Embed Size (px)
Citation preview
CASE PRESENTATIONDEPARTMENT 31
Personal History
Female patient M.A. 65 years old, House wife, married with 14 offspring youngest is 35 years old, living in Elsaff ,with no special habits of medical importance.

Complaint
Pain and swelling of left leg
Present History
Condition started 5 days before admission by pain and swelling of left leg of gradual onset and progressive course, the pain was related to calf, not radiating, bursting, increasing by prolonged standing or walking and decreasing by elevation of the affected leg.
The edema was persistent, increasing by standing and decreasing by elevation of the leg.
The condition is not associated with fever, and not preceeded by trauma, surgical operations or intake of any drugs.
The condition is not associated with chest pain, hemoptysis or dyspnea.
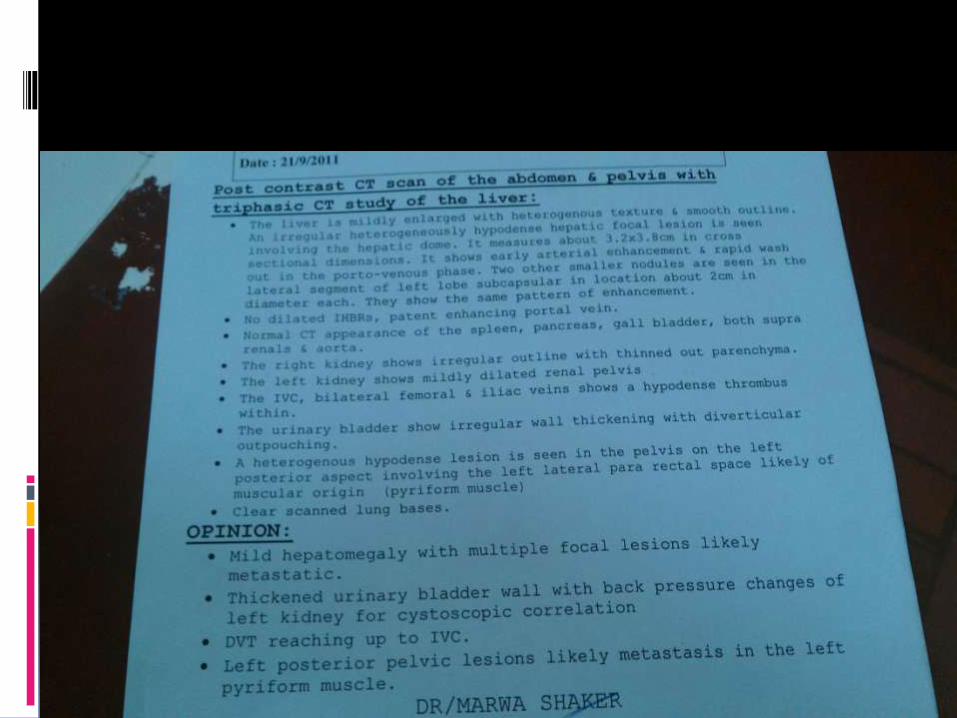
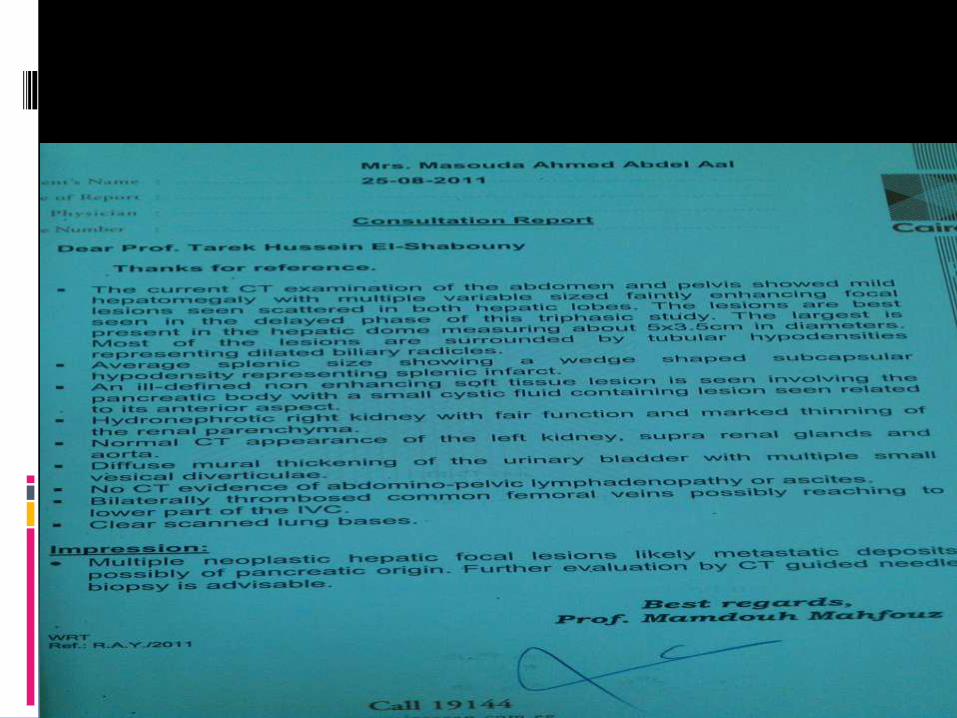
The patient suffered from left hypochondrialstitching pain two Months ago and sought medical care, U/S and CT abdomen were and the condition was diagnosed as multiple splenic and renal infarctions.
