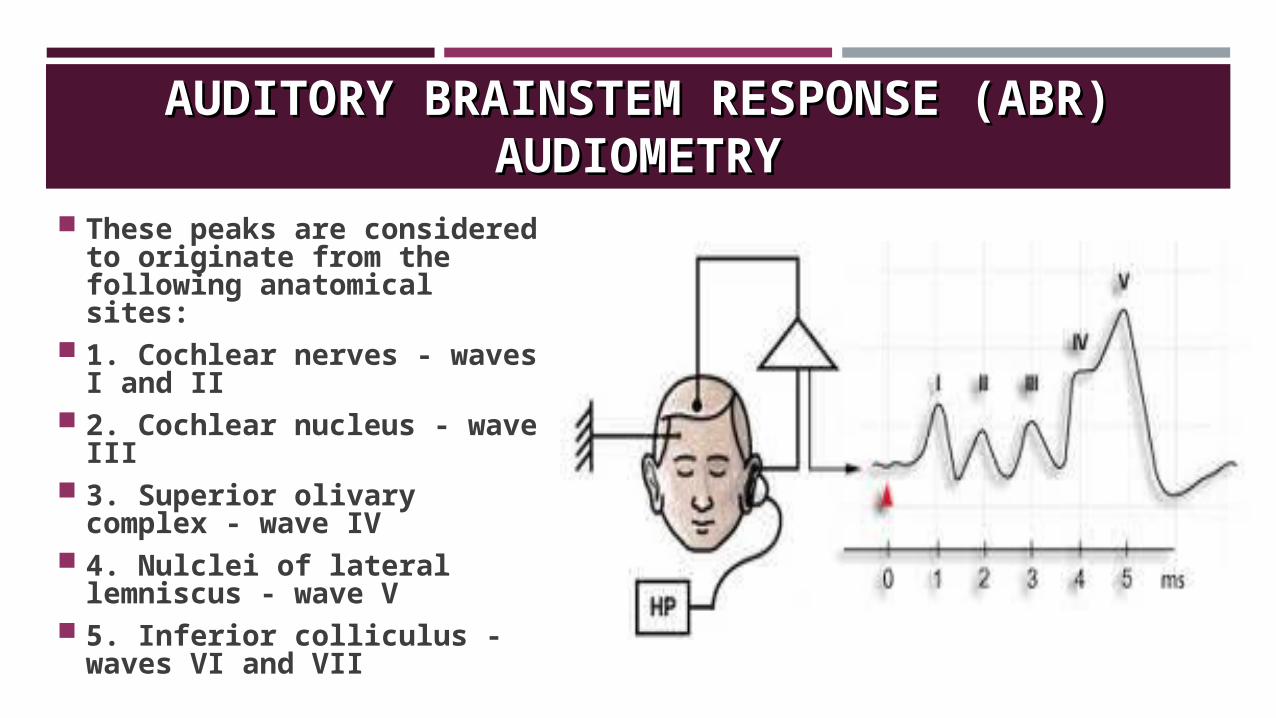
These peaks are considered to originate from the following anatomical sites:
1. Cochlear nerves - waves I and II
2. Cochlear nucleus - wave III
3. Superior olivary complex - wave IV
4. Nulclei of lateral lemniscus - wave V
5. Inferior colliculus - waves VI and VII

CASES
