Embed Size (px)
Citation preview

HYPOXIA AND OXYGEN HYPOXIA AND OXYGEN THERAPYTHERAPY
PRESENTER : DR ANURADHAPRESENTER : DR ANURADHA
MODERATOR : DR SHAILA MODERATOR : DR SHAILA KAMATHKAMATH

QUICK DEFINITION OF HYPOXIAQUICK DEFINITION OF HYPOXIA
INADEQUATE O2 SUPPLY TO THE BODY INADEQUATE O2 SUPPLY TO THE BODY TISSUESTISSUES
(ENTIRE BODY) OR (LOCALIZED REGION)(ENTIRE BODY) OR (LOCALIZED REGION)
HYPOXIA MEANS

SYMPTOMS OF HYPOXIASYMPTOMS OF HYPOXIA
• DEPEND ON:DEPEND ON:
RAPIDITY AND SEVERITYRAPIDITY AND SEVERITY
OF THEOF THE
DECREASE OF ARTERIAL Po2DECREASE OF ARTERIAL Po2

1) FULMINANT1) FULMINANT hypoxia hypoxia (Arterial Po2<20mmHg)(Arterial Po2<20mmHg)
(eg.aircraft loses cabin pressure above 30,000 feet and no supplemental O2 available)(eg.aircraft loses cabin pressure above 30,000 feet and no supplemental O2 available)
Occurs in seconds Unconsciousness in 15-20 sec Occurs in seconds Unconsciousness in 15-20 sec Brain death in 4-5 minBrain death in 4-5 min
2) ACUTE 2) ACUTE hypoxiahypoxia(25mmHg<Arterial Po2<40mmHg)(25mmHg<Arterial Po2<40mmHg)
(eg.altitudesof 18,000-25,000 feet)(eg.altitudesof 18,000-25,000 feet)
Symptoms similar to those of ethyl alcohol(lack of coordination,slowed Symptoms similar to those of ethyl alcohol(lack of coordination,slowed reflexes,overconfidence)reflexes,overconfidence)
UnconsciousnessUnconsciousness
Coma and death(in minutes to hours)Coma and death(in minutes to hours) if the regulatory mechanisms of the body are inadequate if the regulatory mechanisms of the body are inadequate
eventually

3) CHRONIC 3) CHRONIC hypoxiahypoxia
(40mmHg<Arterial Po2<60mmHg)(40mmHg<Arterial Po2<60mmHg)(eg.at altitudes of 10,000-18,000 feet for extended periods of time)(eg.at altitudes of 10,000-18,000 feet for extended periods of time)
FOR EXTENDED PERIODS OF TIME!!!FOR EXTENDED PERIODS OF TIME!!!
Most clinical causes of hypoxia are in these categoryMost clinical causes of hypoxia are in these category
Symptoms similar to those of Symptoms similar to those of severe fatiguesevere fatigue
DYSPNEADYSPNEA
SHORTNESS OF BREATHSHORTNESS OF BREATH
+ +
RESPIRATORY ARRHYTHMIASRESPIRATORY ARRHYTHMIAS

SIGNS OF HYPOXIASIGNS OF HYPOXIA
1. Cyanosis 1. Cyanosis (bluish color of tissue)(bluish color of tissue) caused by more than 5g of deoxyhemoglobin/dl in capillary blood(or caused by more than 5g of deoxyhemoglobin/dl in capillary blood(or
less than 13ml O2 per 100ml of blood)less than 13ml O2 per 100ml of blood)
NOT RELIABLE SIGN OF HYPOXIA!!!NOT RELIABLE SIGN OF HYPOXIA!!!
ANEMIC PATIENTS ANEMIC PATIENTS never developnever develop
cyanosis but are extremely hypoxiccyanosis but are extremely hypoxic
PATIENTS WITH POLYCYTHEMIAPATIENTS WITH POLYCYTHEMIA may be may be
cyanotic but they are perfectly oxygenated cyanotic but they are perfectly oxygenated
2.2. TachycardiaTachycardia
(peripheral chemoreceptor reflex response to Po2 )(peripheral chemoreceptor reflex response to Po2 )
3. Tachypnea and Hyperpnea 3. Tachypnea and Hyperpnea (arterial chemoreceptor reflex response to (arterial chemoreceptor reflex response to
Po2 ) Po2 )

