Embed Size (px)
DESCRIPTION
Citation preview

Presented by: Dr Vineet ChowdharyModerator: Dr Chandrashekar Chatterji
Hyponatremia And Hypernatremia& its Anaesthetic Implications

Sodium is the most prevalent cation in the extracellular fluid (ECF), with a normal level of around 135- 145mmol/L & intracellular concentration of around 10mmol/L
Total body Sodium is about 5000 mEq in a normal adult person
Responsible for 90% of total osmolality of ECF Daily requirement of sodium is about 100 mEq or 6gm Major function of sodium is to maintain ECF volume and
therefore blood pressure In normal individuals, the kidney strives to achieve
Na+ balance – that is, to have Na+ excretion equal to Na+ ingestion. The long-term control of blood pressure is achieved by the excretion or retention of Na+ (and hence plasma volume) in the kidney
SODIUM REGULATION:PHYSIOLOGICAL
BASIS

Hormones increasing sodium reabsorption:
Renin: - Released from the juxtaglomerular apparatus of the kidney - Release is stimulated by: raised sympathetic tone, falling plasma
volume, and certain prostaglandins, such as PGE2
- No direct effects promoting Na+ retention, it controls the renin-angiotensin-aldosterone axis
Angiotensin II: - Levels rise as result of renin release - In turn, it stimulates the release of aldosterone - Also increases tone in the efferent glomerular arteriole. The net
effect is to enhance Na+ reabsorption from the proximal tubule.
Aldosterone: - Steroid hormone released from the adrenal cortex - End product of the renin-angiotensin-aldosterone system - Acts on the distal tubule and collecting duct to increase Na+ and
water reabsorption (proportionately more Na+ than water)
Hormonal Regulation of Sodium

Arginine vasopressin (AVP), AKA anti-diuretic hormone (ADH):-ADH is produced in neuron cell
bodies in supraoptic and paraventricular nuclei of the Hypothalamus, and stored in posterior pituitary.
- passive absorption of water from the collecting ducts, concentrating the urine
- Causes a small degree of Na+ reabsorption, but the retention of water is proportionately much greater
·

Hormones increasing sodium excretion: Atrial Natriuretic Peptide (ANP): - A small peptide
produced from the atrial wall as a result of atrial stretching due to hypervolaemia
- Acts to increase Na (and hence water) excretion by increasing GFR and blocking Na reabsorption in the proximal collecting duct
Other factors secreted by the hypothalamus, termed brain natriuretic peptides (BNP), may have similar roles.

Types and distributionInclude guanylin, uroguanylin,
lymphoguanylin and exogenous peptide toxin produced by enteric bacteria
FunctionIn gastrointestinal tract, stimulate
epithelial secretion of Cl- and HCO-, causing enhanced secretion of fluid and electrolyte into the intestinal lumen.
in kidney, increase excretion of Na+, Cl-, K+ and water
The Guanylin family

Serum sodium concentration regulation Stimulation of thirst Secretion of ADH
Feedback mechanism of Renin- Angiotensin -Aldosterone Renal handling of filtered sodium
Stimulation of thirst :(a) Increase in osmolality is the main driving force which is sufficient if it increases by 2-3 %. (b) A decrease in blood pressure or volume by 10-15 %
Thirst centre is located in the anterolateral centre of the Hypothalamus
Secretion of ADH is triggered by increase in osmolality by approx 1% or the vol. or pressure of the vascular sytem. This increases the passive absorption of water and urea concentrating the urine.
Renin- Angoitensin- Aldosterone axis acts to cause retention of sodium in the event of decreased osmolarity
Physiology

Definition: Hyponatremia is defined as a plasma Na+ concentration <135 mEq/L
It is due to a relative excess of water in relation to sodium.
It can result from excessive loss of sodium from excessive sweating, vomiting, diarrhoea, burns, and diuretics.
It is a very common disorder, occurring in up to 22% of hospitalized patients.
Result of an increase in circulating AVP and/or increased renal sensitivity to AVP, combined with any intake of free water; a notable exception is hyponatremia due to low solute intake.
HYPONATREMIA