CASE 1CASE 1
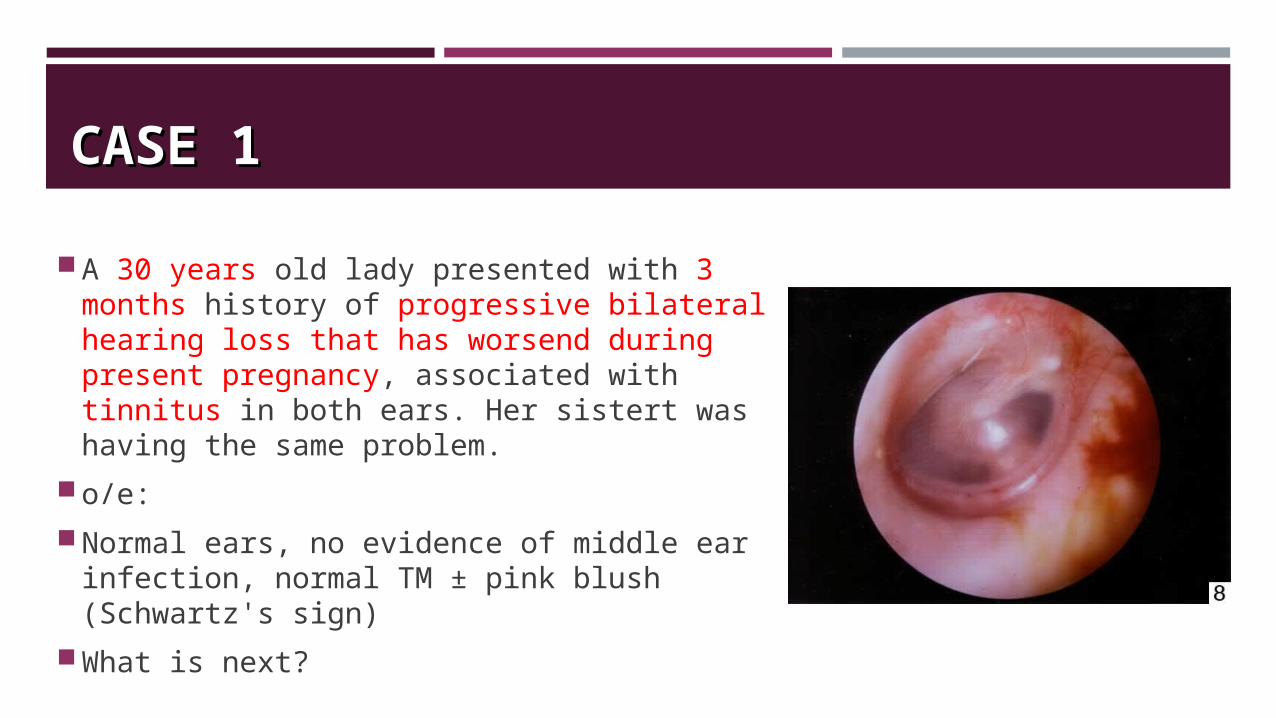
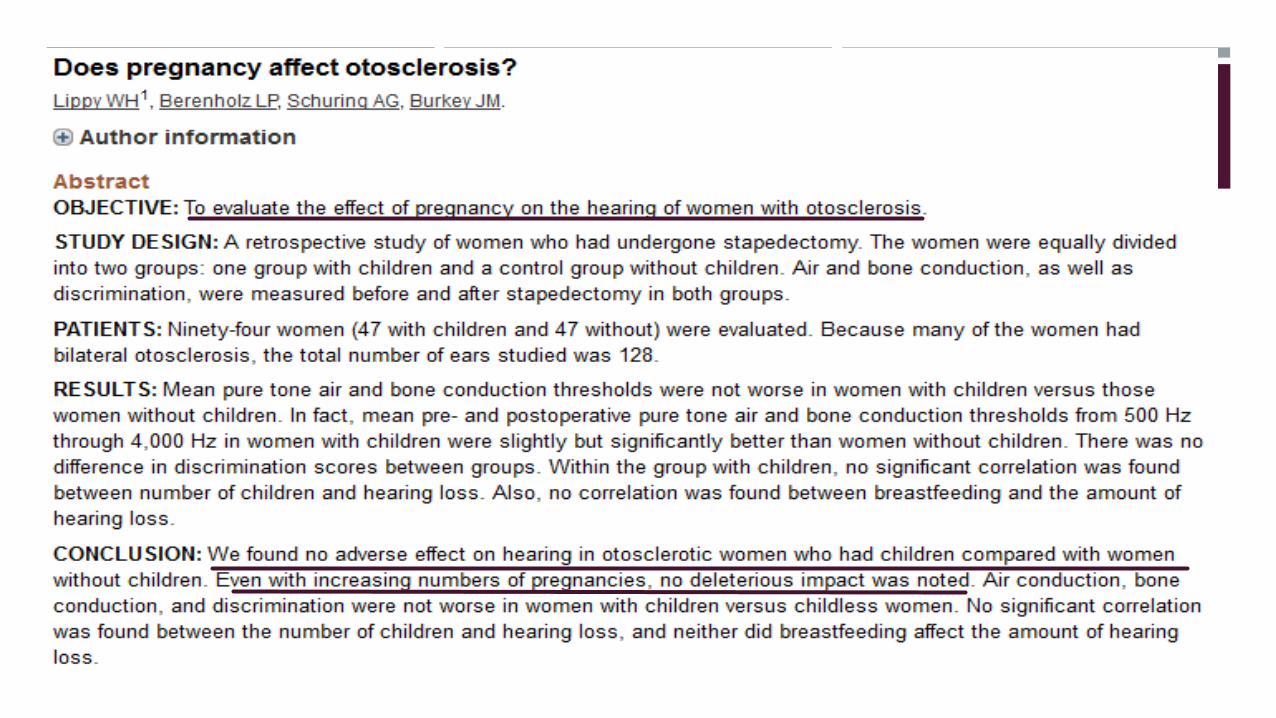
A 30 years old lady presented with 3 months history of progressive bilateral hearing loss that has worsend during present pregnancy, associated with tinnitus in both ears. Her sistert was having the same problem.
