Embed Size (px)
Citation preview
Hemorrhoids:
A common condition and
Effective treatment optionsKevin J. Holzman, MD, FACS, FASCRS
1/15/2015
What are hemorrhoids?
• Alternative Names
• Rectal Lump
• Piles
• Lump in the Rectum
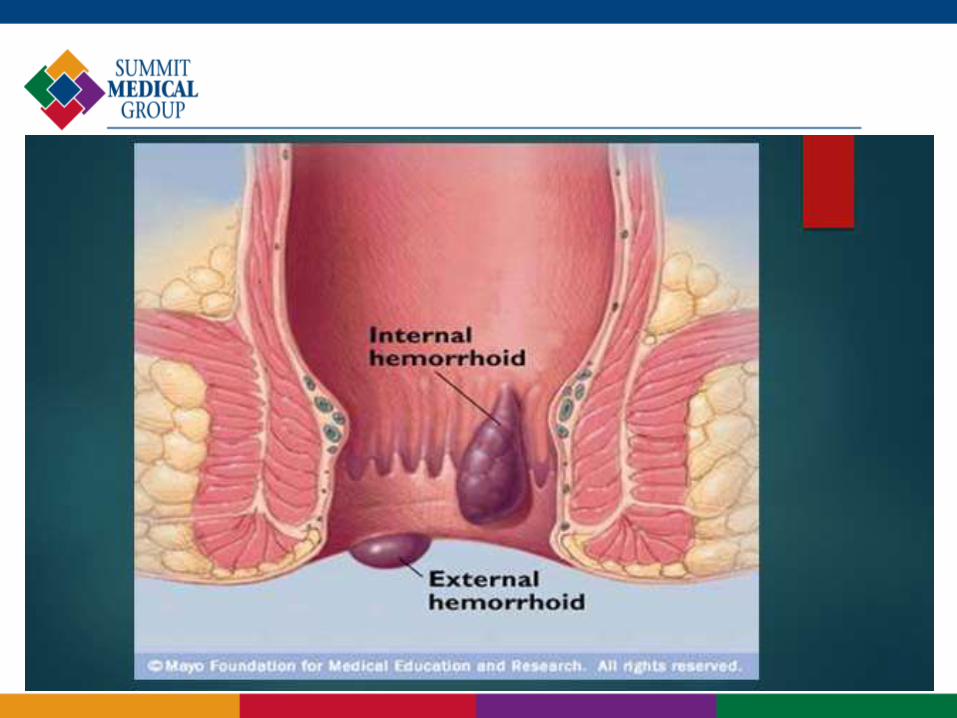
• Definition:
• Dilated or enlarged veins in the lower
portion of the rectum or anus.
Frequency
• 10 million
• Peak ages: 45-65 years
• ½ of adults experience hemorrhoids by
age 50
• Common among pregnant women
Anatomy
• Right anterior, Right posterior and Left lateral
positions
• Only 19% of the time
• Additional smaller accessory bundles between these
• Those originating above the dentate line which are
termed internal
• Those originating below the dentate line which are
termed external.

Pathophysiology
• Represent engorgement or enlargement of the normal
fibrovascular cushions lining the rectum and anal canal.
• Chronic straining secondary to constipation or occasionally
diarrhea
Trauma, inflammation
• Fibrovascular cushions lose their attachment to the underlying
rectal wall
prolapse
Pathophysiology
• Prolapse of internal hemorrhoidal tissue through the
anal canal.
• Overlying mucosa becomes more friable and the
vasculature increases
• With overlying thinning of the mucosa and vascular
engorgement, subsequent rectal bleeding occurs.
Classification
• Classified by history and not by physical examination.
• For INTERNAL hemorrhoids
• Grade I - bleeding without prolapse.
• Grade II - prolapse with spontaneous reduction.
• Grade III - prolapse with manual reduction.
• Grade IV - incarcerated, irreducible prolapse.
Symptoms
• Rectal Bleeding
• Bright red blood in stool
• Pain during bowel movements
• Anal Itching
• Difficult hygeine
• Rectal tissue Prolapse
• Leakage (mucus or stool)
• Thrombosis

Symptoms
• Bright red blood per rectum or a prolapsing anal mass.
• With, or following, bowel movements, is almost universally
bright red, and very commonly drips into the toilet water.
• Blood may also be seen while wiping after defecation.
Described as on “toilet tissue”
Symptoms
• Prolapse usually occurs in association with a bowel movement
• May also prolapse during walking or heavy lifting as a result of
increased intra-abdominal pressure.
Coughing, sneezing
obesity
• Extreme pain, bleeding and occasionally signs of systemic
illness in case of strangulation
rare

