Embed Size (px)
Citation preview

Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Chapter 17 Heart
Purkinje fibers

Functions of the Heart
1. Generating blood pressure• Required for blood flow through the blood
vessels
2. Routing blood• Two pumps, moving blood through the
pulmonary and systemic circulations
3. Regulating blood supply• Adjusts blood flow by changing the rate and
force of heart contractions as needed

Systemic and Pulmonary Circulation
• Pulmonary circulation– The flow of blood from
the heart through the lungs back to the heart
– Picks up oxygen and releases carbon dioxide in the lungs
• System circulation– The flow of blood from
the heart through the body back to the heart
– Delivers oxygen and picks up carbon dioxide in the body’s tissues
Fig. 17.1

Location, Shape, and Size of the Heart
• Location– Anterior to the vertebral column, posterior to
the sternum– Left of the midline– Deep to the second to fifth intercostal spaces– Superior surface of diaphragm
• Shaped like a blunt cone, with an apex and a base
• Approximately the size of your fist

Fig. 17.2

Anatomy of the Heart
• The heart consists of two atria and two ventricles
• Pericardium: a double-walled sac around the heart composed of– A superficial fibrous pericardium– A deep two-layer serous pericardium
• The parietal layer lines the internal surface of the fibrous pericardium
• The visceral layer lines the surface of the heart• They are separated by the fluid-filled (pericardial
fluid) pericardial cavity

Anatomy of the Heart
• The pericardium– Fibrous pericardium
• Protects and anchors the heart• Prevents overfilling of the heart with blood
– Serous pericardium• Allows for the heart to work in a relatively friction-
free environment

Heart in the Pericardium
Fig. 17.3

Anatomy of the Heart
• The heart wall has three layers– Epicardium
• Visceral layer of the serous pericardium (visceral pericardium)• Provides protection against the friction of rubbing organs
– Myocardium• Cardiac muscle layer forming the bulk of the heart• Responsible for contraction
– Endocardium• Endothelial layer over crisscrossing, interlacing layer of
connective tissue• Inner endocardium reduces the friction resulting from the
passage of blood through the heart
• Ventricles have ridges called trabeculae carneae• The inner surfaces of the atria are mainly smooth
– Auricles have raised areas called musculi pectinati

Heart Wall
Fig. 17.4

Anatomy of the Heart
• Atria– Receiving chambers of the heart– Each atrium has a protruding auricle– Pectinate muscles mark atrial walls– Veins entering the right atrium carry blood to the heart
from the systemic circulation• Inferior vena cava• Superior vena cava• Coronary sinus
– Veins entering the left atrium carry blood to the heart from the pulmonary circulation
• Four pulmonary veins

Anatomy of the Heart
• Ventricles– Discharging chambers of the heart– Papillary muscles and trabeculae carneae
muscles mark ventricular walls– Arteries carrying blood away from the heart
• Pulmonary trunk exits the right ventricle carrying blood to the pulmonary circulation
• Aorta exits the left ventricle carrying blood to the systemic circulation

Anatomy of the Heart
• External Anatomy– Each atrium has a flap called an auricle– The coronary sulcus separates the atria from the
ventricles– The interventricular grooves separate the right and left
ventricles
• Heart Chambers– The interatrial septum separates the atria from each
other– The fossa ovalis is the former location of the foramen
ovalis through which blood bypassed the lungs in the fetus
– The interventricular septum separates the ventricles

Fig. 17.5ab
Surface View of
the Heart

Surface View of the Heart
Fig. 17.5c

Anatomy of the Heart
• Heart valves– Ensure unidirectional blood flow through the heart– Atrioventricular (AV) valves lie between the atria and
the ventricles– AV valves prevent backflow into the atria when
ventricles contract– Chordae tendineae anchor AV valves to papillary
muscles– Tricuspid valve: separates the right atrium and
ventricle– Bicuspid valve: separates the left atrium and ventricle

Anatomy of the Heart
• Heart valves (cont.)– Semilunar valves prevent backflow of blood
into the ventricles– Aortic semilunar valve: lies between the left
ventricle and the aorta – Pulmonary semilunar valve: lies between the
right ventricle and pulmonary trunk

Internal Anatomy of the Heart
Fig. 17.6

Heart Valves
Fig. 17.7

Function of the Heart Valves
Fig. 17.8

Route of Blood Flow Through the Heart
• Blood from the body flows through the right atrium into the right ventricle and then to the lungs
• Blood returns from the lungs to the left atrium, enters the left ventricle, and is pumped back to the body

Fig. 17.9
Blood Flow
Through the Heart

Blood Supply to the Heart
• Coronary arteries branch off the aorta to supply the heart
• Blood returns from the heart tissues to the right atrium through coronary sinus and cardiac veins
Fig. 17.10

Page 497

Histology of the Heart
• Fibrous Skeleton of the Heart– Consists of a plate of fibrous connective
tissue– Forms fibrous rings around the AV and SL
valves for support– Provides a point of attachment for heart
muscle– Electrically insulates the atria from the
ventricles