o/e:
Normal ears, no evidence of middle ear infection, normal TM ± pink blush (Schwartz's sign)
What is next?
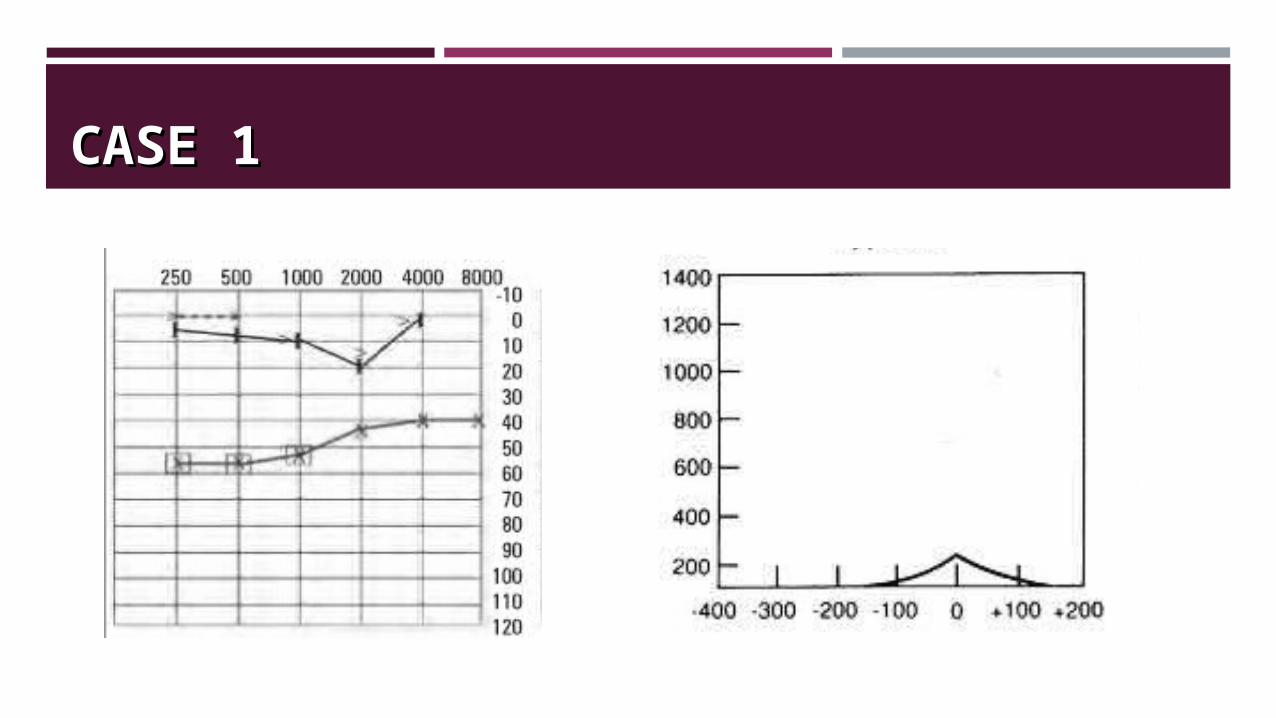
CASE 1CASE 1
OTOSCLEROSISOTOSCLEROSIS
Fusion of stapes footplate to oval window so that it cannot vibrate.
Etiology autosomal dominant female> male, progresses during pregnancy (hormone responsive)
Symptoms include slowly progressive hearing loss,bilateral in 70% of cases.