Causes
• Chronic trauma/inflammation
• Constipation
• Diarrhea
• Sitting or standing for long periods of time
• Obesity
• Heavy Lifting
• Pregnancy
• Aging
Physical exam
• Patients should be examined in the left lateral decubitus
position
Prone-jackknife
• Rule out any rashes, condylomata, fissures, lesions,
abscesses
• External sphincter function
• Rule out tumors
Physical exam
• What to expect
Visual inspection
Digital rectal exam
Small scope
Evaluation of rectal bleeding
• Rule out rectal cancer!!
• Young individual with bleeding associated with hemorrhoidal
disease and no other systemic symptoms, and no family history,
perhaps anoscopy and rigid sigmoidoscopy
• Older individual, with either a family history of colorectal cancer,
or change in bowel habits, a complete colonoscopy should be
performed to rule out proximal neoplasia.
Treatment options
• Varies from simple reassurance to operative hemorrhoidectomy.
• Treatments are classified into three categories:
• 1) Dietary and lifestyle modification.
• 2) Non operative/office procedures.
• 3) Operative hemorrhoidectomy.
• Many patients will require a combination
Dietary and lifestyle modification
• The main goal of this treatment is to minimize straining at stool.
• Achieved by increasing fluid and fiber in the diet, recommending
exercise, and perhaps adding fiber agents to the diet such as
psyllium or methycellulose
• If necessary, stool softeners may be added.
Miralax
• "you don't defecate in the library so you shouldn't read in the
bathroom".
Dietary
• Mild cases are controlled by: Preventing constipation
Drinking Fluids
High-fiber diet
Use of Fiber supplements
Stool softeners
Topicals
Fiber
• 20-30 grams/day
• Psyllium
Metamucil – 3.4g/teaspoon
Metamucil capules – 0.52g/capsule
Konsyl – 6.0g/teaspoon
• Methycellulose
Citrucel – 2.0g/dose
• Calcium polycarbophil
FiberCon – 0.5g/capsule
Fiber
• Insoluble
Does not dissolve in water
Bulks – helps with constipation
Whole grains, wheat cereals
• Soluble
Dissolves in water
Helps control blood sugar and reduce cholesterol
Barley, oat meal, beans, nuts
Nonsurgical
• Apply OTC cream or suppository containing
hydrocortisone
inflammation
• Keep anal area clean
• Soak in a warm bath
• Apply ice packs or compresses x 10min
Thrombosed hemorrhoid
Nonsurgical
• If prolapses, gently push back into anal canal
• Use a sitz bath with warm water
• Use moist towelettes or wet toilet paper
instead of dry toilet paper.
Many options
• For painful or persistant hemorrhoids:
Tying off a hemorrhoid-rubber band ligation
Sclerotherapy
Infrared Light
Laser Therapy
Freezing
Electrical Current
Surgery
Office Rubber Band Ligation
• Grade I or Grade II hemorrhoids and, in some
circumstances, Grade III hemorrhoids.
• Complications include bleeding, pain, thrombosis
• Successful in two thirds to three quarters of all
individuals with first and second degree hemorrhoids.
Office RBL
• Minor pain
• Resume usual activities immediately
• May have feeling of incomplete emptying
• No blood thinners
Office Infrared Coagulation
• Generates infrared radiation which coagulates tissue protein
and evaporates water from cells.
• Most beneficial in Grade I and small Grade II hemorrhoids.
Beneficial for patients on anticoagulants
• 3-4 applications per hemorrhoid/per session
More pain
More time consuming

Office BICAP (bipolar diathermy)
• It works, in theory, similar to photocoagulation
or to rubber banding.
• the probe must be left in place for ten
minutes.
• poor patient tolerance minimized the effect of
this procedure.
Office Sclerotherapy
• Injection of an irritating material into the submucosa
in order to decrease vascularity and increase fibrosis.
• Injecting agents have traditionally been phenol in oil,
sodium morrhuate, or quinine urea.
• Not when prolapse present
• Potential for stricture or scarring
Surgical hemorrhoidectomy
• Indications
Persistent itching
External disease
Anal bleeding
Pain
Blood clots
Infection
Patient wishes
Surgical hemorrhoidectomy
• Risks
Reactions to medications of anesthesia
Bleeding
Infection
Narrowing of the anus
• *The outcome is usually very good in the majority of
cases.
Options
• Excisional hemorrhoidectomy
• Single or multiple
• Transanal hemorrhoidal dearterialization
• With or without hemorrhoidopexy
Ultrasound guided
No excision of tissue
• Stapled hemorrhoidectomy - PPH

Prevention
• Eat high fiber diet
• Drink Plenty of Liquids
• Fiber Supplements
• Exercise
• Avoid long periods of standing or sitting
• Don’t Strain
• Go as soon as you feel the urge