Embed Size (px)
Citation preview

HERNIASURGERY
TONY 2010 MBBS
HERNIA
• PROTRUSION OF A VISCUS OR A PART OF VISCUS THROUGH A NORMAL OR ABNORMAL OPENING IN THE WALLS OF ITS CONTAINING CAVITY
TONY 2010 MBBS
HERNIA COMMONINGUINAL
INCISIONAL
FEMORAL
UMBILICAL
EPIGASTRIC
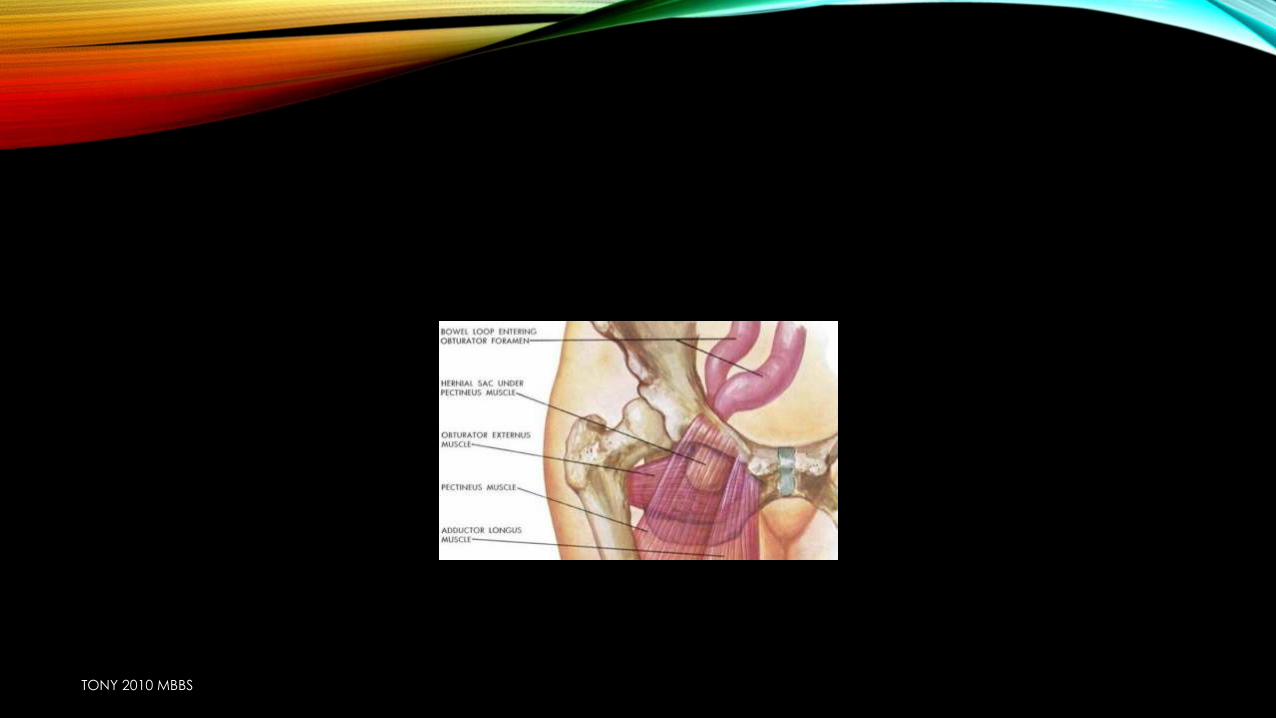
RAREOBTURATOR
SPIGELIAN
GLUTEAL
LUMBAR
DIAPHRAGMATIC
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS

HISTORY
TONY 2010 MBBS
HISTORY
• AGE :
YOUNG
• INDIRECT
OLD AGE (weak musculature)
•DIRECT
TONY 2010 MBBS
HISTORY
• OCCUPATION =STRENOUS
STRENOUS WORK
PERSISTENT PROCESSUS VAGINALIS
WEAK ABDOMINAL
WALL
HERNIATION
TONY 2010 MBBS
• SEX
• MOST COMMON HERNIA (BOTH IN MALES & FEMALES) INDIRECT
• FEMORAL HERNIA IS COMMON IN FEMALES
• DIRECT HERNIA IS ABSENT IN FEMALES & CHILDREN
TONY 2010 MBBS
IN FEMALES
PELVIS IS TILTED ANTERIORLY APEX & BASE OF HSSELBACH TRIANGLE AT THE SAME LEVEL
OBLITERATEDLESS CHANCE

PRESENTING COMPLAINTS
TONY 2010 MBBS
• ABOUT LUMP
• COMPLICATIONS
• ETIOLOGY (PRECIPITATING FACTORS)
TONY 2010 MBBS
LUMP
• 1. Duration
• 2. Onset: Suddenly/gradually
• 3. Site of start: • From groin to scrotum (hernia) • From scrotum to groin (hydrocele and varicocele)
• 4. Aggravating factors:• – On straining• – On standing• – On coughing
• 5. Relieving factors:• – By lying down• – Manuallybyhimself
• 6. Associated with pain: Usually painless
TONY 2010 MBBS
PRESENTING COMPLAINTS
LUMP
• Onset : coughing
lifting weight
• Site: groin scrotum} inguinal hernia
below groin crease & ascends above it} femoral hernia
• Size and extent:
congenital: reaches bottom of scrotum at its first
appearance itselfTHOUGH
CONGENITAL
CAN APPEAR AT
ANY AGE due to
preformed sac
TONY 2010 MBBS
PAIN
• PAIN= DRAGGING & ACHING TYPE
Appears b4 the swelling
Increase with time
Subsides when it is
fully formed
TONY 2010 MBBS

PAIN
Acute pain around
umbilicustenderness strangulation
Due to drag
on mesentry
TONY 2010 MBBS
PAIN
• In strangulation due to drag on mesentrypain all over the abdomen
TONY 2010 MBBS
HISTORY SUGGESTIVE OF COMPLICATIONS:
• Irreducibility,
• severe pain in the groin over the swelling and also
• colicky abdominal pain, abdominal distension, vomiting,
• constipation
TONY 2010 MBBS
acquired } small initially ↑ size gradually
• REDUCIBILITY
Reduces on lying down DIRECT
Does not reduce on lying down
INDIRECT
TONY 2010 MBBS
• SYMPTOMS OF OBSTRUCTION
COLICKY ABDOMINAL PAIN
VOMITING
•BILIOUS
•FAECAL (USUALLY)
ABDOMINAL DISTENSION
ABSOLUTE CONSTIPATION
TONY 2010 MBBS
PRECIPITATING FACTORS
• C/C COUGH=TB ,BA,C/C BRONCHITIS
• STRAINING IN
• CONSTIPATION
• FREQUENCY OF MICTURITION
• URGENCY OF BENIGN ENLARGEMENT OF PROSTATE
• PHIMOSIS
• PINHOLE MEATUS
• PENILE STRICTURES
TONY 2010 MBBS
OBSTRUCTION
PAST HISTORY
• TB BA
• PREVIOUS SURGERY
• Damage to ilioinguinal nerve weak abdominal wallDIRECT hernia
APPENDICECTOMY
• Same side
• Opposite sideRECURRENT HERNIA
TONY 2010 MBBS
FAMILY HISTORY
• CONNECTIVE TISSUE DISORDERS
TONY 2010 MBBS
PERSONAL HISTORY
• History of Smoking:
• Smoking leads to chronic bronchitis
• Collagen deficiency occurs in smokers.
TONY 2010 MBBS
LOCAL EXAMINATION
TONY 2010 MBBS

INSPECTION
TONY 2010 MBBS
INSPECTION
• Patient in standing position
• 1. Site
• 2. Size
• 3. Shape
• 4. Extent
• 5. Surface
• 6. Skin over the swelling
• 7. Visible peristalsis
• 8. Cough impulse
• 9. Draining lymph nodes
• 10. Penis
• 11. Urethral meatus
• 12. Opposite scrotum
TONY 2010 MBBS
INSPECTION
• EXPOSE 4M UMBILICUSMID THIGH
POSITION OF PATIENT
STANDING
Inguinal, lumbar, femoral,
epigastric, obturator, gluteal,
spigelian
SUPINE
TONY 2010 MBBS
SWELLING
shape spherical femoral
direct
pyriform indirect
TONY 2010 MBBS
POSITION & EXTENT
• Inguinal hernia above the inner part of inguinal ligament
Inguinal hernia
Congenital
(complete)
Extend in to scrotum
acquired
(funicular)
Stops above testis
TONY 2010 MBBS
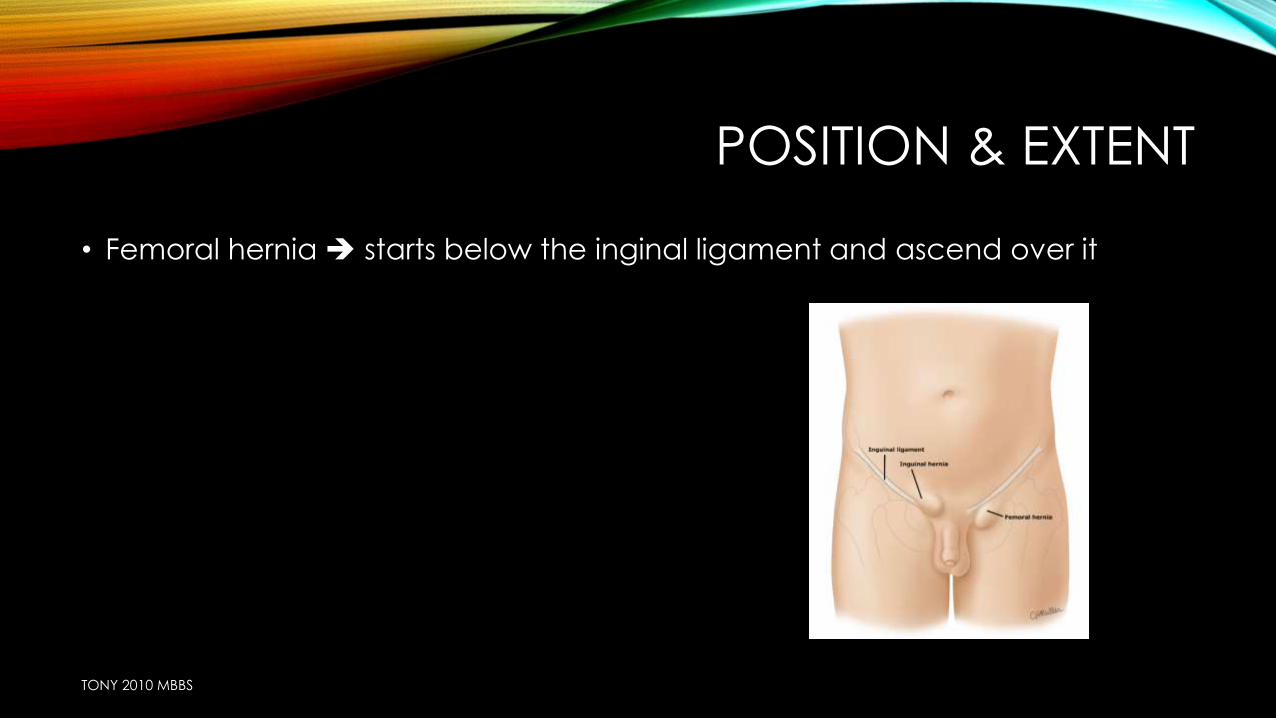
POSITION & EXTENT
• Femoral hernia starts below the inginal ligament and ascend over it
TONY 2010 MBBS
VISIBLE PERISTALSIS
• Invisible = femoral hernia
• Visible in case of inguinal hernia when skin is thin as in case of recurrent hernia
TONY 2010 MBBS
SKIN OVER THE SWELLING
• Uncomplicated=normal
• Strangulated=reddened
• Truss 4 long time=discolouration, due to deposition of hemosiderin
streaks,
• Scar=recurrence
• Wide irregular puckered=wound infectionrecurrence
TONY 2010 MBBS
IMPULSE ON COUGHING
• Characteristic of hernia
Impulse on coughing
present
Expansile impulse on coughing
(increase in size with coughing)
Momentary bulge synchronous with
coughing
absent obstructed
TONY 2010 MBBS
POSITION OF PENIS
• Deviation of penis to opposite side= in large complete inguinal hernia
TONY 2010 MBBS

PALPATION
TONY 2010 MBBS
PALPATION
• 1. Temperature
• 2. Tenderness
• 3. Site
• 4. Size
• 5. Shape
• 6. Extent
• 7. Surface
• 8. Skin over the swelling
• 9. Consistency
• 10. Reducibility
• 11. Get above the swelling
• 12. Cough impulse
• 13. Invagination test
• 14. Ring occlusion test
• 15. Zieman's technique.
TONY 2010 MBBS
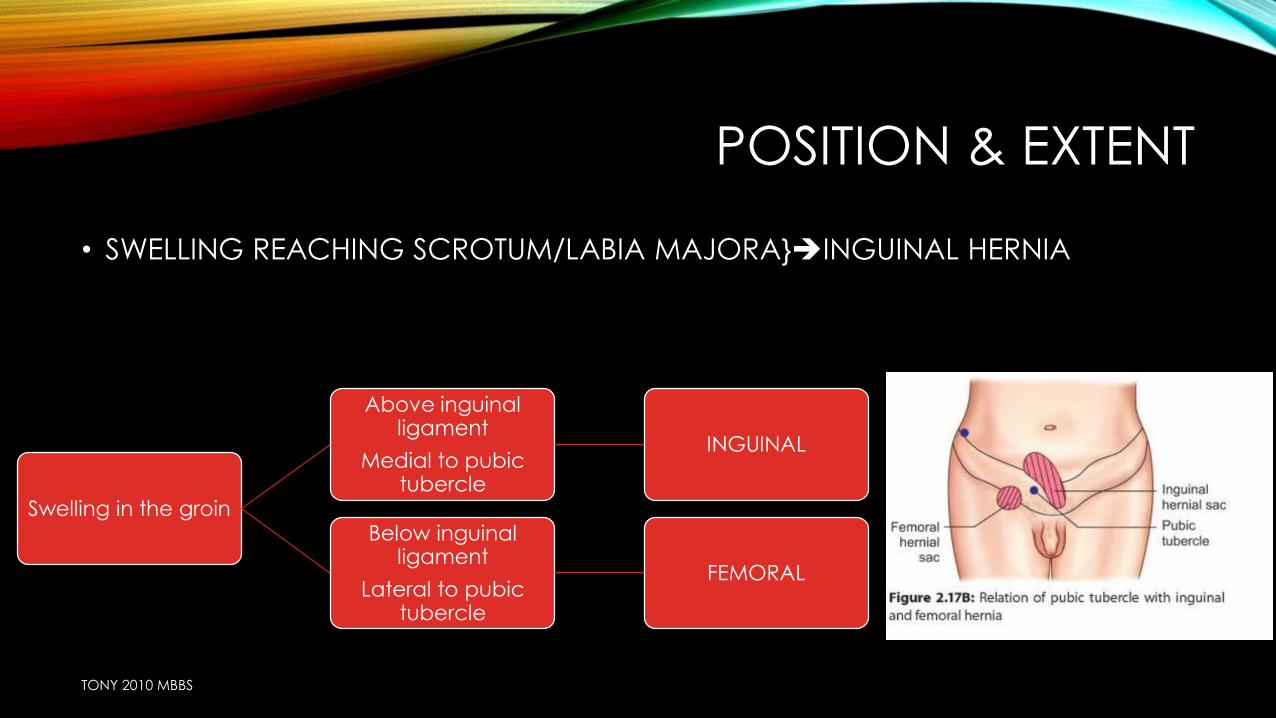
POSITION & EXTENT
• SWELLING REACHING SCROTUM/LABIA MAJORA}INGUINAL HERNIA
Swelling in the groin
Above inguinal ligament
Medial to pubic tubercle
INGUINAL
Below inguinal ligament
Lateral to pubic tubercle
FEMORAL
TONY 2010 MBBS
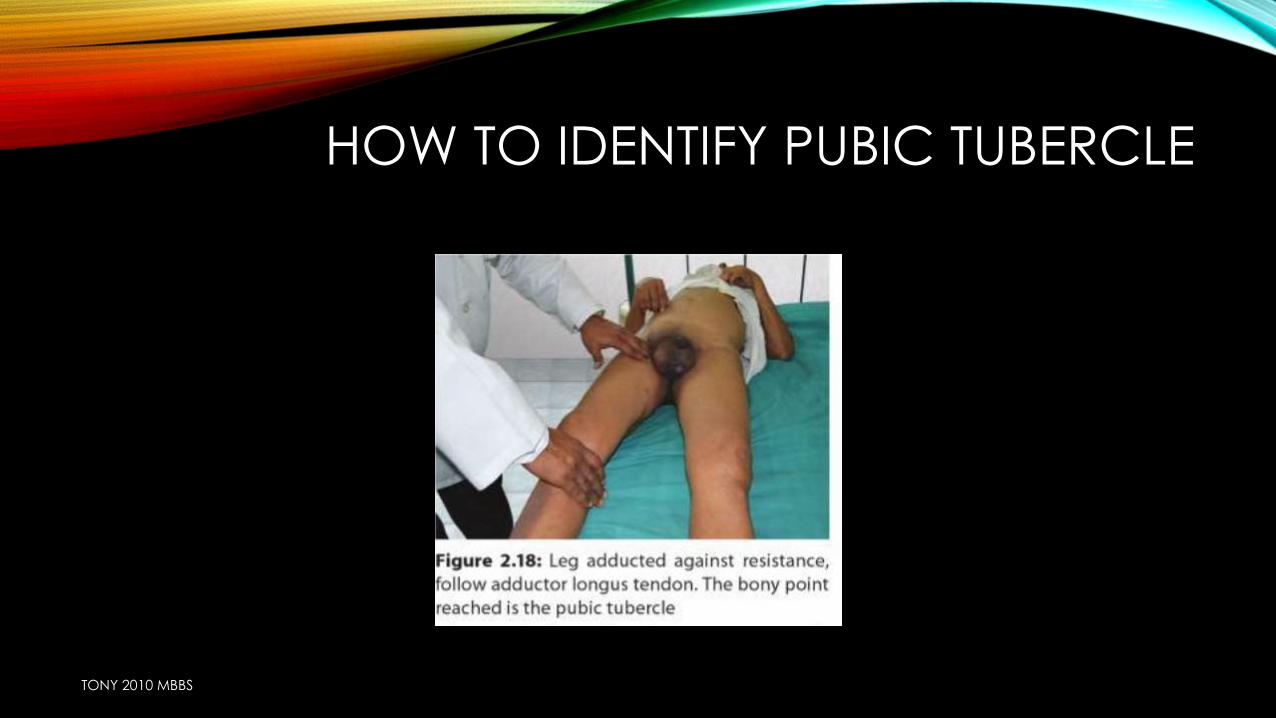
HOW TO IDENTIFY PUBIC TUBERCLE
TONY 2010 MBBS
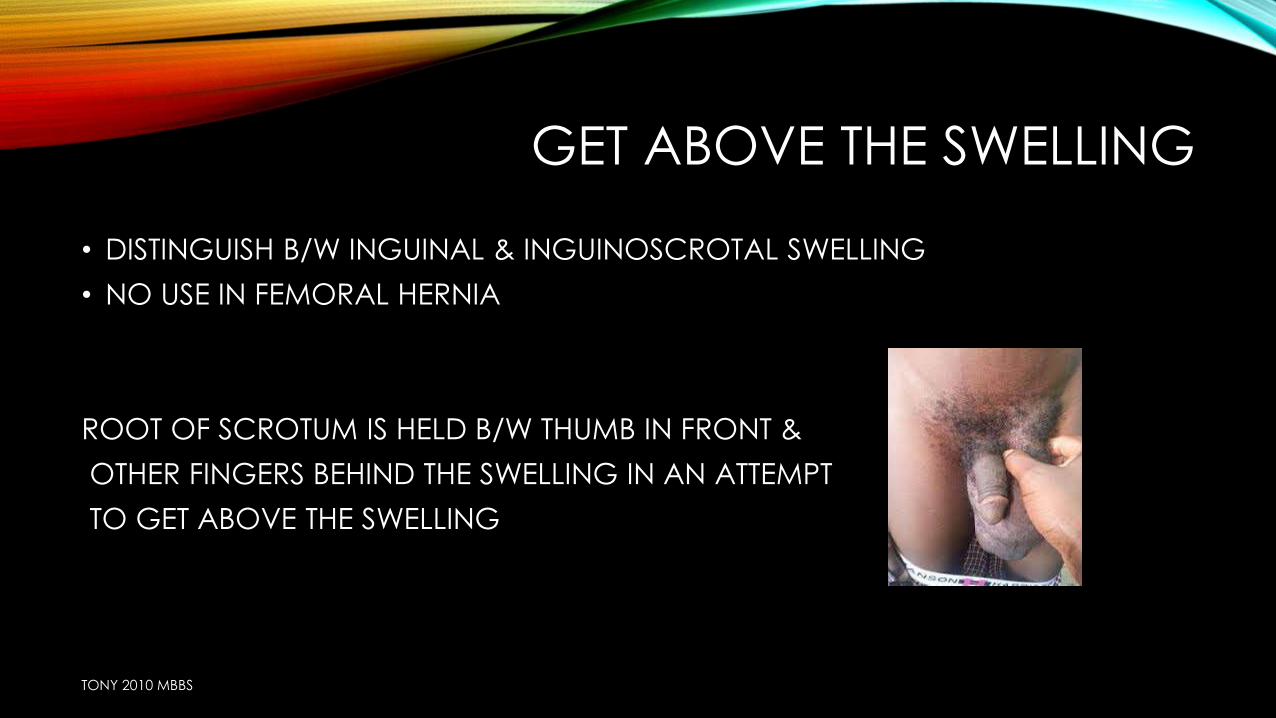
GET ABOVE THE SWELLING
• DISTINGUISH B/W INGUINAL & INGUINOSCROTAL SWELLING
• NO USE IN FEMORAL HERNIA
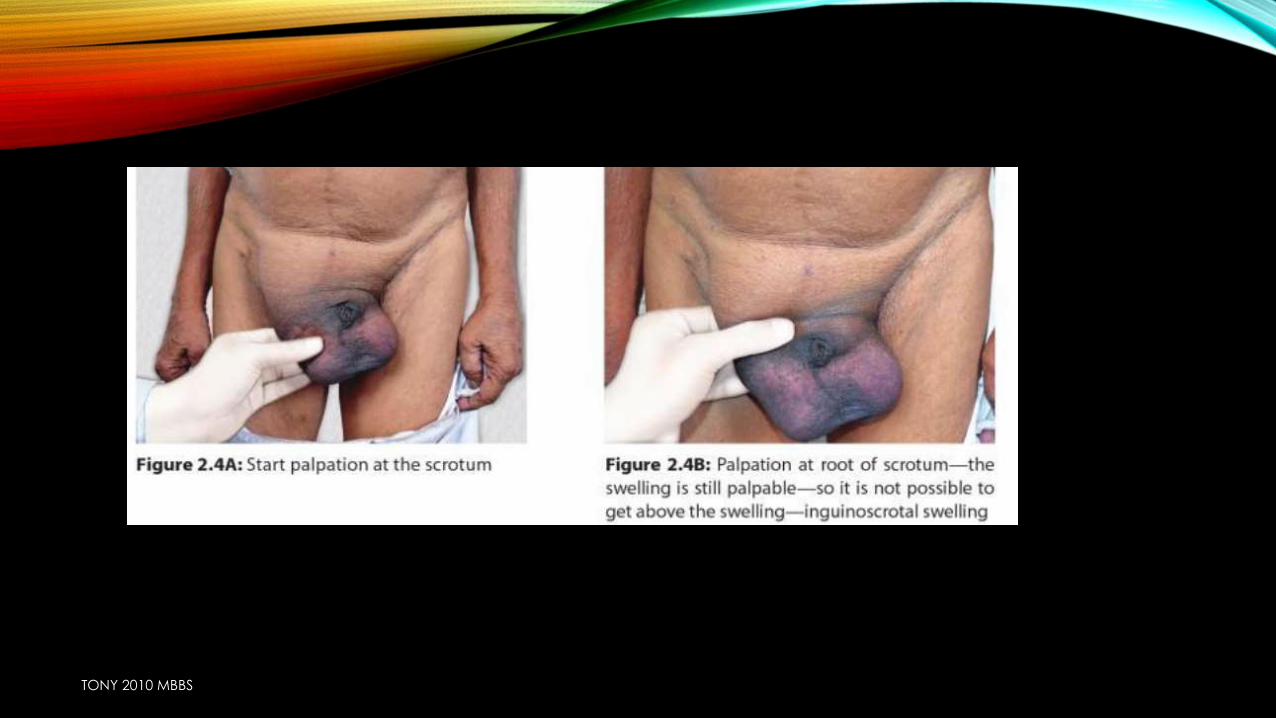
ROOT OF SCROTUM IS HELD B/W THUMB IN FRONT &
OTHER FINGERS BEHIND THE SWELLING IN AN ATTEMPT
TO GET ABOVE THE SWELLING
TONY 2010 MBBS
GET ABOVE THE SWELLING
INGUINAL HERNIA
• NOT ABLE TO GET ABOVE THE SWELLING
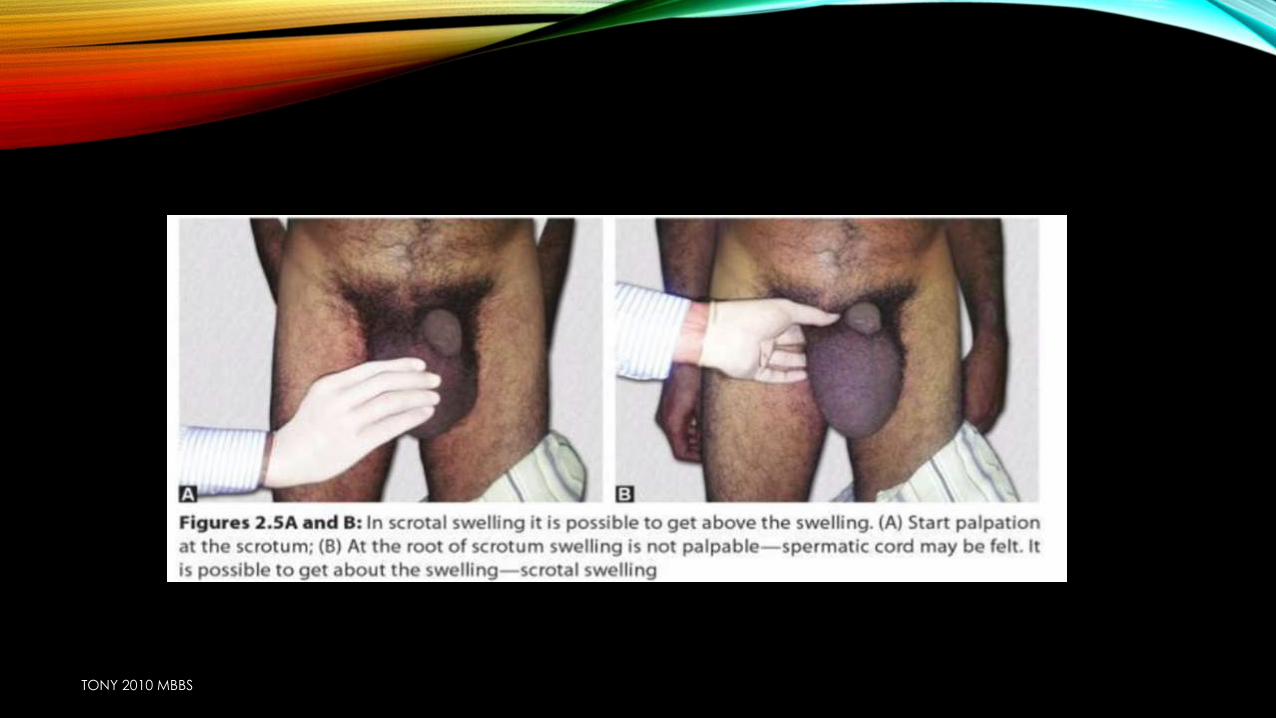
SCROTAL SWELLING
• ABLE TO GET SBOVE THE SWELLING
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
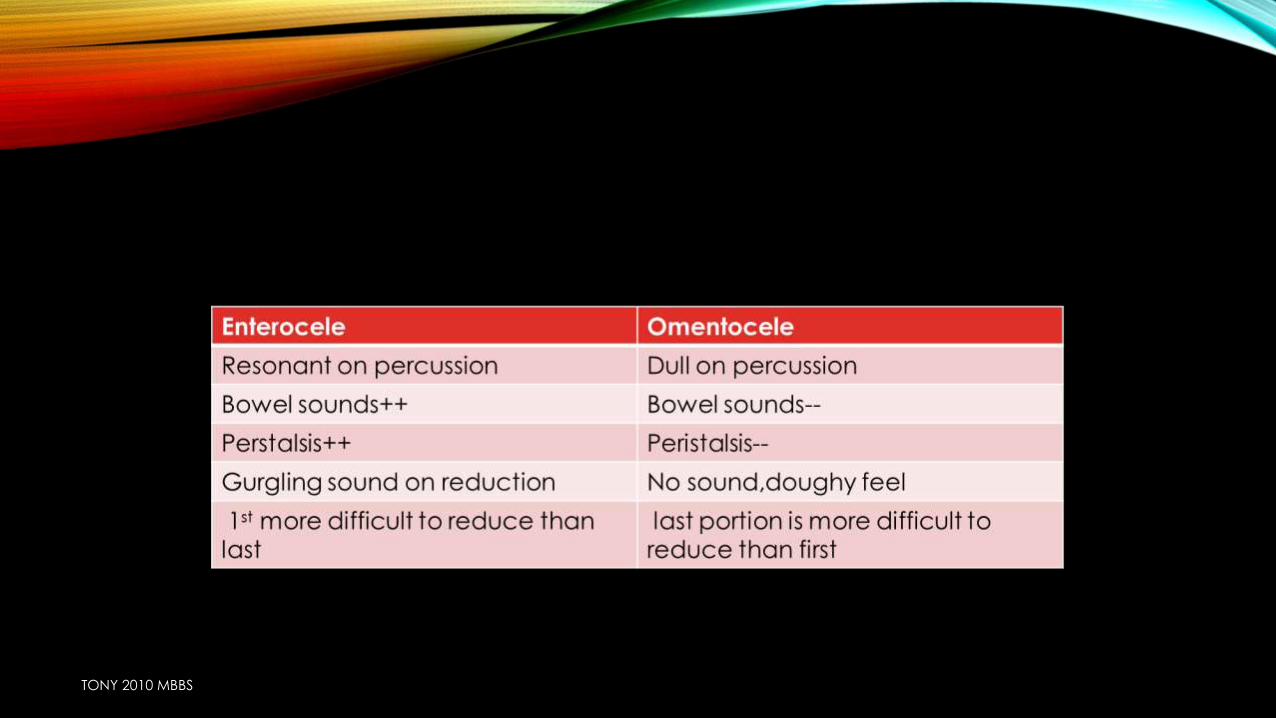
CONSISTENCY
• DOUGHY & GRANULAR} OMENTUM=OMENTOCELE
• ELASTIC} INTESTINE=ENTEROCELE
• TENSE & TENDER} STRANGULATED HERNIA
TONY 2010 MBBS
RELATION OF THE SWELLING TO THE TESTIS & SPERMATIC CORD
INGUINAL HERNIA
•Remains in front & sides of spermatc cord and testes which remains incorporated in front and sides
FUNICULAR
•Stops just above the testis
TONY 2010 MBBS