No history of:
Arthralgias or arthritis
Photosenstivity
Oral ulcers
Excessive hairfall
No history of:
Rapid weight loss
Generalized body swellings
Severe headache, projectile vomiting or blurring of vision.
Chest pain or hemoptysis.
Right hypochondrial pain or jaundice.
Persistent bony pains.
No history of previous strokes, TIAs, myocardial infarctions, intestinal infarctions or limb ischemia.
No history suggestive of other systemic diseases.
The patient is not known to be hypertensive.
Past History
history of previous similar condition.
History of cataract operation done 20 years ago.
Family History
No similar conditions in the family.
Positive consanguinity.( The parents are cousins.)
Obstetric
No history of previous abortions
EXAMINATION
The patient is fully concious, of average mood, and well oriented to time, place and person.
Examination
Vital Signs:B.p.:120/80Pulse:80, Regular, of average pulse volume, equal bilaterally, with no special character. Peripheral pulsations are intact. Arterial wall is not felt.Temp: 37.5R.R.: 20RBS:269
No jaundice
No Pallor
No cyanosis
Carotid pulsations are of average volume and equal bilaterally
No congested neck veins
No thyroid swelling
No cervical lymphadenopathy
Limb examination
Upper limbs:
No clubbing or cyanosis
No flapping tremors or palmar erythema
Lower limbs:
Left lower limb edema, redness and tenderness
Tense calf muscles of the left lower limb
Palpable dorsalis pedis and posterior tibial
Cardiac examination
Inspection:
Apex lies in the 5th space in the MCL
No visible pulsations
Palpation:
No palpable pulsations or thrills
Auscultation:
Normal S1 and S2
No additional heart sounds
No murmurs, rub or gallop
Chest examination
Inspection:
No scars or sinuses or pigmentation
Palpation:
No tenderness
Normal TVF
Percussion:Normal lung resonance
Upper border of the liver in the 5th
MCL
Auscultation:
Normal vesicular breathing
No wheezes or crepitations
No bilateral basal crepitations
Abdominal examination
Inspection: No pigmentation, scratching marks or
sinuses
Palpation:
Superficial palpation:No rigidity, tenderness or rebound
tenderness.No superficial masses.
Deep palpation:
No palpable organomegaly.
Percussion:
No detectable ascites
Auscultation:
Audible intestinal sounds
Neurological examination
Intact cranial nerves.
Normal tone, power and reflexes.
Intact sensation.
Normal coordination.
Joint examination
Normal range of movement of all joints.
No redness or tenderness of any joints.
Lymph node examination
No cervical, axillary or inguinal lymphadenopathy.
Musculoskeletal examination
No sternal tenderness.