Patients’ intravascular volume status must be evaluated to understand further the underlying problem leading to abnormalities in sodium physiology.
Hyponatremia thus is subdivided diagnostically into three groups, depending on clinical history and volume status: hypovolemic, euvolemic, and hypervolemic

I- Hypo-osmolar hyponatremia (true hyponatremia)Hypovolemic HyponatremiaEuvolemic HyponatremiaHypervolemic Hyponatremia
II- Pseudo hyponatremiaNormal OsmolalityHigh Osmolality
TYPES:

Patient dehydrated; reduction in total body sodium exceeds reduction in total body water
NON RENAL LOSSES ( Urinary Sodium excretion < 20 mEq/L)- Vomiting, Diarrhea, Third space losses, Pancreatitis, Burns
RENAL LOSSES (Urinary Sodium excretion > 20 mEq/L)- The renal causes of hypovolemic hyponatremia share an inappropriate loss of Na+-Cl– in the urine, leading to volume depletion and an increase in circulating AVP. Causes include reflux nephropathy recovery phase of acute tubular necrosis, diuretics ,mineralocorticoid deficiency, osmotic diuresis, ketonuria
Hypovolemic Hyponatremia

“Cerebral salt wasting" : rare cause of hypovolemic hyponatremia, and inappropriate natriuresis in association with intracranial disease
Associated disorders include subarachnoid hemorrhage, traumatic brain injury, craniotomy, encephalitis, and meningitis.
Cerebral salt wasting typically responds to aggressive Na+-Cl– repletion.

Patient has a normal store of sodium but an excess of total body water
The most common form seen in hospitalized patients. The most common cause is the inappropriate administration of hypotonic fluid
The syndrome of inappropriate antidiuresis is the most common cause of euvolemic hyponatremia
Other causes include glucocorticoid therapy, stress, drugs , hypothyroidism.
Euvolemic Hyponatremia

Most common cause of euvolemic hyponatremia
The osmotic threshold and osmotic response curves for sensation of thirst are shifted downward
High levels of ADH are secreted intermittently at an abnormally low threshold or continuously despite low osmolality.
The presence of hyponatremia plus a urine osmolality higher than maximal dilution confirms the diagnosis.
Urinary sodium concentration usually exceeds 30 mEq/L
The fractional excretion of sodium is greater than 1%. Patients with SIADH exhibit a characteristic response
to water restriction; a 2- to 3-kg weight loss is accompanied by correction of hyponatremia and cessation of salt wasting over 2 to 3 days
SIADH


Increase in total body water exceeds increase in total body sodium. Patients are edematous.
RENAL CAUSES(urinary sodium > 20mEq/L): Acute or Chronic renal failure
NON RENAL CAUSES: CHF, Cirrhosis, nephrotic syndrome
Hypervolemic Hyponatremia


Normal Osmolarity - Due to a measurement error which can result when the solid
phase of plasma (that due to lipid and protein) is increased - Typically caused by hypertriglyceridaemia or paraproteinaemia.
High Osmolarity: Translocational hyponatraemia - Occurs when an osmotically active solute that cannot cross the
cell membrane is present in the plasma. -In the case of the insulinopaenic diabetic patient, glucose
cannot enter cells and hence water is displaced across the cell membrane, dehydrating the cells and “diluting” the sodium in the serum.
- This is also the cause of hyponatraemia seen in the TURP syndrome, in which glycine is inadvertently infused to the same effect.
Psuedo hyponatremia


Severity of symptoms depends upon the severity of hyponatremia and the rate at which the sodium concentration is lowered.
Acute – develops in 48 hours or less. Subjected to more severe degrees of cerebral edema
Chronic- develops over 48 hours and brain edema is less and is well tolerated.
The signs and symptoms are due to increase in volume of ICF and increase in volume of brain cells rather than decrease in serum sodium.
CLINICAL FEATURES

SIGNS AND SYMPTOMS OF HYPONATREMIACentral Nervous SystemMild – Apathy ,Headache, LethargyModerate- Disorientation, Psychosis, Agitation,
Ataxia Confusion Severe-Stupor, Coma, Pseudobulbar palsy
Tentorial herniation , Cheyne-Stokes respiration, Death
Gastrointestinal SystemAnorexia, Nausea ,VomitingMusculoskeletal SystemCramps Diminished deep tendon reflexes