CLASSICAL SIGNS OF AN UNCOMPLICATED HERNIA
TONY 2010 MBBS
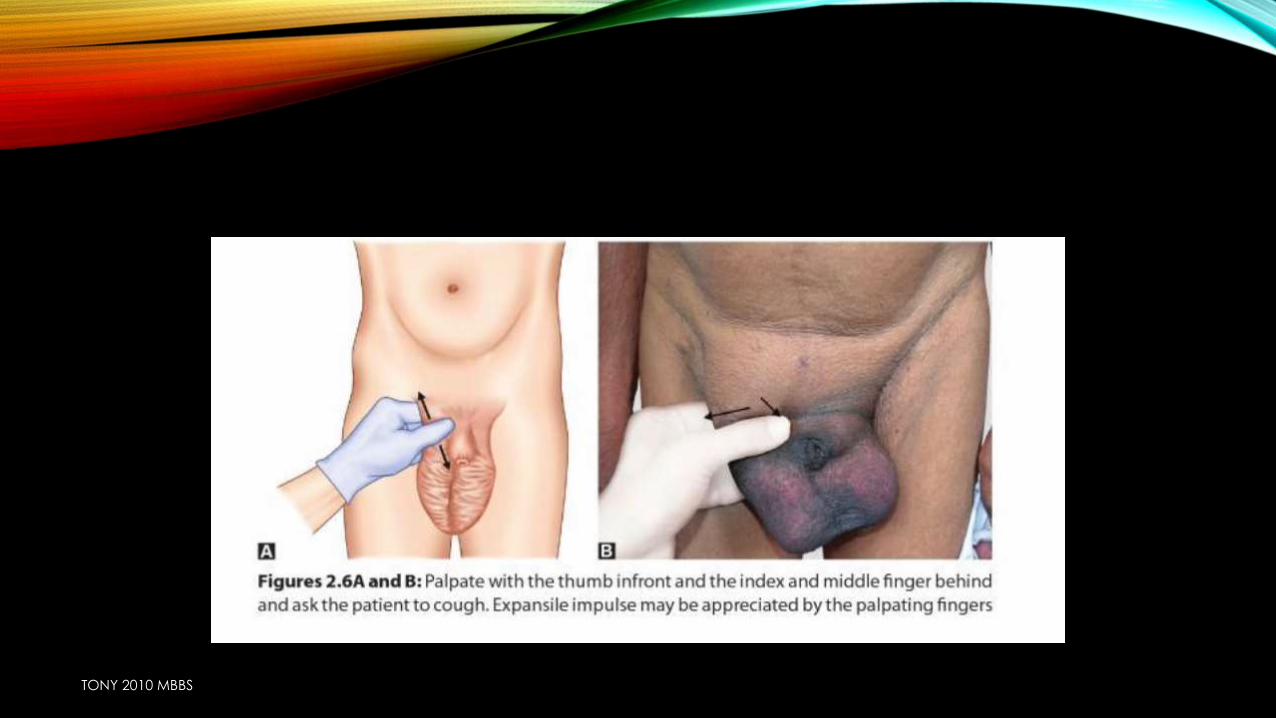
EXPANSILE IMPULSE ON COUGHING
• STANDING POSITION
• ABSENT IN CASE OF STRANGULATED & INCARCERATED HERNIA
1. MOMENTARY BULGE IN SUPERFICIAL RING ON COUGHUING
2. ROOT OF SCROTUM B/W INDEX FINGER & THUMB IS SEPARATED ON COUGHING
TONY 2010 MBBS
TONY 2010 MBBS
EXPANSILE IMPULSE IS ALSO PRESENT IN
• Meningocele
• Laryngocele
• Empyema necessitans
TONY 2010 MBBS
ZEIMANN’S TECHNIQUE
• Distinguish b/w direct, indirect or femoral hernia
• Can be used only when the swelling is completely reduce
when there is no visible swelling
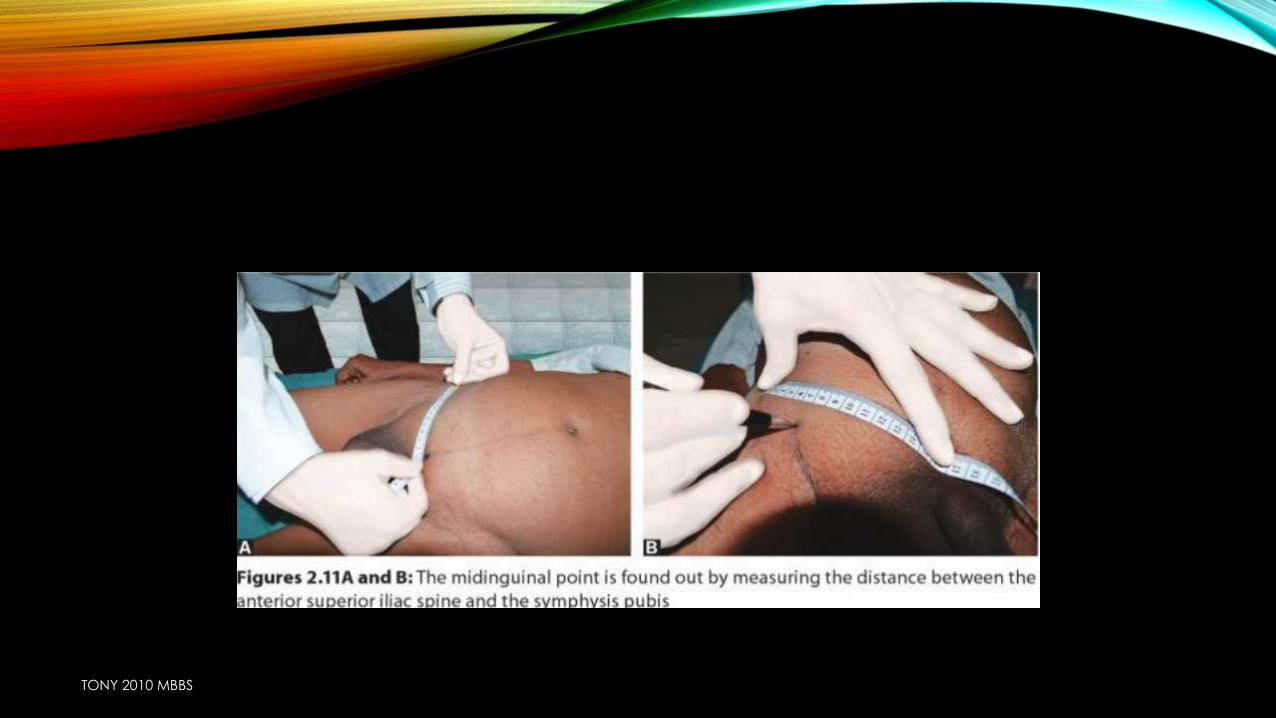
Index finger deep inguinal ring (1/2 “ above mid inguinal point)
Middle fingersuperficial inguinal ring (superomedial to pubic tubercle)
Ring finger saphenous opening (4cm blw & lateral 2 pubic tubercle)
Hold the nose & blow or cough
TONY 2010 MBBS
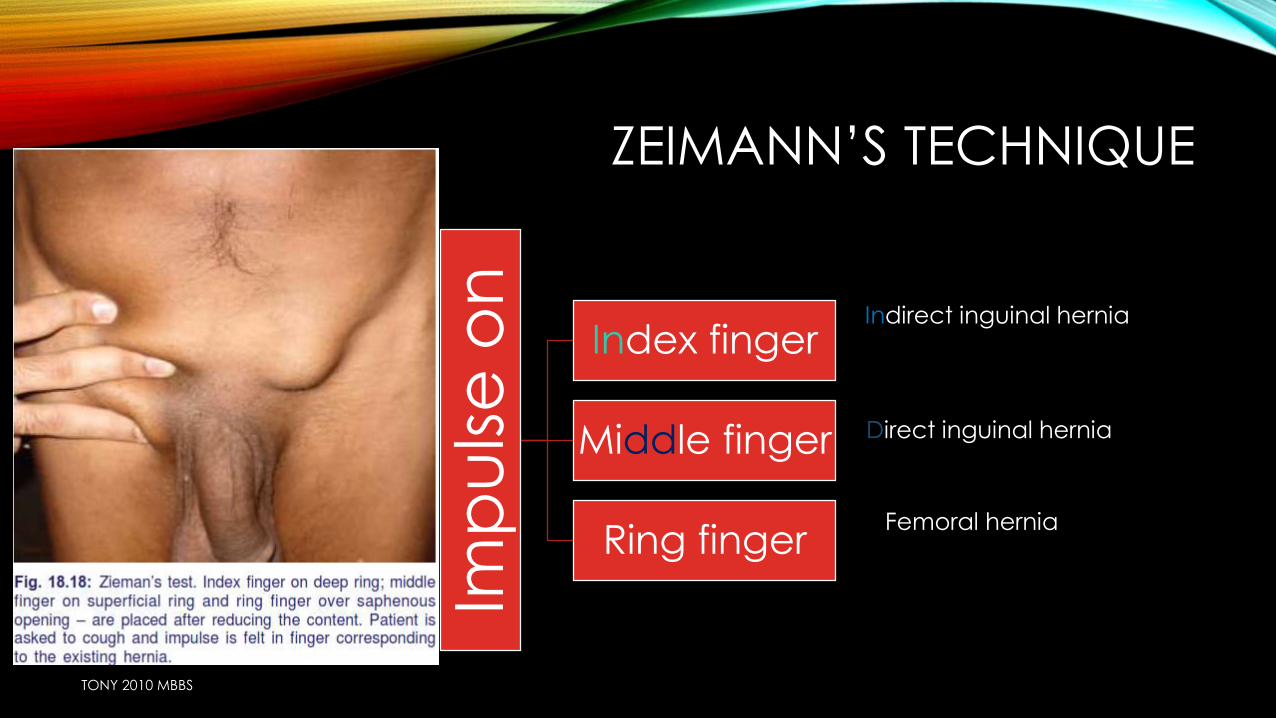
ZEIMANN’S TECHNIQUE
Imp
uls
e o
n
Index finger
Middle finger
Ring finger
Direct inguinal hernia
Indirect inguinal hernia
Femoral hernia
TONY 2010 MBBS
ZEIMANN’S TECHNIQUE
• In presence of swelling coughing expansile impulse on coughing
Movement of swelling is not a criterion
bcz as these swellings move with
coughing
Encysted hydrocele of
cord : localized swelling
of spermatic cord
Undescended testis
TONY 2010 MBBS
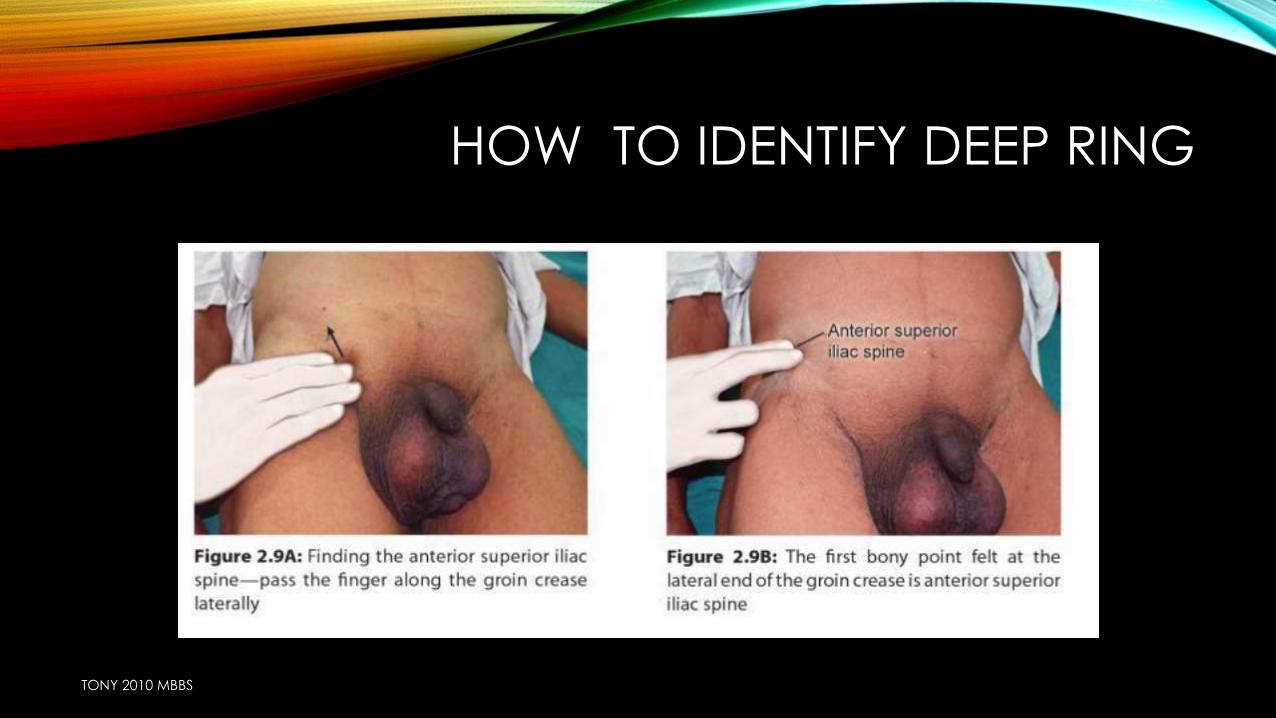
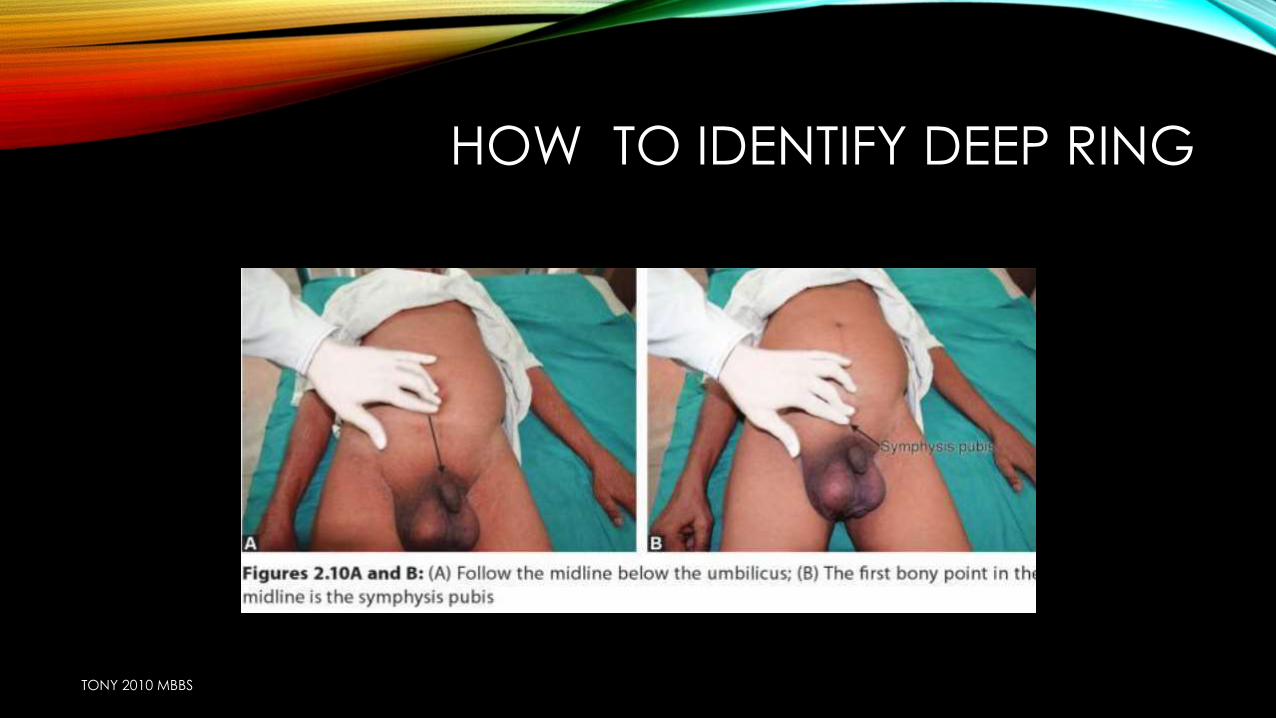
HOW TO IDENTIFY DEEP RING
TONY 2010 MBBS
HOW TO IDENTIFY DEEP RING
TONY 2010 MBBS
TONY 2010 MBBS
REDUCIBILITY
• Reduces on lying down direct hernia
• Using TAXIS
• Flexes the thigh
• Adduct the thigh
• Rotate internally
• Reduces with gurgling=>ENTEROCELE Difficult to reduce initially but last
part slips of easily
• First part reduces easily last part difficultomentocele
Relaxes
superficial
inguinal ring +
oblique muscles
TONY 2010 MBBS
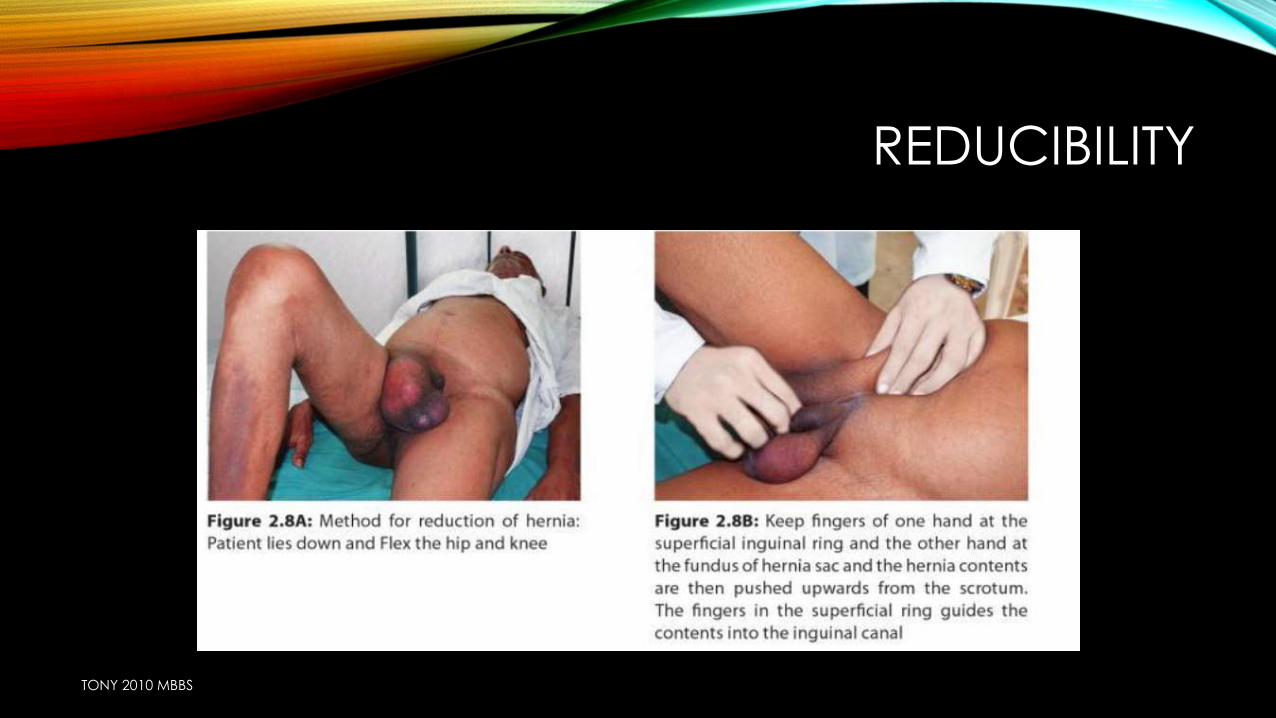
REDUCIBILITY
TONY 2010 MBBS
INVAGINATION TEST
• After reduction of hernia in recumbent position
• Using little finger rt. Hand side for rt. Side
lt. hand side for lt. side
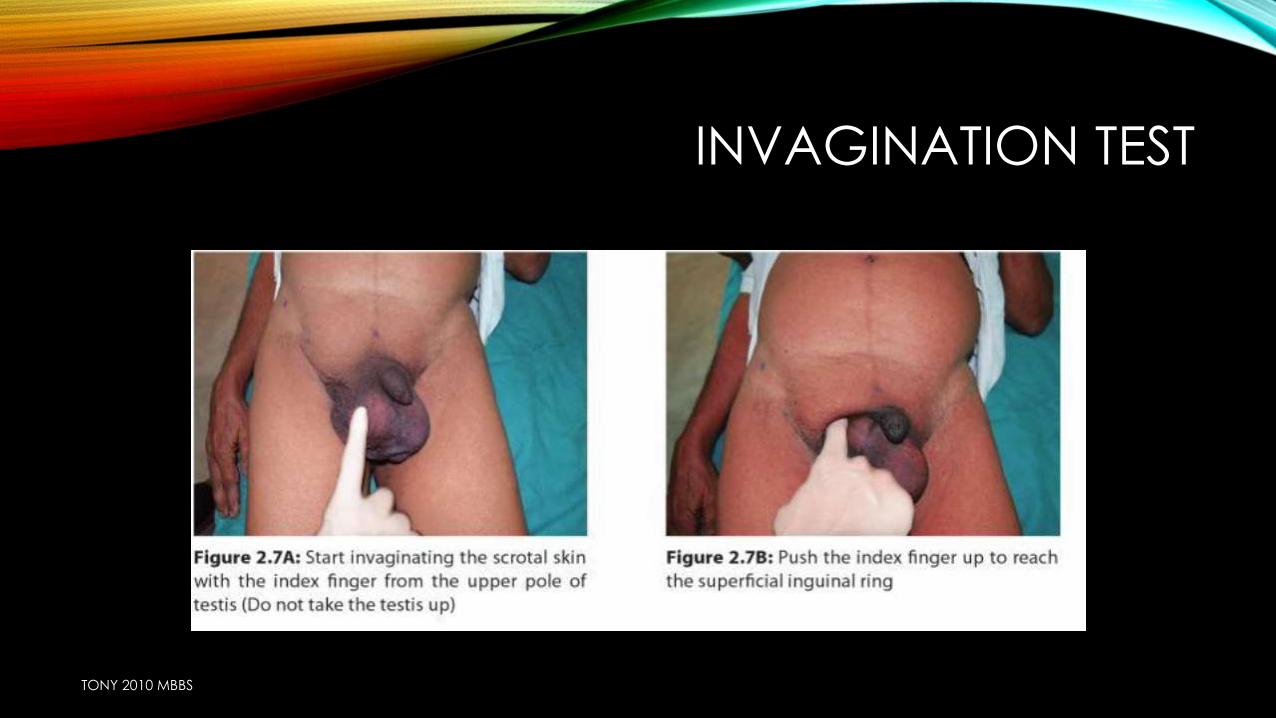
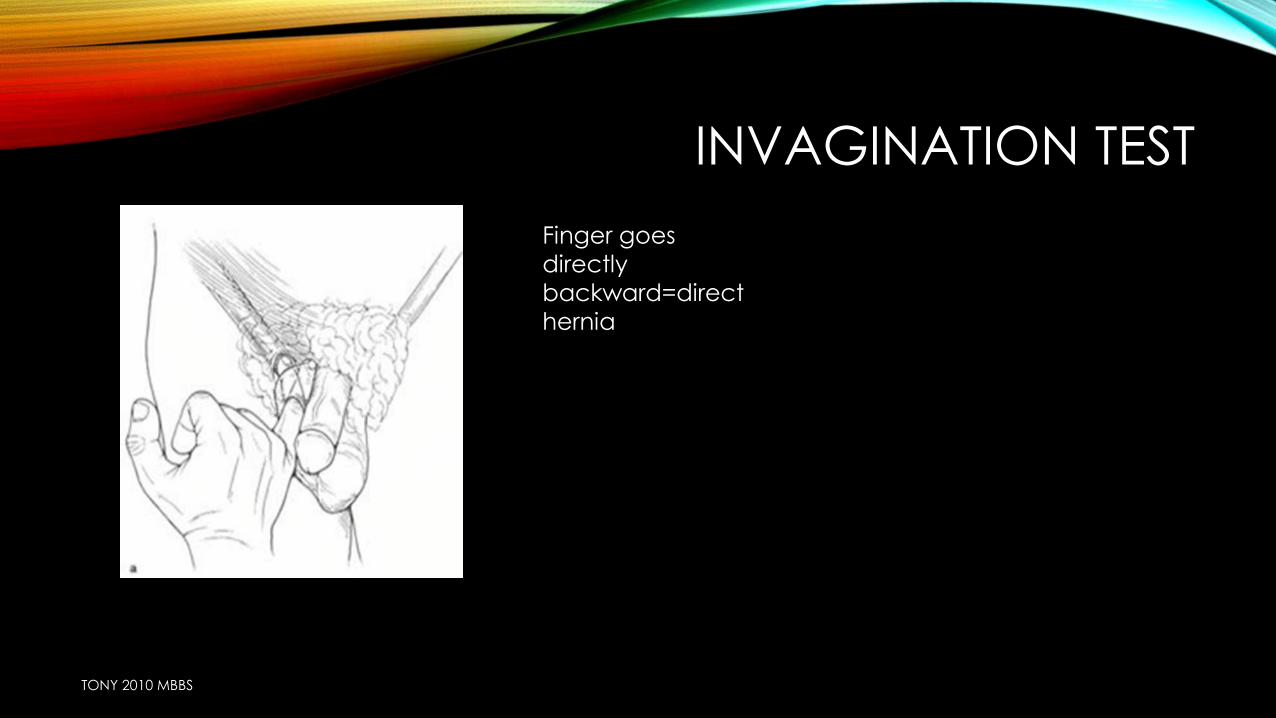
• Invaginate skin 4m the bottom of scrotum & the little finger is pushed to palpate pubic tubercle
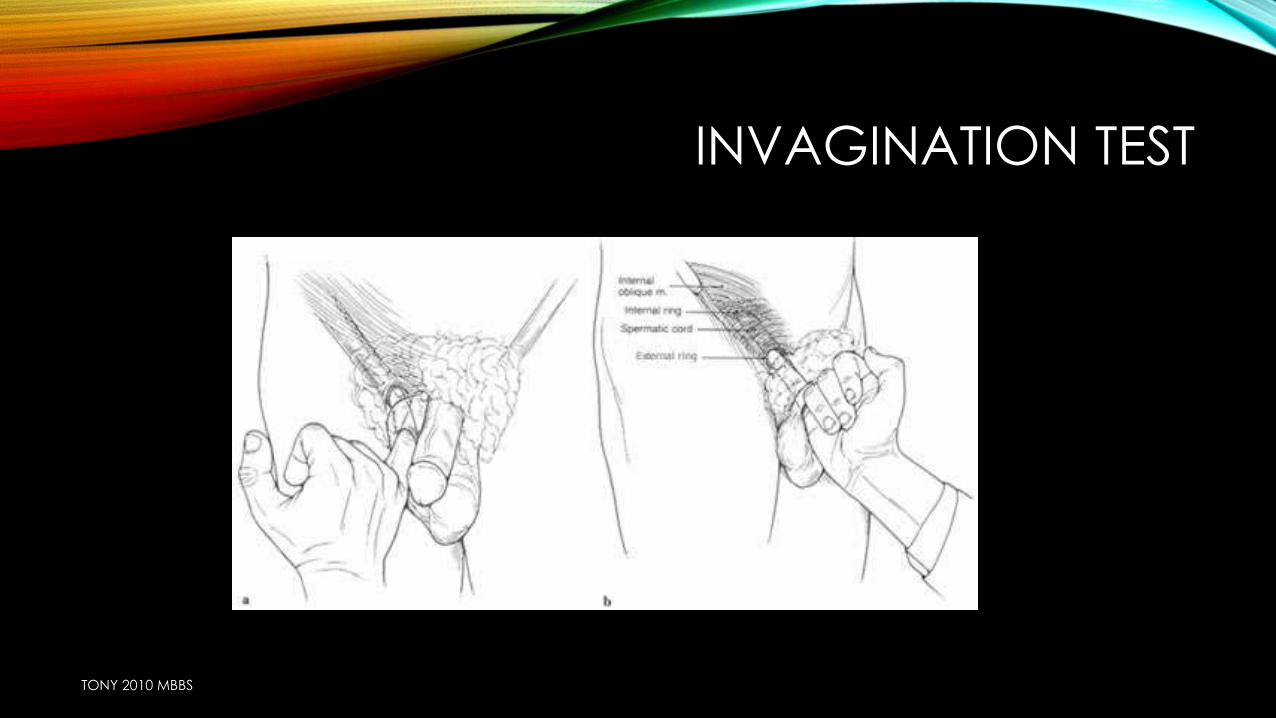
• Finger is then rotated & pushed further up in to superficial inguinal ring
• Nail will be against spermatic cord pulp will feel walls of ring
• Normal ring transmits only tip of finger ,>1 finger}abnormally large
TONY 2010 MBBS
INVAGINATION TEST
TONY 2010 MBBS
INVAGINATION TEST
TONY 2010 MBBS
INVAGINATION TEST
Finger goes
directly
backward=direct
hernia
TONY 2010 MBBS
INVAGINATION TEST
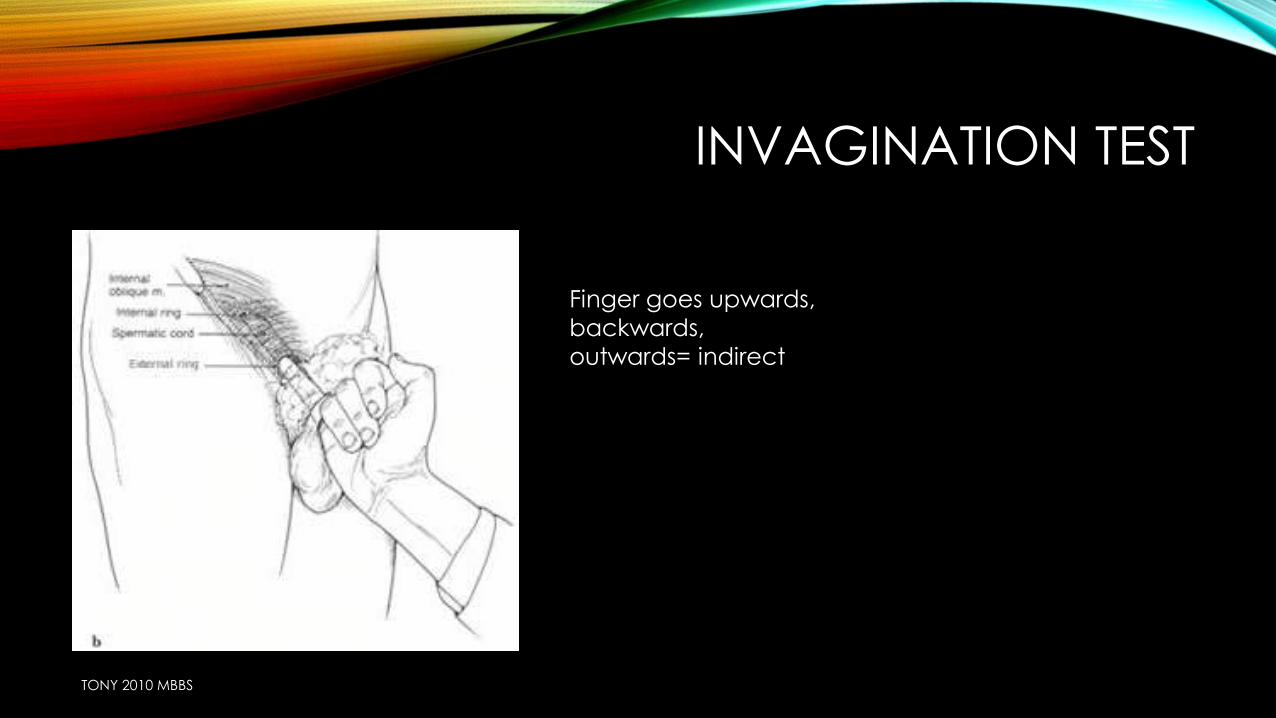
Finger goes upwards,
backwards,
outwards= indirect
TONY 2010 MBBS
INVAGINATION TEST
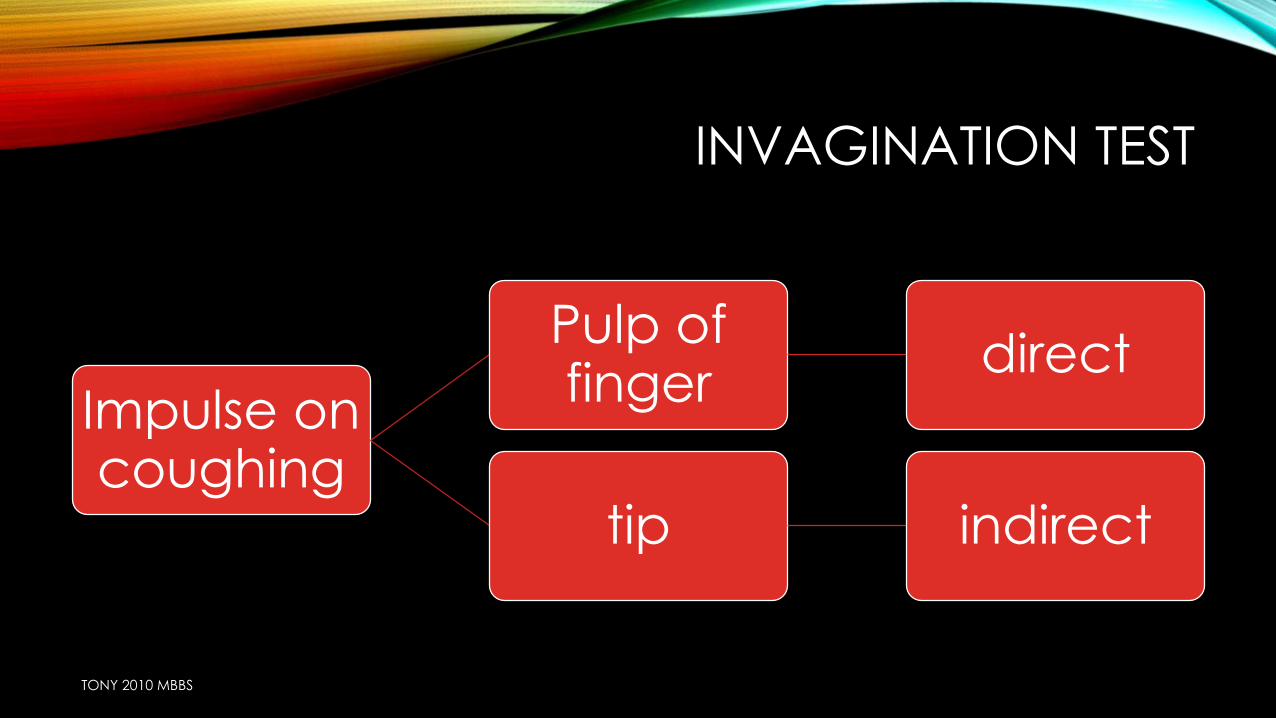
Impulse on coughing
Pulp of finger
direct
tip indirect
TONY 2010 MBBS
RING OCCLUSION TEST
• Standing position after reduction of swelling
• Using thumb pressure over the deep inguinal ring (1/2 “ above mid inguinal point) & is asked to cough
• Occlude direct hernia but not direct hernia
• Similarly on saphenous opening= femoral hernia
TONY 2010 MBBS
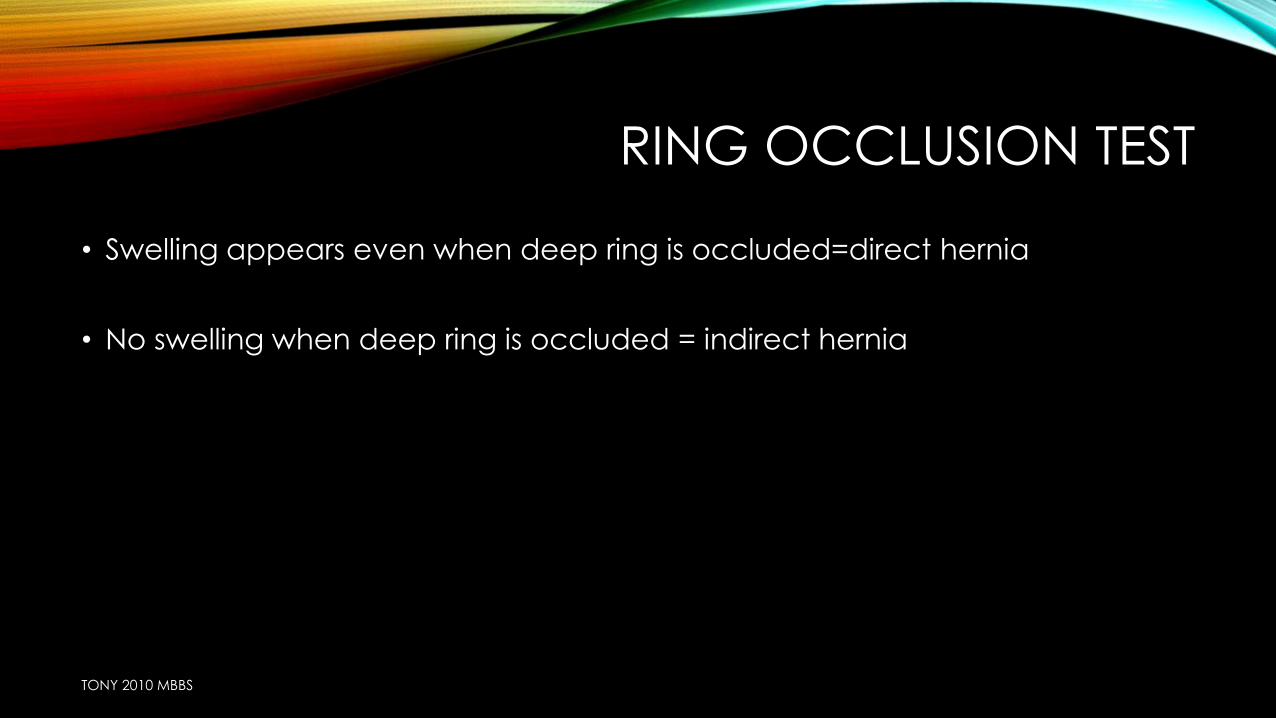
RING OCCLUSION TEST
• Swelling appears even when deep ring is occluded=direct hernia
• No swelling when deep ring is occluded = indirect hernia
TONY 2010 MBBS
TONY 2010 MBBS
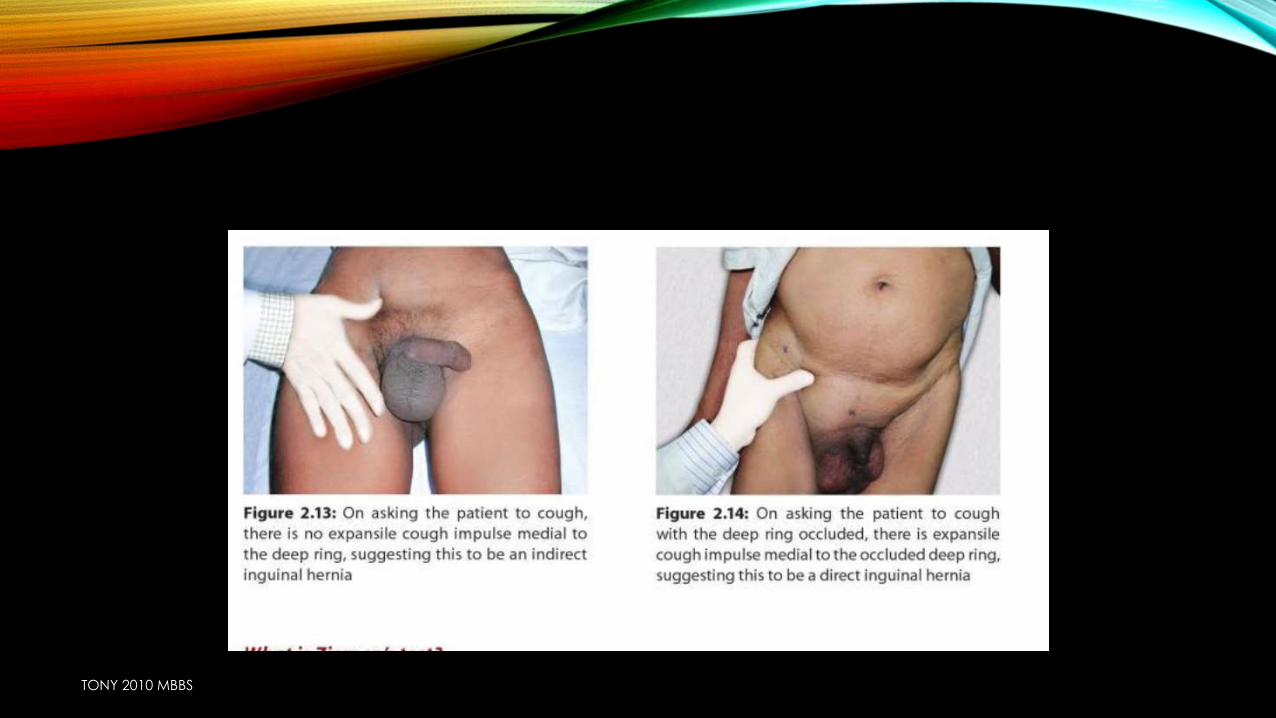
IN CASE OF A CHILD
• Inguinal hernia is invisible in child due to presence of thick pad of fat over inguinal region
• To make it visible ask him to jolt/jump/make it cry
• Gornalls test: child is held from back by both hands of the clinician on its abdomen,abdomen is pressed and child is lifted up
increased intra abdominal pressure
hernia more prominent
TONY 2010 MBBS
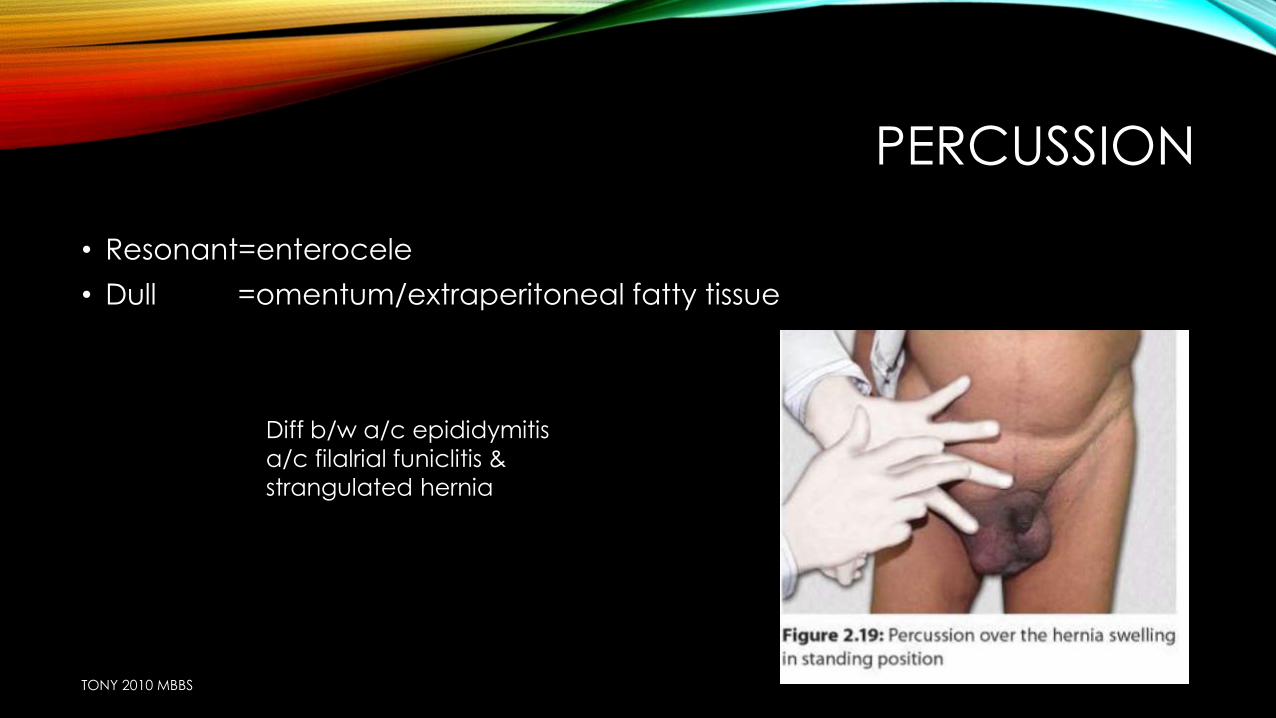
PERCUSSION
• Resonant=enterocele
• Dull =omentum/extraperitoneal fatty tissue
Diff b/w a/c epididymitis
a/c filalrial funiclitis &
strangulated hernia
TONY 2010 MBBS
AUSCULTATION
• Peristaltic sounds=enterocele
TONY 2010 MBBS
EXAMINATION OF TESTIS ,SPERMATIC CORDS & EPIDIDYMIS
• Testis traction test: pull testis downwards
encysted hydrocele}descends slightly & become fixed
inguinal hernia}cant be fixed
TONY 2010 MBBS
EXAMINATION OF TONE OF ABDOMINAL MUSCLES
• Inspectionprotrusion of lower abdominal wall
• Malgaigne’s bulging:
• oval shaped b/l bulge on straining above & parallel to medial half of inguinal ligament
• weakness of abdominal wall
• DIRECT HERNIA
• HERNIOPLASTY IS REQUIRED
TONY 2010 MBBS
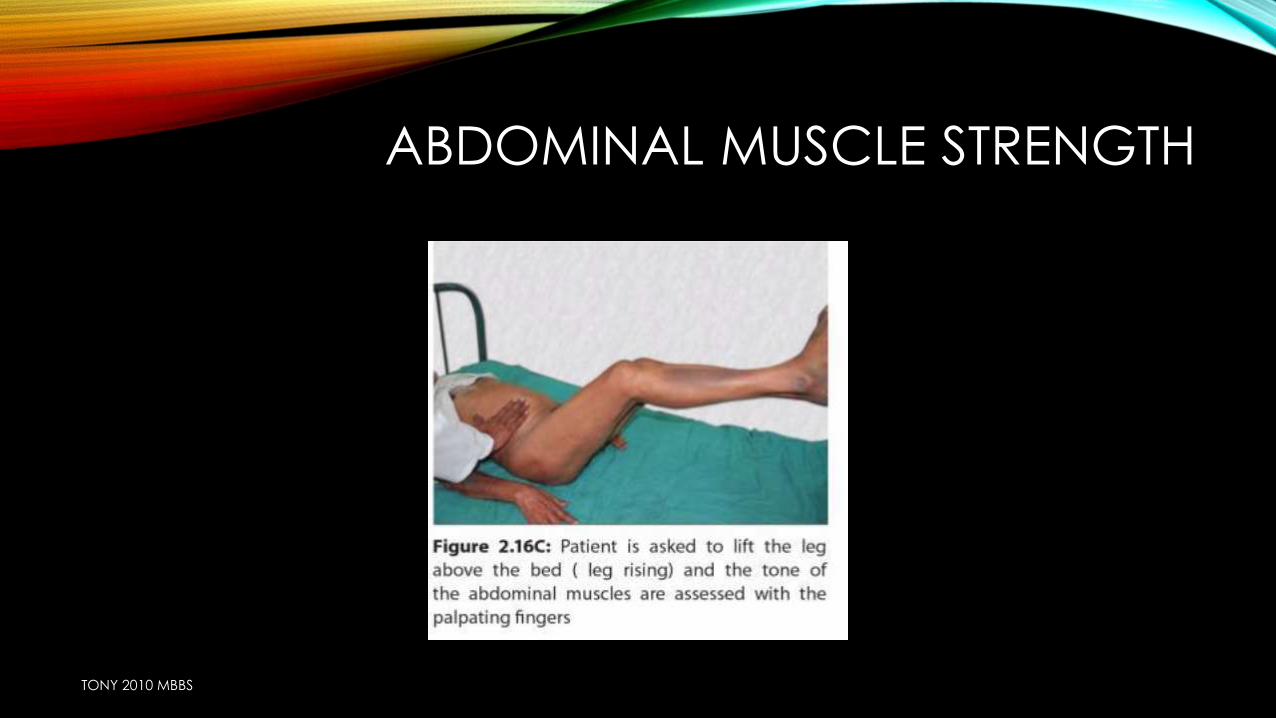
ABDOMINAL MUSCLE STRENGTH
TONY 2010 MBBS
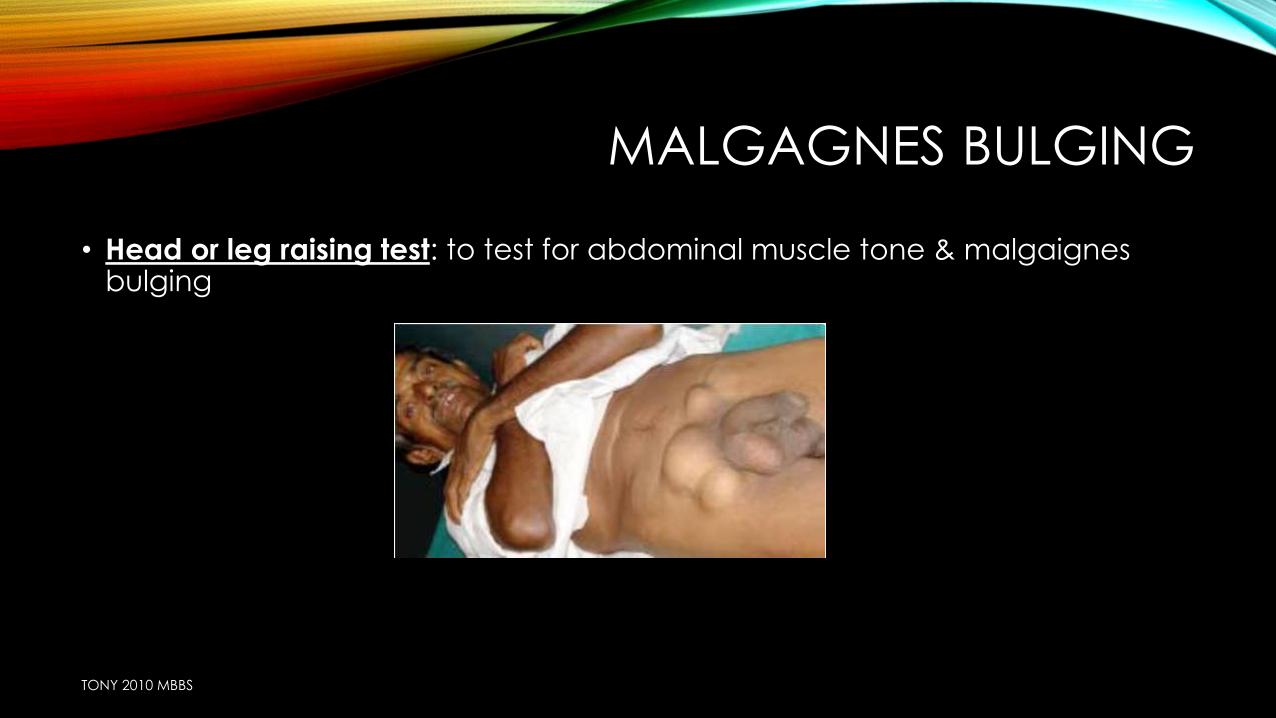
MALGAGNES BULGING
• Head or leg raising test: to test for abdominal muscle tone & malgaignesbulging
TONY 2010 MBBS
SYSTEMIC EXAMINATION
• RESPIRATORY SYSTEM
• R/O
• C/C BRONCHITIS ,TB
• ABDOMEN
• MASS
• ASCITES
TONY 2010 MBBS
• Abdominal examination
• Respiratory system
• Urinary systems
• Per rectal examination
TONY 2010 MBBS
PER-RECTAL EXAMINATION
• 1. Benign Prostate hypertrophy—micturition difficulty
• 2.Malignant obstruction
• 3. Chronic fissure—constipation
TONY 2010 MBBS
• Diagnosis
• • Side—right/left
• • Type—indirect/direct
• • Inguinal—femoral
• • Complete/Incomplete
• • Complicated/Uncomplicated
• • Content—enterocele/omentocele
TONY 2010 MBBS
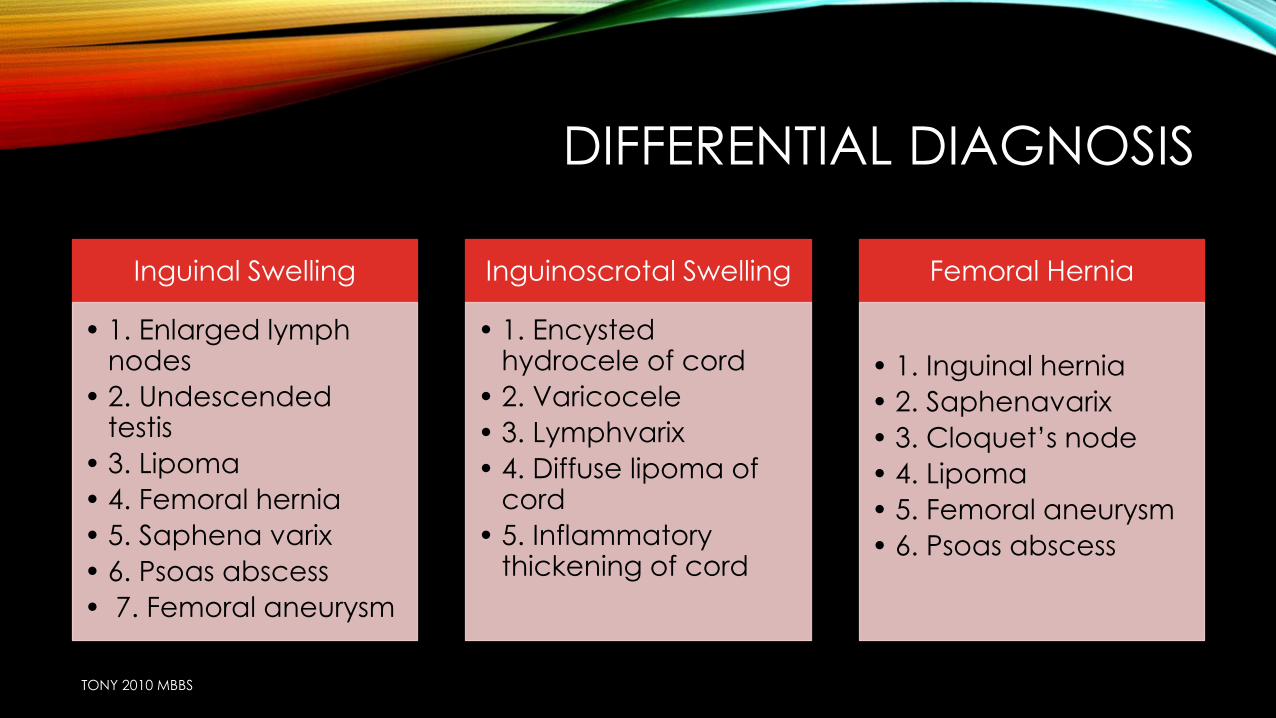
DIFFERENTIAL DIAGNOSIS
Inguinal Swelling
• 1. Enlarged lymph nodes
• 2. Undescended testis
• 3. Lipoma
• 4. Femoral hernia
• 5. Saphena varix
• 6. Psoas abscess
• 7. Femoral aneurysm
Inguinoscrotal Swelling
• 1. Encysted hydrocele of cord
• 2. Varicocele
• 3. Lymphvarix
• 4. Diffuse lipoma of cord
• 5. Inflammatory thickening of cord
Femoral Hernia
• 1. Inguinal hernia
• 2. Saphenavarix
• 3. Cloquet’s node
• 4. Lipoma
• 5. Femoral aneurysm
• 6. Psoas abscess
TONY 2010 MBBS
DIFFERENTIAL DIAGNOSISIn males
• Hydrocele –infantile/encysted/large vaginal/
• Undescended testis
• Femoral hernia
• Lipoma of the cord
• Hydrocele of the canal of nuck (in females)
• Inguinal lymph node enlargement
• Groin abscess
In females
• hydrocele of the canal of Nuck –this is the most common dif-ferential diagnostic problem
• femoral hernia.
TONY 2010 MBBS