INVESTIGATIONS
LABS

ESR
FIRST HOUR :
52
SECOND HOUR: 89
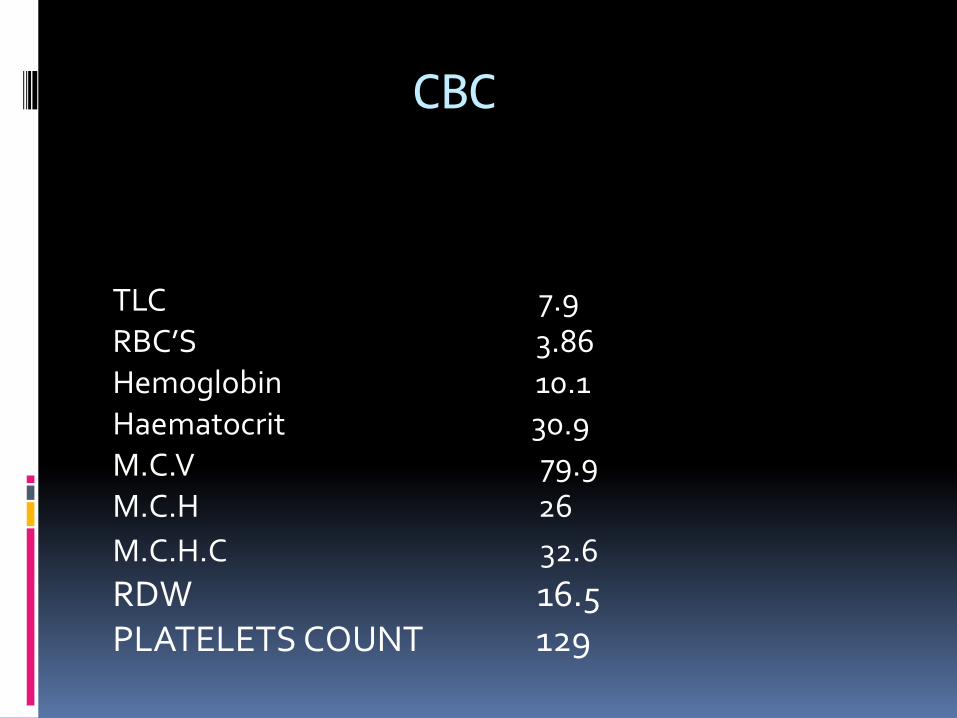
CBC
TLC 7.9RBC’S 3.86Hemoglobin 10.1Haematocrit 30.9M.C.V 79.9 M.C.H 26
M.C.H.C 32.6
RDW 16.5PLATELETS COUNT 129
Mild microcytic hypochromic anemia.
RBCs show anisocytosis.
Mild thrombocytopenia.
Coagulation profile
PT : 23.8
PC : 31.3 %
INR: 1.88
PTT: 38 ( 28-40 sec.)
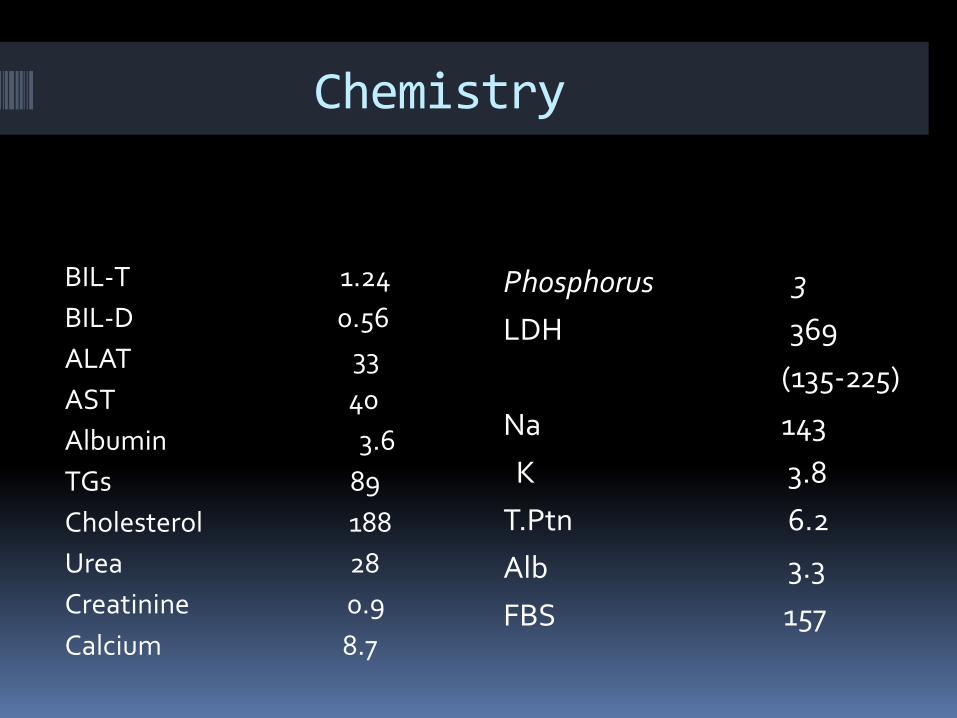
Chemistry
BIL-T 1.24
BIL-D 0.56