History and physical examination- to identify hypovolemic hyponatremia (diarrhoea, vomitting, burns)
Radiologic imaging - to assess whether patients have a pulmonary or CNS cause for hyponatremia. CT scanning of the thorax should be considered in patients at high risk small cell carcinoma
Laboratory tests- Provide important initial clue in the differential diagnosis
1. Plasma Osmolality
2. Urine Osmolality
3. Urine Sodium concentration
4. Uric acid level
5. Serum potassium
6. Serum glucose
DIAGNOSIS

Plasma Osmolality- Normal plasma osmolality is 275-290 mEq/l. >290 mEq/L- hyperglycemia or administration of mannitol 275-290 mEq/L- Hyperlipidemia or hyperproteinemia <275 mEq/L- Evaluate volume status
1. Increased Volume- CHF, Cirrhosis, Nephrotic syndrome
2. Euvolemic- SIADH, Hypothyroidism, psychogenic polydipsia
3. Decreased Volume- GI and 3rd space loss, renal losses
Urine Osmolality- Normal value is > 100 mosmol/kgNormal to high:
Hyperlipidemia, hyperproteinemia, hyperglycemia, SIADH
< 100 mosmol/kgHypo-osmolar hyponatremia -Excessive sweating,
Burns,Vomiting, Diarrhea , Urinary loss

Urine Sodium>20 mEq/L
SIADH, diuretics<20 mEq/L
cirrhosis, nephrosis, congestive heart failure, GI loss, skin, 3rd spacing, psychogenic polydipsia
Uric Acid Level< 4 mg/dl consider SIADH
FeNa(Fractional Excretion of Sodium)Help to determine pre-renal from renal causes
Serum glucose -also should be measured; plasma Na+ concentration falls by 1.6 to 2.4 mM for every 100-mg/dL increase in glucose due to glucose-induced water efflux from cells; this "true" hyponatremia resolves after correction of hyperglycemia
Serum Potassium: Hyperkalemia- Renal insufficiency or Adrenal insufficiency with hypoaldosteronism
Hypokalemia- with metabolic acidosis suggests vomiting or diuretic therapy

Treatment needs to be individualized considering etiology, rate of development, severity and clinical signs and symptoms
Hyponatremia which developed quickly needs to be treated fast whereas slow developing hyponatremia should be corrected slowly
GOALS of THERAPY:
1. To raise the plasma sodium concentration at a slow rate
2. To replace sodium or potassium deficit or both
3. To correct underlying etiology
BASIC PRINCIPLES OF CORRECTION: Rapid correction is indicated in acute (<48hours) symptomatic
or severe hyponatremia.(serum Na <120 mEq/L) In chronic cases patients are at little risk, however rapid
correction can lead to demylination. Use slower acting therapies like water restriction
TREATMENT

Treatment of acute symptomatic hyponatremia Hypertonic 3% saline (513 mM) to acutely increase plasma
Na+ concentration by 1–2 mM/h to a total of 4–6 mM; alleviate severe acute symptoms, after which corrective guidelines for "chronic" hyponatremia are appropriate
The increase in plasma Na+ concentration can be highly unpredictable during treatment ,plasma Na+ concentration should be monitored every 2–4 h during treatment
Vasopressin antagonists do not have an approved role in the management of acute hyponatremia.
Treatment of chronic hyponatremia Rate of correction should be comparatively slow <8–10 mM in the first 24 h and <18 mM in the first 48 h to
avoid ODS

Hypovolemic hyponatremia will respond to intravenous hydration with isotonic normal saline, with a rapid reduction in circulating AVP and a brisk water diuresis. Diuretics induced hyponatremia is treated with saline and potassium supplementation
Hypervolemic hyponatremia responds to no salt, water restriction(intake< urine output), and loop diuretics
Euvolemic hyponatremia will respond to successful treatment of the underlying cause, with an increase in plasma Na+ concentration
Regardless of the initial rate of correction, chosen acute treatment is stopped once
1. patient’s symptoms are abolished 2. A safe plasma sodium (120-125 mEq/L) is achieved