MANAGEMENT
TONY 2010 MBBS
• Investigations
• Treatment
TONY 2010 MBBS
INVESTIGATIONS
• I. Routine• • Hemoglobin• • Bleeding time/Clotting time• • Total count, differential count, ESR• • Urine—albumin, sugar deposits• • Blood—urea, sugar• • Blood grouping/typing—for irreducible hernia/huge hernia
• II. Anesthetic Purpose• • X-ray chest (Chronic TB, Asthma—precipitate hernia)• • ECG all leads
• III. USG Abdomen and Pelvis• • In old age group—to find benign prostate hyperplasia calculate post-voidal
residual urine. If >100 ml it is significant• • To find any mass
TONY 2010 MBBS
TREATMENT
• TREATMENT
• Treat the precipitating cause of hernia first.
• 1. Benign prostate hypertrophy
• 2. Tuberculosis
• 3. Stop smoking
• Conservative management
• indicated only in cases of very old man with direct hernia; since there is no chance of obstruction.
• TRUSS
• surgery
TONY 2010 MBBS
TRUSS
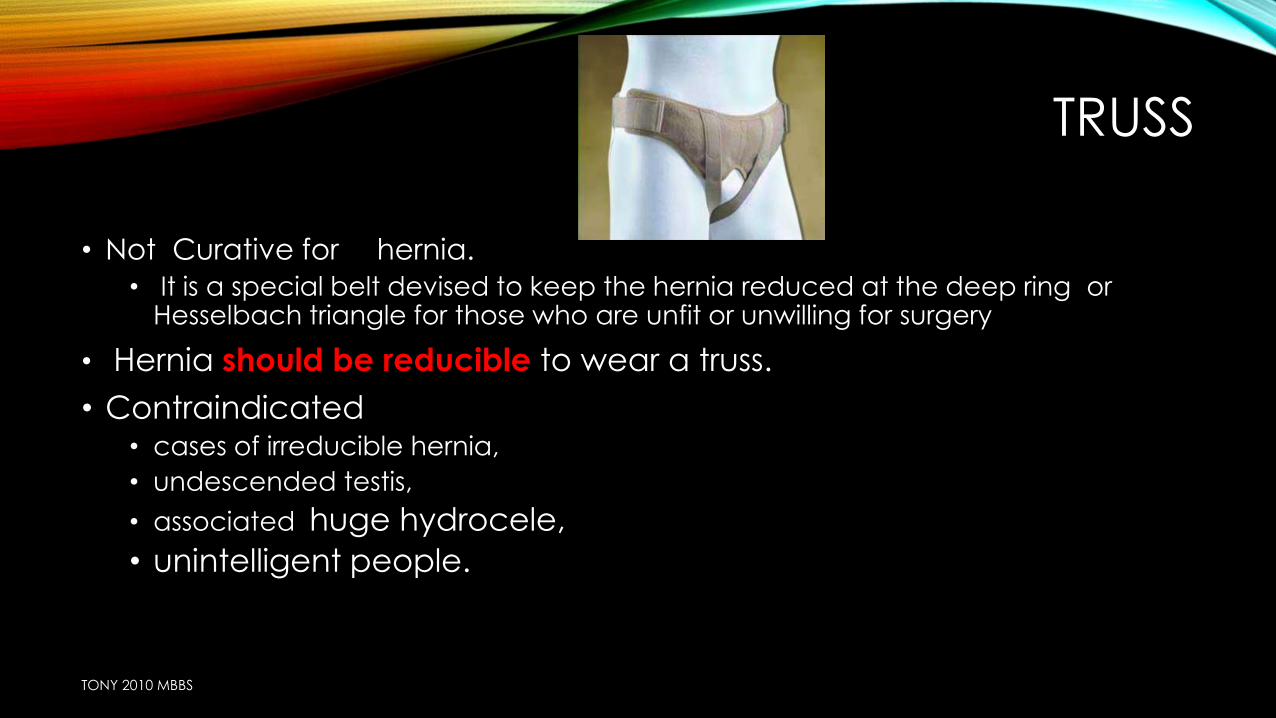
• Not Curative for hernia.
• It is a special belt devised to keep the hernia reduced at the deep ring or Hesselbach triangle for those who are unfit or unwilling for surgery
• Hernia should be reducible to wear a truss.
• Contraindicated • cases of irreducible hernia,
• undescended testis,
• associated huge hydrocele,
• unintelligent people.
TONY 2010 MBBS
TAXIS
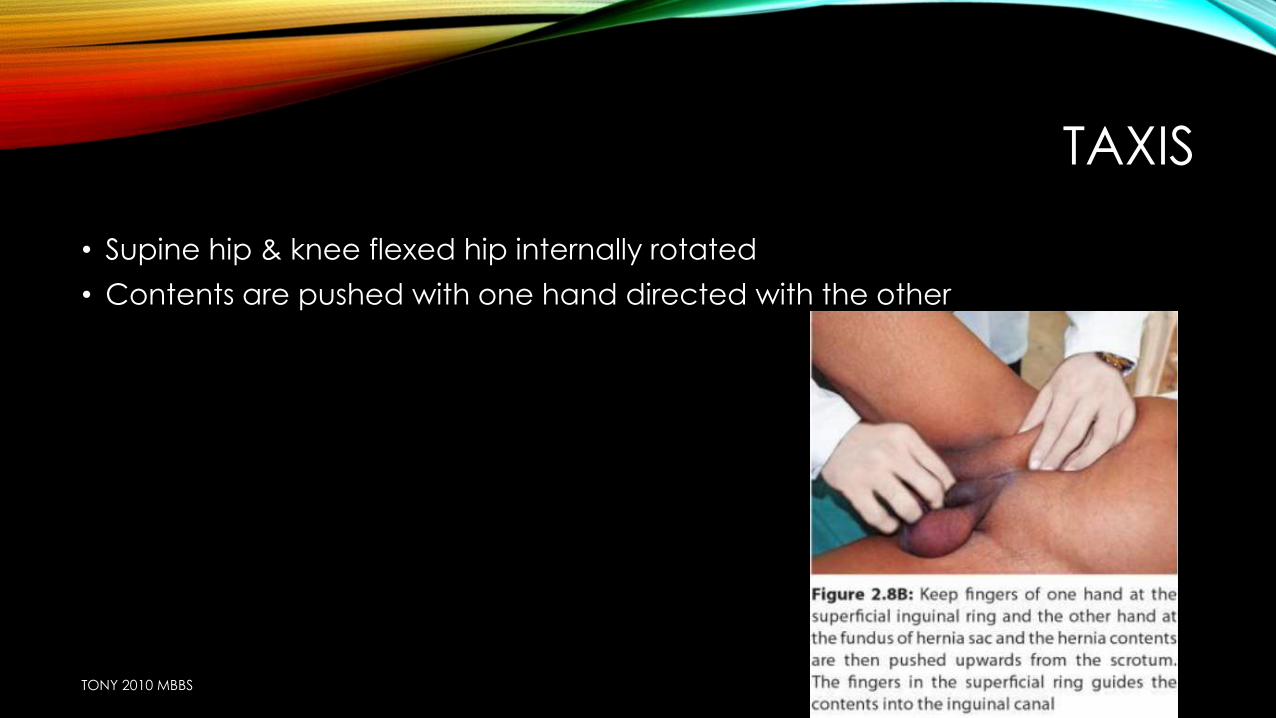
• Supine hip & knee flexed hip internally rotated
• Contents are pushed with one hand directed with the other
TONY 2010 MBBS
TREATMENT
• Surgery= treatment of choice
• Under LA/GA/spinal/epidural
surgery
Hernioplasty
herniorraphy
TONY 2010 MBBS
Herniorraphy(strenghthening of posterior wall)
• 1. Original Bassini
• 2. Modified Bassini
• 3. McVay’s
• 4. Shouldice
Hernioplasty (prosthetic repair )
• 1. Lichtenstein
• 2. Gilbert’s plug
• 3. Prolene hernia system
• 4. Laparoscopic mesh repair
• 5. Stoppas repair
TONY 2010 MBBS
HERNIORRHAPHY
• 1. Herniotomy
• 2. Narrowing of the deepring with 2'0 prolene (Lytle'sRepair)
• 3. Approximation of conjoint tendon with inguinal ligament using 1‘ polypropylene material
TONY 2010 MBBS
HERNIOTOMY
• Dissecting out and opening of hernia sac ,reducing any contents ,transfixing neck of sac & removing the remainder
• NO NEED TO OPEN UP CANAL IN CHILDREN BECAUSE SUPERFICIAL AND DEEP RING ARE SUPERIMPOSED ……THERE FORE NO NEED OF REPAIR
• HENCE DONE ALONE IN CHILDREN,ADOLESCENT
In indirect inguinal hernia
TONY 2010 MBBS
TONY 2010 MBBS
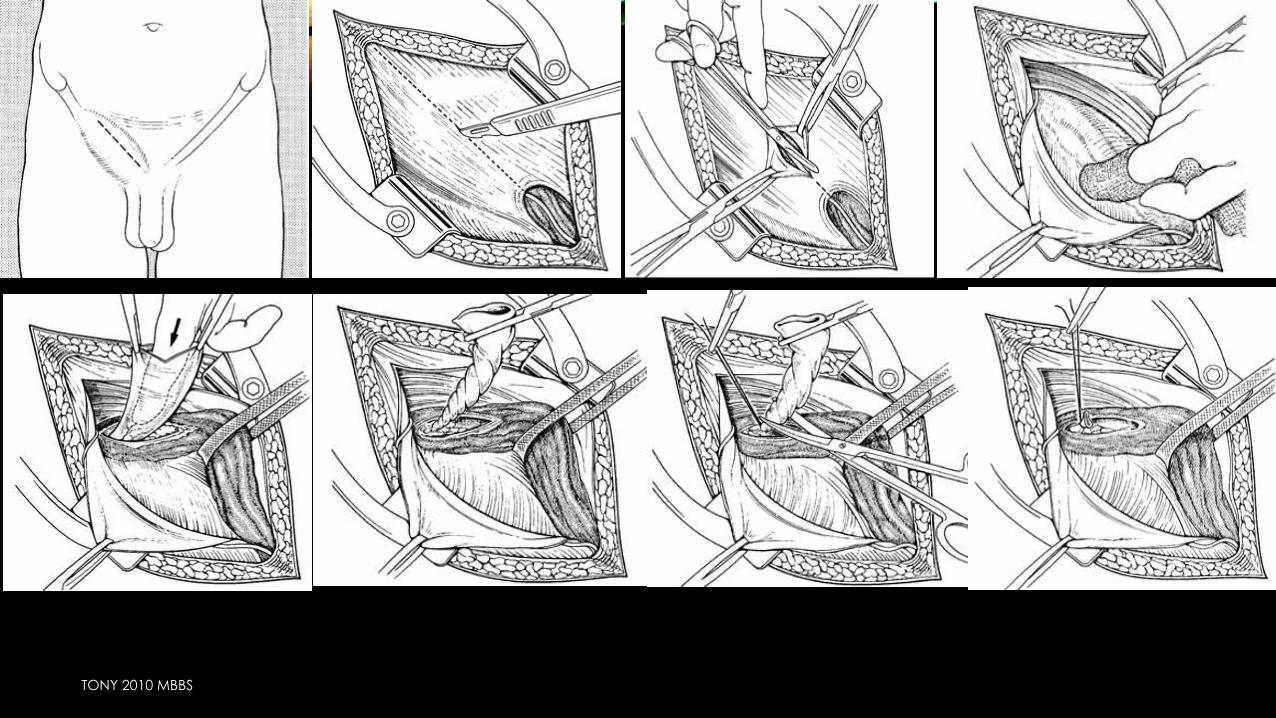
PROCEDURE
• ANAESTHESIA: spinal or G/A
• Incision is made parallel to medial 2/3rd of inguinal ligament about 1.25 cm above inguinal ligament
• After dividing superficial fascia and securing hemostasis
• Identify external oblique muscle & superficial inguinal ring
• External oblique Apo neurosis is incised in the line of its fibers and is reflected above and below.thus visualize inguinal ligament
• Ilioinguinal nerve is thus identified and preserved
TONY 2010 MBBS
PROCEDURE
• Cremasteric muscle is opened
TONY 2010 MBBS
• Herniotomy = ligation & excision of sac only
• Herniorraphy = herniotomy + repair of posterior wall
• Hernioplasty= herniotomy + reconstruction of posterior wall with prosthetics
TONY 2010 MBBS

HERNIORRAPHY
TONY 2010 MBBS
HERNIORRHAPHY
• HERNIOTOMY+ REPAIR OF THE POSTERIOR WALL OF INGUINAL CANAL BY APPOSING CONJOINED MUSCLE TO THE INGUINAL LIGAMENT
• INDN
• IN ALL INDIRECT HERNIA EXCEPT IN CHILDREN
• IN ADULTS WITH GOOD MUSCLE TONE
TONY 2010 MBBS
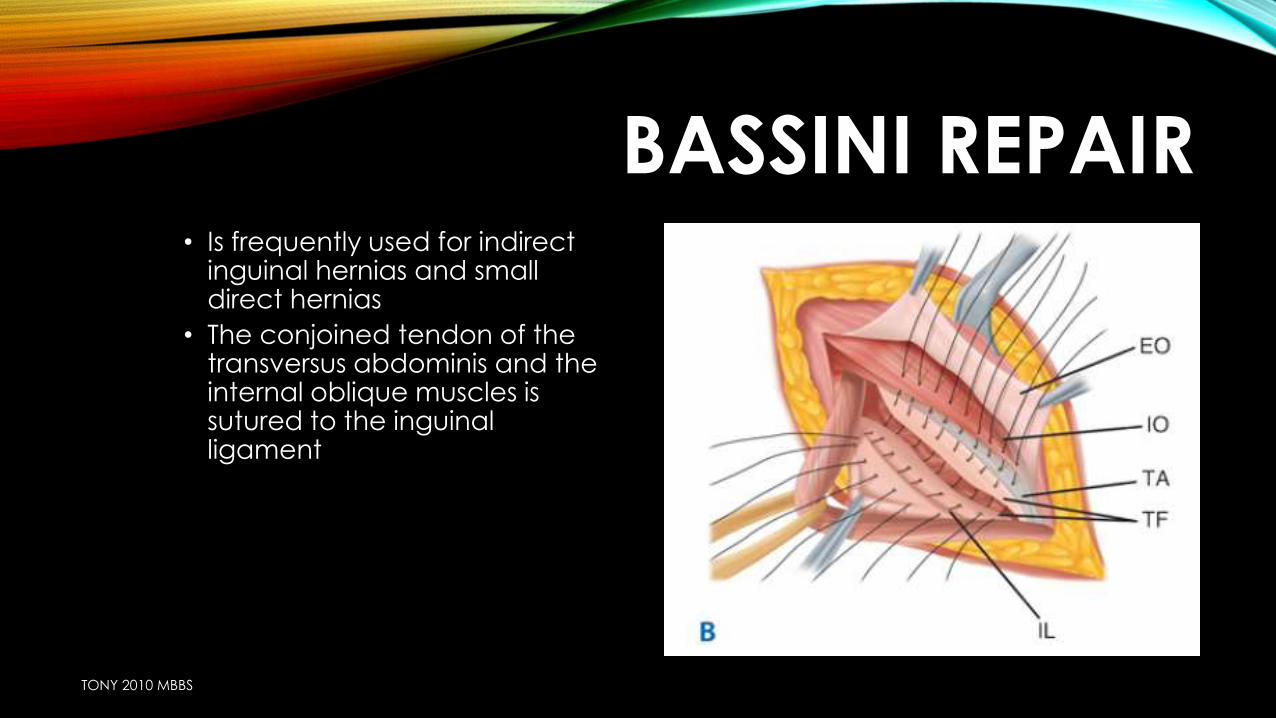
BASSINI REPAIR• Is frequently used for indirect
inguinal hernias and small direct hernias
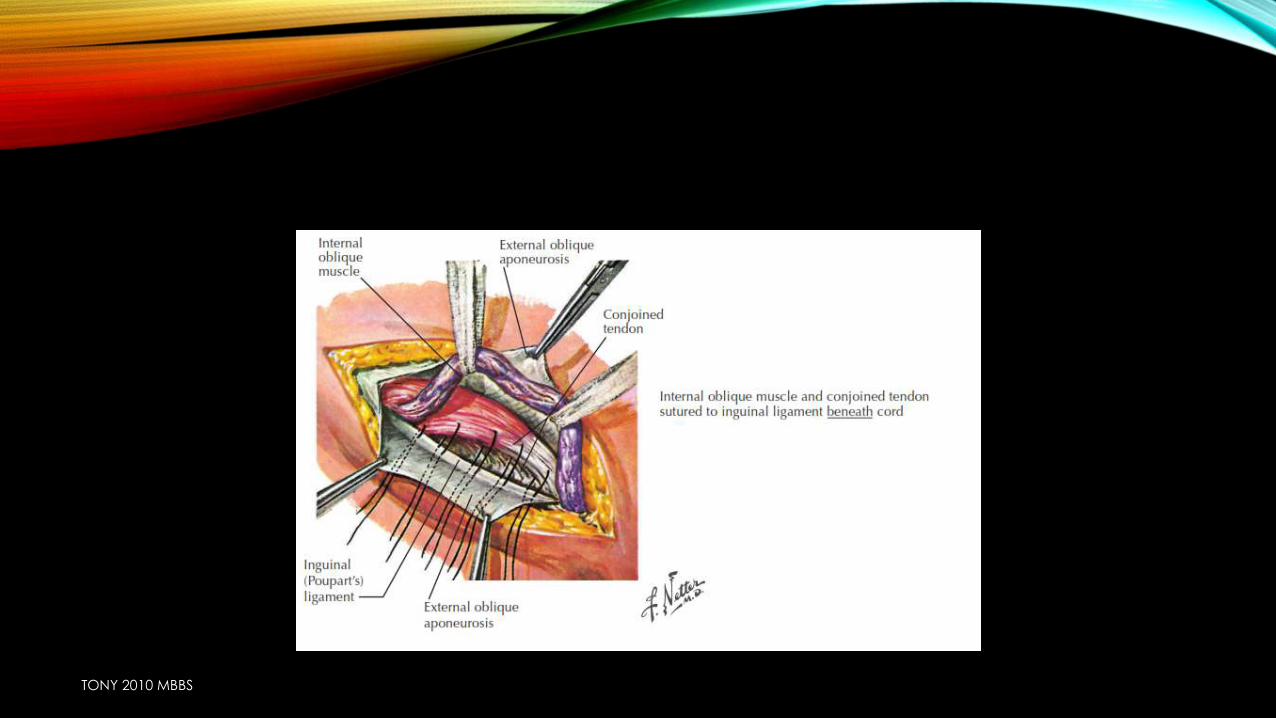
• The conjoined tendon of the transversus abdominis and the internal oblique muscles is sutured to the inguinal ligament
TONY 2010 MBBS
TONY 2010 MBBS
BASSINI REPAIR
• The conjoined tendon is retracted upward
• the aponeurosis of the transversus abdominis muscle is approximated to the iliopubic tract that lies adjacent to the inguinal ligament with several interrupted 3-0 silk sutures.
• The second layer of the repair involves suturing the conjoined tendon to the inguinal ligament with interrupted 2-0 silk sutures.
• This suture line extends from the pubic tubercle to the medial border of the internal ring.
TONY 2010 MBBS
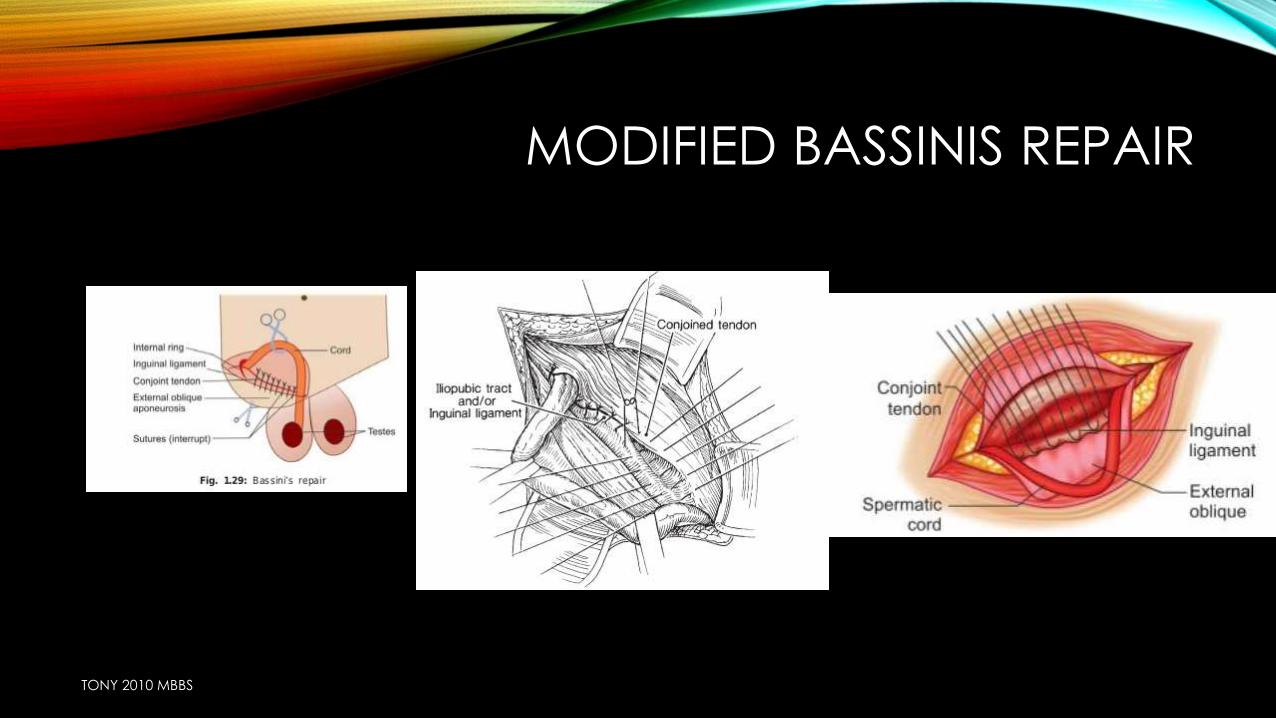
MODIFIED BASSINIS REPAIR
• Most commonly used EARLIER
• Using non absorbable monofilament interrupted suture material strengthening of posterior wall of inguinal canal approximation of conjoint tendon to inguinal ligament
• Nonsorbable adequate tensile strength for about 6 months
• Monofilamentpolyfilament has crevices=infn
• Interrupted continuous suture= decrease blood supply interfere with healing
TONY 2010 MBBS
MODIFIED BASSINIS REPAIR
TONY 2010 MBBS
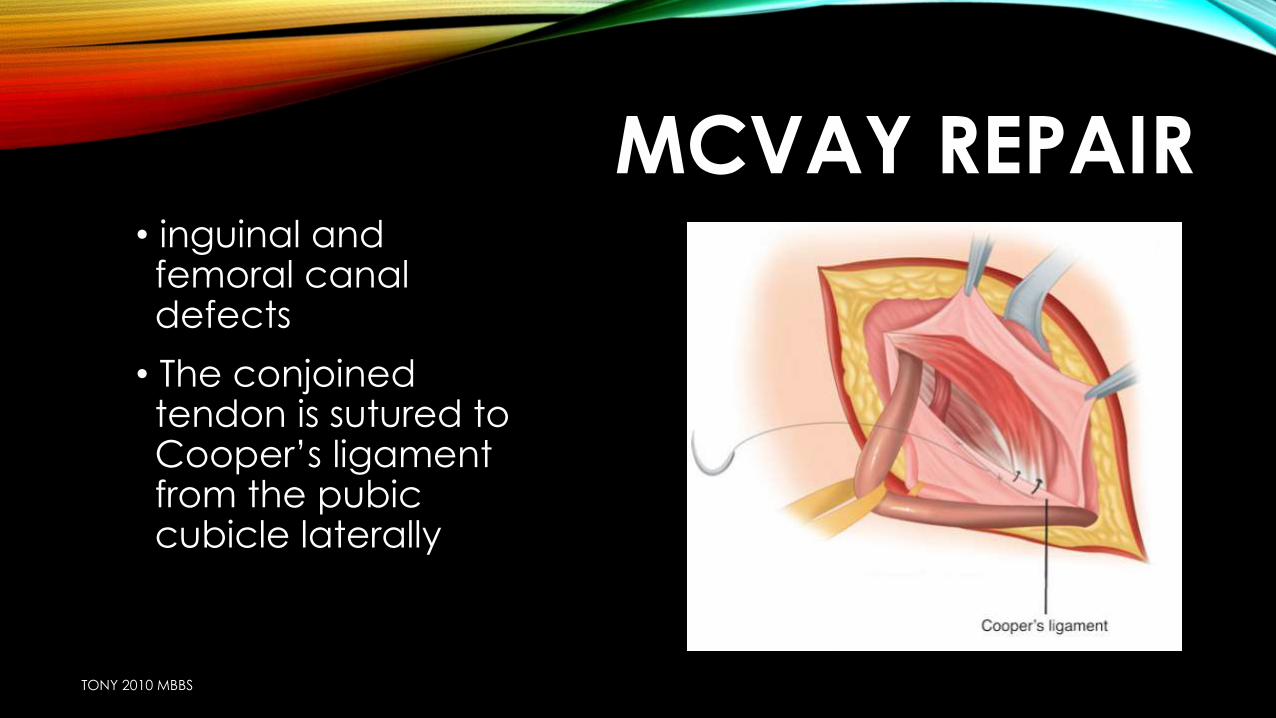
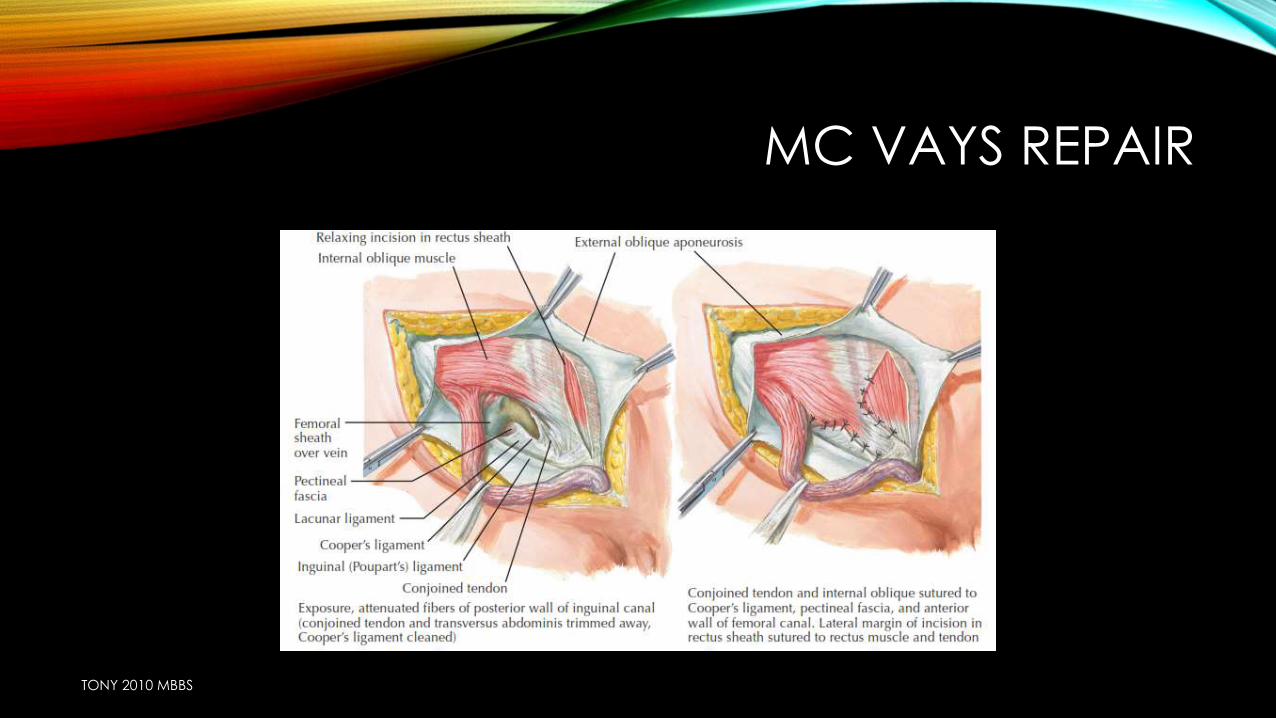
MCVAY REPAIR• inguinal and femoral canal defects
• The conjoined tendon is sutured to Cooper’s ligament from the pubic cubicle laterally
TONY 2010 MBBS
MC VAYS REPAIR
TONY 2010 MBBS
SHOULDICE REPAIR
• With a no. 15 scalpel an incision is made in the transversalis fascia. This incision is extended from the internal ring to the pubic tubercle.
• The repair involves placing four lines of sutures.
TONY 2010 MBBS
SHOULDICE REPAIR
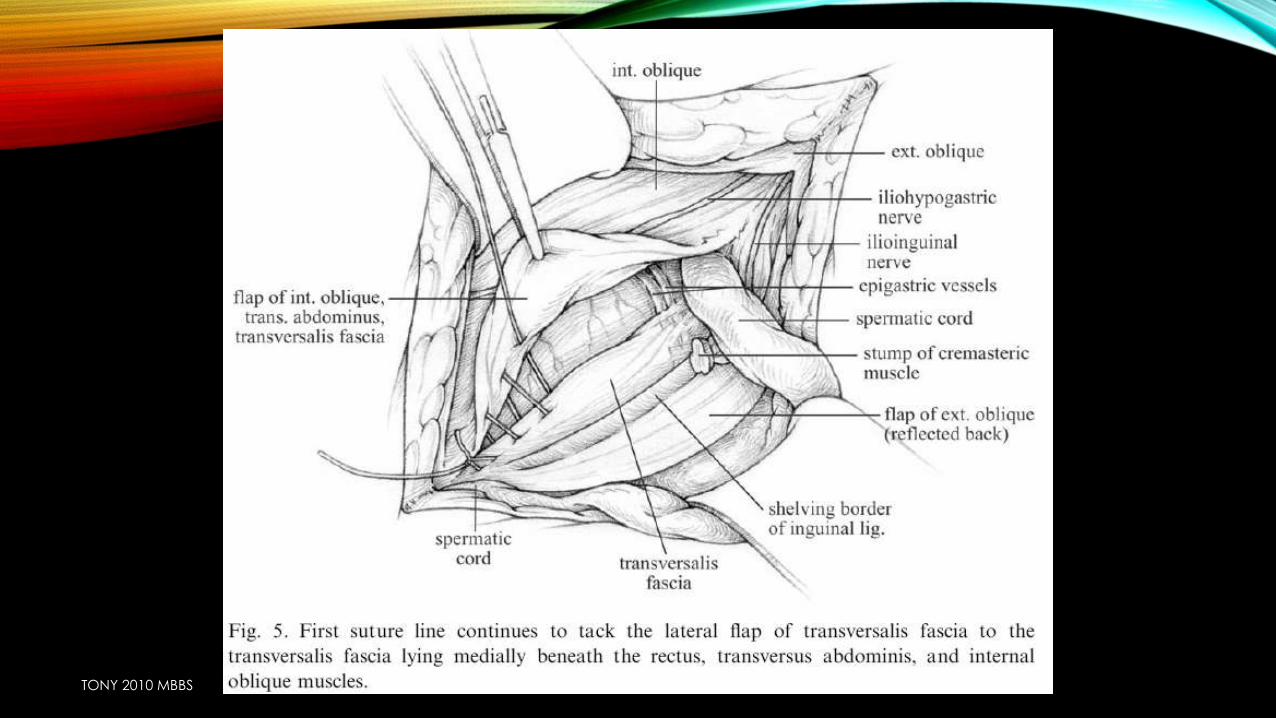
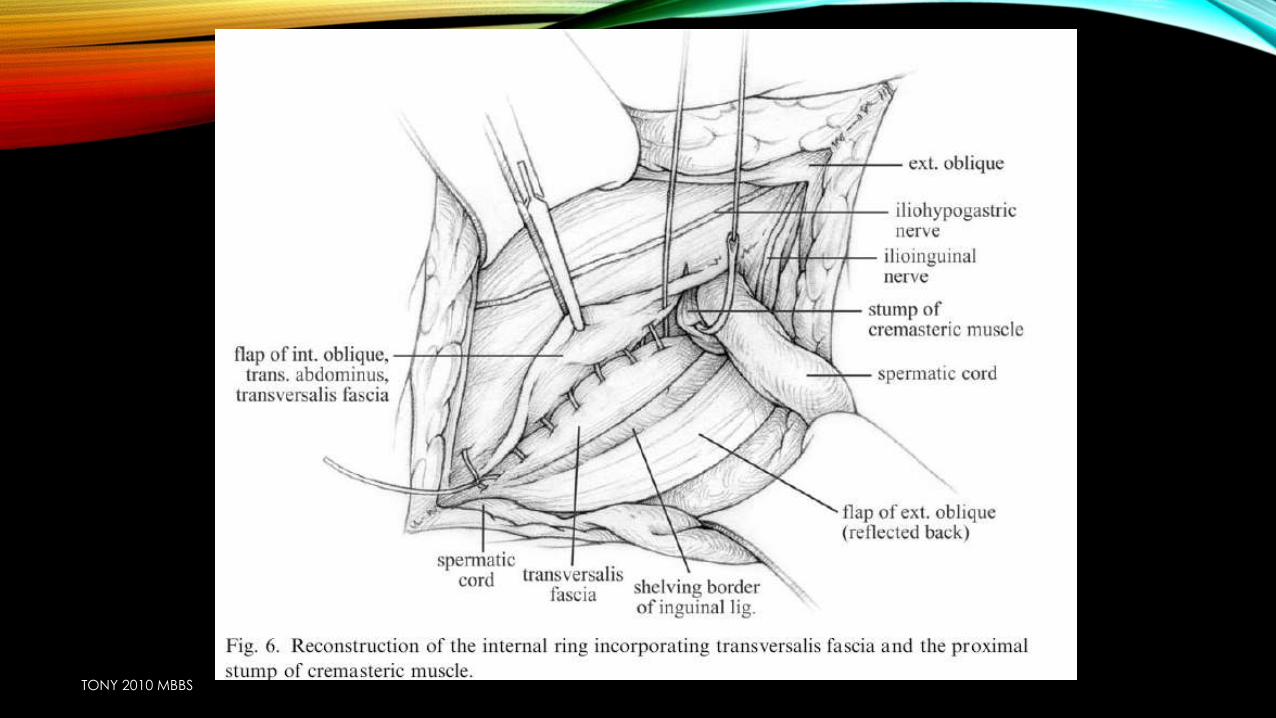
• First, the transversalis fascia is divided from the internal inguinal ring to the pubic tubercle. The posterior wall repair is accomplished by imbricating the lateral and medial leaves of the divided transverse aponeurotic fascial fibers with a continuous suture. The superomedial flap is brought over the inferolateral flap. The first suture line begins at the pubic tubercle and is sewn in a continuous fashion up to the internal ring, suturing the free edge of the inferolateral flap to the underside of the superomedial flap. At the internal inguinal ring, the cranial portion of the cremastermay be included in the suture line. This gives additional strength to the internal inguinal ring. The suture line is then doubled back bringing the leading edge of the superomedial flap to the edge of the inguinal ligament. The lacunar ligament is included in this suture line to obliterate the dead space medial to the femoral vessels. A second suture, beginning at the internal ring, brings the internal oblique and transversus muscles down to the deep surface of the inguinal ligament. At the level of the pubic bone, this suture doubles back, attaching the same structures in a more superficial plane and the suture is tied to itself at the internal ring.
TONY 2010 MBBS
SHOULDICE REPAIR
• The first suture line
• is started at the pubic tubercle using 3-0 continuous polypropylene, and the white line is approximated to the free edge of the inferior transversalis fascialflap.
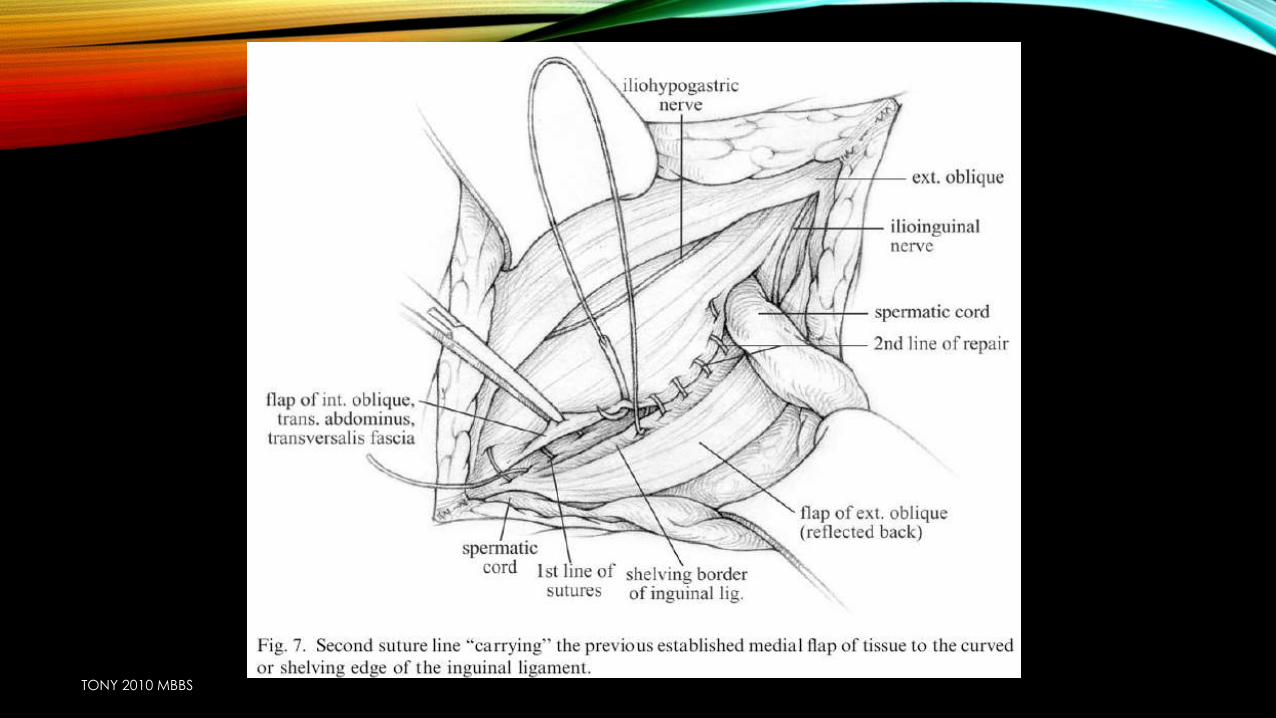
• The 2nd suture line :
• At the internal ring the suture is tied and then continued medially by approximating the free edge of the superior flap to the shelving edge of the inguinal ligament. When the pubic tubercle is reached, the suture is tied and divided.
TONY 2010 MBBS
SHOULDICE REPAIR
• The third suture line is started at the level of the internal ring where the conjoined tendon is approximated to the inguinal ligament and tied when the pubic tubercle is reached.
• Using the same suture, the fourth suture line attaches these same structures to one another and is tied at the level of the internal ring.
TONY 2010 MBBS
SHOULDICE REPAIR
• The cord is replaced within the inguinal canal, and the external inguinal aponeurosis is reapproximated with continuous 2-0 absorbable sutures
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
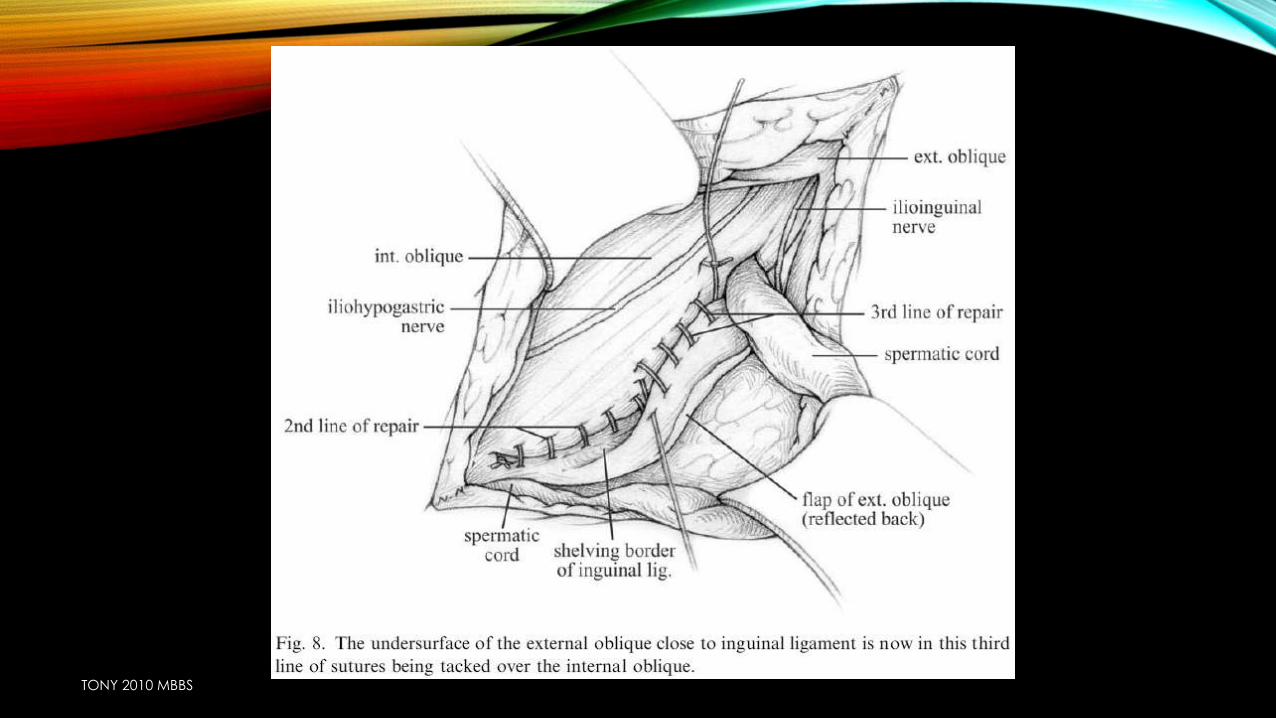
TONY 2010 MBBS
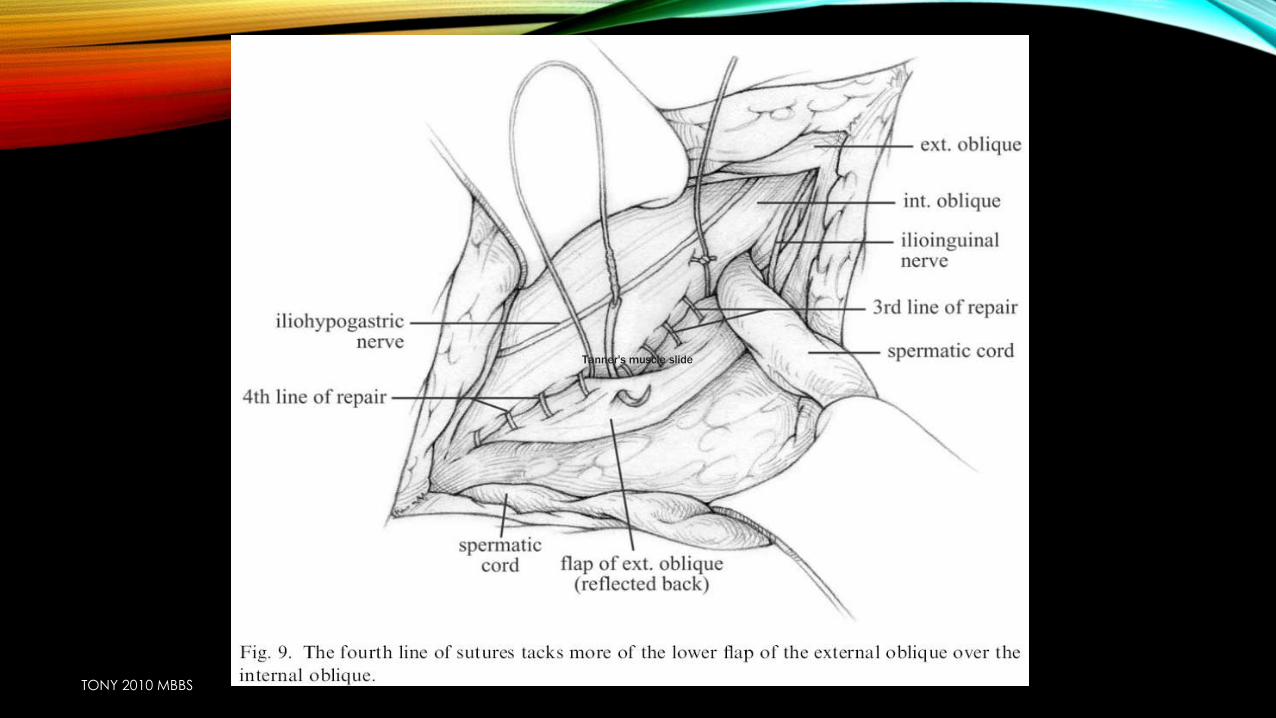
TONY 2010 MBBS
Tanner's muscle slide
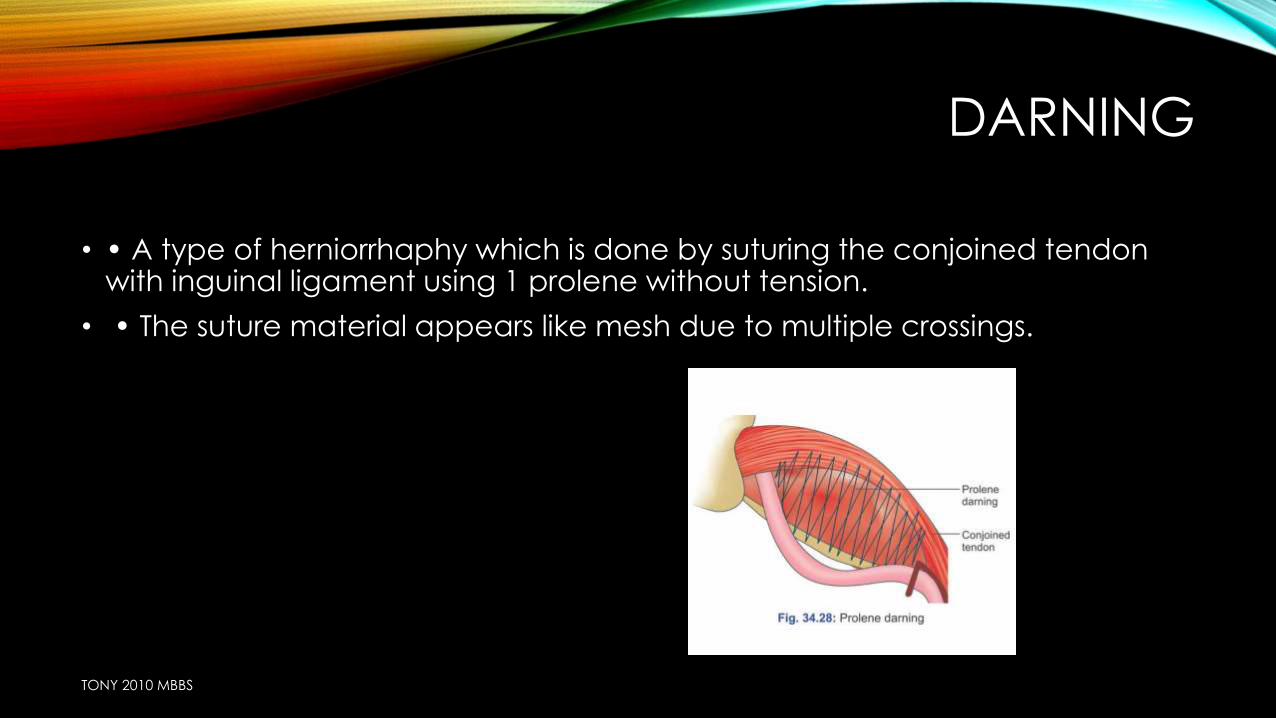
DARNING
• • A type of herniorrhaphy which is done by suturing the conjoined tendon with inguinal ligament using 1 prolene without tension.
• • The suture material appears like mesh due to multiple crossings.
TONY 2010 MBBS
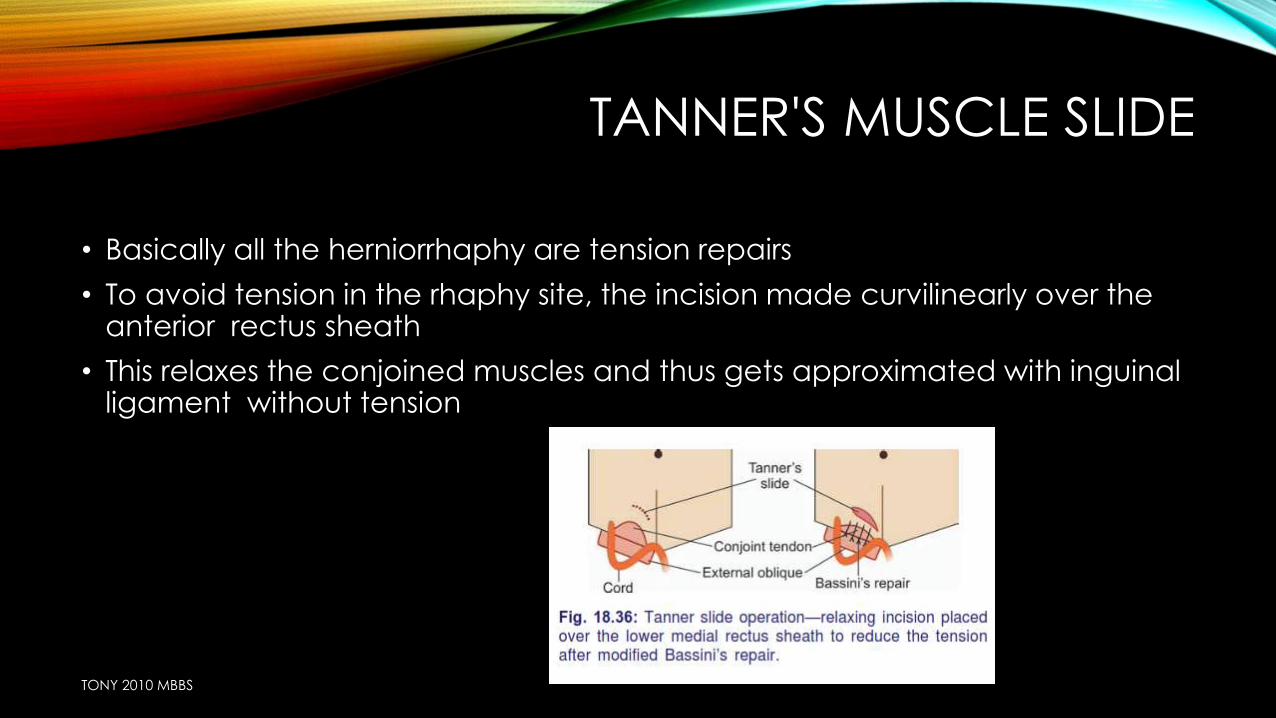
TANNER'S MUSCLE SLIDE
• Basically all the herniorrhaphy are tension repairs
• To avoid tension in the rhaphy site, the incision made curvilinearly over the anterior rectus sheath
• This relaxes the conjoined muscles and thus gets approximated with inguinal ligament without tension
TONY 2010 MBBS
HERNIOPLASTY
• SOME FORM OF supportive MATERIAL IS USED TO STRENGTHEN POSTERIOR ABDOMINAL WALL
HERNIOPLASTY
SYNTHETIC
BIOLOGICAL
Synthetic non
absorbable prolene,
Dacron are used
Tensor fascia
lata,temporal
fascia,skin
TONY 2010 MBBS