ALAT 33
AST 40
Albumin 3.6
TGs 89
Cholesterol 188
Urea 28
Creatinine 0.9
Calcium 8.7
Phosphorus 3
LDH 369
(135-225)
Na 143
K 3.8
T.Ptn 6.2
Alb 3.3
FBS 157
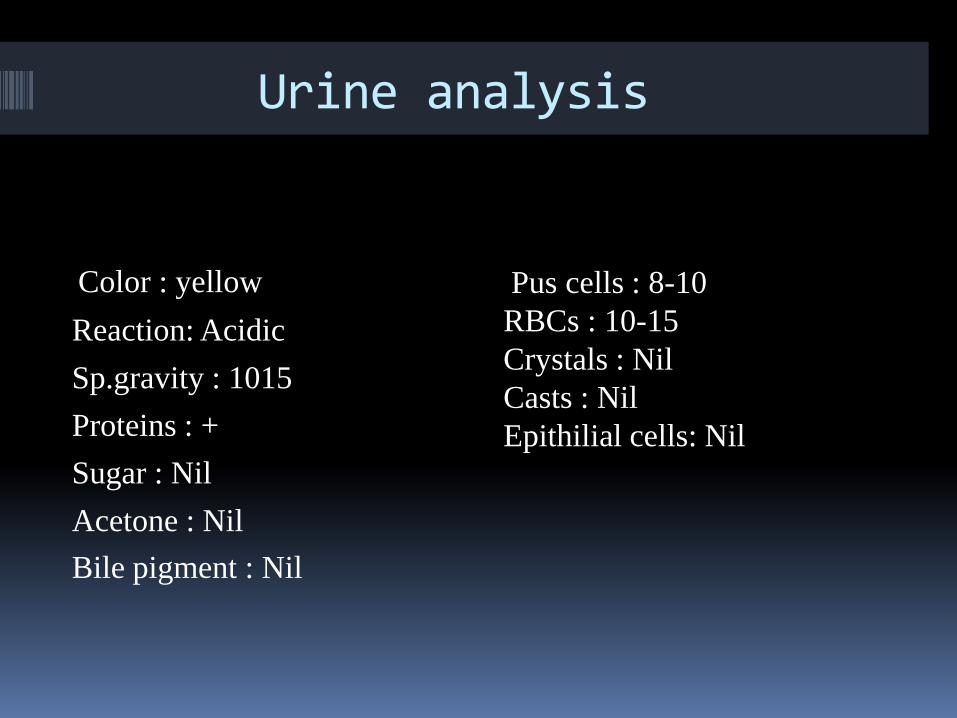
Urine analysis
Color : yellow
Reaction: Acidic
Sp.gravity : 1015
Proteins : +
Sugar : Nil
Acetone : Nil
Bile pigment : Nil
Pus cells : 8-10
RBCs : 10-15
Crystals : Nil
Casts : Nil
Epithilial cells: Nil
Immune profile
ANA : +ve speckled and nucleolar