SPECIFIC THERAPY:1. Removal of responsible drugs- diuretics, chlorproamide
etc2. Management of physical stress or post operative pain3. Specific treatment of underlying cause4. Vasopressin antagonists (vaptans) are highly effective in
treating SIAD and hypervolemic hyponatremia, reliably increasing plasma Na+ concentration as a result of their aquaretic effects (augmentation of free-water clearance). Most of these agents specifically antagonize theV2 vasopressin receptor
TO CALCULATE NEED OF REPLACEMENT SODIUM CONTAINING FLUID:0.9% saline (154mEq/L) and 3% NaCl- hypertonic saline
(513 mEq/L) are the only two routinely used I.V. fluids . However 0.9% NS is not used to correct hyponatremia in SIADH

estimate SNa change on the basis of the amount of Na in the infusate
ΔSNa = {[Na + K]inf − SNa} ÷ (TBW + 1)ΔSNa is a change in SNa[Na + K]inf is infusate Na and K concentration
in 1 liter of solution
Total Body Water= 0.6* B.W(kg) in children and nonelderly man
=0.5*B.W.(kg) in nonelderly woman and elderly man
=0.45*B.W.(kg) in elderly women

Asymptomatic or ChronicSIADH
response to isotonic saline is different in the SIADH
In hypovolemia both the sodium and water are retained
Sodium handling is intact in SIADHAdministered sodium will be excreted in the
urine, while some of the water may be retained possibly worsening the hyponatremia
Water restriction 0.5-1 liter/day
Salt tabletsDemeclocycline
Inhibits the effects of ADHOnset of action may require up to one week

Hypernatremia is defined as an increase in the plasma Na+ concentration to >145 mM. Considerably less common than hyponatremia, hypernatremia nonetheless is associated with mortality rates as high as 40–60%.Hypernatremia is caused by a relative deficit of water in relation to sodium which can result fromNet water loss: accounts for majority of cases
pure water loss hypotonic fluid loss
Hypertonic gain results from iatrogenic sodium loading
HYPERNATREMIA

Net water lossPure water loss•Unreplaced insensible losses (dermal and respiratory)•Hypodipsia•Neurogenic diabetes insipidus
Post-traumatic tumors, cysts, histiocytosis, tuberculosis, sarcoidosis Idiopathic aneurysms, meningitis, encephalitis, Guillain-Barre´ syndrome
Congenital nephrogenic diabetes insipidusAcquired nephrogenic diabetes insipidus
Renal disease (e.g. medullary cystic disease) Hypercalcemia or hypokalemia Drugs (lithium, methoxyflurane, amphotericin B,
vasopressin V2-receptor antagonists)
Causes of Hypernatremia

Hypotonic fluid loss• Renal causes
Loop diureticsOsmotic diuresis (glucose, urea, mannitol)Post obstructive diuresisPolyuric phase of acute tubular necrosis
• Gastrointestinal causesVomitingNasogastric drainageEntero cutaneous fistulaDiarrheaUse of osmotic cathartic agents (e.g., lactulose)
• Cutaneous causesBurnsExcessive sweating

Hypertonic sodium gainHypertonic sodium bicarbonate infusionIngestion of sodium chlorideIngestion of sea waterHypertonic sodium chloride infusionPrimary hyper-aldosteronismCushing’s syndrome

The symptoms of hypernatremia are predominantly neurologic.
Altered mental status is the most common manifestation, ranging from mild confusion and lethargy to deep coma.
The sudden shrinkage of brain cells in acute hypernatremia may lead to parenchymal or subarachnoid haemorrhages and/or subdural hematomas; however, these vascular complications are encountered primarily in paediatric and neonatal patients
Osmotic damage to muscle membranes also can lead to hypernatremic rhabdomyolysis
Clinical Features