INDICATION FOR HERNIOPLASTY
• Direct hernia,
• Indirect hernia with poor muscle tone
• Recurrent hernia
• Re-recurrent hernia
• Incisional hernia
• Old age
• Sliding hernia
TONY 2010 MBBS
COMPLICATION
• Mesh extrusion
• Foreign body reaction
• infection
TONY 2010 MBBS
PRINCIPLE
• Size of mesh >size of defect
• Attached above & below to conjoint tendon & inguinal ligament/abdominal wall using non absorbable sutures
• Haemostasis, reduce risk of infection
TONY 2010 MBBS
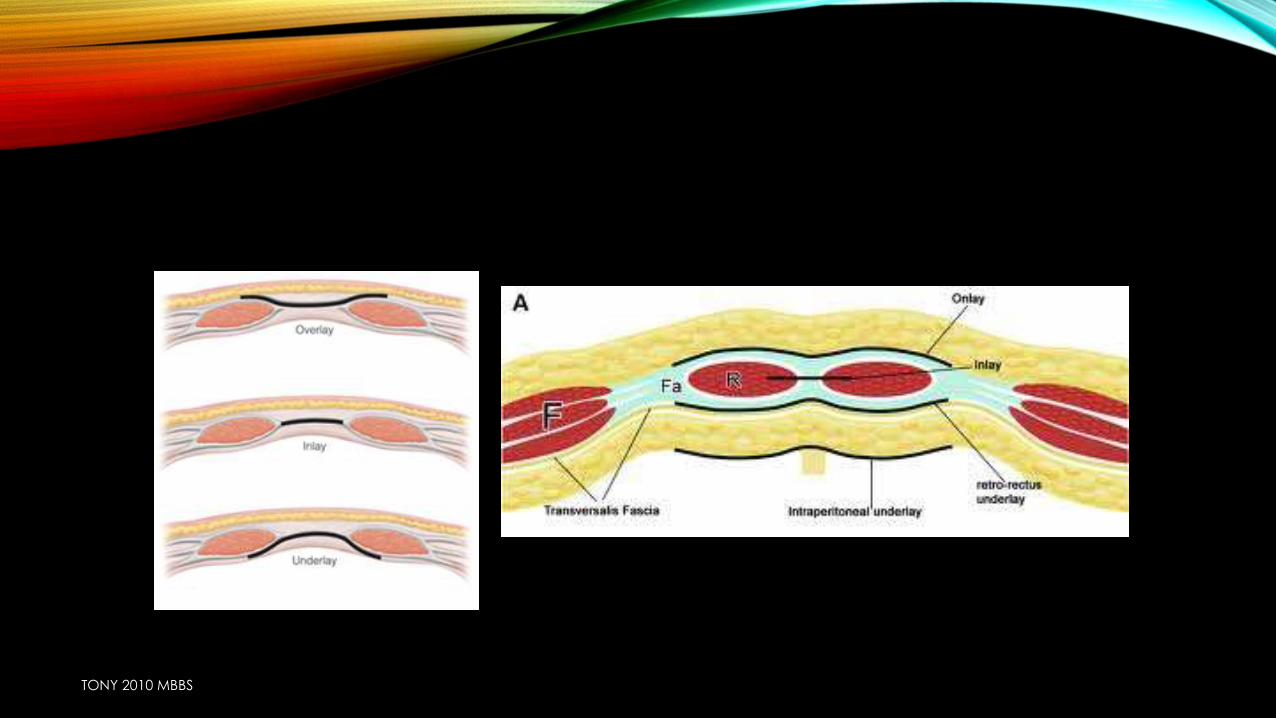
TYPES OF MESH REPAIR
• 1. In lay mesh
• 2. On lay mesh
• 3. Nyhus preperitoneal mesh repair
• 4. Stoppa procedure
• 5. Gilbert mesh repair
• 6. Lichtenstein’s method
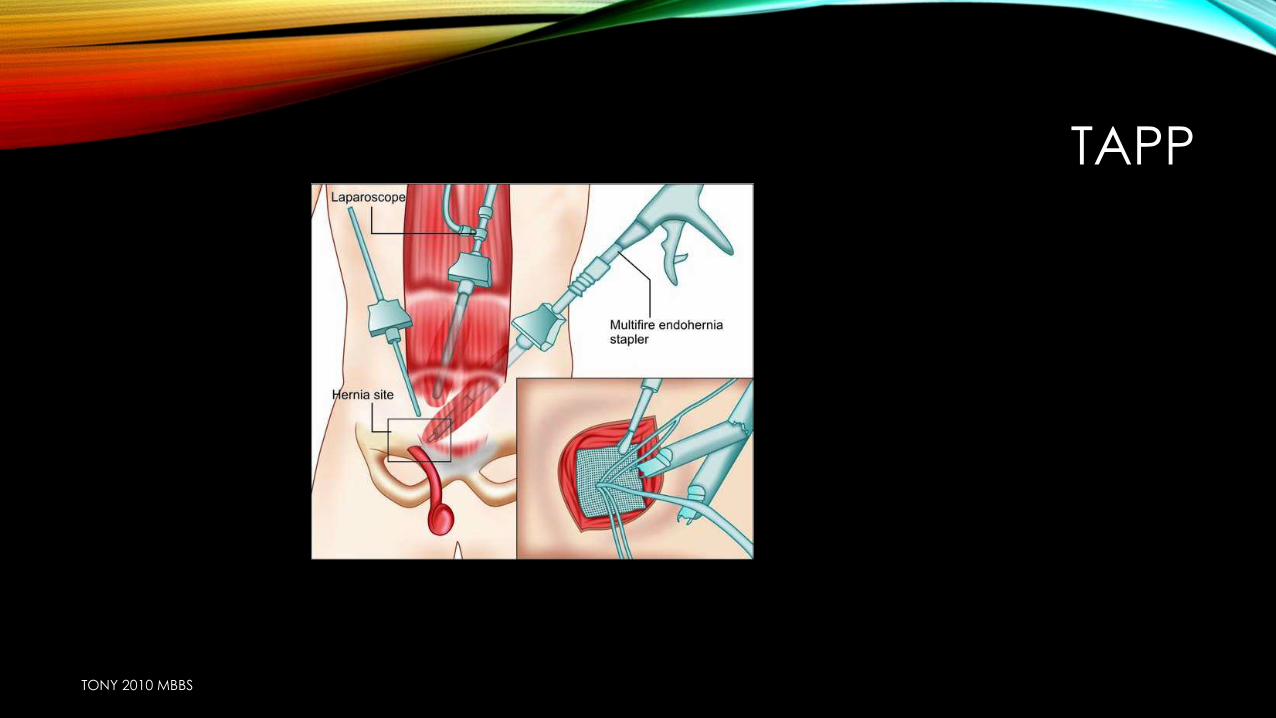
• 7. TAPP
• 8. TEP
TONY 2010 MBBS
TONY 2010 MBBS

ONLAY MESH METHOD:
• repair by placing mesh in front…..using monofilament non absorbable suture material….above to conjoint tendon & below to inguinal ligament
TONY 2010 MBBS

INLAY MESH METHOD
• mesh deep to conjoint tendon
TONY 2010 MBBS
NYHUS PREPERITONEAL MESH REPAIR
• Broad mesh is kept in the preperitoneal space in b/l direct or recurrent hernia
TONY 2010 MBBS
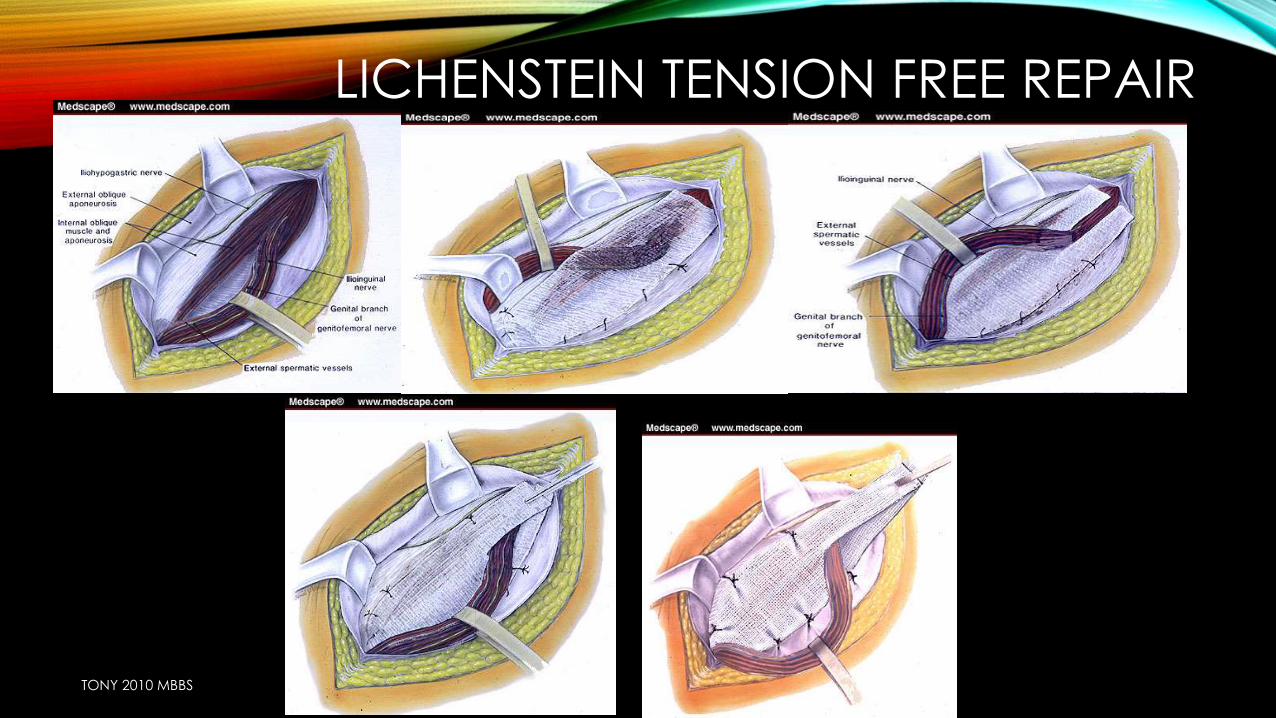
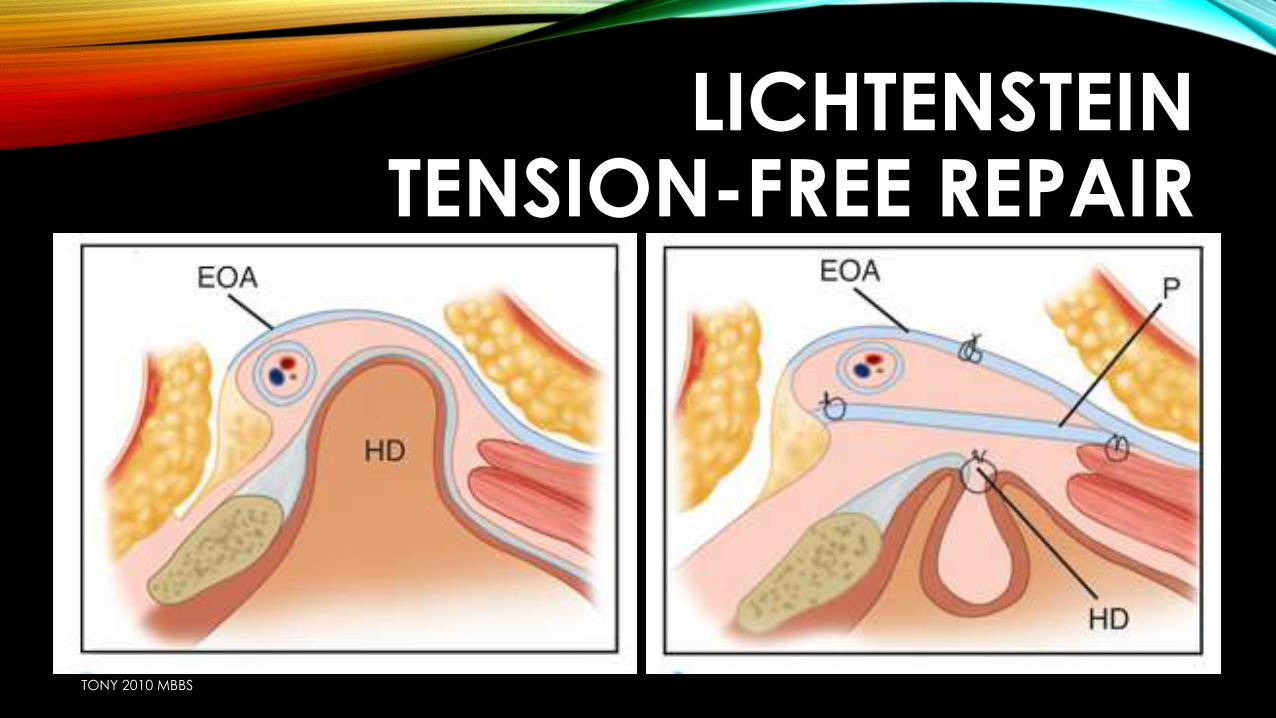
LICHTENSTEIN TENSION FREE MESH REPAIR
• Less recurrence
• Cord is covered with mesh and is sutured as in onlay method
TONY 2010 MBBS
LICHENSTEIN TENSION FREE REPAIR
TONY 2010 MBBS
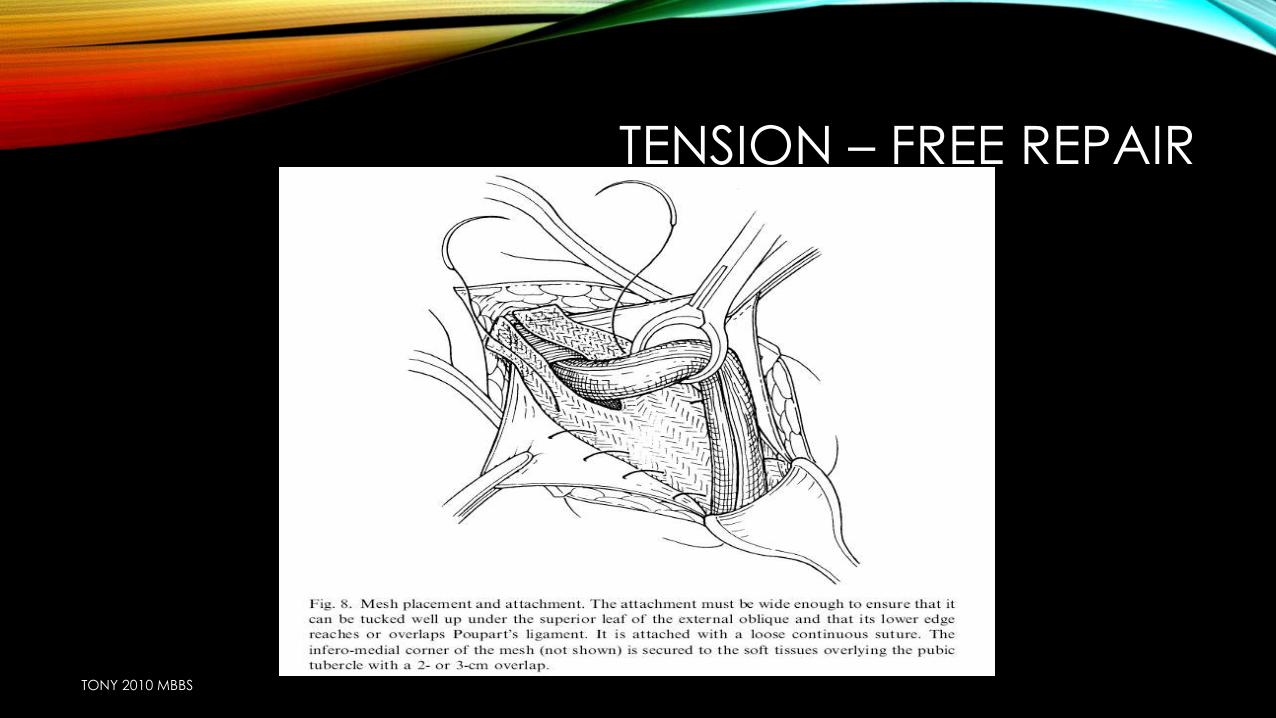
TENSION – FREE REPAIR
TONY 2010 MBBS
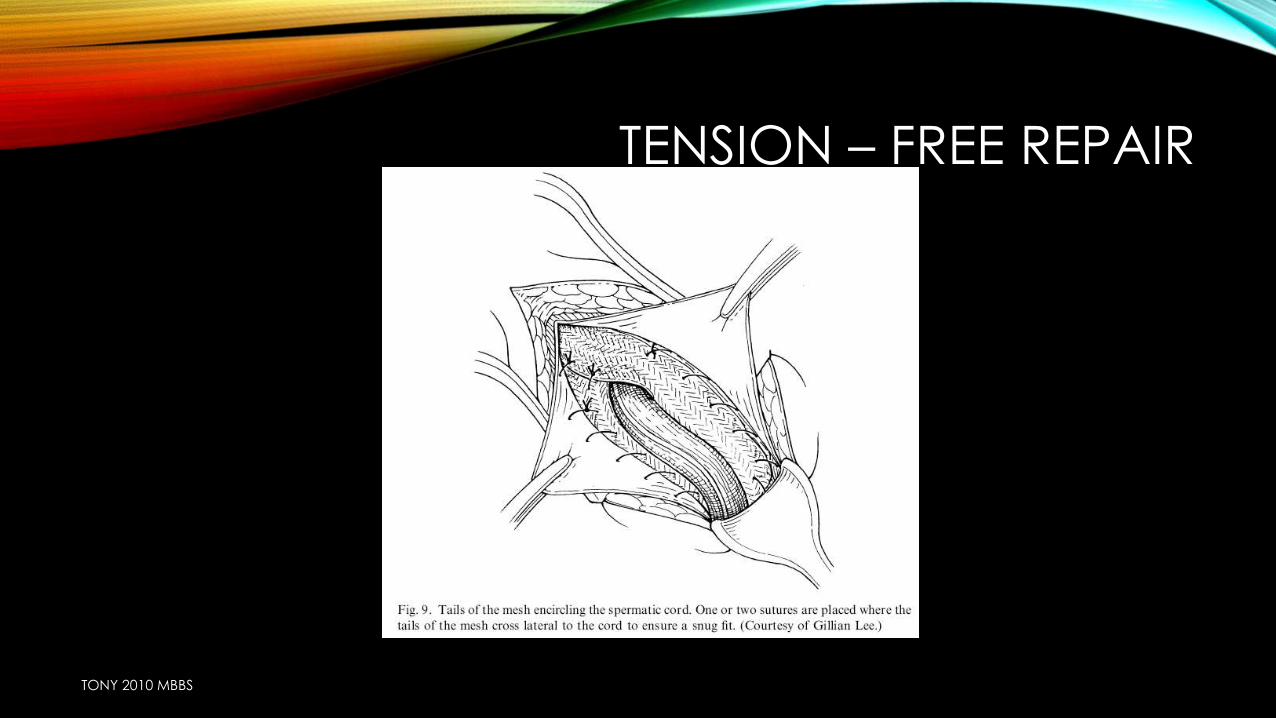
TENSION – FREE REPAIR
TONY 2010 MBBS
LICHTENSTEIN TENSION-FREE REPAIR
TONY 2010 MBBS
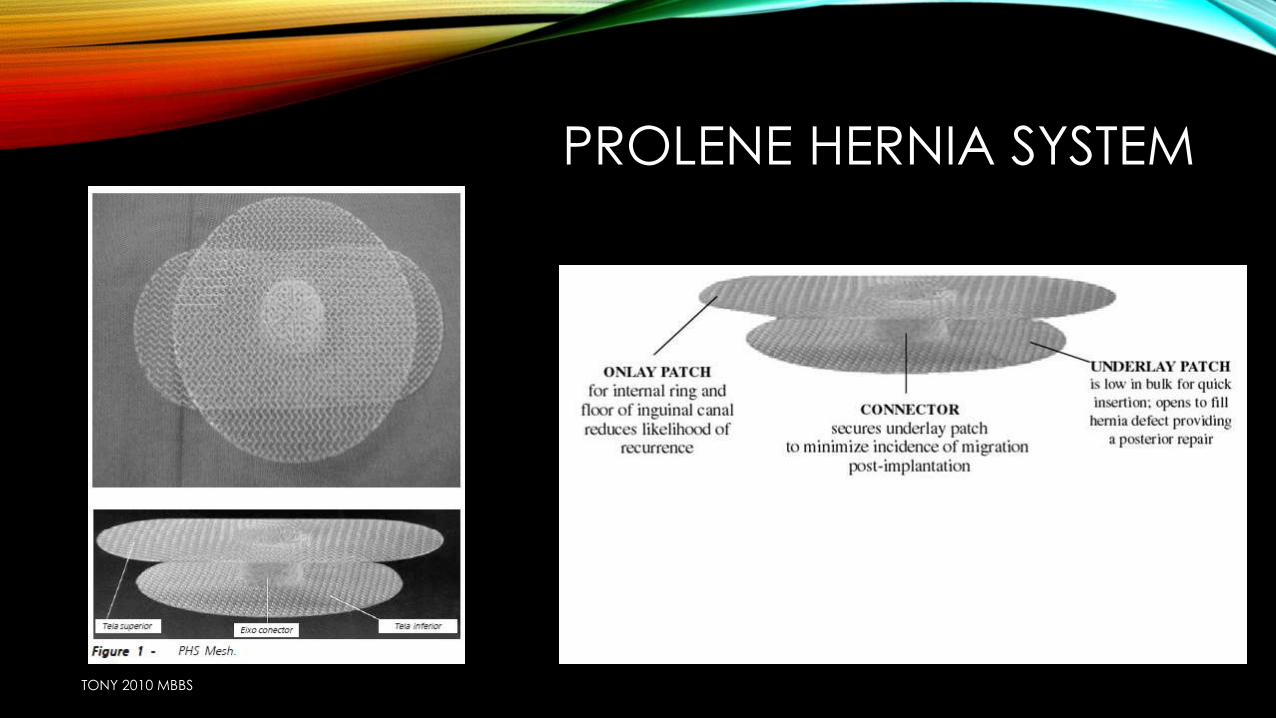
PROLENE HERNIA SYSTEM
TONY 2010 MBBS
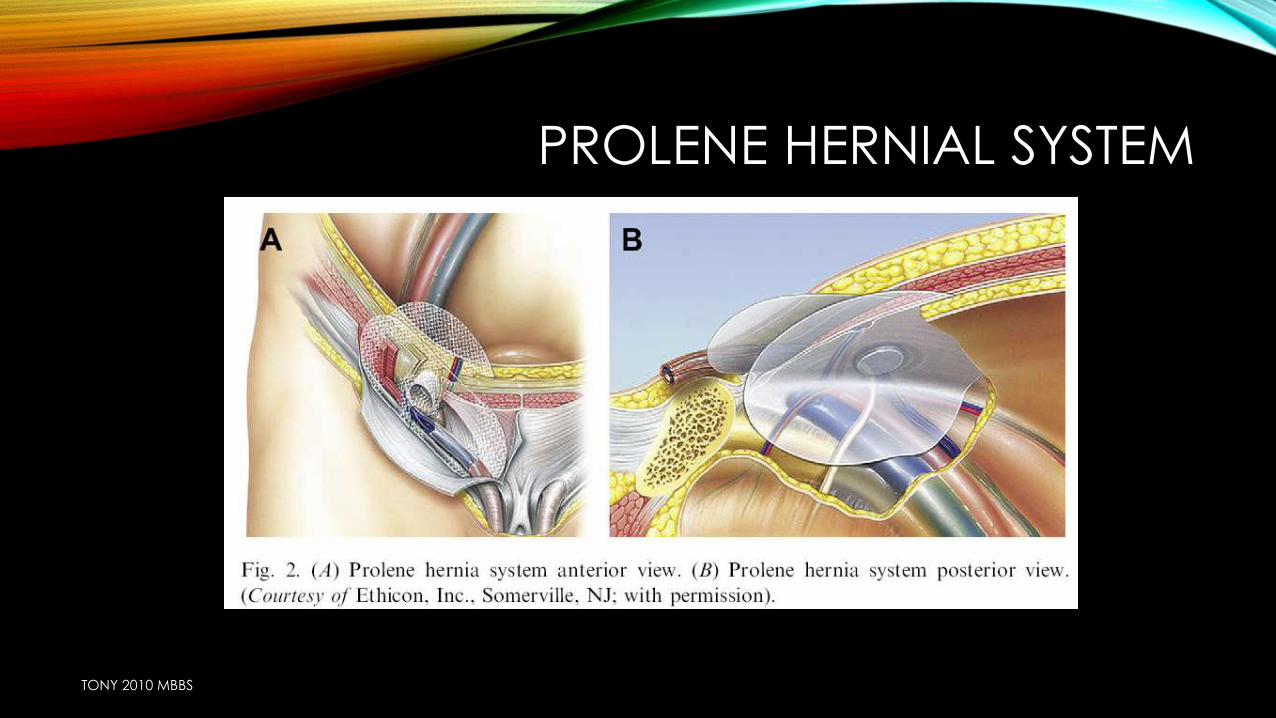
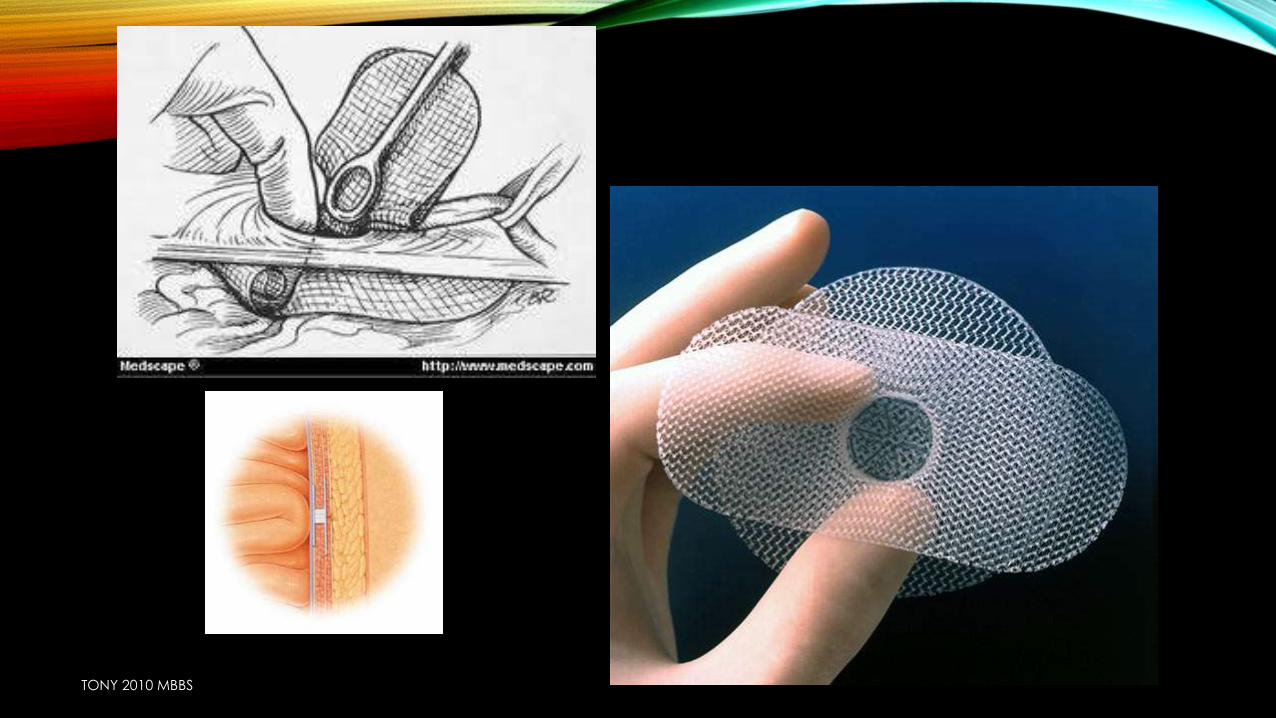
PROLENE HERNIAL SYSTEM
TONY 2010 MBBS
TONY 2010 MBBS
STOPPAS REPAIR
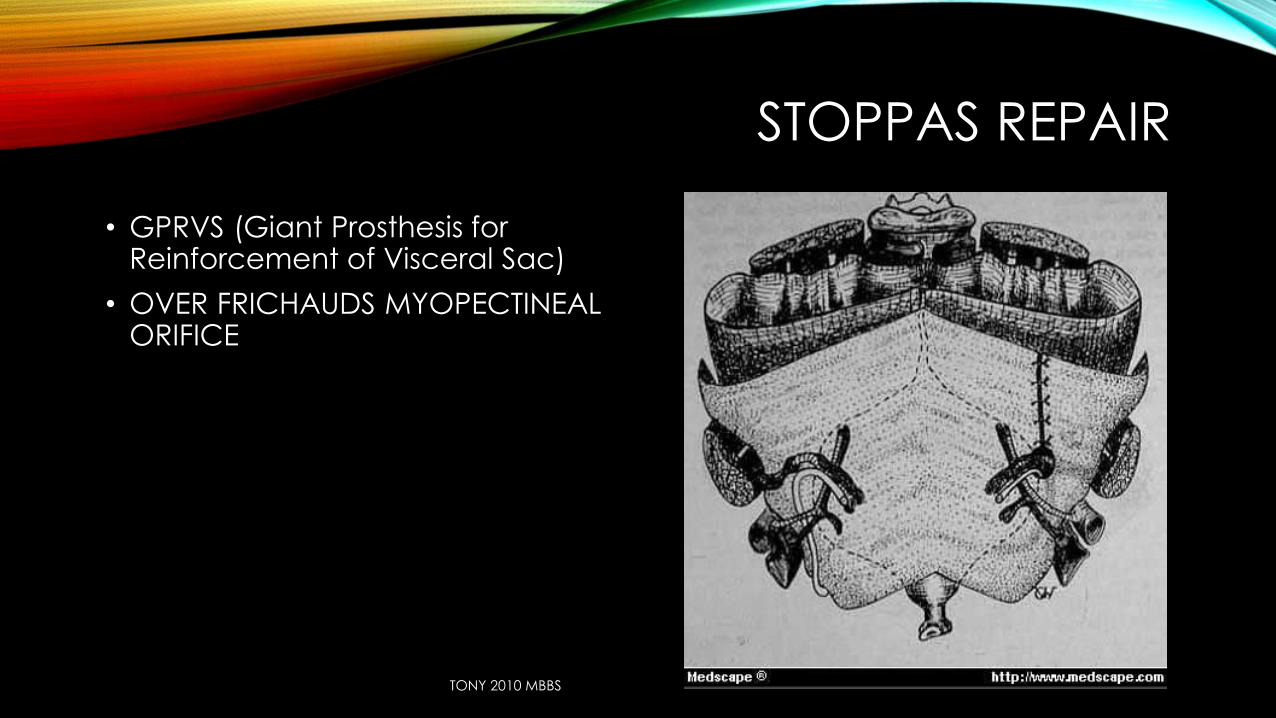
• GPRVS (Giant Prosthesis for Reinforcement of Visceral Sac)
• OVER FRICHAUDS MYOPECTINEAL ORIFICE
TONY 2010 MBBS
• The Stoppa Repair is a tension free type of hernia repair. It is performed by wrapping the lower part of the parietal peritoneum with prosthetic mesh and placing it at a preperitoneal level over Fruchauds myopectineal orifice. It was first described in 1975 by Rene Stoppa.[1] This operation is also known as giant prosthetic reinforcement of the visceral sac (GPRVS).[2]
• This technique has met particular success in the repair of bilateral hernias, large scrotal hernias, and recurrent or rerecurrent hernias in which conventional repair is difficult and carries a high morbidity and failure rate.
TONY 2010 MBBS
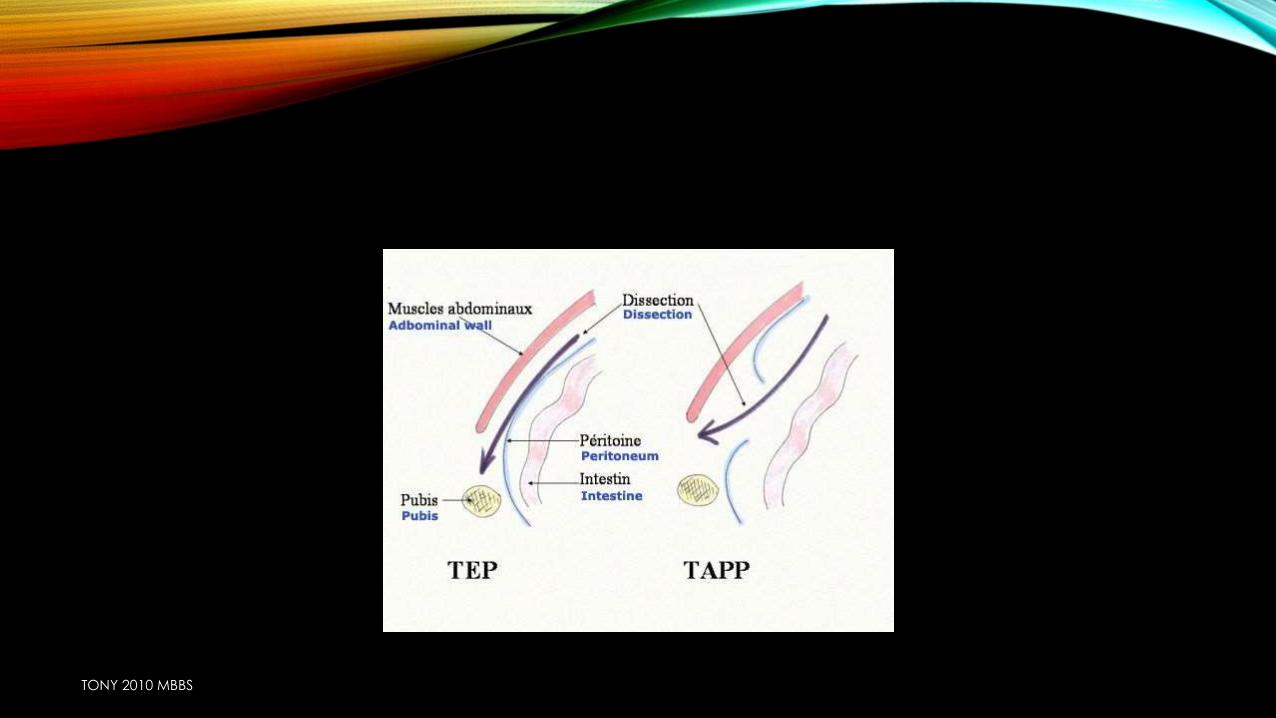
LAPAROSCOPIC HERNIA REPAIR
• Transabdominal Preperitoneal Procedure (TAPP)
• Totally Extraperitoneal (TEP) Repair
• Indications include bilateral inguinal hernia, recurring hernia, need for early recovery
TONY 2010 MBBS
TONY 2010 MBBS
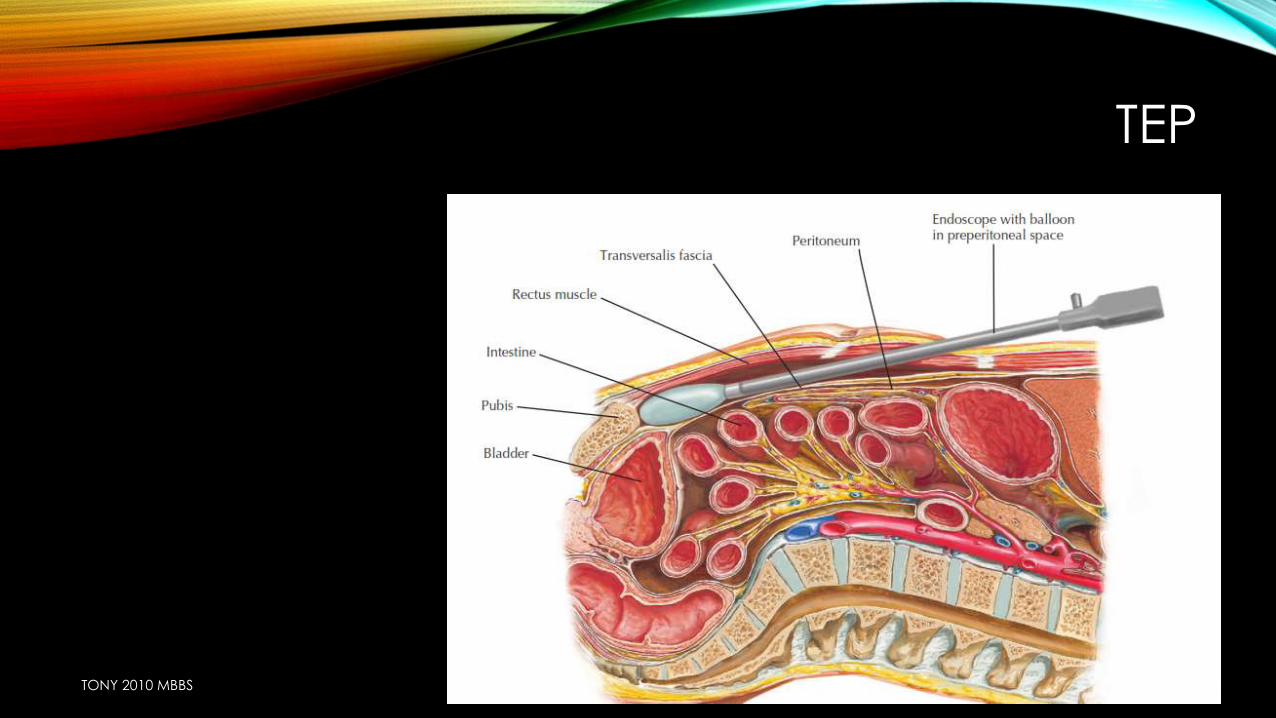
TEP
TONY 2010 MBBS
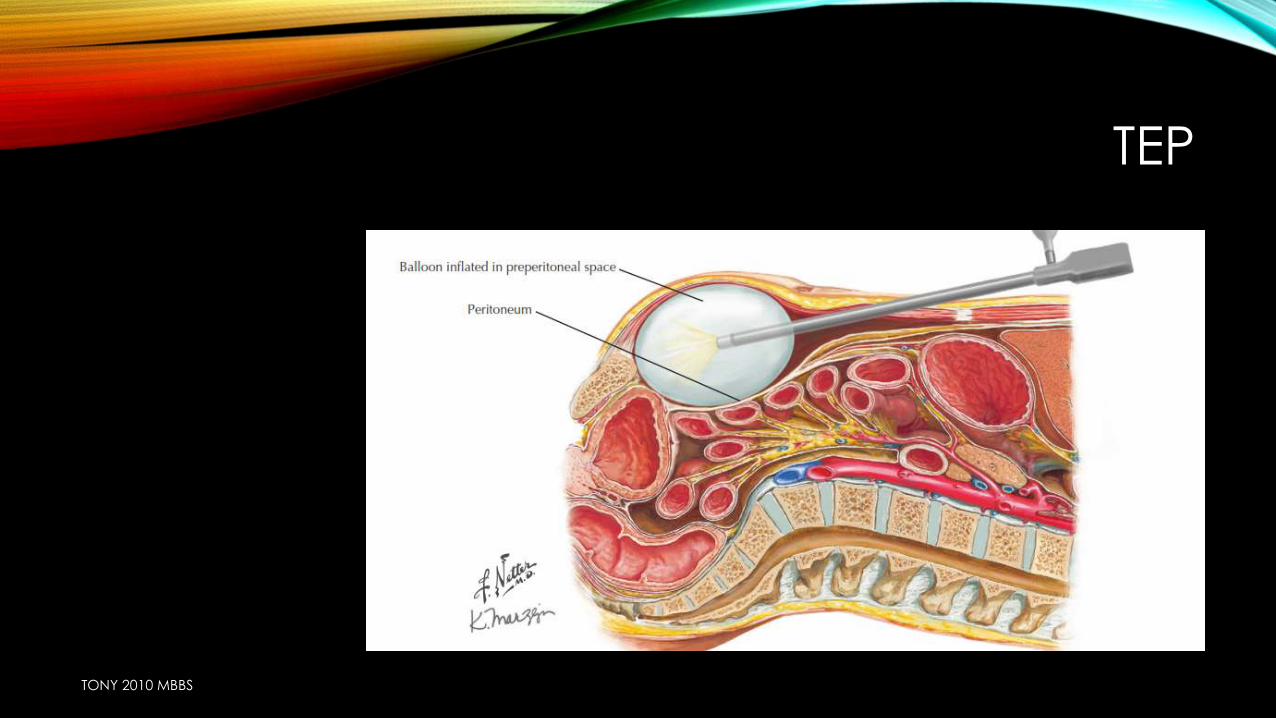
TEP
TONY 2010 MBBS
TAPP
TONY 2010 MBBS