C4 : 39.9 ( 10-40)
C3 : 159 (90-180)
Anti-ds DNA : Pending
ANCA : Pending
Lupus anticoagulant : 133
Anticardiolipin : Pending
Anti-B2-glycoprotein 1 IgG AM screen :
56 (Up to 10 )
Protein C : 37 ( 82-110)
Protein S: 61 ( 71-113)
Tumor markers
AFP : 2.5
CA 15-5 : Pending
CA19-9 : Pending
CA125 : Pending
IMAGING
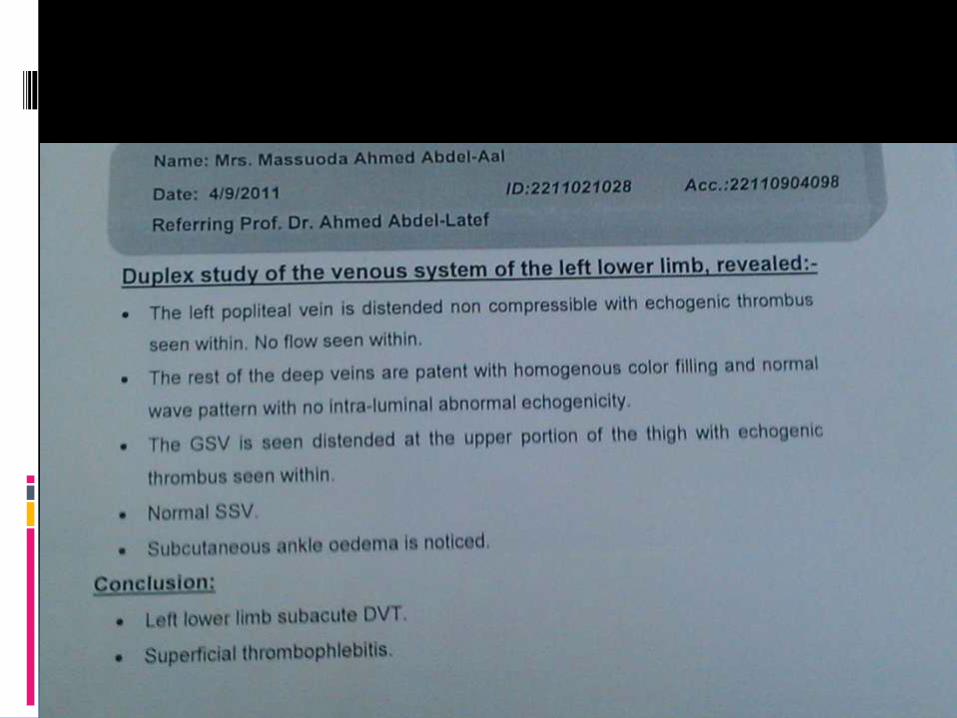
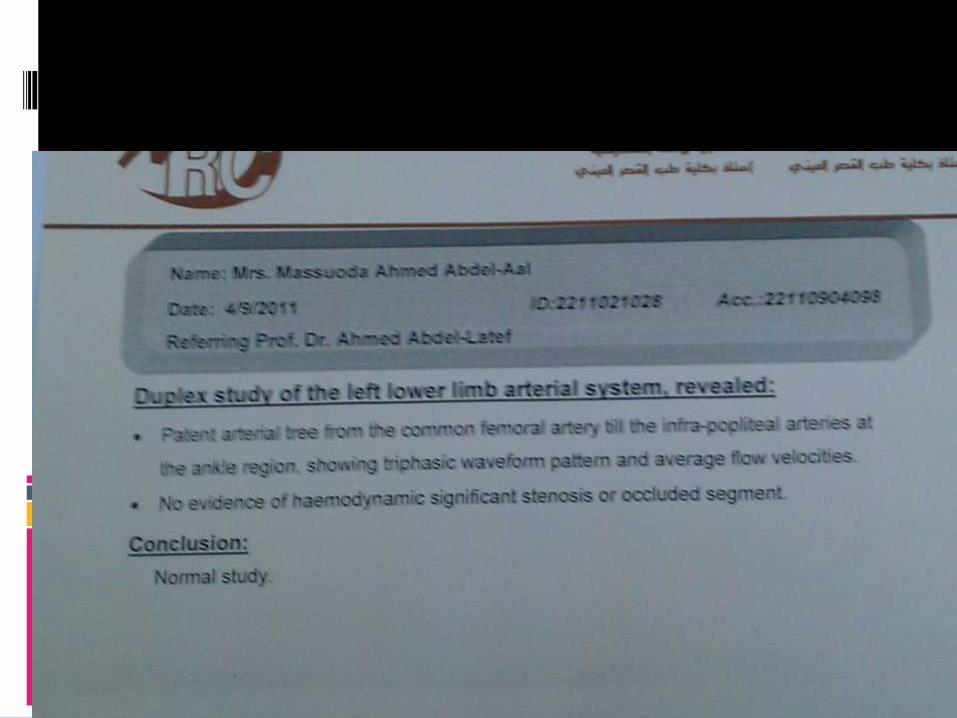
Duplex
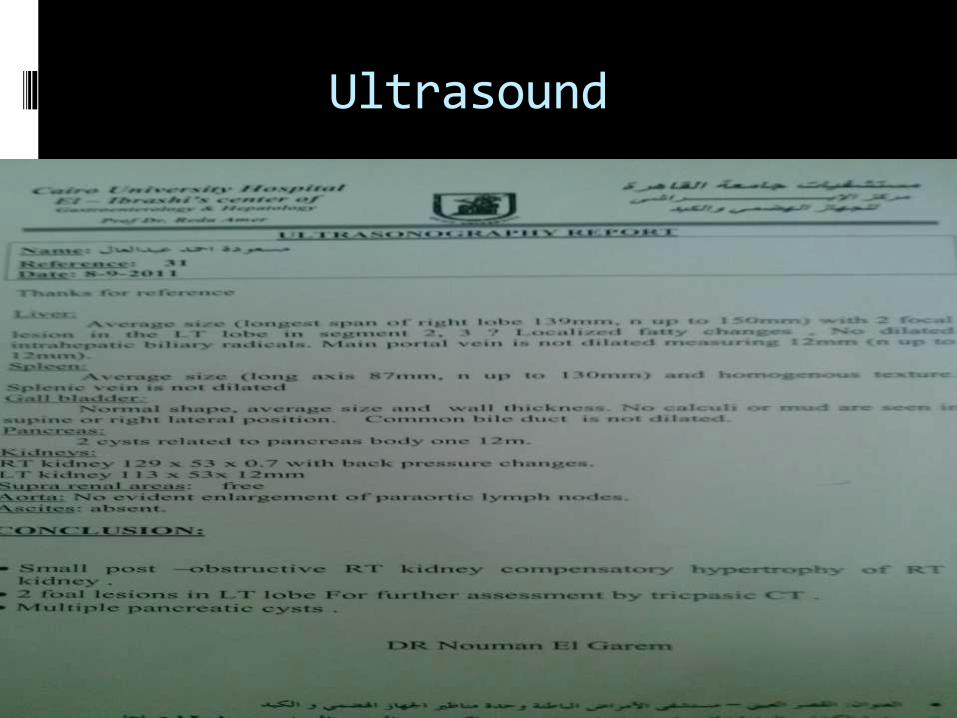