HISTORY AND PHYSICAL EXAMINATION: The history should focus on the presence or absence of thirst,
polyuria, and/or an extrarenal source for water loss, such as diarrhoea
The physical examination should include a detailed neurologic exam and an assessment of the ECFV; patients may be hypovolemic, with reduced JVP and orthostasis
Accurate documentation of daily fluid intake and daily urine output
LAB INVESTIGATIONS: Measurement of serum and urine osmolality in addition to urine
electrolytes
- The appropriate response to hypernatremia and a serum osmolality >295 mosmol/kg is an increase in circulating AVP and the excretion of low volumes (<500 mL/d) of maximally concentrated urine, i.e., urine with osmolality >800 mosmol/kg
DIAGNOSIS

Diabetes insipidus may result from a deficiency of ADH (vasopressin) or inability of the kidney to produce a hypertonic medullary interstitium
Diabetes insipidus is characterized by production of a large volume of dilute urine.
Deficiency of vasopressin is known as central diabetes insipidus .Vasopressin deficiency is seen after pituitary surgery, basal skull fracture, and severe head injury.
Nephrogenic diabetes insipidus is defined as renal tubule cell insensitivity to the effects of vasopressin.
In patients with DI a significant amount of body water is lost in a short period, which can cause profound hypovolemia
Diabetes Insipidus

Patients with continued urine output of more than 100 mL/hr who develop hypernatremia should be evaluated for diabetes insipidus by determining the osmolalities of urine and serum.
If the urine osmolality is less than 300 mOsm/L, and serum sodium exceeds 150 mEq/L, the diagnosis of diabetes insipidus is likely.
Patients with central DI should respond to the administration of intravenous, intranasal, or oral Desmopressin.
Patients with NDI due to lithium may reduce their polyuria with amiloride (2.5–10 mg/d)
Thiazides may reduce polyuria due to NDI Occasionally (NSAIDs) have been used to treat
polyuria associated with NDI

A two-pronged approach: Addressing the underlying causeCorrecting the prevailing hypertonicity
RATE OF CORRECTION:
Hypernatremia that developed over a period of hours (accidental loading)
Rapid correction improves prognosis without cerebral edema
Reducing Na+ by 1 mmol/L/hr appropriate
Hypernatremia of prolonged or unknown durationa slow pace of correction prudentmaximum rate 0.5 mmol/L/hr to prevent cerebral
edemaA targeted fall in Na+ of 10 mmol/L/24 hr
Management

Reduce serum sodium concentration to 145 mmol/LMake allowance for ongoing obligatory or incidental
losses of hypotonic fluids that will aggravate the hypernatremia
In patients with seizures prompt anticonvulsant therapy and adequate ventilation
Administration of FluidsWater ideally should be administered by mouth or by
nasogastric tube as the most direct way to provide free water, i.e., water without electrolytes.
Alternatively, patients can receive free water in dextrose-containing IV solutions such as 5% dextrose
Goal of Treatment

Hypernatremia with ECF vol contraction- Isotonic saline is given initially till ECF vol is restored. Subsequently water deficit can be replaced with water by mouth or I.V. 5% dextrose or 0.45% NaCl
Hypernatremia with increased ECF volume: since hypernatremia is secondary to solute administration it can be rapidly corrected . Patients are volume overloaded- loop diuretic is given along with water to remove sodium excess

If at all possible, hyponatremia, especially if symptomatic, should be corrected prior to surgery. Level above 130mEq/L is considered safe
If lower than 130 mEq/L it can be the cause of :-1. Cerebral edema2. Decreased MAC3. Post op agitation and confusion4. Problems of hypervolemia
If the surgery is urgent, then appropriate corrective treatment should continue throughout the surgery and into the postoperative period.
ANAESTHETIC IMPLICATIONS OF HYPONATREMIA

Frequent measurement of serum sodium is necessary to avoid overly rapid correction of hyponatremia with resultant osmotic demyelination or overcorrection resulting in hypernatremia.
Treatment of the underlying cause of the hyponatremia should also continue throughout the perioperative period.
Induction and maintenance of anesthesia in patients with hypovolemic hyponatremia are fraught with the risk of hypotension. In addition to fluid therapy, vasopressors and/or inotropes may be required to treat the hypotension
Hypovolemic patients are sensitive to the vasodilating and negative inotropic effects of the volatile anesthetics, barbiturates, and agents associated with histamine release (morphine, meperidine, curare, atracurium).