COMPLICATIONS OF HERNIA REPAIR
IMMEDIATE
1. Injury to the blood vessels
(inferior epigastric and
femoral)
2. Injury to bowel and bladder
3. Injury to ilioinguinal and
iliohypogastric nerves
4. Injury to cord structures
EARLY
1. Urine retention
2. Hematoma
3. Infection
4. Periostitis of pubic tubercle (as
the stitch is taken from periosteum)
5. Postherniorrhaphy hydrocele
(due to obstruction of lymphatics
At deep ring when narrowed tightly)
LATE
1. Recurrence
2. Numbness over the
local region if the
nerve was cut during
surgery
TONY 2010 MBBS

DISCUSSION
TONY 2010 MBBS
INGUINAL HERNIA
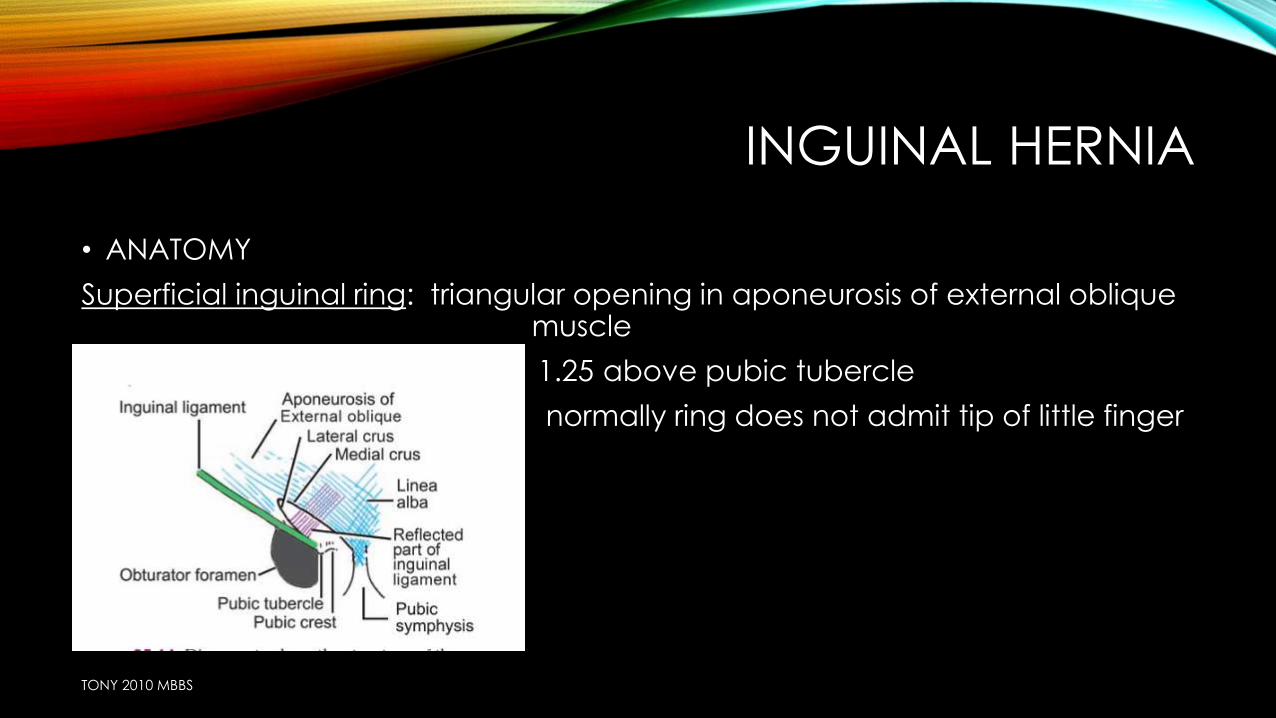
• ANATOMY
Superficial inguinal ring: triangular opening in aponeurosis of external oblique muscle
1.25 above pubic tubercle
normally ring does not admit tip of little finger
TONY 2010 MBBS
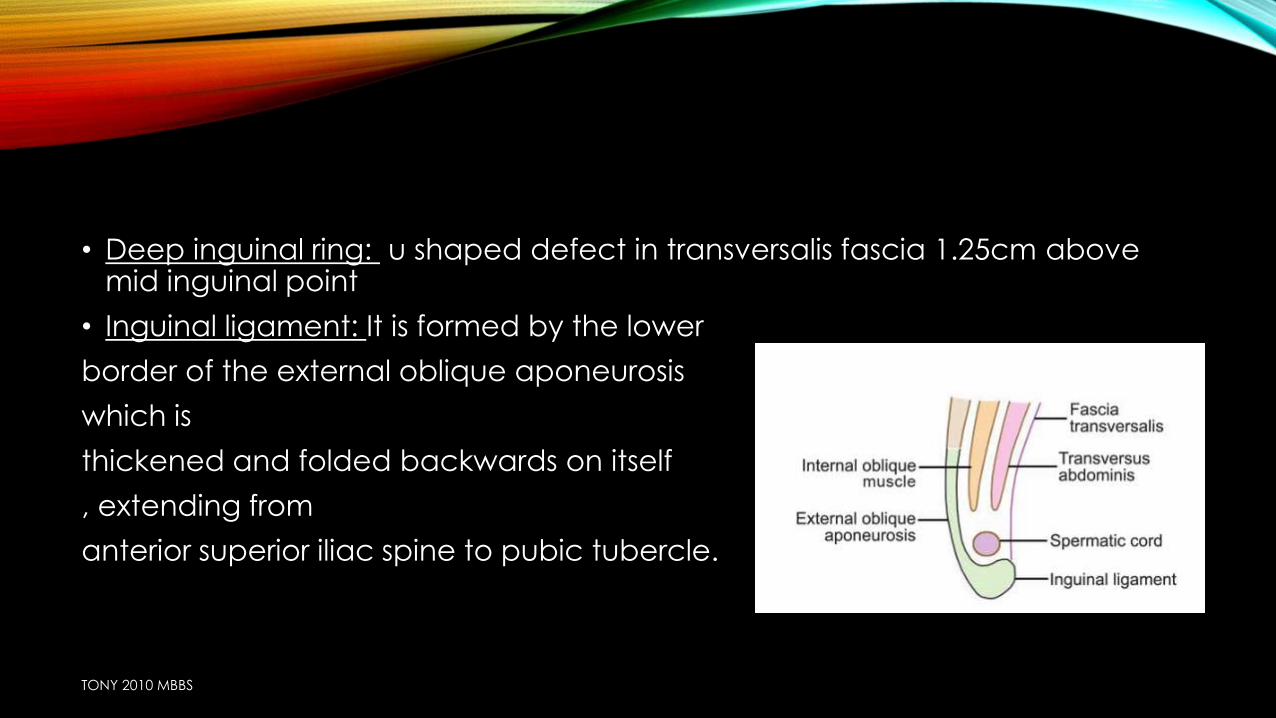
• Deep inguinal ring: u shaped defect in transversalis fascia 1.25cm above mid inguinal point
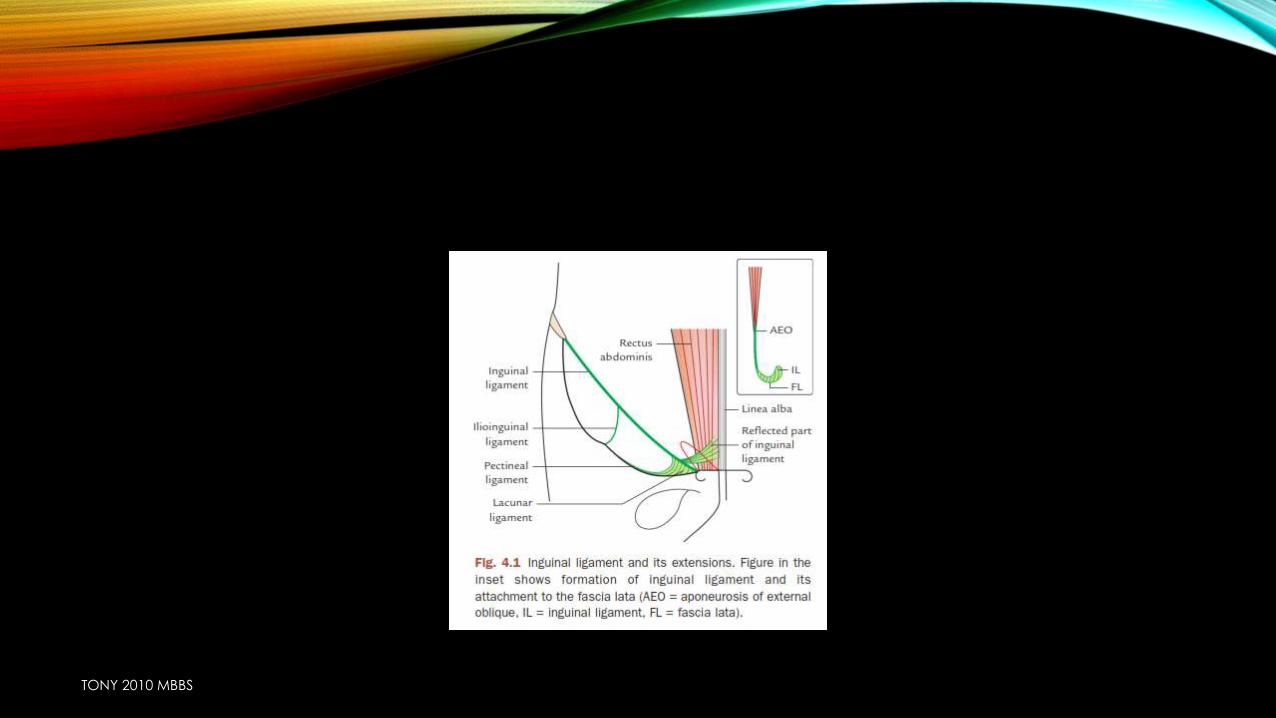
• Inguinal ligament: It is formed by the lower
border of the external oblique aponeurosis
which is
thickened and folded backwards on itself
, extending from
anterior superior iliac spine to pubic tubercle.
TONY 2010 MBBS
TONY 2010 MBBS
• Inguinal canal
• :It is an oblique passage in lower part of abdominal wall, 4 cm long, situated above the medial ½ of inguinal ligament,
• extending from deep inguinal ring to superficial inguinal ring.
TONY 2010 MBBS
BOUNDARIES
• Anteriorly: external oblique muscle
fleshy fibres of internal oblique lateral 1/3rd
skin & superficial fascia
• Posteriorly: transversalis fascia
conjoint tendon
reflected part of inguinal ligament
• Floor inguinal ligament
• Roof fibres of internal oblique
TONY 2010 MBBS
TONY 2010 MBBS
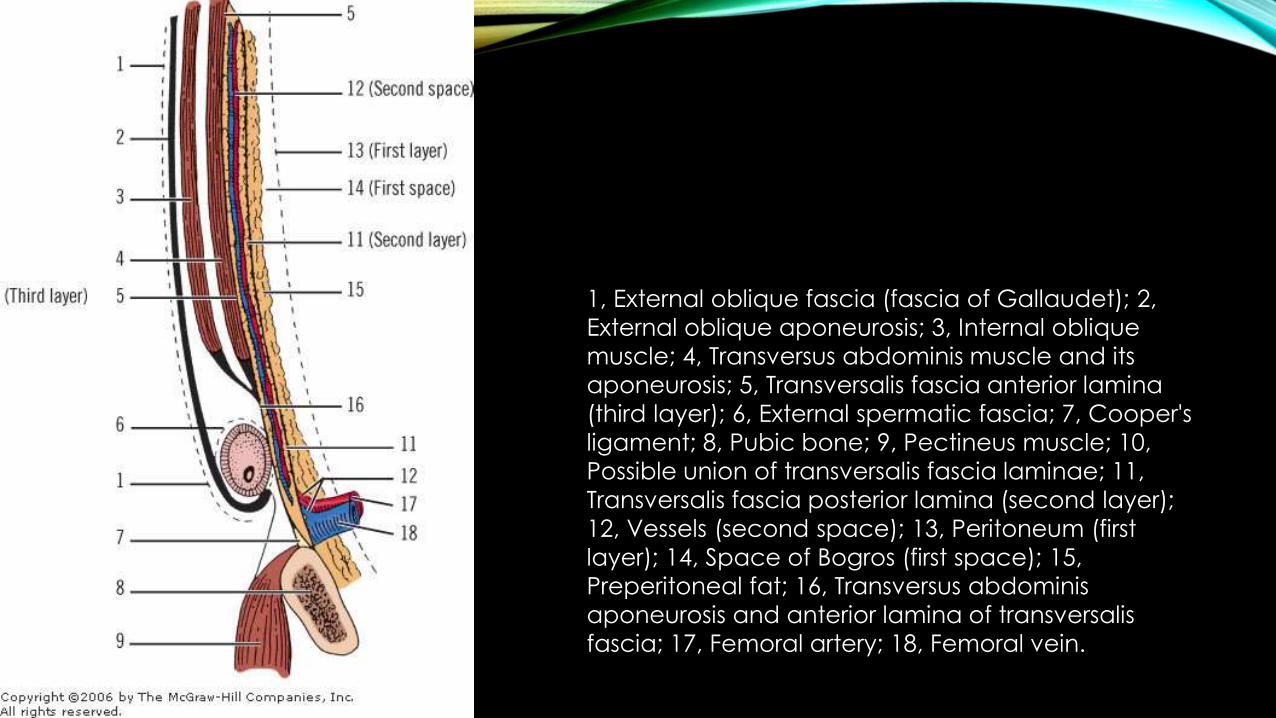
1, External oblique fascia (fascia of Gallaudet); 2,
External oblique aponeurosis; 3, Internal oblique
muscle; 4, Transversus abdominis muscle and its
aponeurosis; 5, Transversalis fascia anterior lamina
(third layer); 6, External spermatic fascia; 7, Cooper's
ligament; 8, Pubic bone; 9, Pectineus muscle; 10,
Possible union of transversalis fascia laminae; 11,
Transversalis fascia posterior lamina (second layer);
12, Vessels (second space); 13, Peritoneum (first
layer); 14, Space of Bogros (first space); 15,
Preperitoneal fat; 16, Transversus abdominis
aponeurosis and anterior lamina of transversalis
fascia; 17, Femoral artery; 18, Femoral vein.
TONY 2010 MBBS
TONY 2010 MBBS
CONTENTS OF INGUINALCANAL
SPERMATIC CORD IN MALE
• Vas deferens
• Artery to vas
• Testicular & cremasteric artery
• Pampiniform plexus
• Remains of processus vaginalis
• Genital branch of genitofemoral nerve
• Sympathetic plexus
• lymphatics
ROUND LIGAMENT IN FEMALE
ILIO INGUINAL NERVE
TONY 2010 MBBS
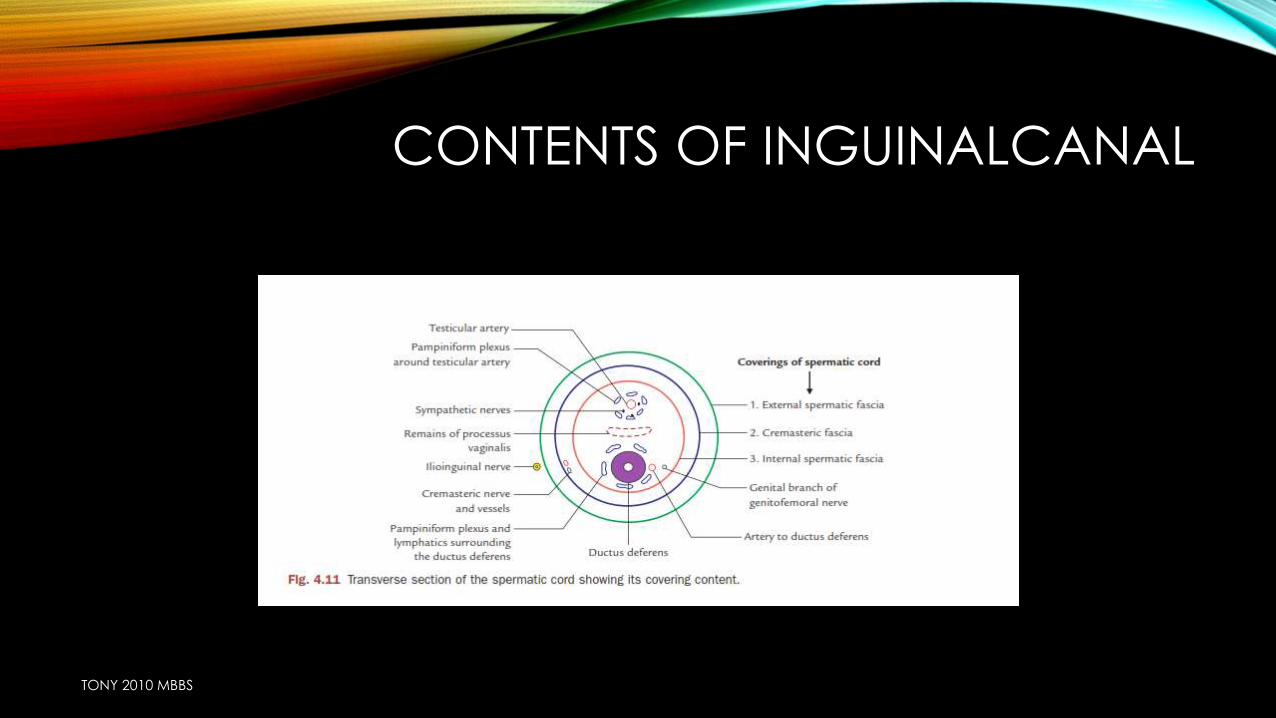
CONTENTS OF INGUINALCANAL
TONY 2010 MBBS
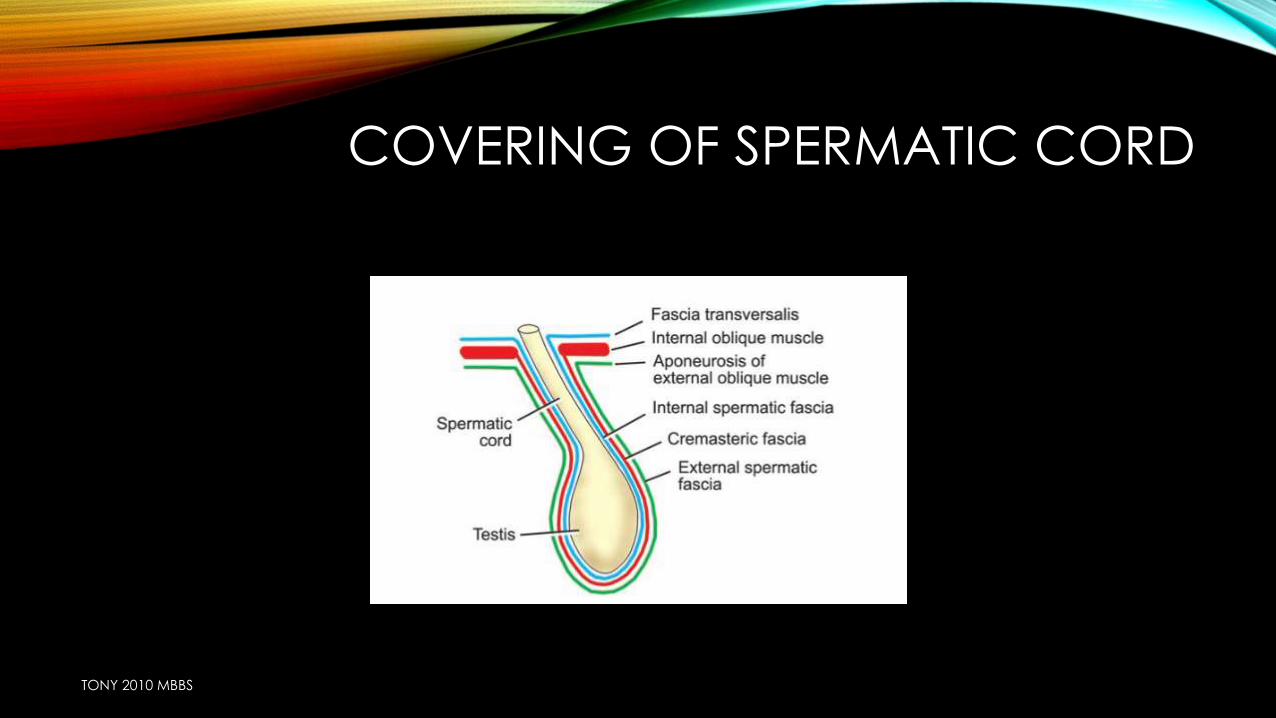
COVERING OF SPERMATIC CORD
TONY 2010 MBBS
DEFENCE MECHANISM OF INGUINAL CANAL
• Obliquity of inguinal canal
• Arching of conjoint tendon
• Shutter mechanism of internal oblique
• Ball valve mechanism due to contraction of cremasteric muscle
• Slit valve mechanism due to contraction of external oblique muscle
• hormone
TONY 2010 MBBS
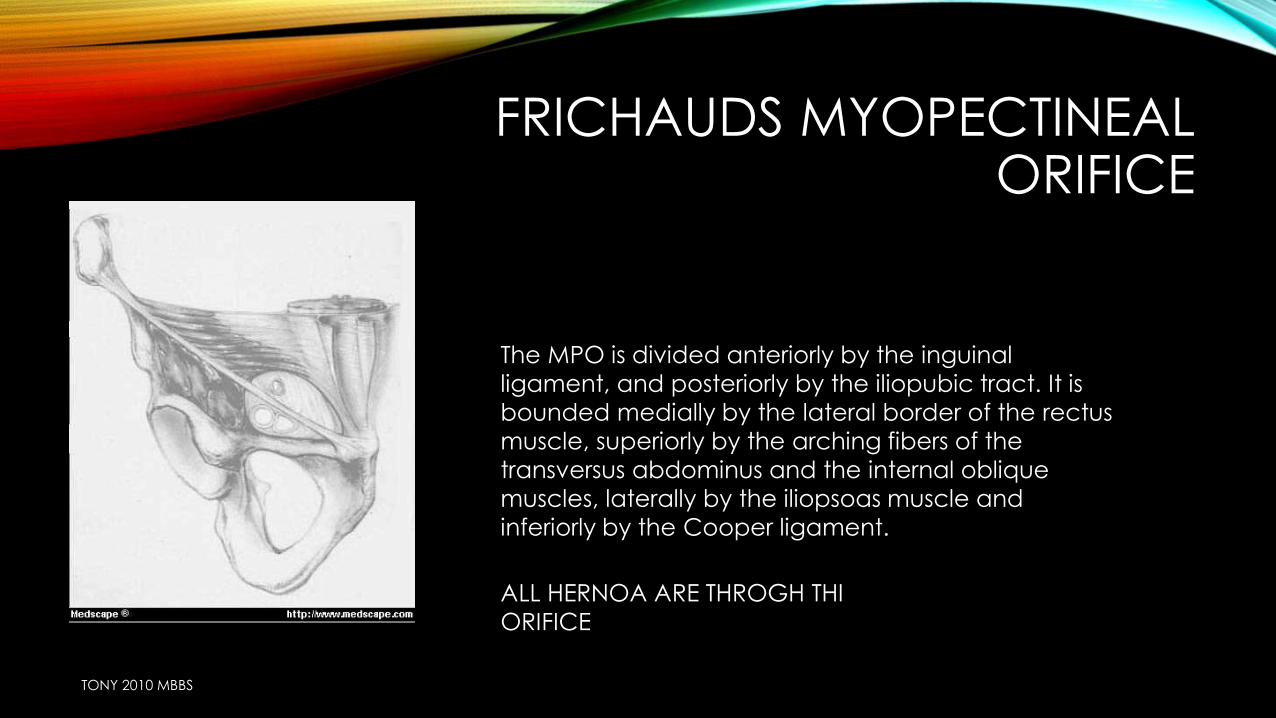
FRICHAUDS MYOPECTINEAL ORIFICE
The MPO is divided anteriorly by the inguinal
ligament, and posteriorly by the iliopubic tract. It is
bounded medially by the lateral border of the rectus
muscle, superiorly by the arching fibers of the
transversus abdominus and the internal oblique
muscles, laterally by the iliopsoas muscle and
inferiorly by the Cooper ligament.
ALL HERNOA ARE THROGH THI
ORIFICE
TONY 2010 MBBS
TONY 2010 MBBS
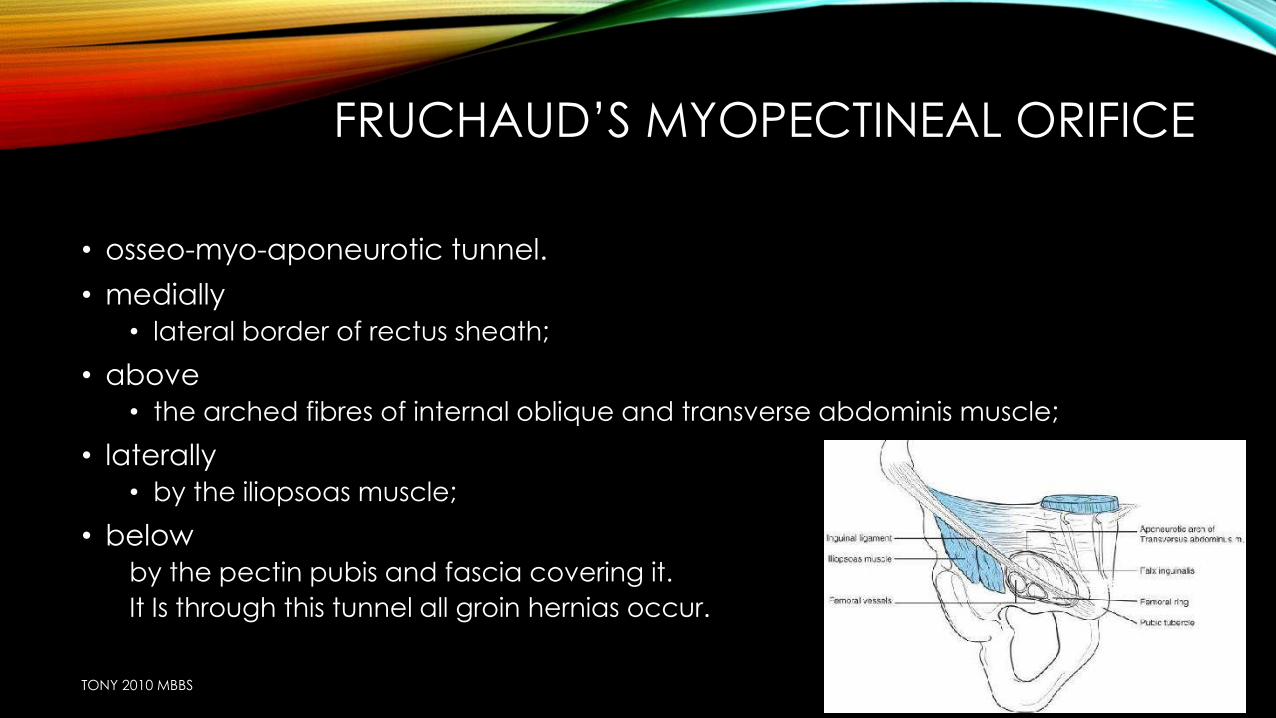
FRUCHAUD’S MYOPECTINEAL ORIFICE
• osseo-myo-aponeurotic tunnel.
• medially
• lateral border of rectus sheath;
• above
• the arched fibres of internal oblique and transverse abdominis muscle;
• laterally
• by the iliopsoas muscle;
• below
by the pectin pubis and fascia covering it.
It Is through this tunnel all groin hernias occur.
TONY 2010 MBBS
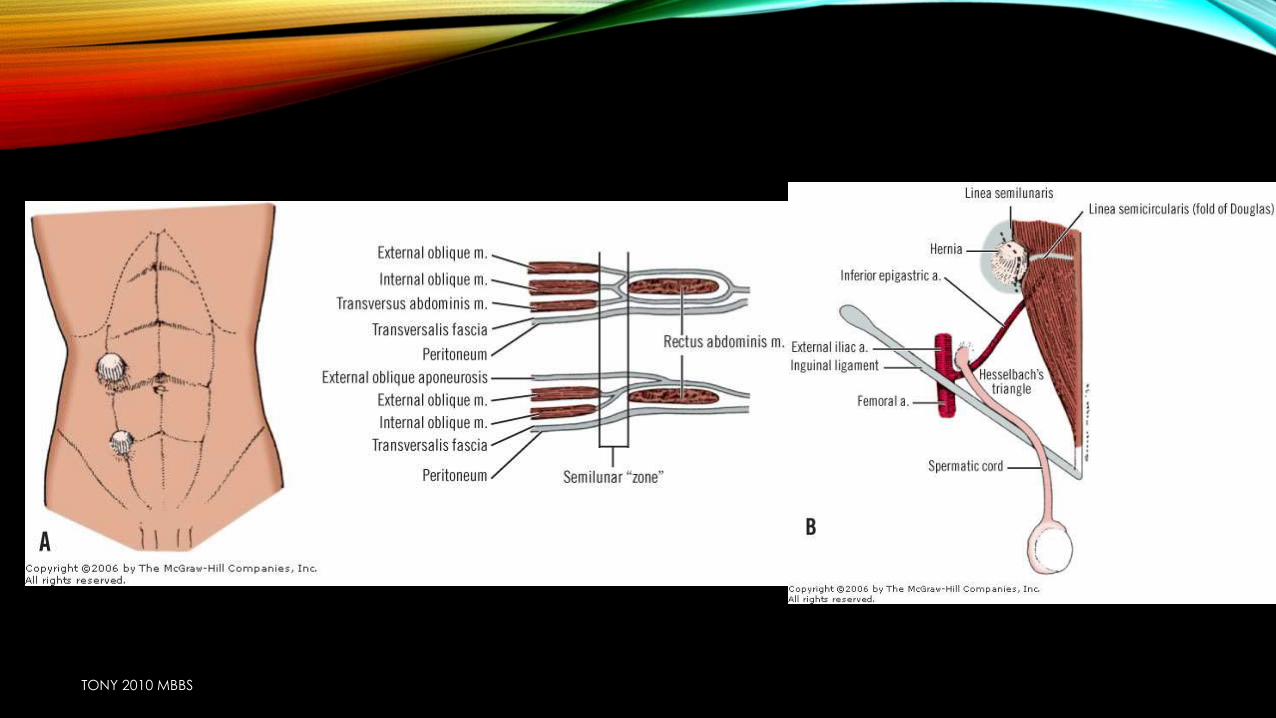
HASSELBACHS TRIANGLE
TONY 2010 MBBS
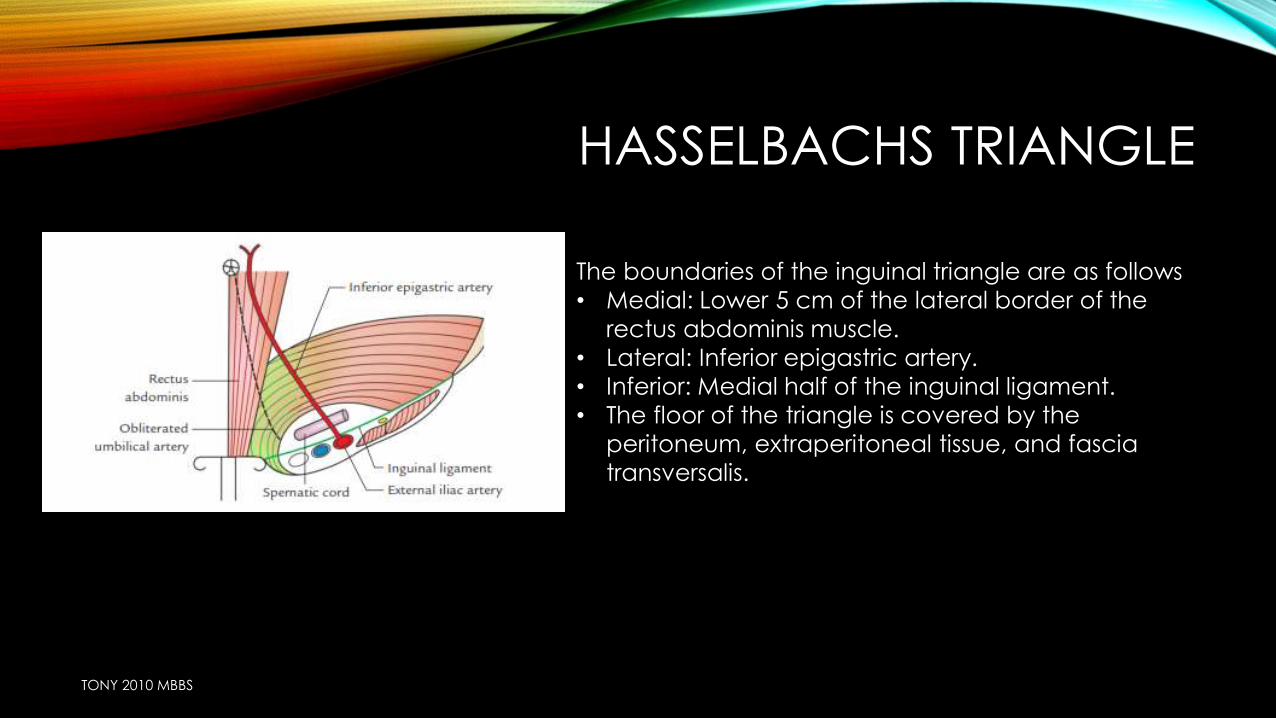
The boundaries of the inguinal triangle are as follows
• Medial: Lower 5 cm of the lateral border of the
rectus abdominis muscle.
• Lateral: Inferior epigastric artery.
• Inferior: Medial half of the inguinal ligament.
• The floor of the triangle is covered by the
peritoneum, extraperitoneal tissue, and fascia
transversalis.
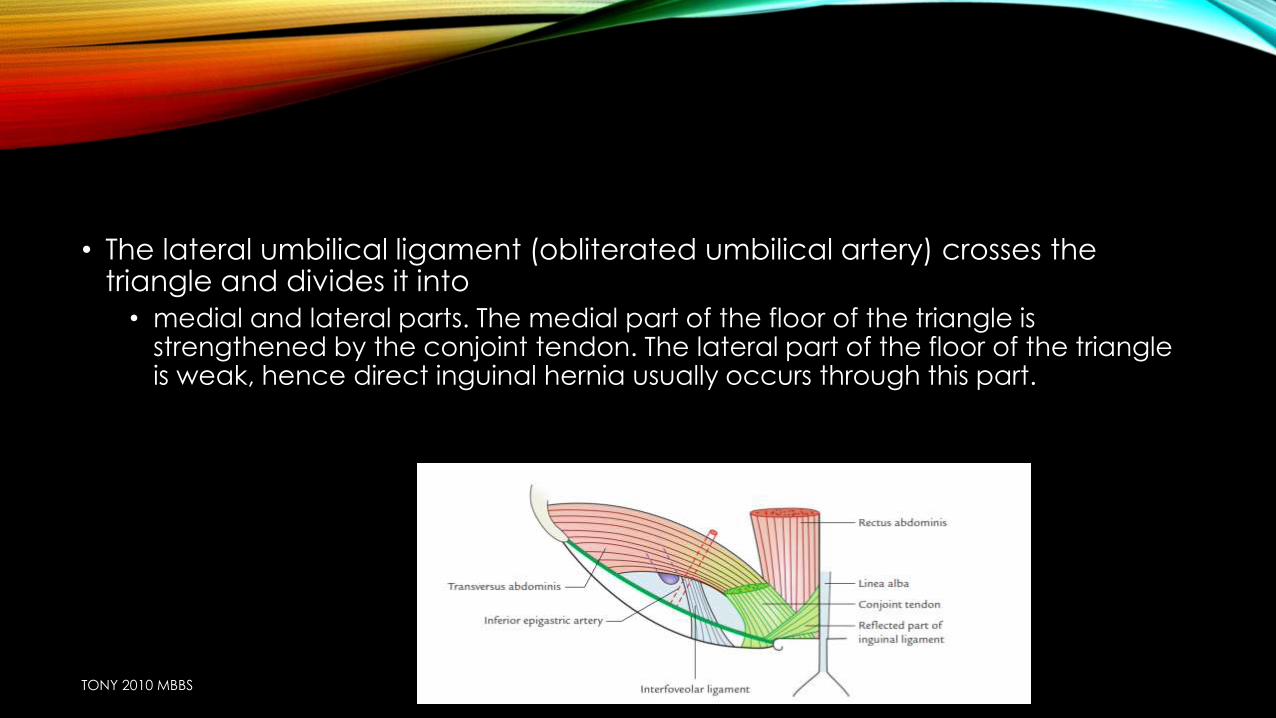
• The lateral umbilical ligament (obliterated umbilical artery) crosses the triangle and divides it into
