Embed Size (px)
Citation preview

ENT
726 THE PRACTITIONER, SEPTEMBER 2003, VOL 247
Management
JARROD J HOMERMD, FRCS, FRCS(ORL-HNS)
Consultant Otolaryngologist/Head-and-NeckSurgeon, Manchester Royal Infirmary & ChristieHospital, Manchester. Mr Homer is HonoraryClinical Lecturer, University of Manchester. Hismain clinical interest is in head and neckoncology/tumour surgery
PRIYA SILVAMRCS
Senior House Officer in Otolaryngology,Department of Otolaryngology-Head and NeckSurgery, Manchester Royal Infirmary
Neck lumps are common inpatients of all ages, and canbe due to a variety of
pathologies in a number of differentstructures in the neck. Most arebenign, but it is essential to promptlyinvestigate and treat patients withpotentially serious disease.
In the past, patients with necklumps have been referred to a vari-ety of clinics for investigation,sometimes with either sub-optimalor even dangerous management.
•What symptoms and signs pointtowards possible malignancy?
•What conservative measures canbe addressed to help preventsalivary gland calculi forming?
•How are thyroglossal andbronchial cysts best managed?
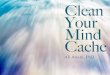
Area Structures givingrise to neck lumps
A Submental area Lymph nodes
B Submandibular area Submandibular gland,lymph nodes
C Upper Tail of parotid gland,lymph nodes, branchialcyst, carotid sheath structures
D Mid Lymph nodes, branchial cyst,carotid sheath structures
E Lower Lymph nodes, thyroidgland
F Central neck compartment Thyroid gland, thyroglossal cyst, lymph nodes
G Posterior triangle Lymph nodes, parotid gland
H Supraclavicular fossa Lymph nodes (infraclavicular drainage), mediastinal structures
Figure 1 Regions of neck and tissues from which neck lumps arise
Jugular chain(deep tosternocleidoma-stoid muscle)

THE PRACTITIONER, SEPTEMBER 2003, VOL 247 727
Neck lumps
Examples include failure to exam-ine the upper aerodigestive tract,delayed diagnosis and inappropri-ate open biopsy. Today, however,most otolaryngology/head-and-neck-surgery departments havededicated neck-lump clinics, andthe situation has improved.
This article aims to outline thecauses of neck lumps. We haveexcluded acute disease, but empha-sise the common, classic or seriouspathologies. We also briefly describe
of neck lumps
investigation and further manage-ment by the neck lump clinic.�Differentiation of neck lumpsIn the majority of cases it is possibleto make a diagnosis based upon thehistory, site and characteristics ofneck lumps, and the age of thepatient.
In general terms the clinicianneeds to consider where the necklump is and what structures lie inthat area (see figure 1). Then con-sideration of the age of patient and
symptoms will, in many cases, givethe underlying pathology away.
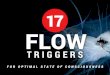
COMMON, CLASSIC ANDIMPORTANT CAUSES OFNECK LUMPSThese are: �Major salivary gland lumps,including parotid and sub-mandibular glands It is usuallystraightforward to identify theanatomical origin of parotid (see figure 2) or submandibular gland
Figure 2Parotid lump –pleomorphicadenoma
•Salivary gland neoplasias aremore common with increasingage but not rare in youngadults. They are, however,rare in children. Often, thelump itself is asymptomaticand discovered incidentally
•In sialolithiasis, calculi formwithin the duct system of thesalivary gland. The calculus canoften be merely a sludge. Thehistory is very characteristic.There is swelling andtenderness of salivary glandwhen eating or just beforeeating. The treatment is usuallyto remove the calculus, ifpresent and distal enough. Thisprocedure is peroral, andusually carried out under localanaesthetic
•In branchial cysts the history isof a painless lump in the neck,with or without recurrentinfection. They arise usuallyduring the second to forthdecade of life. A cystic lump isfound most commonly just
anterior to the sternomastoidmuscle at the junction of theupper third and lower two-thirds
•In thyroglossal cysts the historyis of a painless midline neckswelling. On examination amidline (usually) cystic necklump is most often situatednear the hyoid bone. It moveson both swallowing andtongue protrusion
•Solitary thyroid nodules mayoccur at any age from youngadulthood onwards. Thehistory is of a painless lump inthe neck with or withoutcompression symptoms. Onexamination there is a solitarythyroid lump. Cervicallymphadenopathy or vocalcord palsy on laryngoscopysuggest malignancy. The lumpshould be investigated byFNAC; an ultrasound scan isrequired to delineate the lumpfurther. Thyroid functionshould also be tested
Clinical focus
�

728 THE PRACTITIONER, SEPTEMBER 2003, VOL 247
Neck lumps
lumps. The main alternative in bothsites is cervical lymphadenopathy. •Salivary gland neoplasias Thesemost commonly occur in theparotid gland. Some 80 per cent arebenign; the common histologiesare pleomorphic adenoma and ade-nolymphoma (Warthin’s tumour).The commonest malignant typesare adenoid cystic carcinoma andadenocarcinoma.
Salivary gland neoplasias aremore common with increasing agebut not rare in young adults. Theyare, however, rare in children.Often, the lump itself is asympto-matic and discovered incidentally.
Features that raise the possibilityof malignancy include noticeable
enlargement, pain, paraesthesiaand facial nerve dysfunction(parotid).
Examination reveals a firm lumpwithin the gland of origin. Facialnerve paralysis, skin tethering orskin involvement would suggestmalignancy.
Fine needle aspiration cytology(FNAC) may be used but the resultsare not as accurate as for otherneck lumps. Diagnosis may not bemade until after surgery.
MR scan is the optimal way ofimaging, but ultrasound will sufficein some cases.
Benign neoplasias are treated bycomplete excision on the basis that:a definitive diagnosis can be made,
benign tumours will continue togrow and become more difficult toexcise, and there is a small risk ofmalignant transformation withtime. The facial nerve shouldalways be preserved.
Malignant cases should bereferred to the head and neckoncology multidisciplinary clinicfor radical excision of the tumour(with facial nerve preservation inmost cases), neck dissection (oflymph nodes) and possible post-operative radiotherapy. •Sialolithiasis (salivary glandcalculi) and sialectasis (duct sys-tem distortion) In sialolithiasis cal-culi form within the duct system ofthe salivary gland. The calculus can
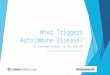
Figure 3Branchial cyst,cystic lump justanterior toupper part ofsternocleido-mastoid. Ifsolid it wouldbe massivelymphaden-opathy andpossibly due tolymphoma orupperaerodigestivecarcinoma

THE PRACTITIONER, SEPTEMBER 2003, VOL 247 729
Neck lumps
often be merely a sludge. Theobstruction causes the gland toswell, especially when saliva produc-tion is increased, usually when eat-ing, and can lead to secondaryinfection.
These most commonly occur (80per cent of cases) in the sub-mandibular gland. Predisposingfactors include reduced flow rates,duct obstruction, especially afterchronic inflammation (sialectasis),changes in salivary pH and dehy-dration.
The history is very characteristic.There is swelling and tenderness ofthe salivary gland when eating orjust before eating. This can berecurrent, that is, it may last for
minutes or hours before settlingdown, or it may last for a few days,in which case a secondary infectionis suggested.
Sialolithiasis may occur at anyage from the teens onwards.
When examined, the gland itselfmay be normal between episodes,or generally enlarged and withsome tenderness. Palpation biman-ually of the relevant salivary ductmay reveal the responsible stone.Massage of the gland occasionallyproduces a purulent secretion.
On plain X-ray most sub-mandibular gland calculi are radio-opaque. Sialography will reveal afilling defect due to intraductalstones, and flushing of the duct is
often therapeutic.If, at the time of assessment,
there has been no recent episodeand there is no calculus to palpate,no investigation may be necessary.
The treatment is usually toremove the calculus, if present anddistal enough. This procedure isperoral, and usually carried outunder local anaesthetic.
Conservative measures are usedif there is no detectable calculusand the symptoms are recurrent;these include regular gland andduct massage, maintenance of goodhydration and regular saliva stimu-lation with sialogues (a lemon or alemon sweet may be used) to ‘flush’the duct system out.
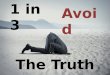
Figure 4 (centre)Thyroglossalcyst
Figure 5 (topright)Solitary thyroidnodule
�

730 THE PRACTITIONER, SEPTEMBER 2003, VOL 247
Neck lumps
The terminal duct may be mar-supialised if the symptoms arerecurrent and there is a stenosis inthis duct.
The gland is removed if thesymptoms are recurrent and sialog-raphy shows proximal calculiand/or intraglandular duct disrup-tion, or if other treatments fail.•Sialadenitis is a chronic inflam-mation of the salivary glands. Insialectasis there is resultant disrup-tion to the duct system and symp-toms of sialolithiasis. Clinicallythere may generalised glandenlargement with or without ten-derness.
Most cases are non-specific, butspecific causes include granuloma-
tous disorders, such as TB or sar-coid, and autoimmune disease,such as Sjögren’s syndrome.
Investigation is geared towardsexcluding either these specific dis-orders or a tumour. Management isgenerally conservative.�Branchial cysts The classicexplanation of branchial cysts isthat they are a congenital persis-tence of cervical sinus duringbranchial cleft development, but amore modern explanation is thatthey result from degeneration ofcervical lymph nodes that have con-genital epithelial inclusions.
The history is of a painless lumpin the neck, with or without recur-rent infection. They arise usually
during the second to forth decadeof life.
On examination, a cystic lump isfound most commonly just anteriorto the sternomastoid muscle at thejunction of the upper third andlower two-thirds (see figure 3).FNAC will show the lump is cystic.
Some ‘branchial cysts’ will benecrotic metastatic lymph nodesfrom primary undiagnosed head-and-neck cancer. It is hence manda-tory that the patient undergoesthorough head and neck examina-tion including fibreoptic laryn-gopharyngoscopy, and that theaspirate is submitted for cytology.
Treatment is by surgical exci-sion. Every patient over 30 years of
Figure 7 (centre)Lymphoma.Multipleposteriortrianglelymphadenopathy
Figure 6 Goitre

THE PRACTITIONER, SEPTEMBER 2003, VOL 247 731
Neck lumps
age should undergo panendoscopyof the upper aerodigestive tract atthe same time to look for a possibleprimary in case the branchial cyst isa lymph node metastasis.
At-risk patients (those over theage of 40 with tobacco or excessivealcohol consumption) should beconsidered for panendoscopy aswell as on-table frozen sectionpathology with the option to pro-ceed to definitive neck dissection ifmalignancy is found.�Thyroglossal cyst This is a con-genital condition. The thyroidgland descends in utero from thetongue as the thyroglossal duct. Athyroglossal cyst arises from persis-tent epithelial tissue along the duct.
The history is of a painless mid-line neck swelling with or without ahistory of recurrent enlargementand tenderness caused by infection.
Thyroglossal cysts are usuallyseen in the first two decades of life,but presentations later in life arenot uncommon.
On examination a midline (usu-ally) cystic neck lump is most oftensituated near the hyoid bone. Itmoves on both swallowing andtongue protrusion (see figure 4).
Ultrasound investigation identi-fies and and delineates the cyst andensures the thyroid tissue is normal.This is important because there is asmall chance that the ‘cyst’ will rep-resent an ectopic thyroid gland.
These patients should also be inves-tigated by FNAC.
Treatment is to excise the cystand the tract that extends from thecyst superiorly around the hyoidbone to the tongue base (the latterincludes resection of the middleportion of the hyoid bone). Thisminimises the chance of recur-rences that can be difficult to man-age.�Thyroid lumps When a patienthas a thyroid mass, it is necessary todistinguish a solitary or dominantthyroid nodule (see figure 5) froma goitre (a generalised enlargementof the entire gland – see figure 6).•Goitre The pathology may bephysiological (in which case it
Figure 8Squamous cellcarcinomametastasis –firm nodalmass upperjugular chain
�

732 THE PRACTITIONER, SEPTEMBER 2003, VOL 247
Neck lumps
typically arises during puberty orpregnancy), or due to autoimmunedisease (often with hypo- or hyper-thyroidism), or due to hyperplasia,(which is usually euthyroid and canbe smooth or multinodular withcolloid nodules).
Hyperplasia is usually idiopathicbut can be drug-induced, for exam-ple, from use of carbimazole, ordue to iodine deficiency.
The history is of a painless mid-line neck lump. There may besymptoms of hypo- or hyper-thyroidism; there may also be masseffect from the goitre, most com-monly in the form of a perceptionof a lump in the throat.
Rarely, there may be dysphagiaor stridor. The condition is muchmore common in females.
On examination there is a
smooth or nodular goitre. Thyroidfunction tests reveal thyroid autoan-tibodies. If there appears to besome possibility of a dominant nod-ule, ultrasound examination maybe required(see below). Computedtomography is needed if there arethoracic inlet compression symp-toms.
Most cases need no treatment;however, any underlying thyroiddysfunction should be treated inthe usual way. Surgery (sub- ornear-total thyroidectomy) may benecessary for compression symp-toms, cosmetic concerns or failedendocrine treatment of Graves’ dis-ease. •Solitary or dominant thyroidnodule Some five per cent of theseare malignant neoplasms and maybe papillary, follicular, medullary or
Figure 9Primarysquamous cellcarcinoma oftongue – easilydetected iflooked for inany setting
Figure 10(centre)Primarysquamous cellcarcinoma oflarynx – onlydetectable bylaryngoscopyin neck lumpclinic
anaplastic carcinomas. Othercauses include a benign neoplasm(follicular adenoma), colloid nod-ule, cyst or an autonomous hyper-functional adenoma.
Solitary thyroid nodules mayoccur at any age from young adult-hood onwards. The history is of apainless lump in the neck with orwithout compression symptoms.
On examination there is a soli-tary thyroid lump. Cervical lym-phadenopathy or vocal cord palsyon laryngoscopy suggest malig-nancy.
The lump should be investigatedby FNAC; an ultrasound scan isrequired to delineate the lump fur-ther or to enhance the accuracy ofFNAC. Thyroid function shouldalso be tested.
There is no longer any indica-

THE PRACTITIONER, SEPTEMBER 2003, VOL 247 733
Neck lumps
tion for the routine use of radio-isotope scans for diagnosis.
Where the FNAC reveals malig-nancy the patient is referred to ahead-and-neck oncology team fordefinitive surgical resection. This isusually total thyroidectomy with orwithout neck dissection.
Where the FNAC result is suspi-cious or non-diagnostic it should berepeated. If the result is the same, adiagnostic thyroid lobectomy isrequired.
Where the FNAC result is benignit should be repeated in 6–12months, because of the small possi-bility of a false-negative result.�Cervical lymph node•Lymphoma These are eitherHodgkin’s disease or non-Hodgkin’s lymphoma. the history isof one or more painless neck
Figure 11Apparatus forfine needleaspirationcytology(FNAC)
lumps, with or without constitu-tional symptoms, such as fever,night sweats, fatigue and weightloss. They may occur at any age,including childhood.
On examination there is a rub-bery lymphadenopathy ofteninvolving the posterior triangle (seefigure 7). There may be infraclavic-ular lymph nodes or hepatospleno-megaly.
FNAC may produce suggestiveresults, but biopsy is necessary fordefinitive diagnosis and accuratehistiotyping. A chest X-ray is usefulat an early stage when this diagnosisis suspected.
The treatment depends on his-tiotype and stage (after CT scans,bone marrow trephine), and willcomprise chemotherapy or radio-therapy, or both.
•Cervical lymph node metastasisfrom head and neck cancer Theseare mostly a squamous cell carci-noma (SCC) arising in the upperaerodigestive tract (oral cavity,oropharynx, larynx, hypopharynx,cervical oesophagus or nasophar-ynx) that has metastasised to thecervical lymph nodes. Moreuncommonly, metastases may befrom a cutaneous SCC.
The history is of a lump in theneck with or without symptomsfrom the primary tumour, such ashoarseness, dysphagia, odonopha-gia (painful swallowing), sorethroat or mouth ulcer.
The patient is usually middle-aged and older, and may have ahigh-risk history with regard totobacco and alcohol consumption.
On examination there is a firm �

734 THE PRACTITIONER, SEPTEMBER 2003, VOL 247
Neck lumps
neck lump, especially in the jugularchain (see figure 8). There may besigns of a primary tumour in theoral cavity (see figure 9), orophar-ynx or in the larynx, hypopharynx,tongue base, nasopharynx (on flex-ible endoscopy, see figure 10), or inthe skin or scalp.
Investigations should includeFNAC, biopsies of suspected or pos-sible primary sites, a CT or MR scanfor more accurate staging, and achest X-ray or CT of the thorax toexclude synchronous primary lungcancer or lung metastasis.
Treatment starts with referral toa multidisciplinary head and neckoncology team. When there is a cer-vical lymph node metastasis, treat-ment usually involves surgical neckdissection, whatever the modality oftreatment of the primary tumour(surgery or radiotherapy).•Cervical lymph node metastasisfrom cancer below the claviclesNeck lumps that are supraclavicularlymph nodes may be metastasesfrom infraclavicular sites, such asintra-abdominal malignancy, orfrom the breast or lungs.
FNAC will often suggest malig-nancy but not give histologicalinformation beyond ‘carcinoma’.In this situation primary head andneck cancers, including thyroid,must be excluded. The search for ainfraclavicular primary will includebasic investigations, such as chest X-ray and abdominal ultrasound,and specific investigations accord-ing to symptoms, sex, age of patientand so on. Incisional biopsy may berequired.•Inflammatory cervical lym-phadenitis Cervical lymphadenitisoccurs universally at some point inlife, especially during the firstdecade. When chronic, it is usuallyreactive to ongoing local non-spe-cific viral or bacterial infections.
Specific underlying disease includeEpstein-Barr virus, HIV, granuloma-tous disorders such as TB or catscratch fever, and protozoal agentssuch as toxoplasmosis.
For persistent lymphadenopathyin adults, a full work-up will includethorough head and neck examina-tion, FNAC plus or minus serologi-cal blood testing.
If there is doubt raised in theFNAC or if there is clinical suspi-cion of a specific underlying disor-der, biopsy will help with thediagnosis.
CHILDRENThe above comments regardingcervical lymphadenopathy apply tochildren. In most cases FNAC is notpossible in children. The norm is,therefore, repeated examinationwith excision biopsy reserved forlarge nodes, especially in the poste-rior triangles or supraclavicular fos-sae, rapid increase in size or otherworrying history.
SUBCUTANEOUS LESIONSSubcutaneous lesions arise frommany areas including the neck, themost common being lipoma andsebaceous cysts. The former canoften be left alone if they do notbother the patient and the latterare usually excised.
EXAMINATIONIt is advised that a systematicapproach is adopted towards theexamination of neck lumps. A sug-gested approach is the move fromone area to another, consideringwhich tissue pathology may arisefrom each area.
In figure 1 one would move fromareas A to B and C (includingparotid), then down the jugularchain feeling initially anterior tothe sternocleidomastoid muscle
(C,D,E), anterior compartment ofthe neck (F), back up the jugularchain but now posterior to the ster-nocleidomastoid (C,D,E again) andfinally the posterior triangle of theneck (G) ending up in thesupraclavicular fossa (H).
It is essential that the examina-tion includes the oral cavity andoropharynx, and skin and scalp. Inprimary care, further examinationof the rest of the upper aerodiges-tive tract will not be possible.
THE NECK LUMP CLINIC Secondary care referral should be toa dedicated neck lump clinic. Such aservice should be based upon:•Clinical examination including a
thorough examination of theupper aerodigestive tract, andflexible laryngopharyngoscopy.
•FNAC (see figure 11), preferablywith a ‘hotlab’ facility offeringresults available in about onehour. The experience and auditwithin a dedicated neck lumpclinic will optimise accuracy ofFNAC.
•Ultrasound examination, prefer-ably available within the clinic.
•Access to pan-endoscopy andbiopsy of upper aerodigestivetract under general anaesthetic.
•Links to a multidisciplinary headand neck oncology team.
WARNINGThe practice of early excisionbiopsy of all neck lumps withoutthorough work-up is to be con-demned, but still occurs and is usu-ally performed by surgeons who arenot head-and-neck specialists. Atbest, this may be unnecessary, but atworst, in the case of metastasis fromhead-and-neck cancer, excisionresults in the need to performmore radical salvage surgery andconfers a worse prognosis.
‘When cervical lymphadenitis is chronic, it is usually reactive toongoing local non-specific viral or bacterial infections’