Dosage requirements for other drugs must also be reduced to compensate for decreases in their volume of distribution. Hypovolemic patients are particularly sensitive to sympathetic blockade from spinal or epidural anesthesia.
If an anesthetic must be administered prior to complete correction of the hypovolemia, ketamine may be the induction agent of choice for general anesthesia; etomidate may be a suitable alternative.

It involves the resection of the prostate via a cystoscope with continuous irrigation of the bladder.
The irrigating fluid is a nonelectrolyte fluid containing glycine, sorbitol, or mannitol, and this fluid may be absorbed rapidly causing volume overload, hyponatremia, and hypo-osmolality.
An awake patient permits detection of the signs of hyponatremia, including nausea, vomiting, visual disturbances, depressed level of consciousness, agitation, confusion, coma, seizures, muscle cramps, and death.
In TURP syndrome-

Cerebral edema occurs at or below a serum level of 123 mEq/L, and cardiac symptoms occur at 100 mEq/L. It can result in pulmonary edema, hypertension, and heart failure.[19]
Monitoring - direct neurologic assessment in the patient under regional anesthesia
- Measurement of serum sodium concentration and osmolality in the patient under general anesthesia.Treatment -Terminating the surgical procedure -Diuretics if needed for relief of cardiovascular symptoms- Hypertonic saline administration if severe neurologic symptoms are present or the serum sodium concentration is less than 120 mEq/L.

Overly rapid correction of hyponatremia (>8–10 mM in 24 h or 18 mM in 48 h) also is associated with a disruption in integrity of the blood-brain barrier.
The lesions of ODS classically affect the ponsClinically, patients with central pontine myelinolysis
can present one or more days after overcorrection of hyponatremia with para- or quadraparesis, dysphagia, dysarthria, diplopia, a "locked-in syndrome," and/or loss of consciousness.
Other regions of the brain also can be involved in ODS.
In order of frequency, the lesions of extrapontine myelinolysis can occur in the cerebellum, lateral geniculate body, thalamus, putamen, and cerebral cortex or subcortex.
OSMOTIC DEMYLINATION SYNDROME

Development of ataxia, mutism, parkinsonism, dystonia, and catatonia is seen in these
Relowering of plasma Na+ concentration after overly rapid correction can prevent or attenuate ODS
However, even appropriately slow correction can be associated with ODS, particularly in patients with additional risk factors; these factors include alcoholism, malnutrition, hypokalemia, and liver transplantation.

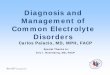
(a) Normal MRI scan taken five months before the episode of severe hyponatremia, when serum sodium was 140
mmol/l. (b) Ten days after the episode of severe hyponatremia, MRI scan showed bilateral high-intensity abnormalities in the lenticular nuclei and in the head of the caudate nucleus (arrows). (c) At day 32, the lesions shown in panel b appear more pronounced (arrows). (d) At day 32 with fluid-attenuation inversion recovery, high intensity lesions were also observed in the precentral gyrus (arrows)
Severe hyponatremia followed by extrapontine myelinolysis

Osmolar gap is considered significant when the difference between the measured and calculated osmolarity is > 10
Some critically ill patients have an unexplained osmolar gap which is thought to result from escape of osmotically active intracellular solutes into extracellular fluid
Increased membrane permeability to Na and decreased active removal of sodium from the cells by energy dependent cation exchange pump leads to redistribution hyponatremia with increased osmolar gap- a concept called sick cell syndrome.
This state has been described during a great variety of human diseases such as traumatic shock, diabetic ketoacidosis, lactic acidosis and multiple organ failure
Both the osmolar gap and hyponatremia correct simultaneously in this condition as the primary illness is treated
Sick Cell Syndrome

If at all possible, surgery should be delayed until the hypernatremia has been corrected or at least until symptoms have abated.
Frequent serum sodium measurements will be required perioperatively, and invasive hemodynamic monitoring may be useful.
Hypovolemia will be exacerbated by induction and maintenance of anesthesia and prompt correction of hypotension with fluids, vasopressors, and/or inotropes may be required.
Increased MAC seen in animal studies
ANAESTHETIC IMPLICATION OF HYPERNATREMIA

THANK YOU