• medial and lateral parts. The medial part of the floor of the triangle is strengthened by the conjoint tendon. The lateral part of the floor of the triangle is weak, hence direct inguinal hernia usually occurs through this part.
TONY 2010 MBBS
ETIOLOGY
• STRAININGC/C CONSTIPATION (HABITUAL,STRICTURE)
URINARY PROBLEMS OLD AGE =BPH, Ca prostate
YOUNG AGE=STRICTURE URETHRA
VERY YOUNG=PHIMOSIS,MEATAL STENOSIS
LIFTING OF HEAVY WEIGHT
• C/C COUGH =T.B, B.A, C/C BRONCHITIS
• OBESITY
• PREGNANCY
• SMOKING
• ASCITES
TONY 2010 MBBS
ETIOLOGY
• APPENDICECTOMY DESTROY ILIO INGUINAL NDIRECT INGUINALHERNIA
McBURNEYS INCISION
• FAMILIAL COLLAGEN DISORDER
• CONGENITAL PREFORMED SAC (REMAINS OF PROCESSUS VAGINALIS)
TONY 2010 MBBS
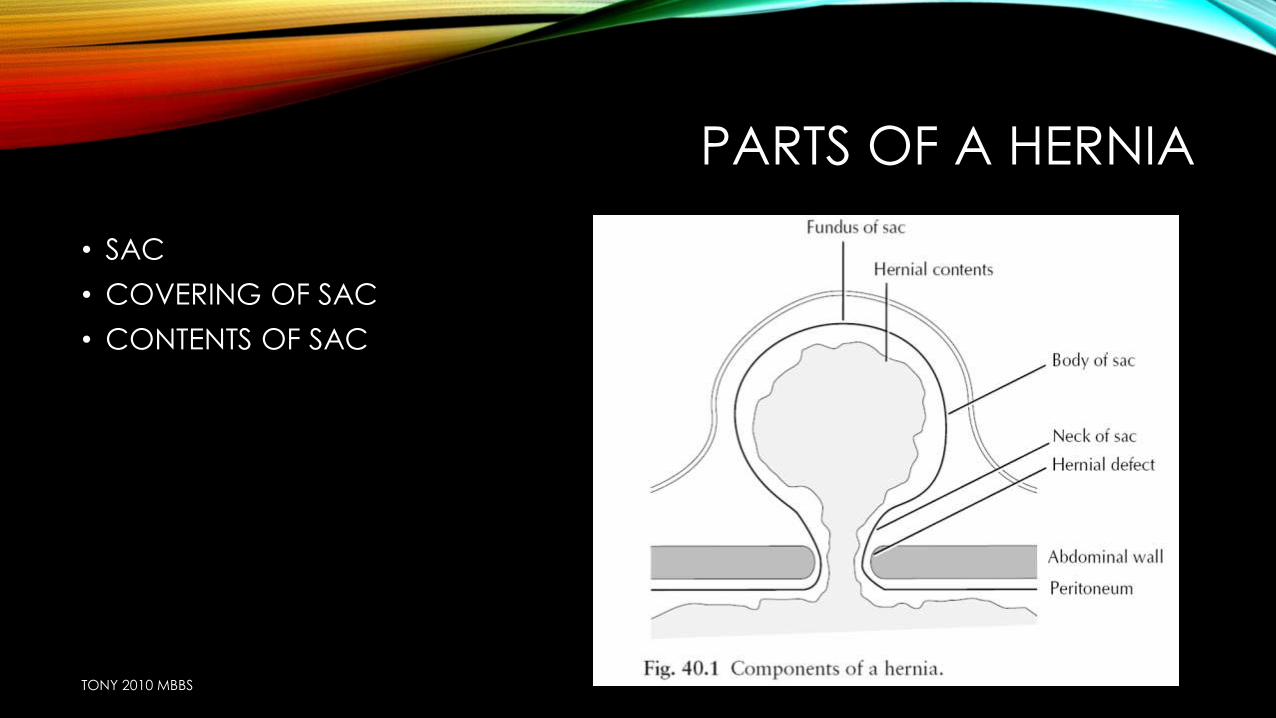
PARTS OF A HERNIA
• SAC
• COVERING OF SAC
• CONTENTS OF SAC
TONY 2010 MBBS
SAC
• A DIVERTICULUM OF PERITONEUM WITH MOUTH
NECK
BODY
FUNDUS
• NECK IS NARROW IN CASE OF INDIRECT WIDE IN CASE OF DIRECT
• HERNIA WITHOUT NECK: HERNIA WITH A WIDE MOUTH ,DIRCT HERNIA,INCISIONAL HERNIA
• SAC IS THIN IN INFANTS & CHILD THICK IN LONG STANDING & DIRECT HERNIA
• HERNIA WITHOUT SAC: EPIGASTRIC HERNIA(Protrusion of extra peritoneal pad of fat)
TONY 2010 MBBS
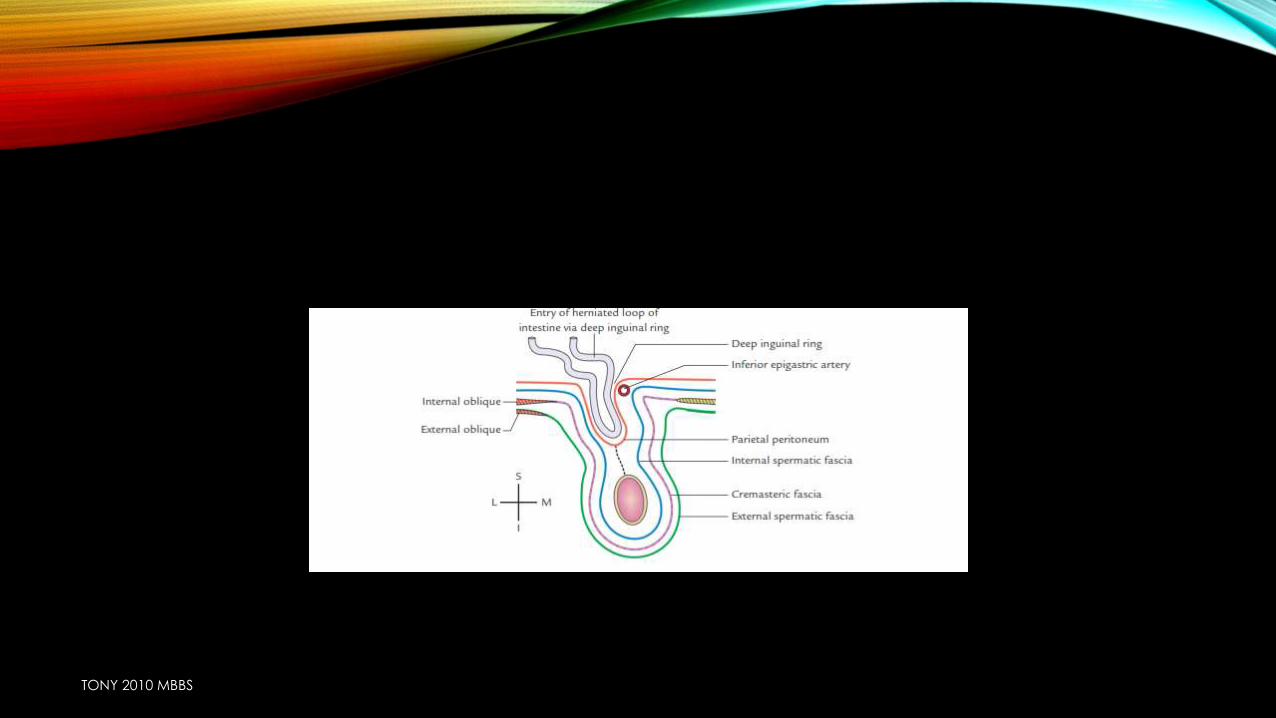
COVERING OF SAC
• LAYERS OF ABDOMINAL WALL
TONY 2010 MBBS
CONTENTS OF SAC
• OMENTOCELE: omentum….easy to reduce initially,…but difficult later
• ENTEROCELE: usuaslly SI,….difficult to reduce initially…easy later
• RICHTERS HERNIA :a portion of circumference of bowel
• LITTRE’S HERNIA: meckels diverticulum
• CYSTOCELE :bladder
• Ovary,fallopian tube
• Fluid :ascitic, blood from strangulated hernia, from congested bowel
TONY 2010 MBBS
TONY 2010 MBBS
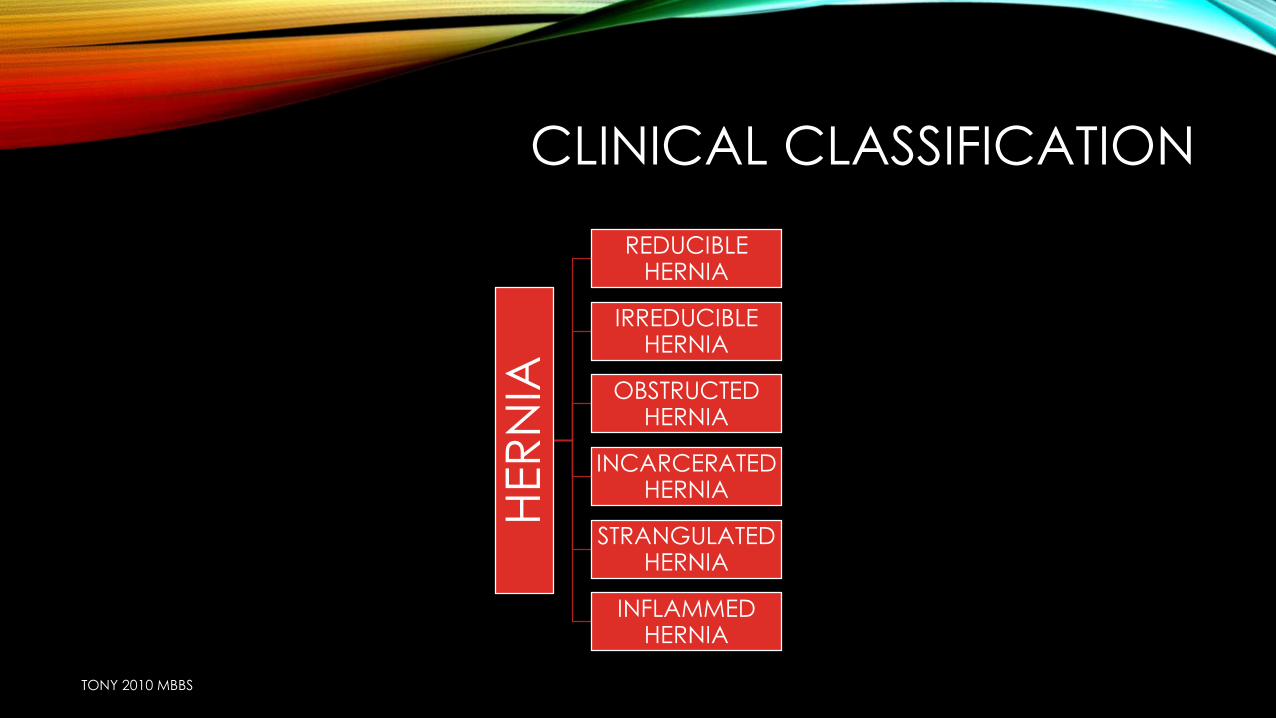
CLINICAL CLASSIFICATION
HER
NIA
REDUCIBLE HERNIA
IRREDUCIBLE HERNIA
OBSTRUCTED HERNIA
INCARCERATED HERNIA
STRANGULATED HERNIA
INFLAMMED HERNIA
TONY 2010 MBBS
CLINICAL CLASSIFICATION
• REDUCIBLE HERNIA contents can be reduced by the patient or surgeon
expansile impulse on coughing
TONY 2010 MBBS
• IRREDUCIBLE HERNIA can’t be reduced …due to adhesions b/w contents and sac…or due to crowding
irreducibility + no other symptoms}OMENTOCELE
Irreducibility predisposes to strangulation
TONY 2010 MBBS
OBSTRUCTED HERNIA : bowel is obstructed…but blood supply is good
TONY 2010 MBBS
INCARCERATED HERNIA
that the lumen of that portion of the colon
occupying a hernial sac is blocked with faeces. In this case, the
scybalous contents of the bowel should be capable of being
indented with the finger, like putty.
In incarcerated hernia, sac and contents are densely
adherent to each other (contents are fixed to sac). It
is always irreducible; often obstructed but may not
be strangulated.
TONY 2010 MBBS
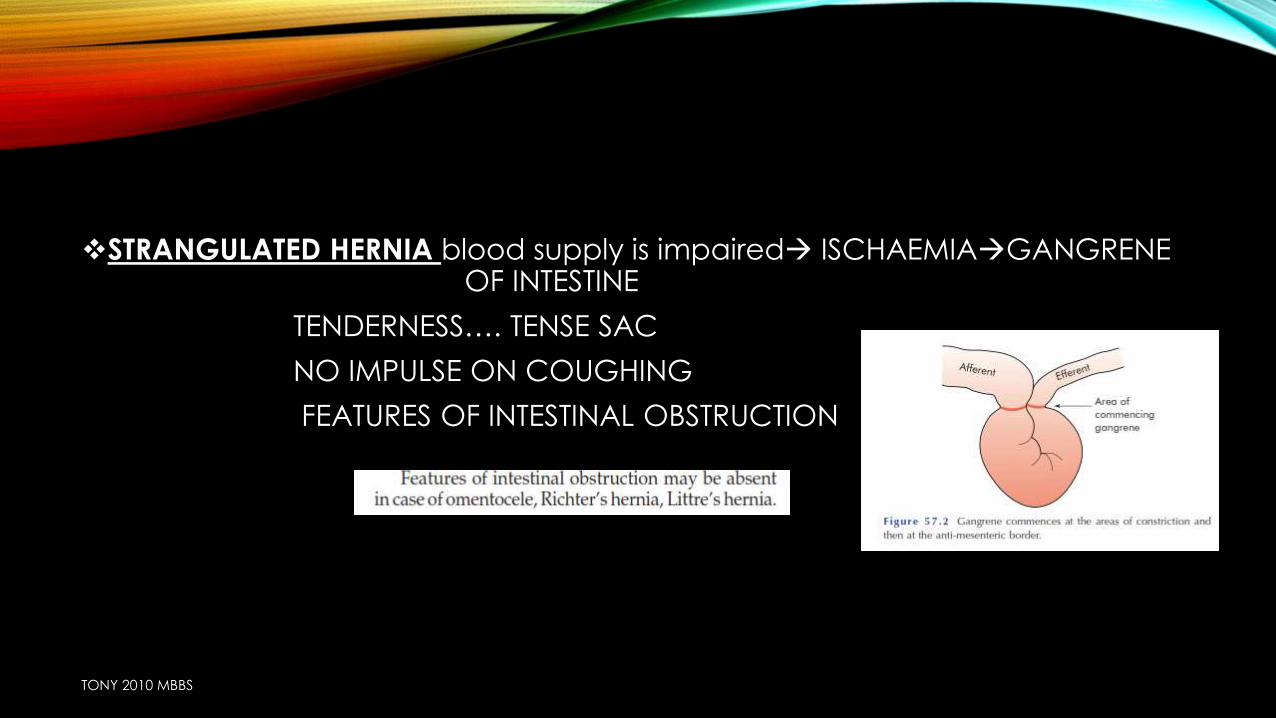
STRANGULATED HERNIA blood supply is impaired ISCHAEMIAGANGRENE OF INTESTINE
TENDERNESS…. TENSE SAC
NO IMPULSE ON COUGHING
FEATURES OF INTESTINAL OBSTRUCTION
TONY 2010 MBBS
• INFLAMMED HERNIA
inflammation of contents of hernia sac
appendicitis,salpingitis
TONY 2010 MBBS
CLASSIFICATION
hernia
congenital
acquired
TONY 2010 MBBS
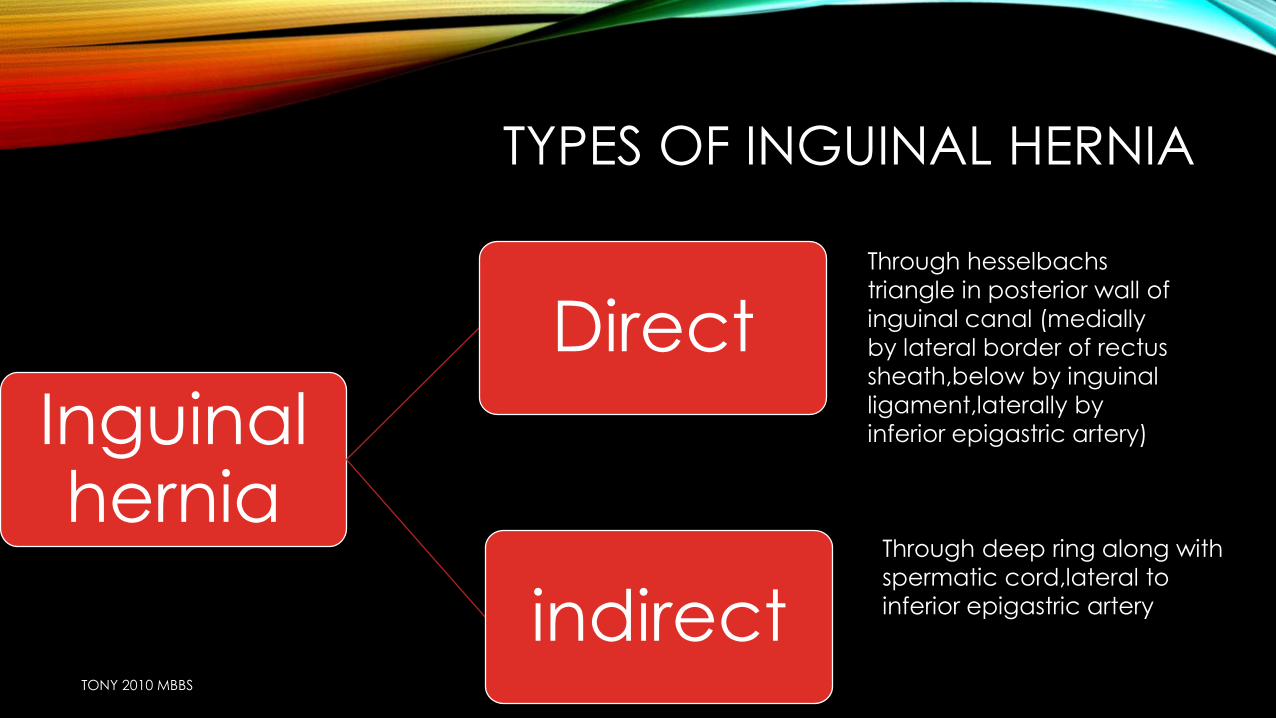
TYPES OF INGUINAL HERNIA
Inguinal hernia
Direct
indirect
Through hesselbachs
triangle in posterior wall of
inguinal canal (medially
by lateral border of rectus
sheath,below by inguinal
ligament,laterally by
inferior epigastric artery)
Through deep ring along with
spermatic cord,lateral to
inferior epigastric artery
TONY 2010 MBBS
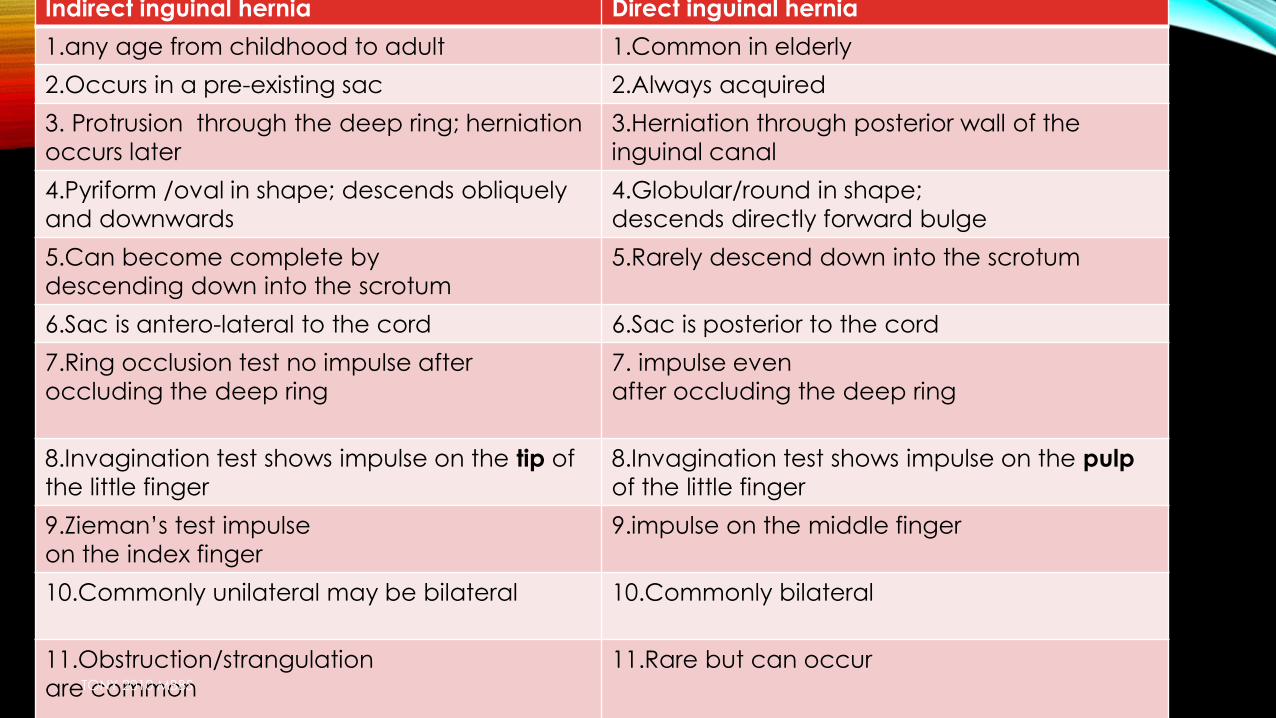
Indirect inguinal hernia Direct inguinal hernia
1.any age from childhood to adult 1.Common in elderly
2.Occurs in a pre-existing sac 2.Always acquired
3. Protrusion through the deep ring; herniation
occurs later
3.Herniation through posterior wall of the
inguinal canal
4.Pyriform /oval in shape; descends obliquely
and downwards
4.Globular/round in shape;
descends directly forward bulge
5.Can become complete by
descending down into the scrotum
5.Rarely descend down into the scrotum
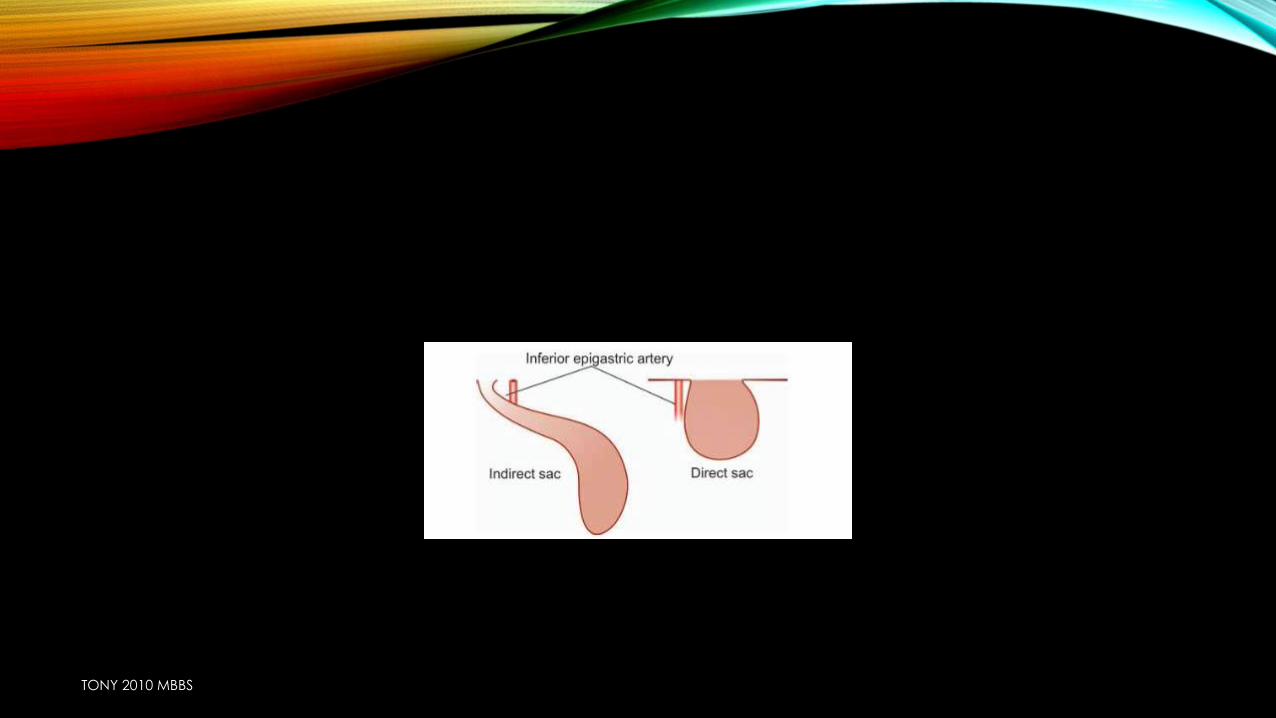
6.Sac is antero-lateral to the cord 6.Sac is posterior to the cord
7.Ring occlusion test no impulse after
occluding the deep ring
7. impulse even
after occluding the deep ring
8.Invagination test shows impulse on the tip of
the little finger
8.Invagination test shows impulse on the pulp
of the little finger
9.Zieman’s test impulse
on the index finger
9.impulse on the middle finger
10.Commonly unilateral may be bilateral 10.Commonly bilateral
11.Obstruction/strangulation
are common
11.Rare but can occurTONY 2010 MBBS
TONY 2010 MBBS
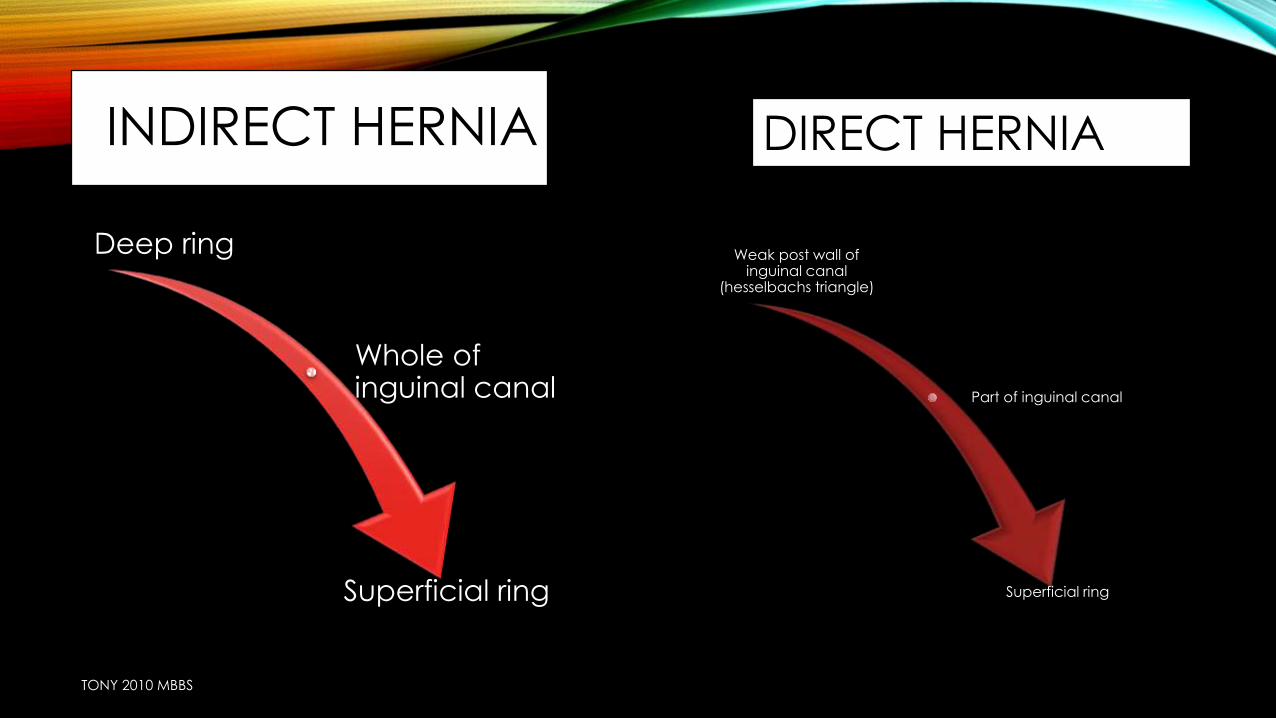
INDIRECT HERNIA
Deep ring
Whole of inguinal canal
Superficial ring
TONY 2010 MBBS
Weak post wall of inguinal canal