Histology of the Heart
• Cardiac Muscle Cells– Are branched and have a centrally located nucleus– Actin and myosin are organized to form sarcomeres
(striated)– T tubules and sarcoplasmic reticulum are not as
organized as in skeletal muscle– Normal contraction depends on extracellular Ca2+
– Rely on aerobic respiration for ATP production• They have many mitochondria and are well supplied with blood
vessels
– Joined by intercalated disks• Allow action potentials to move from one cell to the next, thus
cardiac muscle cells function as a unit

Histology of the Heart
Fig. 17.11


Electrical Activity of the Heart
• Action Potentials 1. After depolarization and partial repolarization, a
plateau phase is reached, during which the membrane potential only slowly repolarizes
2. The opening and closing of voltage-gated ion channels produce the action potential • The movement of Na+ through Na+ channels causes
depolarization • During depolarization, K+ channels close and Ca2+ channels
begin to open • Early repolarization results from closure of the Na+ channels
and the opening of some K+ channels • The plateau exists because Ca2+ channels remain open • The rapid phase of repolarization results from the closure of
the Ca2+ channels and the opening of many K+ channels

Electrical Activity of the Heart
• Refractory Periods – Absolute refractory period
• Cardiac muscle cells are insensitive to further stimulation
– Relative refractory period• Stronger than normal stimulation can produce an action
potential
– Cardiac muscle has a prolonged depolarization and thus a prolonged absolute refractory period, which allows time for the cardiac muscle to relax before the next action potential causes a contraction

Fig. 17.12


Electrical Activity of the Heart
• Autorhythmicity of Cardiac Muscle– Some cardiac muscle cells are autorhythmic because
of the spontaneous development of a prepotential• Prepotential: slowly developing local action potential
– The sinoatrial (SA) node is the pacemaker of the heart
• Collection of cardiac muscle cells capable of spontaneously generating action potentials
– The prepotential results from the movement of Na+ and Ca2+ into the SA node cells
– The duration of the prepotential determines heart rate

Electrical Activity of the Heart
• Conducting System of the Heart– The sinoatrial (SA) node and the
atrioventricular (AV) node are in the right atrium
– The AV node is connected to the bundle branches in the interventricular septum by the AV bundle
– The bundle branches give rise to Purkinje fibers, which supply the ventricles

Electrical Activity of the Heart
• Conducting System of the Heart– The SA node initiates action potentials, which spread
across the atria and cause them to contract• SA node generates impulses about 75 times/minute
– Action potentials are slowed in the AV node, allowing the atria to contract and blood to move into the ventricles
• AV node delays the impulse approximately 0.11 seconds
– Then the action potentials passes from atria to ventricles via the atrioventricular bundle


Electrical Activity of the Heart
• Conducting System of the Heart– AV bundle splits into two pathways in the
interventricular septum (bundle branches)– Bundle branches carry the impulse toward the
apex of the heart– Purkinje fibers carry the impulse to the heart
apex and ventricular walls

Fig. 17.13


Electrical Activity of the Heart
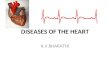
• Electrocardiogram (ECG)– Records only the electrical activities of the heart– P wave corresponds to depolarization of the atria (SA
node)– QRS complex corresponds to ventricular
depolarization– T wave corresponds to ventricular repolarization– Atrial repolarization record is masked by the larger
QRS complex
• Based on the magnitude of the ECG waves and the time between waves, ECGs can be used to diagnose heart abnormalities

Fig. 17.14

Cardiac Cycle
• Repetitive contraction and relaxation of the heart chambers
• Overview of Systole and Diastole • Atrial systole is contraction of the atria• Systole is contraction of the ventricles• Atrial diastole is relaxation of the atria• Diastole is relaxation of the ventricles

Cardiac Cycle
• Overview of Systole and Diastole (cont.)– During systole
• AV valves close• Pressure increases in the ventricles• Semilunar valves are forced to open• Blood flows into the aorta and pulmonary trunk
– At the beginning of diastole• Pressure in the ventricles decreases• Semilunar valves close to prevent backflow of blood from the
aorta and pulmonary trunk into the ventricles– When the pressure in the ventricles is lower than in
the atria, the AV valves open and blood flows from the atria into the ventricles
– During atrial systole, the atria contract and complete the filling of the ventricles

Fig. 17.15
Cardiac Cycle

Cardiac Cycle
• Events Occurring During Ventricular Systole – Ventricular depolarization
• Produces the QRS complex• Initiates contraction of the ventricles, which increases
ventricular pressure– The AV valves close
– Semilunar valves open
– Blood is ejected from the heart
– The volume of blood in a ventricle just before it contracts is the end- diastolic volume
– The volume of blood after contraction is the end- systolic volume

Cardiac Cycle
• Events Occurring During Ventricular Diastole
– Ventricular repolarization• Produces the T wave • Ventricles relax
– Blood flowing back toward the relaxed ventricles closes the semilunar valves
– The AV valves open and blood flows into the ventricles
• Approximately 70% of ventricular filling occurs when blood flows from the higher pressure in the veins and atria to the lower pressure in the relaxed ventricles
• Atrial depolarization produces the P wave• The atria contract and complete ventricular filling