Vertigo is uncommon. Tinnitus may be present and often resolves after successful
surgical management
OTOSCLEROSISOTOSCLEROSIS
Conductive hearing loss
In 80-90% of patients, lesions are limited to the anterior oval window and affect its pathology by involving the stapes
sensorineural hearing loss
In 8% of patients, the process involves the cochlea and parts of the labyrinth (labyrinthine otosclerosis)
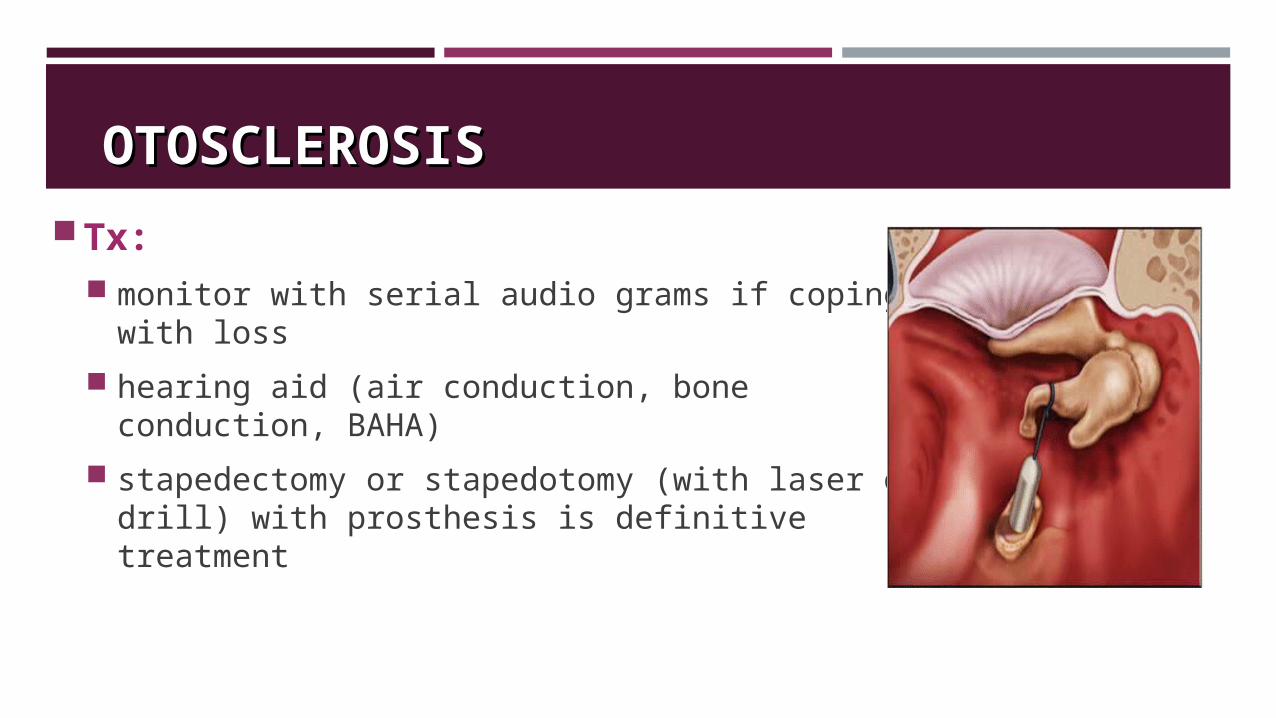
OTOSCLEROSISOTOSCLEROSIS
Tx: monitor with serial audio grams if coping with loss
hearing aid (air conduction, bone conduction, BAHA)
stapedectomy or stapedotomy (with laser or drill) with prosthesis is definitive treatment
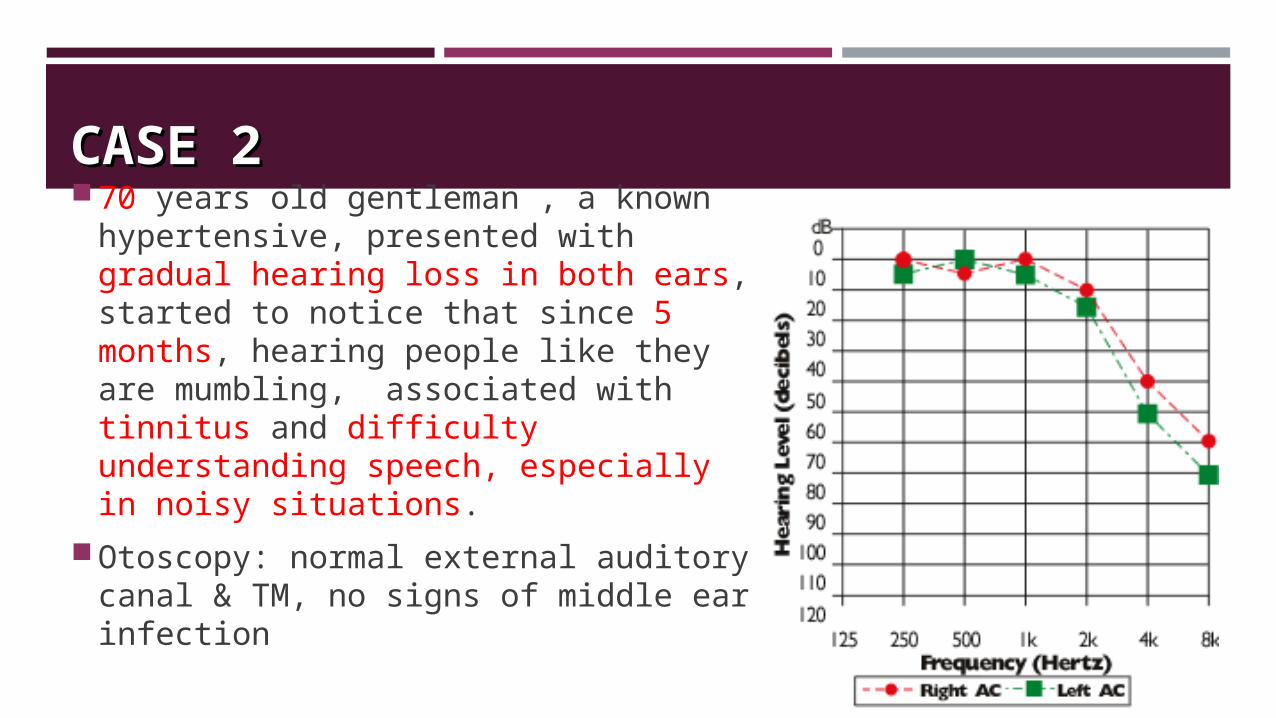
CASE 2CASE 270 years old gentleman , a known
hypertensive, presented with gradual hearing loss in both ears, started to notice that since 5 months, hearing people like they are mumbling, associated with tinnitus and difficulty understanding speech, especially in noisy situations.
Otoscopy: normal external auditory canal & TM, no signs of middle ear infection
PRESBYCUSISPRESBYCUSIS
Sensorineural hearing loss associated with aging (staging in 5th and 6th decades).
Etiology hair cell degeneration
age related degeneration of basilar membrane
cochlear neuron damage
ischemia of inner ear