Ultrasound
CT Neck
CT chest
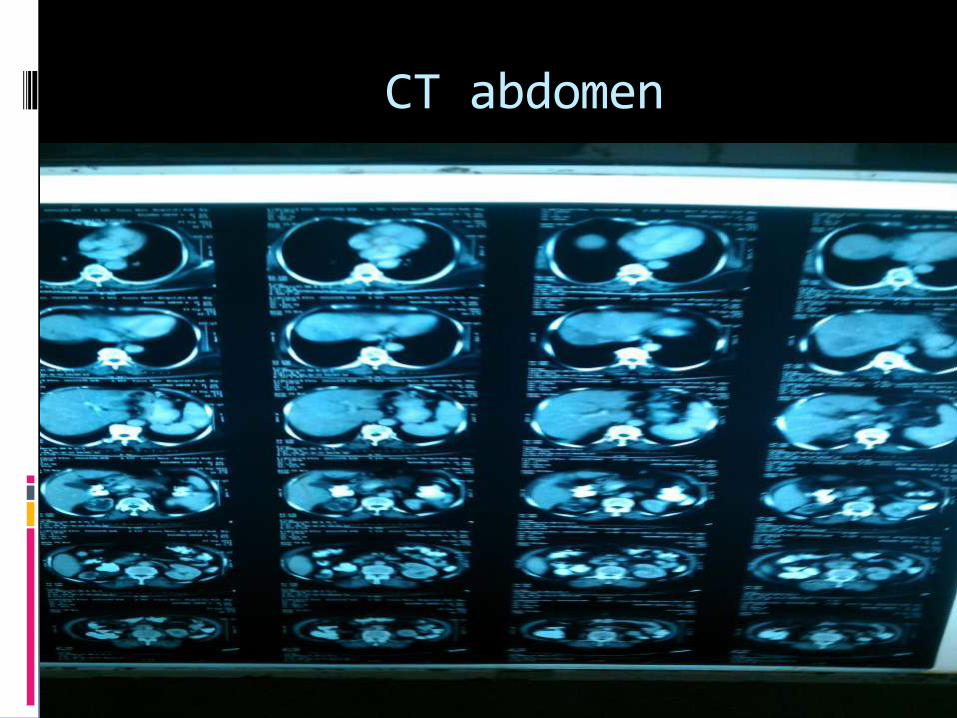
CT abdomen







![Peripartum Cardiomyopathy Acute Heart Failure: … groups A, AB and higher plasmatic levels of factor VIII, vWF and thrombotic events than blood group O[5]. Hypercoagulability state](https://img.pdfslide.net/doc/110x75/5c0cec8309d3f247038cd26d/peripartum-cardiomyopathy-acute-heart-failure-groups-a-ab-and-higher-plasmatic.jpg)





