Cardiac Cycle
• Aortic Pressure Curve– Contraction of the ventricles forces blood into
the aorta• The maximum pressure in the aorta is the systolic
pressure
– Elastic recoil of the aorta maintains pressure in the aorta and produces the dicrotic notch
– Blood pressure in the aorta falls as blood flows out of the aorta
• The minimum pressure in the aorta is the diastolic pressure

Cardiac Cycle
• Heart sounds (lub-dup) are associated with closing of heart valves– First sound occurs as AV valves close and
signifies beginning of systole– Second sound occurs when SL valves close
at the beginning of ventricular diastole

Fig. 17.17

Fig. 17.16
Events Occurring
During the
Cardiac Cycle

Tab. 17.2

Tab. 17.1


Mean Arterial Blood Pressure
• Mean arterial pressure is the average blood pressure in the aorta– Adequate blood pressure is necessary to
ensure delivery of blood to the tissues – Proportional to cardiac output (amount of
blood pumped by the heart per minute) times peripheral resistance (total resistance to blood flow through blood vessels)
– CO X PR

Mean Arterial Blood Pressure
• CO is the product of heart rate (HR) and stroke volume (SV)– HR is the number of heart beats per minute– SV is the amount of blood pumped out by a ventricle
with each beat• SV = end-diastolic volume (EDV) minus end-systolic
volume (ESV)– EDV = amount of blood collected in a ventricle during diastole– ESV = amount of blood remaining in a ventricle after
contraction
– CO (ml/min) = HR (72 beats/min) x SV (70 ml/beat)– CO = 5040 ml/min (~5 L/min)
• Cardiac reserve is the difference between resting and maximal CO

Mean Arterial Blood Pressure
• Venous return is the amount of blood returning to the heart
– Increased venous return increases stroke volume by increasing end-diastolic volume
• Increased force of contraction increases stroke volume by decreasing end-systolic volume

Regulation of the Heart
• Intrinsic Regulation– Modifies stroke volume through the functional
characteristics of cardiac muscle cells– Starling’s law of the heart describes the
relationship between preload and the stroke volume of the heart
• An increased preload causes the cardiac muscle fibers to contract with a greater force and produce a greater stroke volume
– Afterload is the pressure against which the ventricles must pump blood.

Regulation of the Heart
• Extrinsic Regulation – Modifies heart rate and stroke volume through
nervous and hormonal mechanisms• The cardioregulatory center in the medulla
oblongata regulates the parasympathetic and sympathetic nervous control of the heart
• Epinephrine and norepinephrine are released into the blood from the adrenal medulla as a result of sympathetic stimulation. They increase the rate and force of heart contraction

Regulation of the Heart
• Parasympathetic stimulation is supplied by the vagus nerve– Decreases heart rate. – Postganglionic neurons secrete acetylcholine, which
increases membrane permeability to K. Hyperpolarization of the plasma membrane increases the duration of the prepotential
• Sympathetic stimulation is supplied by the cardiac nerves – Increases heart rate and the force of contraction
(stroke volume) – Postganglionic neurons secrete norepinephrine,
which increases membrane permeability to Ca2+. Depolarization of the plasma membrane decreases the duration of the prepotential

The Heart and Homeostasis
• Effect of Blood Pressure – Baroreceptors monitor blood pressure and the
cardioregulatory center modifies heart rate and stroke volume
– In response to a decrease in blood pressure, the baroreceptor reflexes increase heart rate and stroke volume
– When blood pressure increases, the baroreceptor reflexes decrease heart rate and stroke volume



The Heart and Homeostasis
• Effect of pH, Carbon Dioxide, and Oxygen– Carotid body and aortic chemoreceptor
receptors monitor blood oxygen levels– Medullary chemoreceptors monitor blood pH
and carbon dioxide levels– Chemoreceptors are not important for the
normal regulation of the heart, but are important in the regulation of respiration and blood vessel constriction

Baroreceptor and Chemoreceptor Reflexes
Fig. 17.18

Fig. 17.19

The Heart and Homeostasis
• Effect of Ions and Body Temperature– Increased extracellular K+ decrease heart rate and
stroke volume– Decreased extracellular K+ decrease heart rate– Increased extracellular Ca2+ increase stroke volume
and decrease heap rate– Decreased extracellular Ca2+ levels produce the
opposite effect– Heart rate increases when body temperature
increases, and it decreases when body temperature decreases

Effects of Aging on the Heart
• Aging results in gradual changes in the function of the heart, which are minor under resting conditions but are more significant during exercise
• Some age-related changes to the heart are the following– Decreased cardiac output and heart rate– Increased cardiac arrhythmias– Hypertrophy of the left ventricle– Development of stenoses or incompetent valves– Development of coronary artery disease and heart
failure• Exercise improves the functional capacity of the
heart at all ages.