Accumulated exposure to noise
Drug and environmental chemical exposure
Stress
Genetics
Arteriosclerosis
Diet and metabolism
CAUSESCAUSES
The inability to hear or understand speech in a crowded or noisy environment
Difficulty understanding consonants
The inability to hear high pitched voices or noises
Tinnitus is often present
COMMON COMPLAINTSCOMMON COMPLAINTS
Tx: hearing aid if patient has difficulty functioning, hearing loss >30-
35 dB, and good speech discrimination
±lip reading, auditory training, auditory aids (doorbell and phone lights)
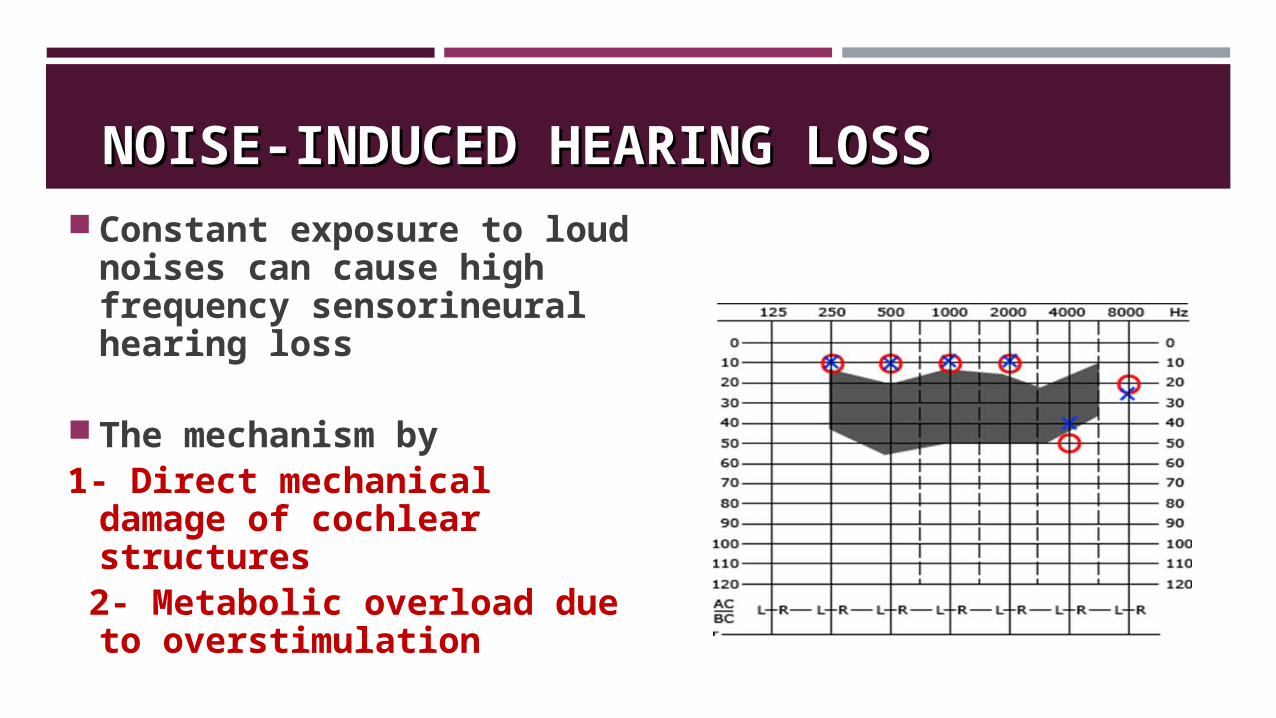
NOISE-INDUCED HEARING LOSSNOISE-INDUCED HEARING LOSS Constant exposure to loud
noises can cause high frequency sensorineural hearing loss
The mechanism by 1- Direct mechanical
damage of cochlear structures
2- Metabolic overload due to overstimulation
OTOTOXICITYOTOTOXICITY
Antibiotics
1-Aminoglycosides (gentamicin > tobramycin > amikacin > neomycin)
2-Erythromycin and tetracycline
Chemotherapeutic agents are known to cause hearing loss. The worst ototoxicity occurs with cisplatin.
High-dose aspirin.
Antimalarial medications such as quinine and chloroquine
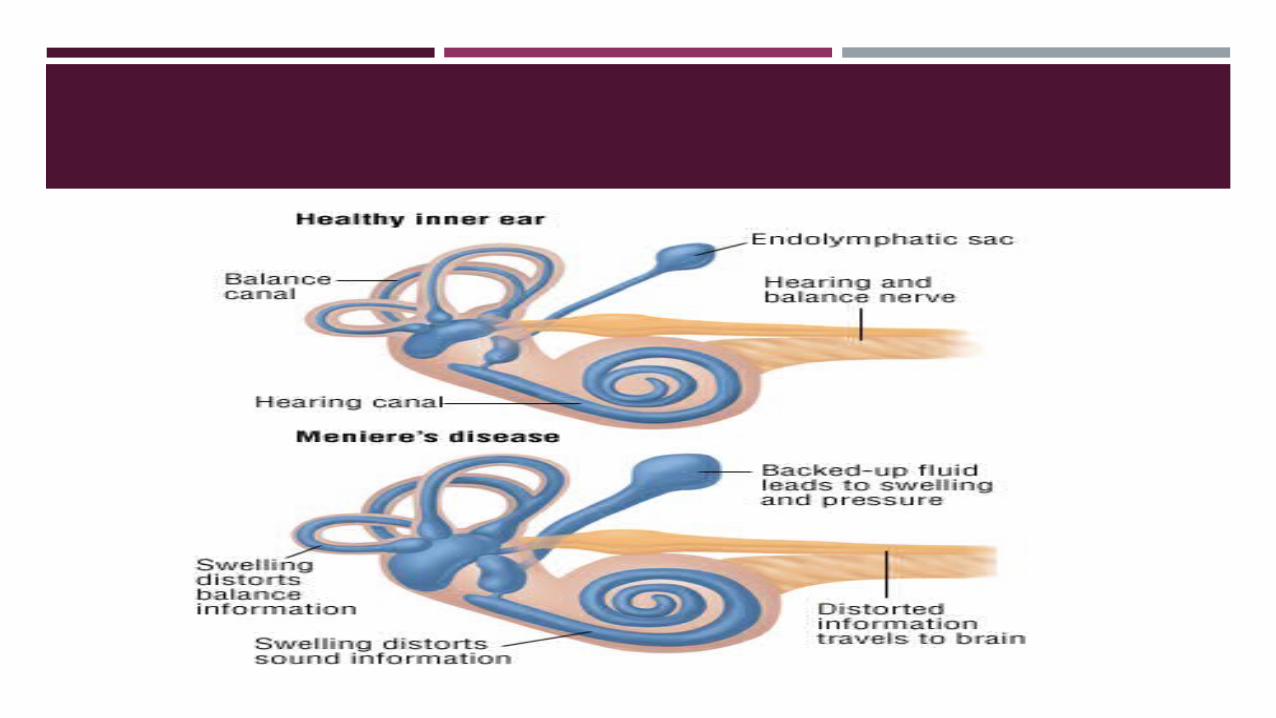
MÉNIÈRE DISEASEMÉNIÈRE DISEASE
Endolymphatic hydrops refers to a condition of increased hydraulic pressure within the inner ear endolymphatic system.