(hesselbachs triangle)
Part of inguinal canal
Superficial ring
DIRECT HERNIA
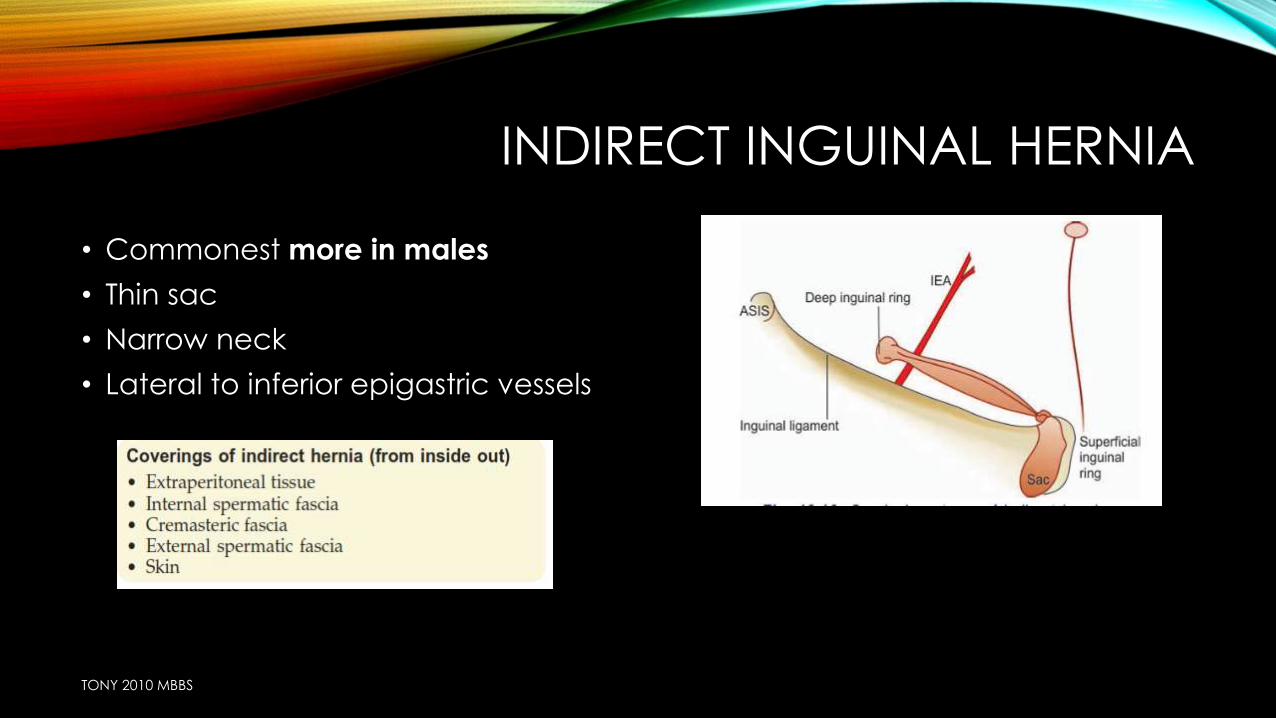
INDIRECT INGUINAL HERNIA
• Commonest more in males
• Thin sac
• Narrow neck
• Lateral to inferior epigastric vessels
TONY 2010 MBBS
TONY 2010 MBBS
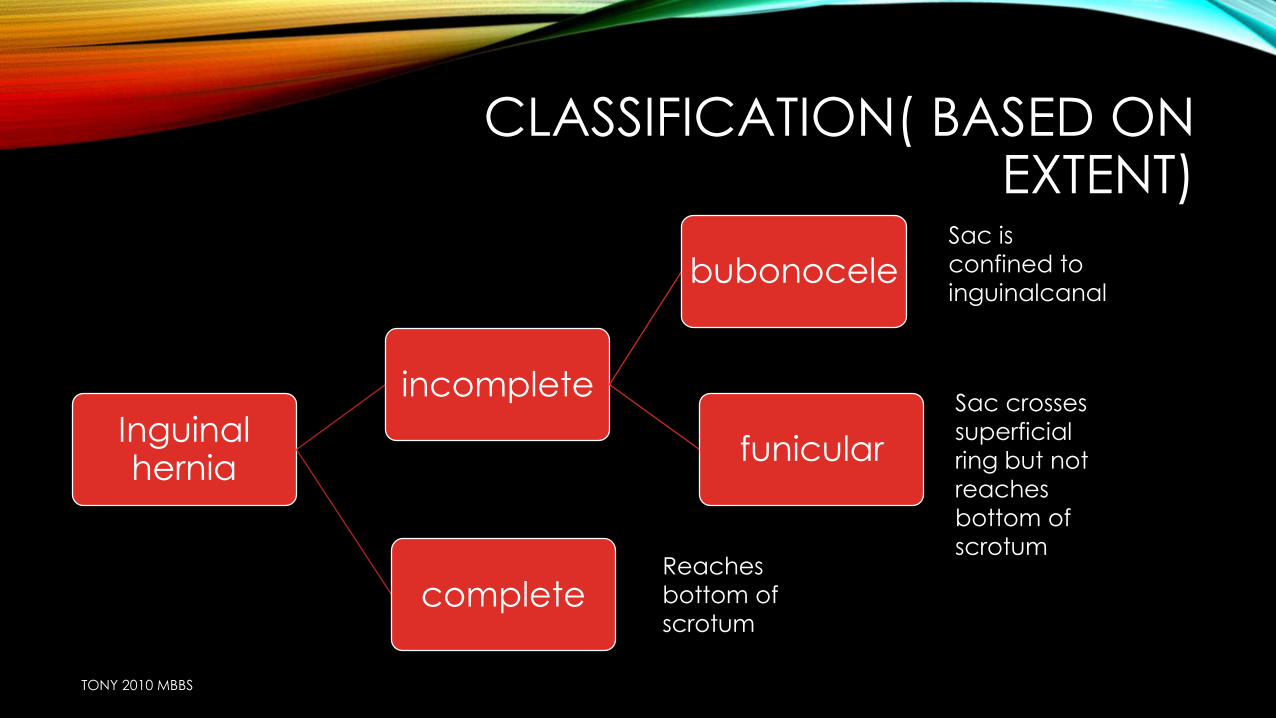
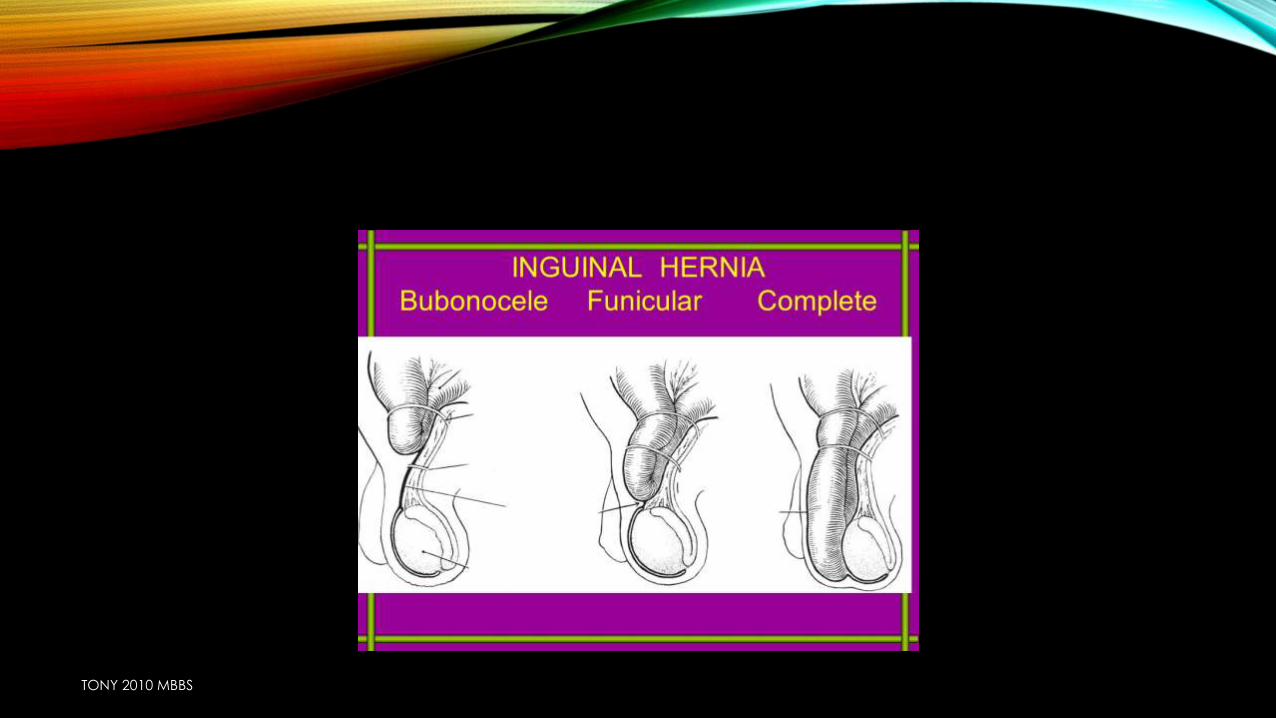
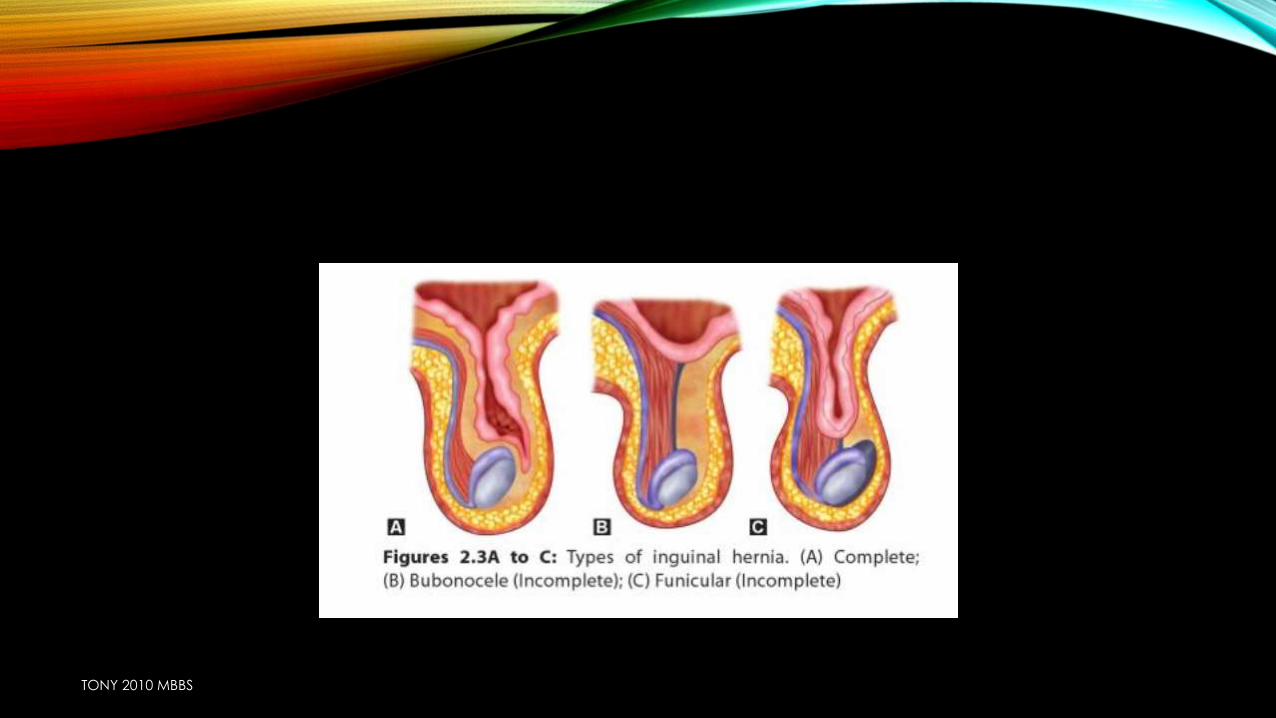
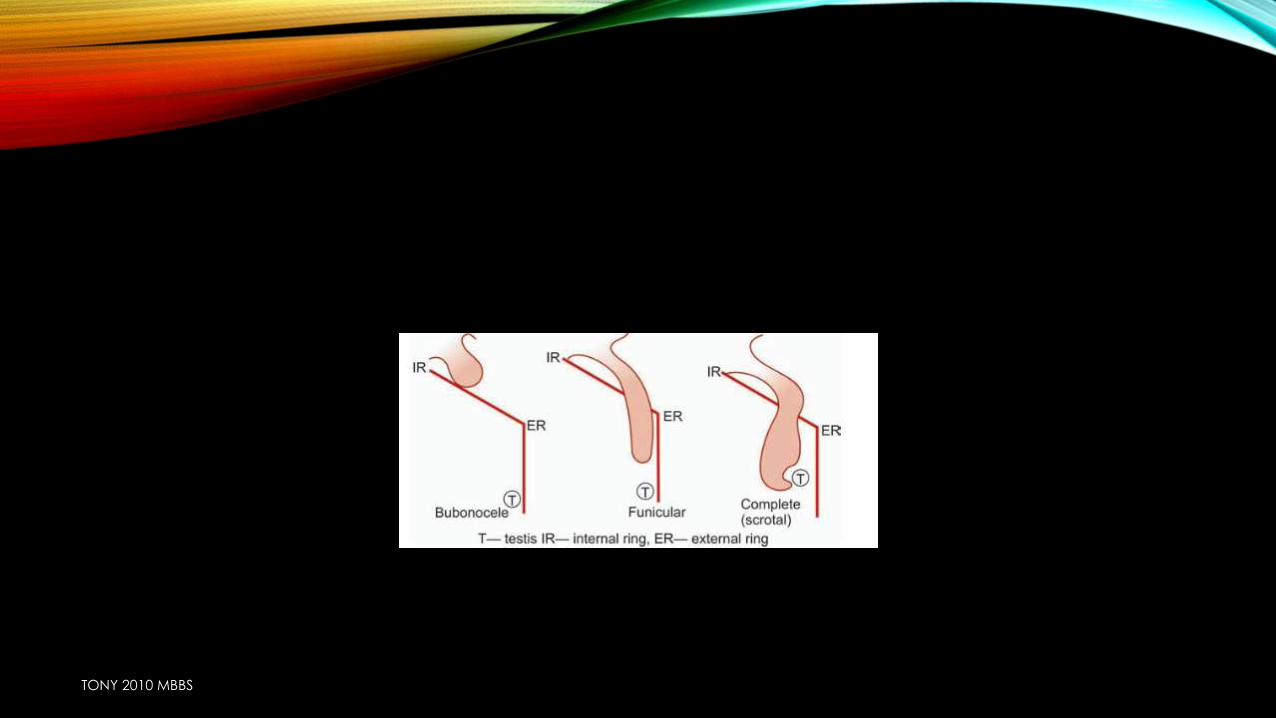
CLASSIFICATION( BASED ON EXTENT)
Inguinal hernia
incomplete
bubonocele
funicular
complete
Sac is
confined to
inguinalcanal
Sac crosses
superficial
ring but not
reaches
bottom of
scrotumReaches
bottom of
scrotum
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
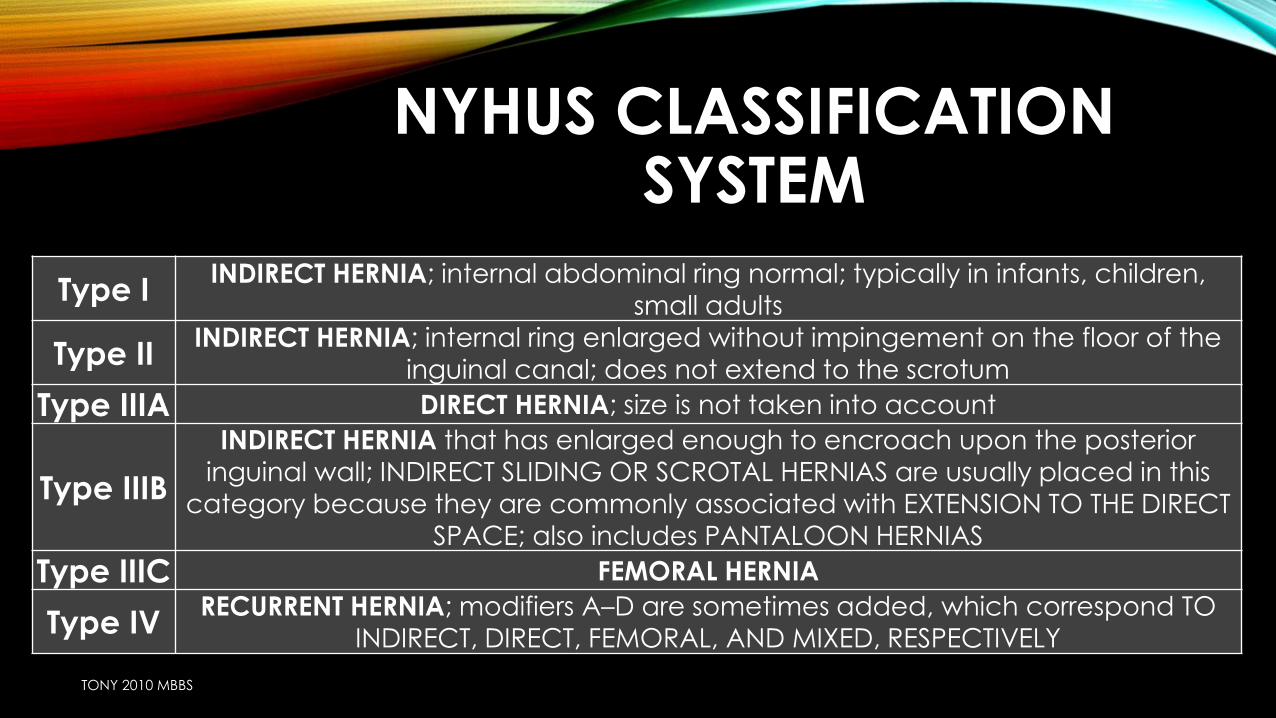
NYHUS CLASSIFICATION SYSTEM
Type IINDIRECT HERNIA; internal abdominal ring normal; typically in infants, children,
small adults
Type IIINDIRECT HERNIA; internal ring enlarged without impingement on the floor of the
inguinal canal; does not extend to the scrotum
Type IIIA DIRECT HERNIA; size is not taken into account
Type IIIB
INDIRECT HERNIA that has enlarged enough to encroach upon the posterior
inguinal wall; INDIRECT SLIDING OR SCROTAL HERNIAS are usually placed in this category because they are commonly associated with EXTENSION TO THE DIRECT
SPACE; also includes PANTALOON HERNIAS
Type IIIC FEMORAL HERNIA
Type IVRECURRENT HERNIA; modifiers A–D are sometimes added, which correspond TO
INDIRECT, DIRECT, FEMORAL, AND MIXED, RESPECTIVELY
TONY 2010 MBBS
DIRECT INGUINAL HERNIA
• ALWAYS ACQUIRED
• MEDIAL TO INFERIOR EPIGASTRIC ARTERY
• SAC IS THICK
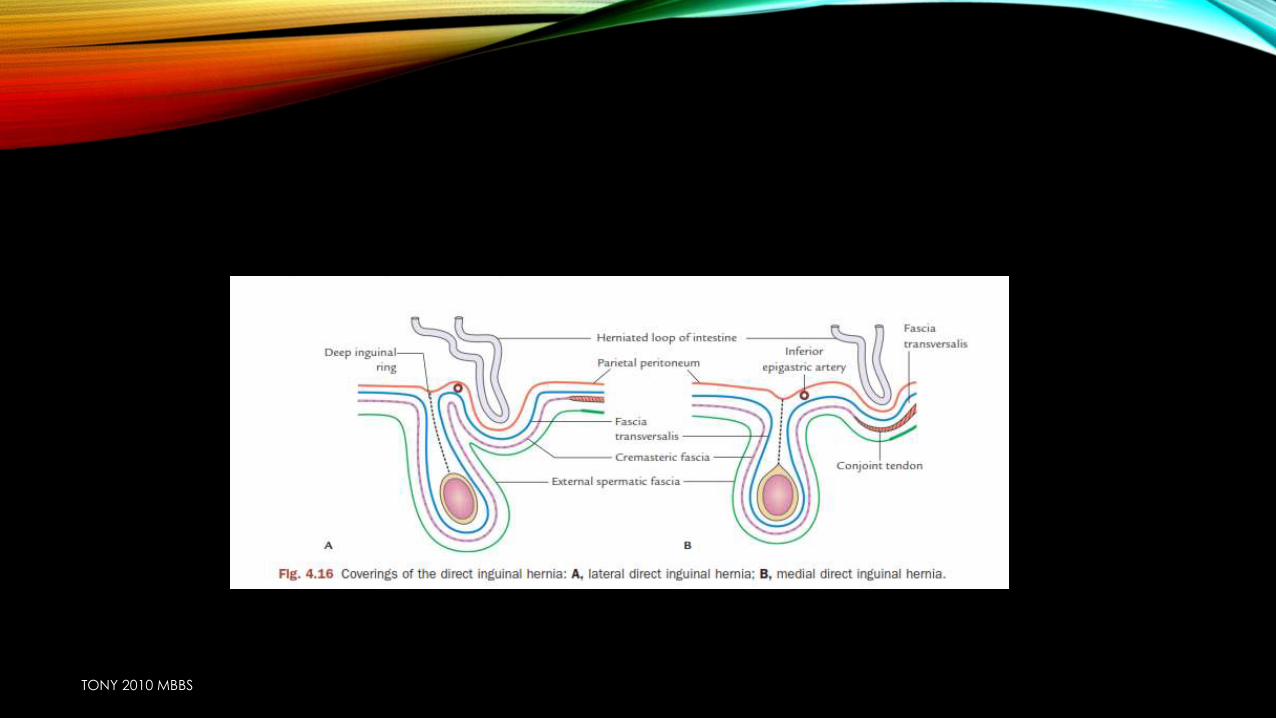
• THROUGH HESSELBACHS TRIANGLE….. HESSELBACHS TRIANGLE IS DIVIDED IN TO LATERAL & MEDIAL HALVES BY OBLITERATED UMBILICAL ARTERY(LATERAL UMBILICAL LIGAMENT) DIRECT HERNIA CAN BE DIVIDED IN TO LATERAL AND MEDIAL BASED UPON THIS LIGAMENT
TONY 2010 MBBS
Direct hernia
medial
lateral
TONY 2010 MBBS
TONY 2010 MBBS
2 CLASSICAL SIGNS OF UNCOMPLICATED HERNIA
• Impulse on coughing
• Reducibility
TONY 2010 MBBS
COMPLICATIONS OF HERNIA
• Irreducibility
• Obstructed hernia
• Strangulated hernia
• Inflammation
• Incarceration
TONY 2010 MBBS
IRREDUCIBILITY
• Adhesions of its contents to each other
• Adhesion of its contents with the sac
• Adhesion of one part of sac to other
• Sliding hernia
• Massive hernia (scrotal abdomen)
TONY 2010 MBBS
OBSTRUCTED HERNIA
• Irreducibility + intestinal obstruction ( lumen obstruction)
• It does not occur in
• Richters hernia
• Omentocele
• Littres hernia
• Features of obstructed hernia
• No expansile impulse on coughing
• Irreducible
• No pain
• Lax non tender
• symptoms
TONY 2010 MBBS
INCARCERATED HERNIA
• When it contains a portion of colon with faeces indenting with fingers putty like feeling
TONY 2010 MBBS
STRANGULATED HERNIA
• Irredudicibility + intestinal obstruction + arrest of blood supply
• Due to constriction at the neck
TONY 2010 MBBS
SIGNS OF STRANGULATED HERNIA
• Tense
• Tender
• No impulse on coughing
• irreducible
• Recent increase in size
TONY 2010 MBBS
TREATMENT
• Raise the foot end (gravityredn of hernia)
• Ice bag applin redue congestion & edema
• Nasogastric tube for gastric aspiration
• Iv fluid admn
• Parenteral antibiotics.
• Herniotomy open at the fundus & drain the fluid divide constriction ring & examine the bowel for viability
• Nonviable Bowel
• Small bowel—end to end resection anastomosis
• Omentum—excise the gangrenous part.
TONY 2010 MBBS
• Non viable bowel
• Greenish/blackish in colour
• No peristalsis
• Gut is flaccid & lusture less
• Fluid of sac is bllod stained & foul smelling
TONY 2010 MBBS
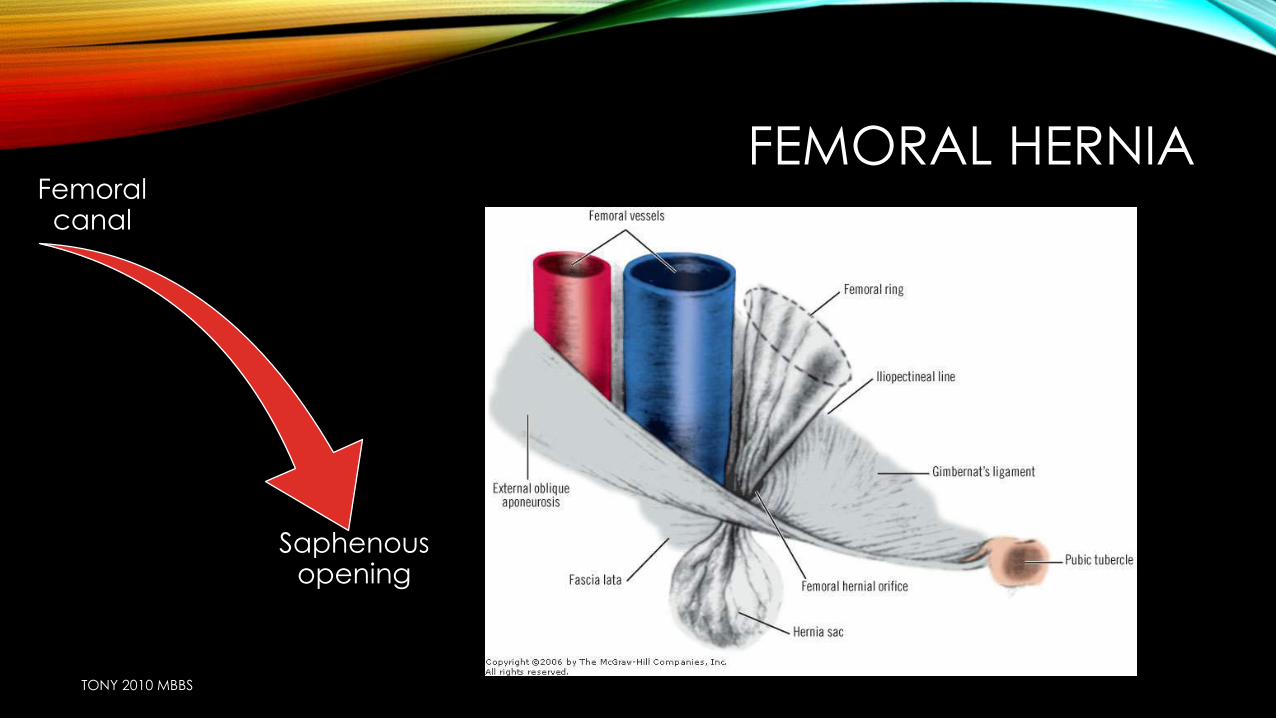
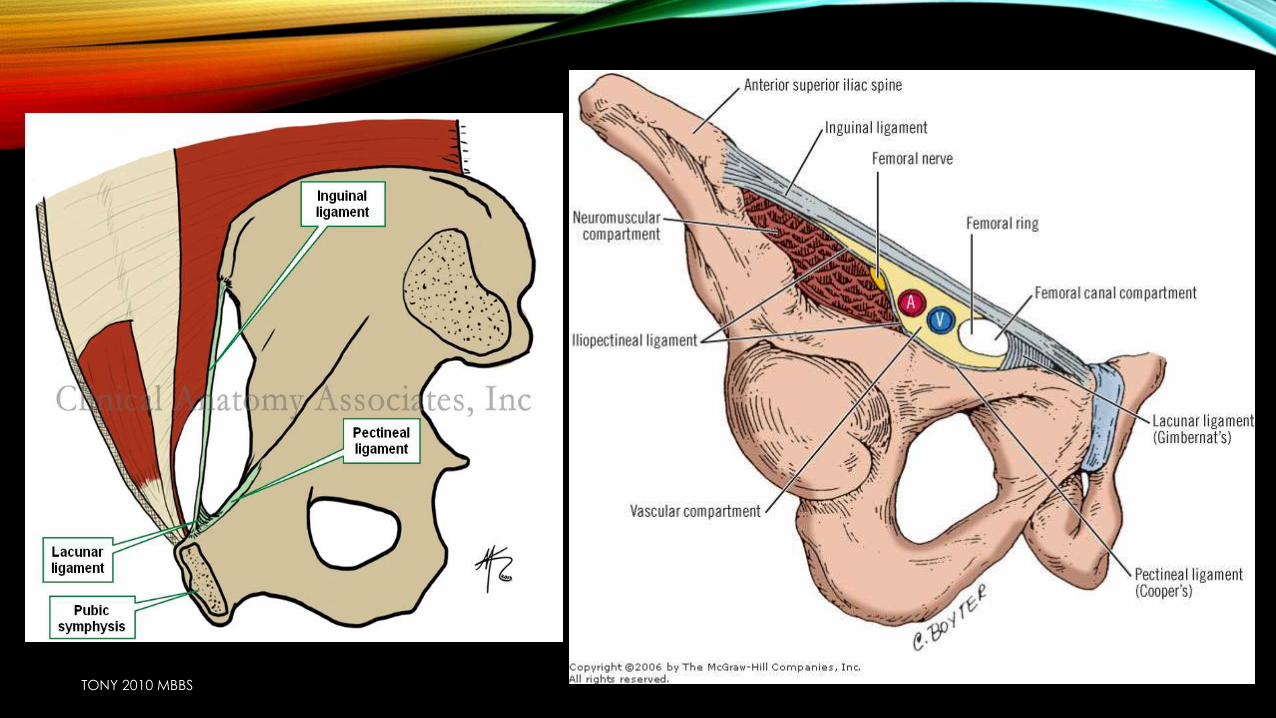
FEMORAL HERNIAFemoral canal
Saphenous opening
TONY 2010 MBBS
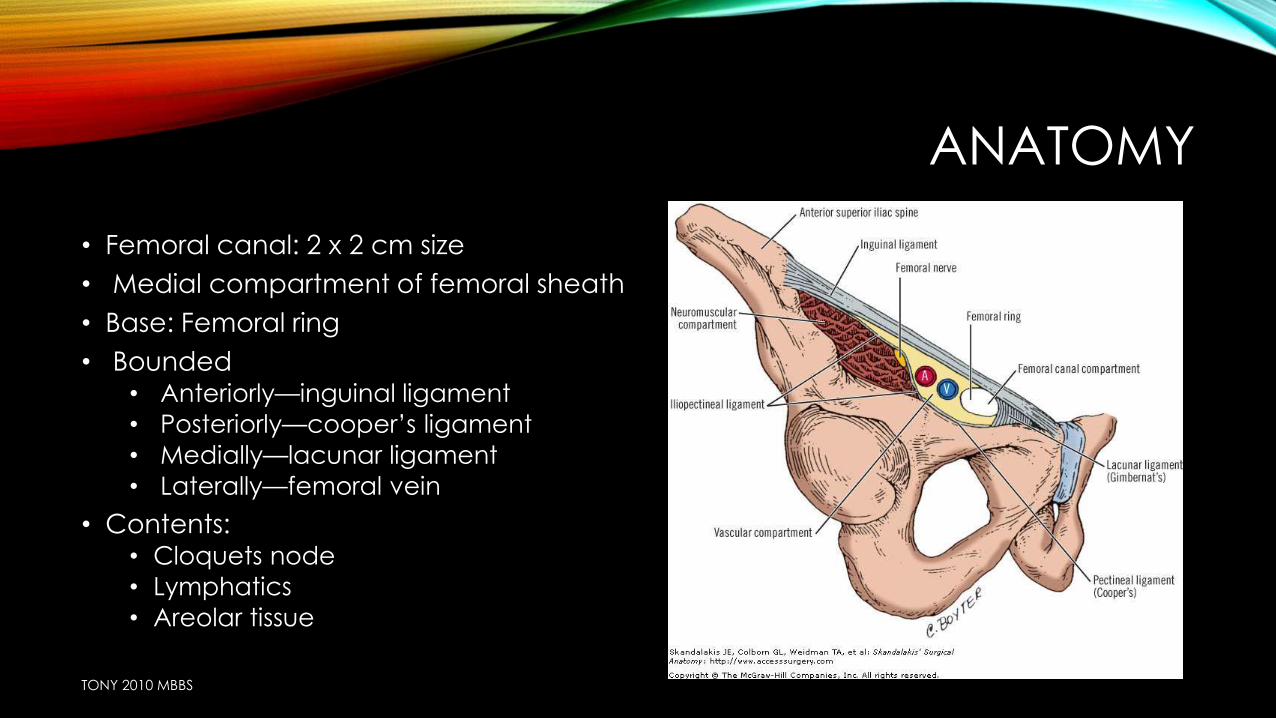
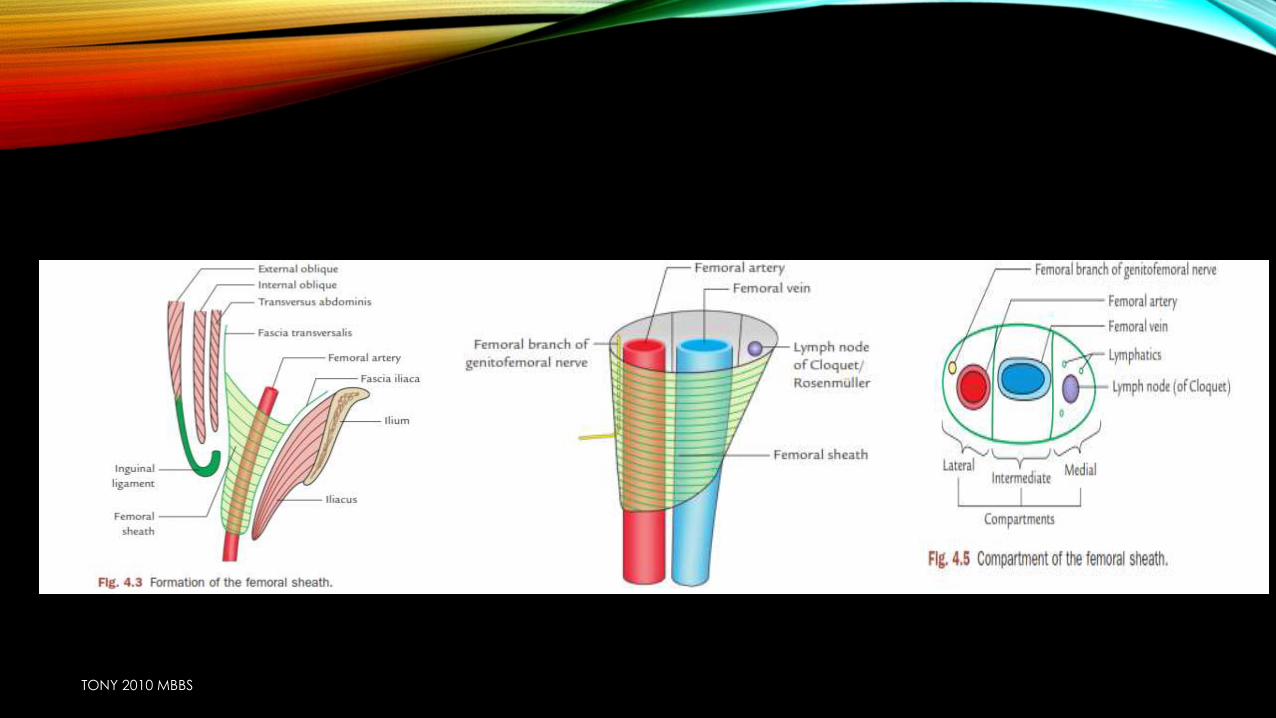
ANATOMY
• Femoral canal: 2 x 2 cm size
• Medial compartment of femoral sheath
• Base: Femoral ring
• Bounded• Anteriorly—inguinal ligament
• Posteriorly—cooper’s ligament
• Medially—lacunar ligament
• Laterally—femoral vein
• Contents: • Cloquets node
• Lymphatics
• Areolar tissue
TONY 2010 MBBS
TONY 2010 MBBS
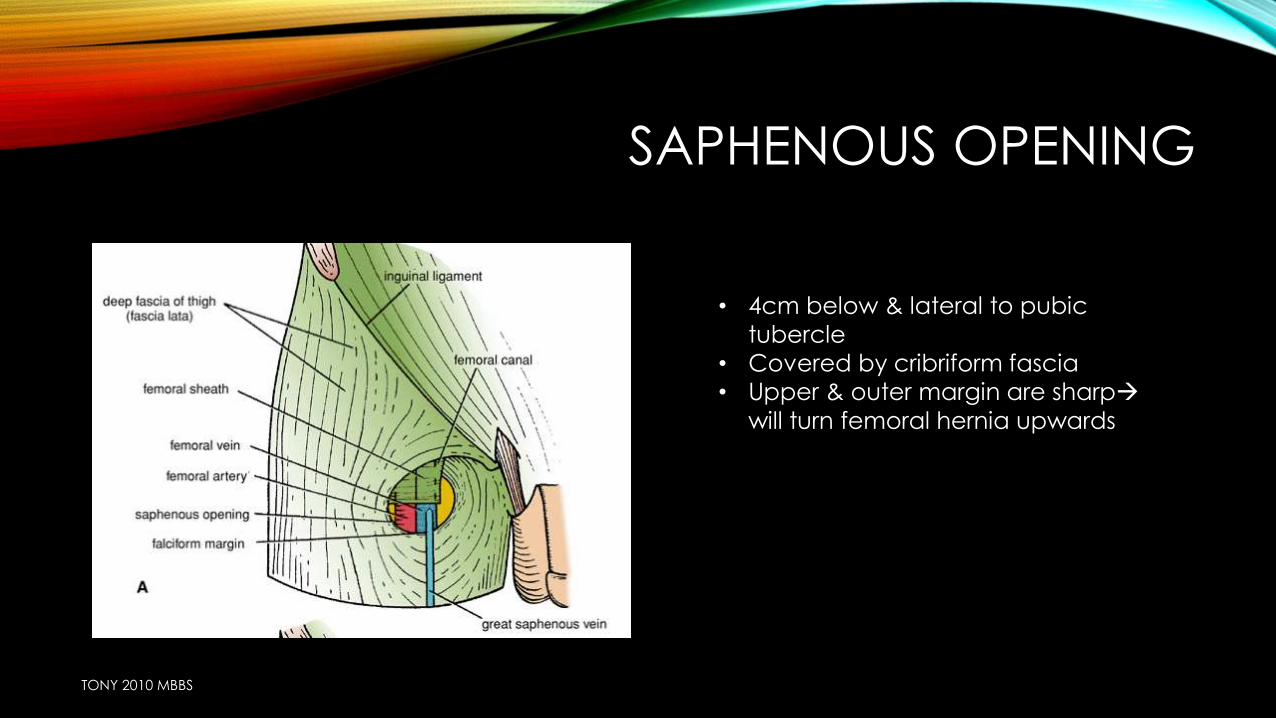
SAPHENOUS OPENING
TONY 2010 MBBS
• 4cm below & lateral to pubic
tubercle
• Covered by cribriform fascia• Upper & outer margin are sharp
will turn femoral hernia upwards
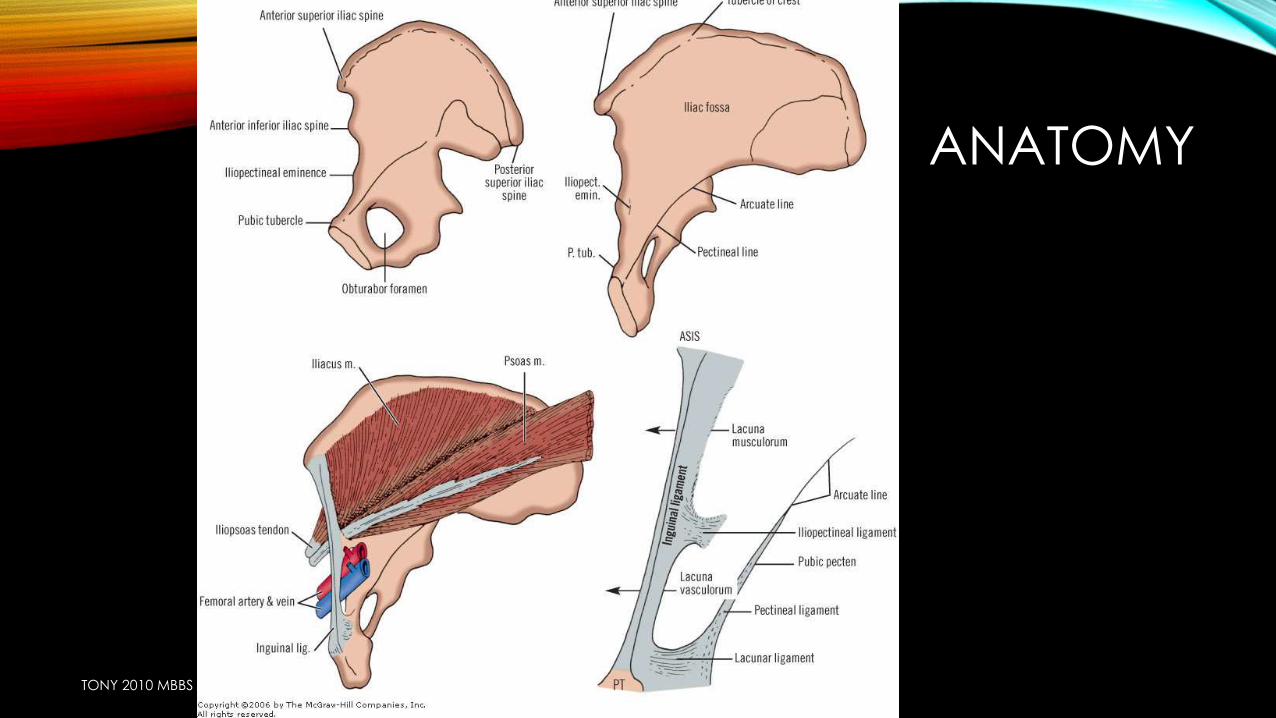
ANATOMY
TONY 2010 MBBS
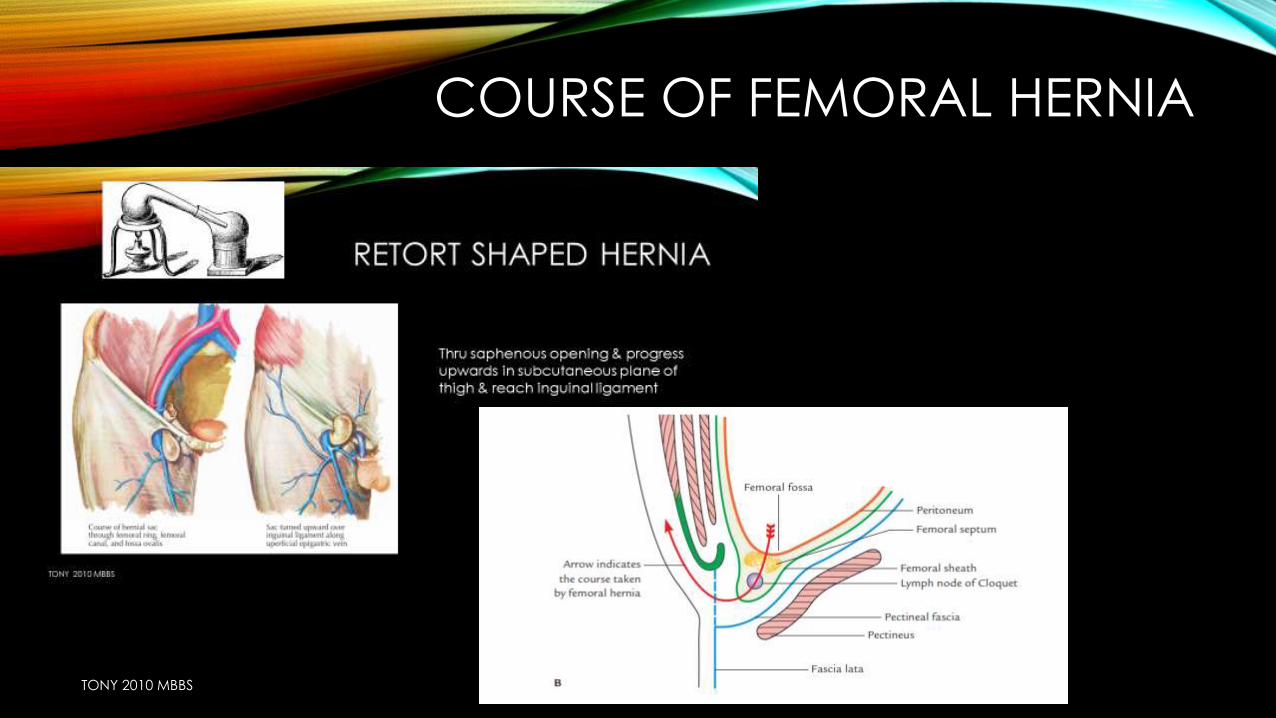
COURSE OF FEMORAL HERNIA
TONY 2010 MBBS
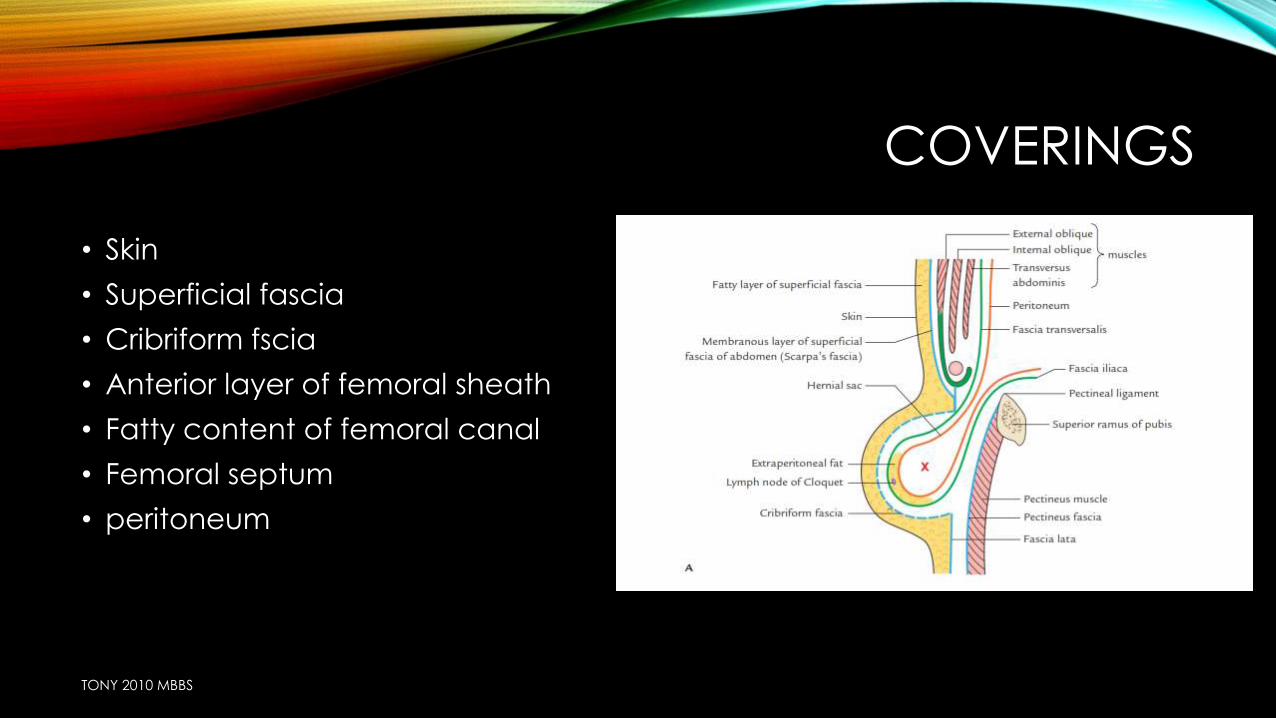
COVERINGS
• Skin
• Superficial fascia
• Cribriform fscia
• Anterior layer of femoral sheath
• Fatty content of femoral canal
• Femoral septum
• peritoneum
TONY 2010 MBBS