Episodic attacks of tinnitus, hearing loss, aural fullness, and vertigo lasting minutes to hours.
peak incidence 40 to 60 years
Acute management:: Bed rest, antiemetics, antivertiginous drugs [e.g. betahistine].
Long term management may include: Medical:Medical:
low salt diet, Local application of gentamicin, betahistine
Surgical. Surgical. Decompressing the inner ear ( draining the endolymphatic sac) Vestibular neurectomy Labyrinthectomy
SUMMARYSUMMARY
Patients with hearing loss may have conductive, sensorineural, or mixed hearing loss.
Patients with hearing loss should undergo a directed history and examination.
Weber and Rinne tests to distinguish conductive from sensorineural hearing loss
Patients with conductive hearing loss should undergo physical examination of the auricle and external auditory canal (EAC) looking for evidence of blockage to explain the hearing loss.
Patients without an obvious etiology for hearing loss (such as external otitis or cerumen impaction) should undergo formal audiologic testing.
SUMMARYSUMMARY
Otoscelerosis is the second most common cause of conductive hearing loss in 15-50 years olds (eftar cerumen impation).
Presbycusis is the most common cause of SNHL
Short exposure to louder sounds can cause significant SNHL
Features of Ménière disease; tinnitus, hearing loss, aural fullness, and vertigo
QUIZQUIZ
Q.With negatives Renne’s test on the right side and Weber’s test lateralized to the right ear could be suffering from:
Bilateral chronic suppuratiove otitis media
Right CSOM
Bilateral otosclerosis
Right secretory otitis media and left Eustachian tube dysfunction
Left CSOM only
Q.A progressing conductive hearing loss in an adult with a normal appearing, mobile tympanic membrane is most likely due to:
a. serous otitis media
b. otosclerosis
c. acute otitis media
d. external otitis media
Q.Most common cause of conductive hearing loss in children:
C.S.O.M.
Acute O.M.
Chronie recurrent S.O.M
Otitis externa.
Q. Meniere's syndrome is a symptom complex characterized by:
a) conductive hearing loss and tinnitus.b) fluctuating Sensorineural hearing loss, tinnitus, and
constant vertigo.c) intermittent vertigo lasting several days each time.d) fluctuating Sensorineural hearing loss, vertiginous
episodes lasting 1-2 hours, and tinnitus.e) vertigo precipitated by lying down and turning over
to one side.
REFERENCESREFERENCES
Ear, nose and throat and head and neck surgery, R. S. Dhillon, C.A East, third edition.
Otolaryngology- head and neck surgery, Toronto notes 2011
http://www.ncbi.nlm.nih.gov
http://www.uptodate.com