• Increased chance of strangulation
• F>M
• Uncommon in children
• Symptoms
• Pain
• Swelling
TONY 2010 MBBS
TONY 2010 MBBS
• Position
• Below & lateral to pubic tubercle
• Shape
• Globular/ retort (if large)
• Narrow neck
• Absent impulse on coughing
• Irreducible
• Strangulation
• consistency
• Position
• Zeimanns test
• Impulse on ring finger
• Invagination test
• Empty inguinal canal
• Ring occlusion of saphenous opening
TONY 2010 MBBS
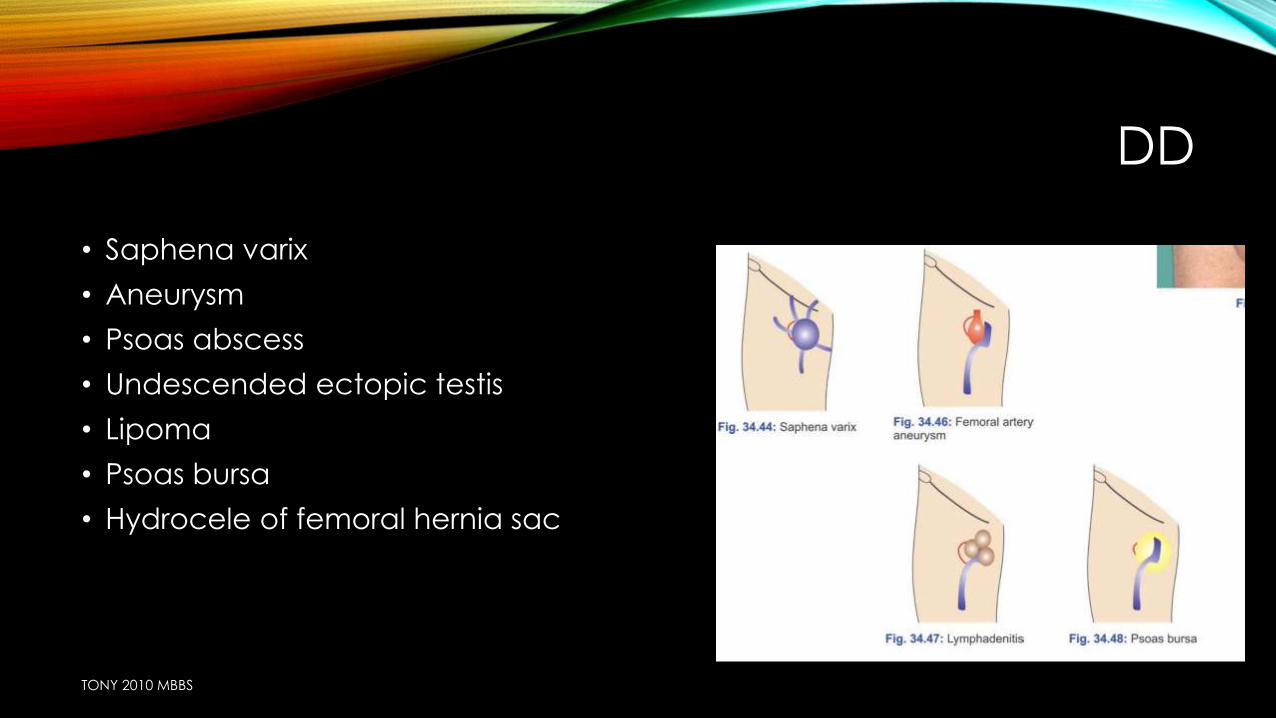
DD
• Saphena varix
• Aneurysm
• Psoas abscess
• Undescended ectopic testis
• Lipoma
• Psoas bursa
• Hydrocele of femoral hernia sac
TONY 2010 MBBS
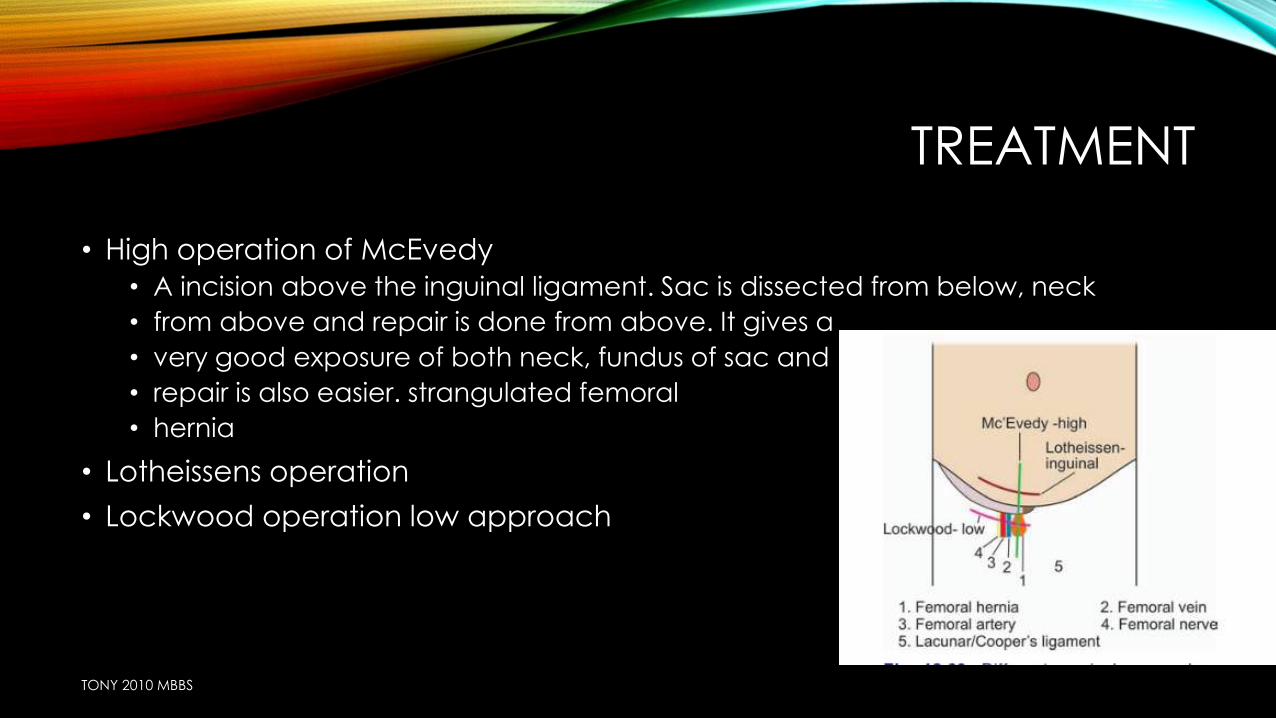
TREATMENT
• High operation of McEvedy
• A incision above the inguinal ligament. Sac is dissected from below, neck
• from above and repair is done from above. It gives a
• very good exposure of both neck, fundus of sac and
• repair is also easier. strangulated femoral
• hernia
• Lotheissens operation
• Lockwood operation low approach
TONY 2010 MBBS
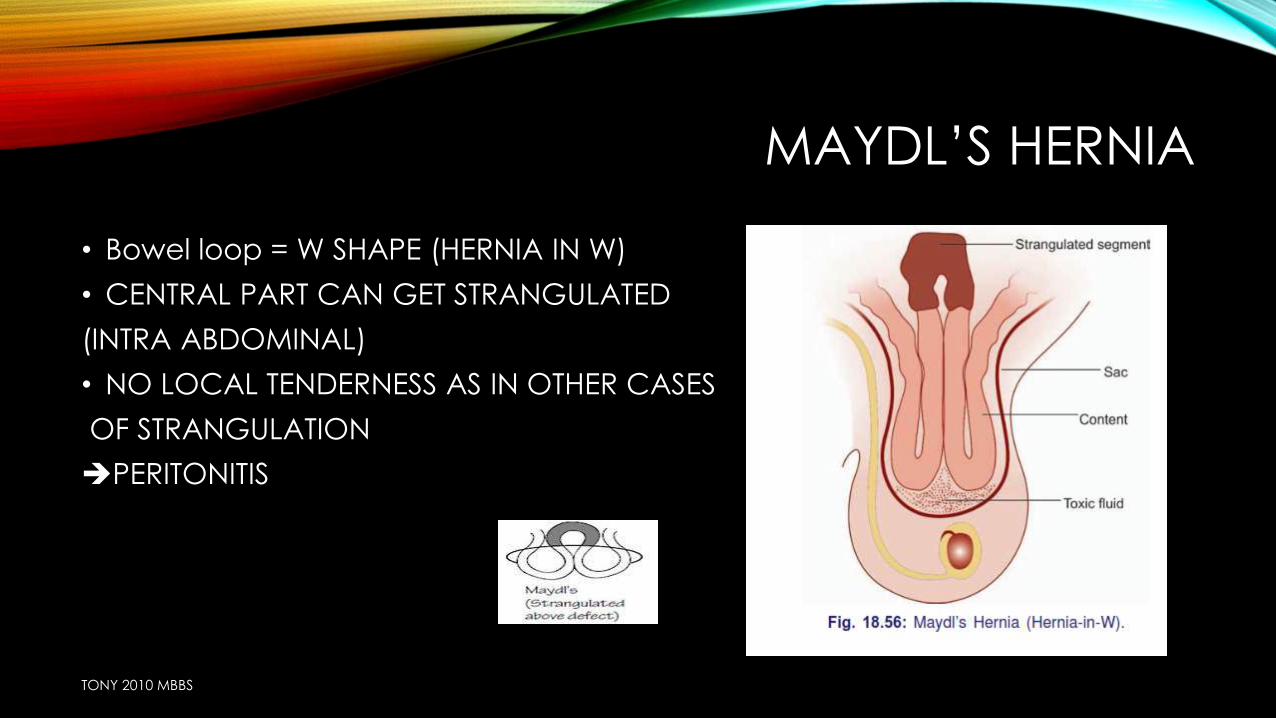
MAYDL’S HERNIA
• Bowel loop = W SHAPE (HERNIA IN W)
• CENTRAL PART CAN GET STRANGULATED
(INTRA ABDOMINAL)
• NO LOCAL TENDERNESS AS IN OTHER CASES
OF STRANGULATION
PERITONITIS
TONY 2010 MBBS
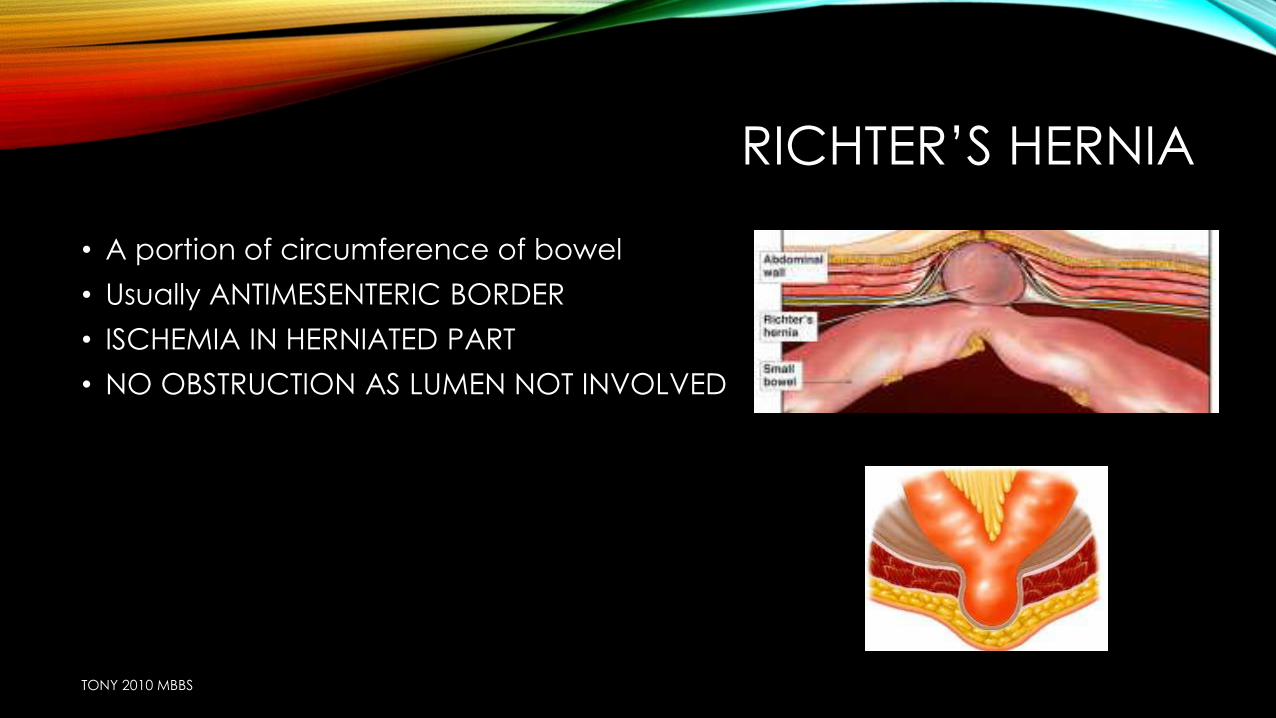
RICHTER’S HERNIA
• A portion of circumference of bowel
• Usually ANTIMESENTERIC BORDER
• ISCHEMIA IN HERNIATED PART
• NO OBSTRUCTION AS LUMEN NOT INVOLVED
TONY 2010 MBBS
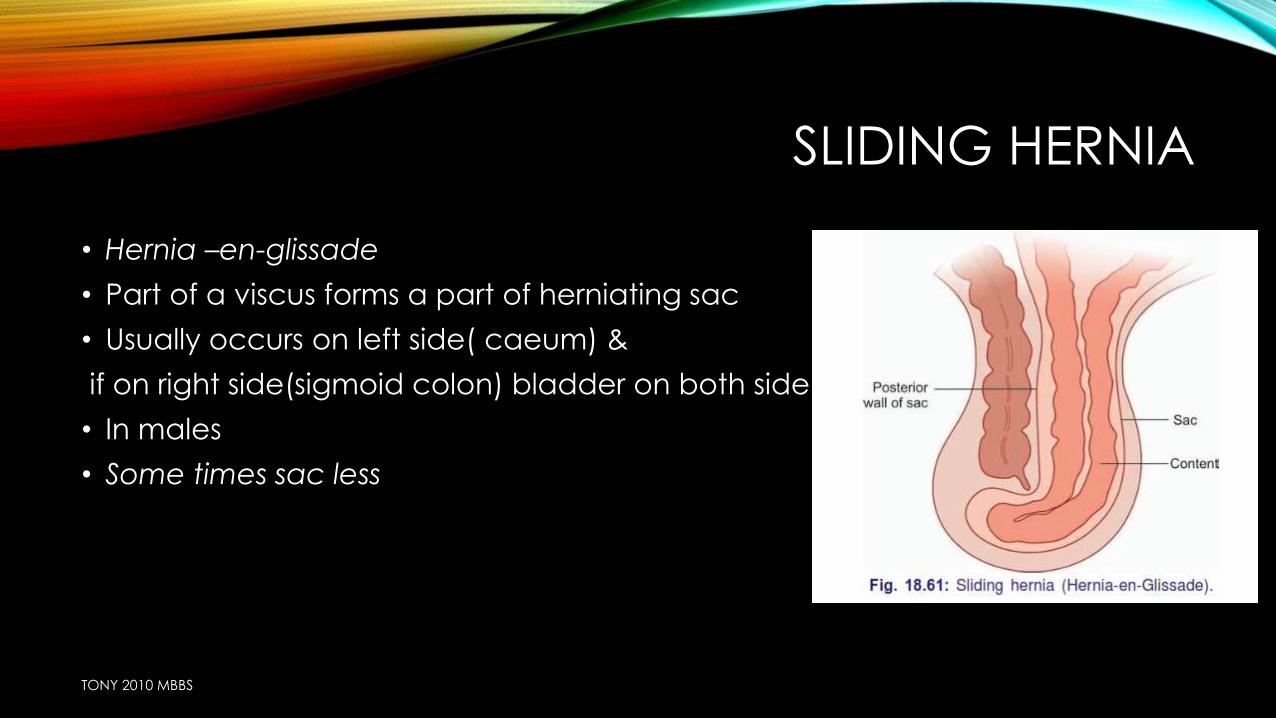
SLIDING HERNIA
• Hernia –en-glissade
• Part of a viscus forms a part of herniating sac
• Usually occurs on left side( caeum) &
if on right side(sigmoid colon) bladder on both side
• In males
• Some times sac less
TONY 2010 MBBS
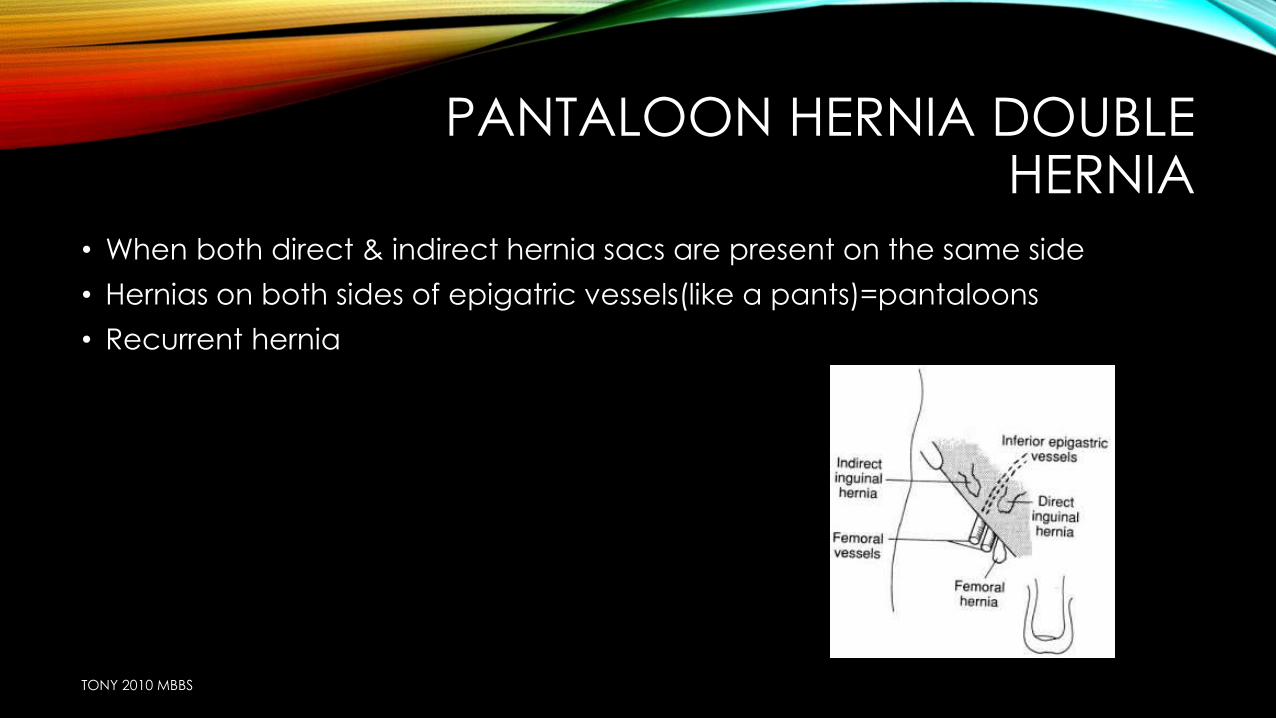
PANTALOON HERNIA DOUBLE HERNIA
• When both direct & indirect hernia sacs are present on the same side
• Hernias on both sides of epigatric vessels(like a pants)=pantaloons
• Recurrent hernia
TONY 2010 MBBS
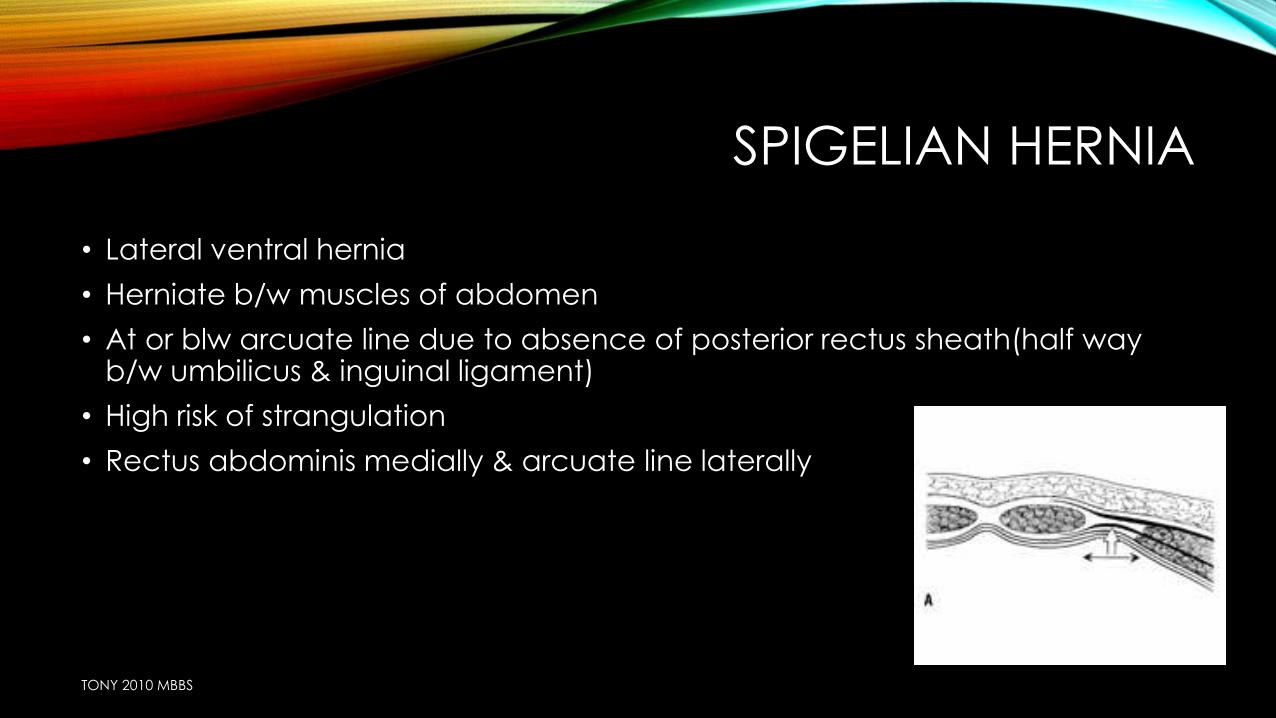
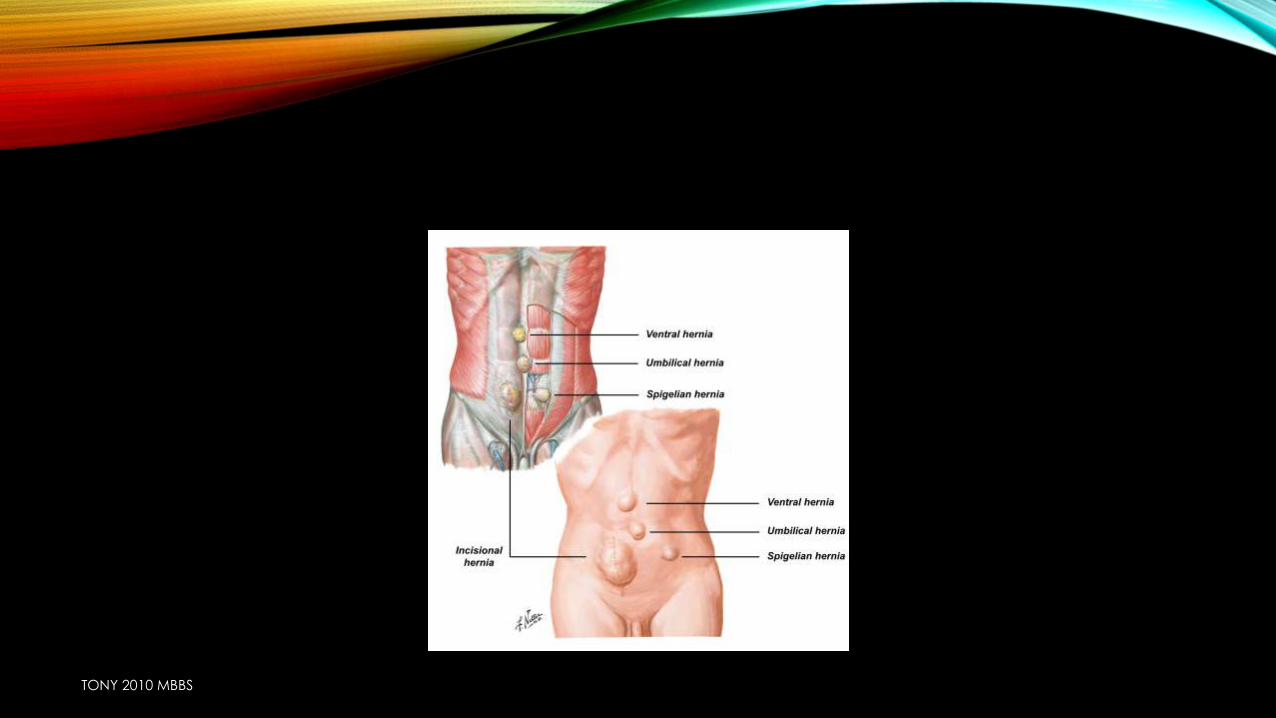
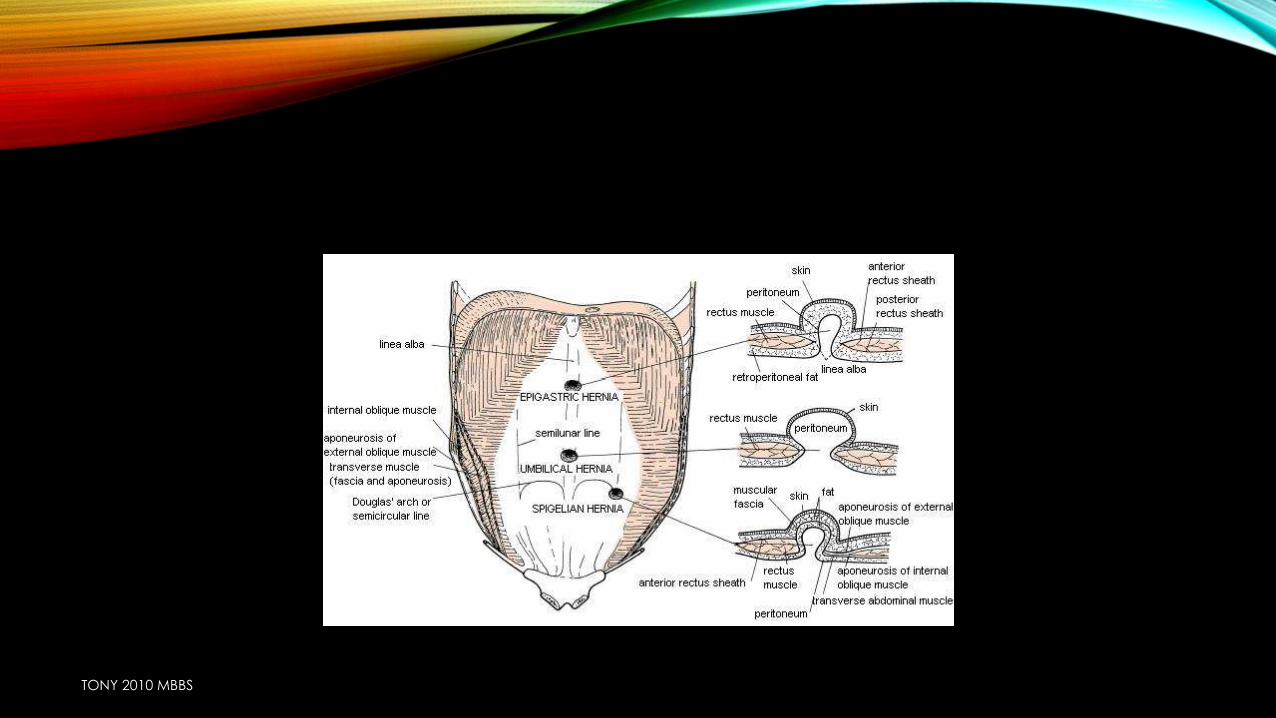
SPIGELIAN HERNIA
• Lateral ventral hernia
• Herniate b/w muscles of abdomen
• At or blw arcuate line due to absence of posterior rectus sheath(half way b/w umbilicus & inguinal ligament)
• High risk of strangulation
• Rectus abdominis medially & arcuate line laterally
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
TONY 2010 MBBS
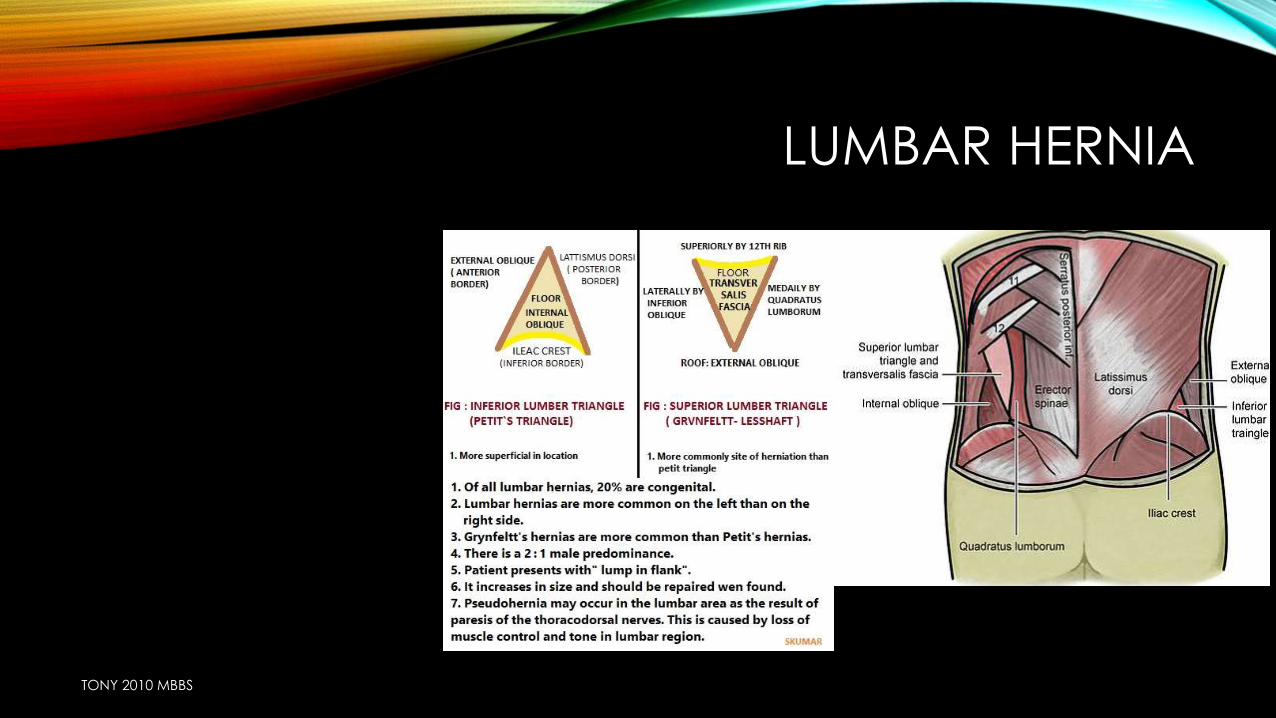
LUMBAR HERNIA
TONY 2010 MBBS
UMBILICAL HERNIA
Um
bili
ca
l h
ern
ia
Exomphalos
Umbilical hernia in infants & children
Para umbilical hernia of adults
TONY 2010 MBBS
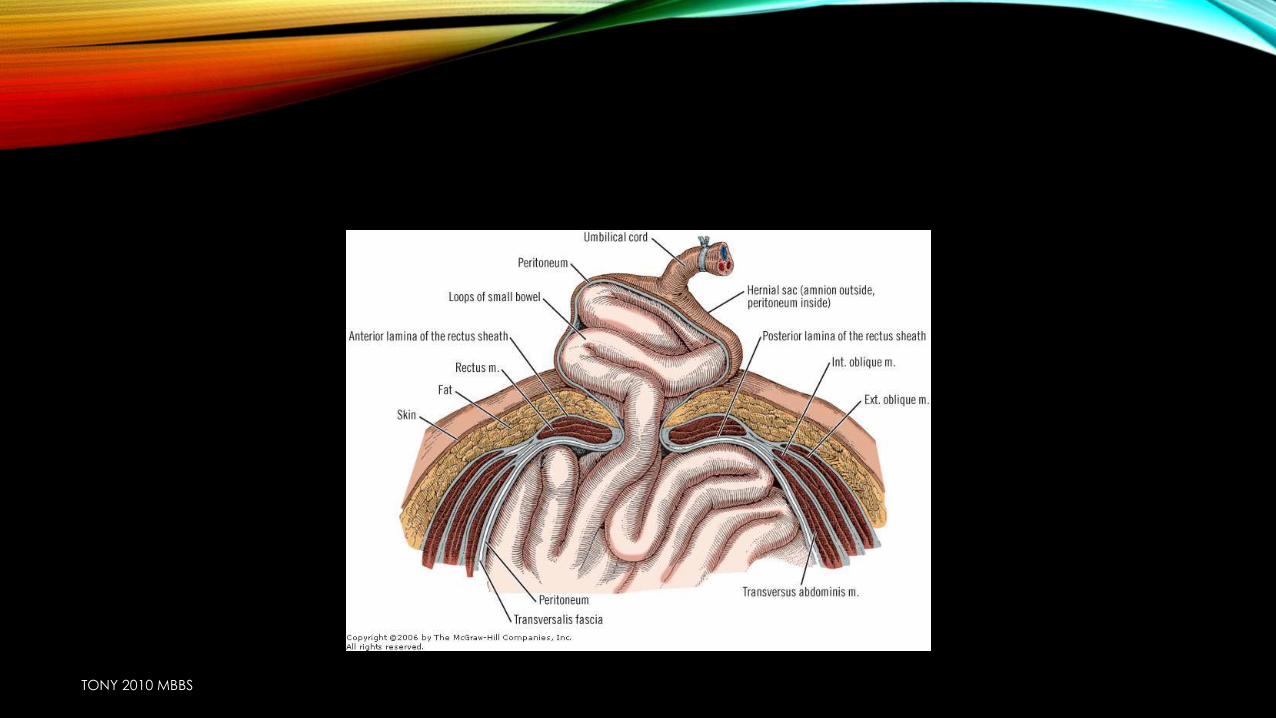
EXOMPHALOS
• Failure of all or part of the midgutto return to the abdominal cavity during early fetal life
• Outer } amniotic membrane
• Middle } whartons jelly
• Inner } peritoneum exomphalos
Exomphalosminor
Exomphalosmajor
TONY 2010 MBBS
TONY 2010 MBBS
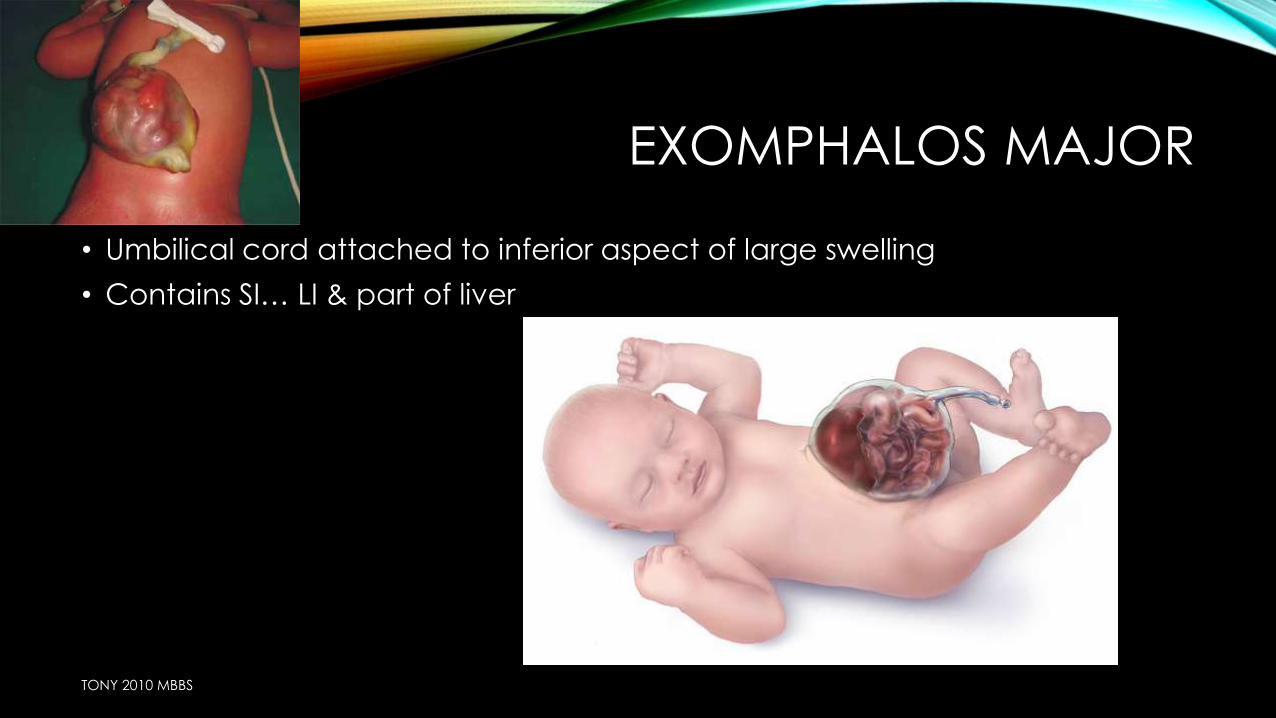
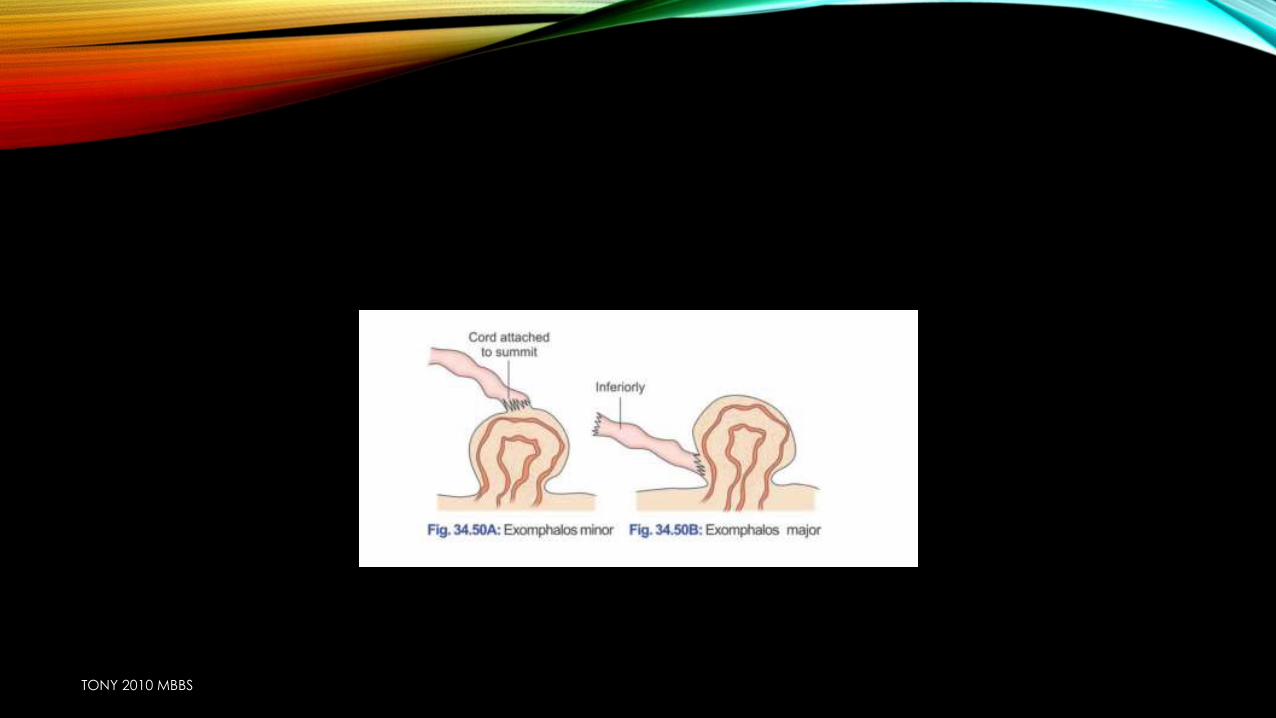
EXOMPHALOS MAJOR
• Umbilical cord attached to inferior aspect of large swelling
• Contains SI… LI & part of liver
TONY 2010 MBBS
• Exomphalos major may burst
• So emergency Sx is needed
TONY 2010 MBBS
EXOMPHALOS MINOR
• Sac is small
• Umbilical cord is attached to its summit
TONY 2010 MBBS
TONY 2010 MBBS
UMBILICAL HERNIA IN INFANTS & CHILDRENS
• Through umbilical cicatrix
• Spherical in shape
• Increase in size in crying
TONY 2010 MBBS
TONY 2010 MBBS
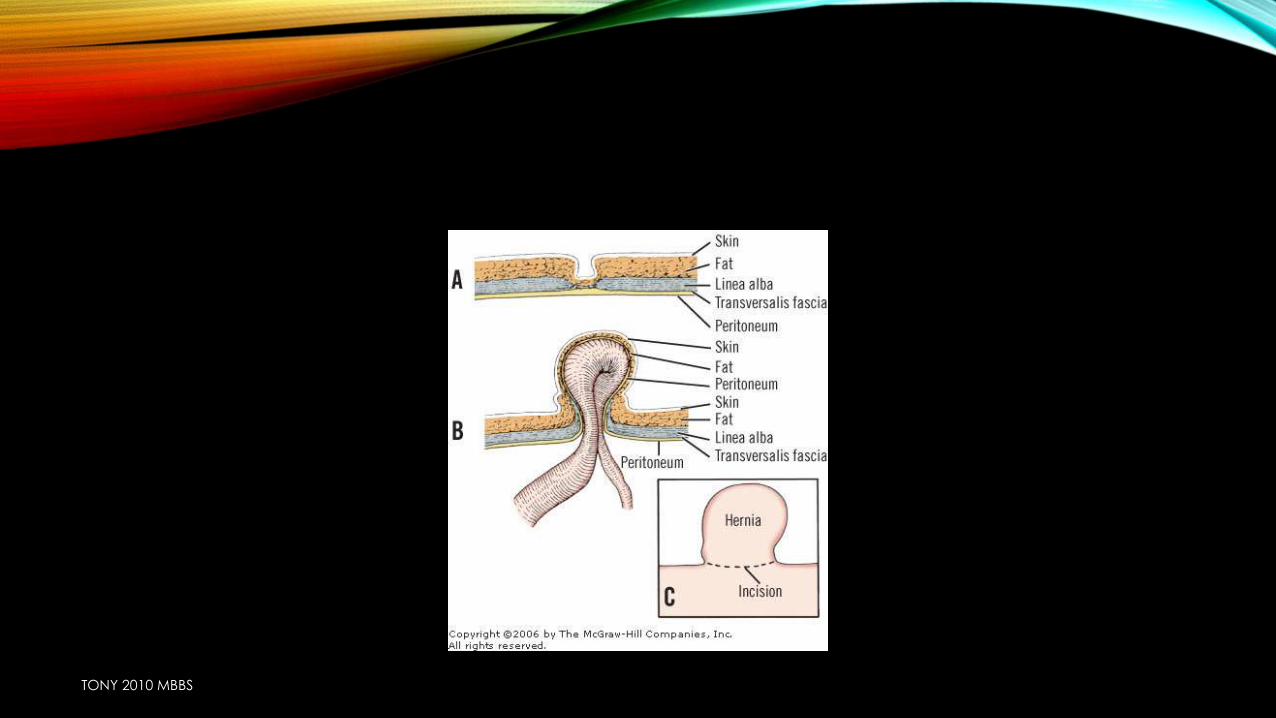
PARAUMBILICAL HERNIA OF ADULTS
• Not through umbilical cicatrix but through linea alba
• Above (supraumbilical)
• Below (infraumbilical)
TONY 2010 MBBS
INTERSTITIAL HERNIA
• Hernial sac lies between muscle layers of abdominal wall
• Preperitoneal/intraparietal
• Interparietal
• Extraparietal
TONY 2010 MBBS
LITTRE’S HERNIA
• Meckels diverticulum is the content
TONY 2010 MBBS
CAUSES OF RECURRENCE OF INGUINAL HERNIA
• Failure to ligate the sac at the neck
• Increased tension
• Use of absorbable sutures
• Fault in selection of operation
• Infection
• Lifting of heavy weight with in 3 months
• Persistent predisposing factors
• Appearance of new hernia
TONY 2010 MBBS
HERNIA OF A HYDROCELE
LOCALIZED THINNING OF TUNICA LEADING TO PSEUDOPODIUM-LIKE PROJECTION, USUALLY SEEN WHEN THE SAC IS THICK AND FLUID IS UNDER TENSION through
HYDROCELE OF A HERNIA
FLUID SEQUESTRATION IN A LOCULUS OF THE HERNIAL SAC, RESEMBLING HYDROCELE. THIS IS SEEN IN LONG STANDING CASES WITH ADHESIONS WITHIN THE SAC
MORE COMMON IN VENTRAL HERNIA CONTAING OMENTUM
OGILVIE HERNIA
• • Direct hernias are always acquired. Indirect may be congenital or acquired.
• • Only congenital direct hernia is ogilvie hernia; through a rigid circular orifice
• in the conjoined tendon just lateral to where it inserts into the rectus sheath.
TONY 2010 MBBS




