TYPES OF HYPOXIATYPES OF HYPOXIA

ARTERIAL(HYPOXIC) HYPOXIAARTERIAL(HYPOXIC) HYPOXIARESULTS FROM:RESULTS FROM:
INADEQUATE OXYGENATION OF THE ARTERIALINADEQUATE OXYGENATION OF THE ARTERIAL BLOODBLOOD
CAUSED BY:CAUSED BY:
1)1) Breathing gas with Po2Breathing gas with Po2
2)2) One or more pathophysiologic mechanisms:One or more pathophysiologic mechanisms:
a) HYPOVENTILATION a) HYPOVENTILATION (not adequate alveolar ventilation)(not adequate alveolar ventilation) alveolar and arterial Po2 alveolar and arterial Pco2alveolar and arterial Po2 alveolar and arterial Pco2 Hypercapnia Hypercapnia
so
b)DIFFUSION LIMITATION b)DIFFUSION LIMITATION
(diffusion capacity of lungs decreased by a pulmonary disease)(diffusion capacity of lungs decreased by a pulmonary disease)

c) PHYSIOLOGIC SHUNTS [ c) PHYSIOLOGIC SHUNTS [ VVAA/Q imbalance/Q imbalance ] ]
most common cause of hypoxiamost common cause of hypoxia d) ANATOMIC SHUNTS d) ANATOMIC SHUNTS (mixing of venous and oxygenated(arterial)blood (mixing of venous and oxygenated(arterial)blood
which dicreases the Po2)which dicreases the Po2)
normallynormally there is an there is an anatomic shunt of about 3%anatomic shunt of about 3% of the cardiac outputof the cardiac output caused caused by the mixing of the oxygenated blood coming from the lungs with the venous blood by the mixing of the oxygenated blood coming from the lungs with the venous blood of bronchial veins before entering the left atriumof bronchial veins before entering the left atrium
Pathologically is caused by Pathologically is caused by congenital cardiac malformations congenital cardiac malformations
diagnosis: arterial Po2<500mmHg when breathing 100% O2diagnosis: arterial Po2<500mmHg when breathing 100% O2

Po2(mmHg)
O2
in b
lood
(vol
umes
%)
ARTERIAL(HYPOXIC)HYPOXIA
Arterial Po2 Venous Po2

STAGNANT(ISCHEMIC) HYPOXIASTAGNANT(ISCHEMIC) HYPOXIA
RESULTS FROM:RESULTS FROM:
INADEQUATE BLOOD FLOWINADEQUATE BLOOD FLOW
entire body or localized areaentire body or localized area
caused by caused by
Congestive heart failureCongestive heart failure ArteriosclerosisArteriosclerosis
Arterial Po2 may be normal BUT because Q (blood flow),tissues Arterial Po2 may be normal BUT because Q (blood flow),tissues withdraw larger amounts of O2 from the blood ,so, Venous Po2withdraw larger amounts of O2 from the blood ,so, Venous Po2

Po2(mmHg)
O2
in b
lood
(vol
umes
%)
STAGNANT(ISCHEMIC)HYPOXIA
Arterial Po2
Venous Po2
BUT

ANEMIC HYPOXIAANEMIC HYPOXIA
RESULTS FROM:RESULTS FROM:
INSUFFICIENT AMOUNT OF FUNCTIONAL HEMOGLOBININSUFFICIENT AMOUNT OF FUNCTIONAL HEMOGLOBIN
CAUSED BY:CAUSED BY:
1) Deficiency of essential nutrients(iron,B12 vitamin)1) Deficiency of essential nutrients(iron,B12 vitamin) 2) Blood loss2) Blood loss
Patients with Anemic hypoxia have Patients with Anemic hypoxia have reduced O2 capacityreduced O2 capacity so they have so they have
reduced content of O2reduced content of O2 in their blood in their blood
Arterial Po2is Normal but Venous Po2Arterial Po2is Normal but Venous Po2

ANEMIC HYPOXIAANEMIC HYPOXIA
Po2(mmHg)
O2
in b
lood
(vol
umes
%)
Arterial Po2 BUT Venous Po2

HISTOTOXIC HYPOXIAHISTOTOXIC HYPOXIA
RESULTS FROM: RESULTS FROM:
DISABILITY OF CELLS TO USE O2DISABILITY OF CELLS TO USE O2
CAUSED BY:CAUSED BY:
1) INACTIVATION OF CERTAIN METABOLIC ENZYMES1) INACTIVATION OF CERTAIN METABOLIC ENZYMES
2) CHEMICAL POISONS2) CHEMICAL POISONS
Tissues are unable to use O2 so Tissues are unable to use O2 so Venous Po2Venous Po2

HISTOTOXIC HYPOXIAHISTOTOXIC HYPOXIA
Po2(mmHg)
O2
in b
lood
(vol
umes
%)
Arterial Po2 Venous Po2 BUT

SUMMARYSUMMARY
TYPE OF TYPE OF HYPOXIAHYPOXIA
ArteriArterial Po2al Po2
VenouVenous Po2s Po2
ArteriArterial al Pco2Pco2
Arterial Po2 Arterial Po2 during during exerciseexercise
Effect of Effect of 100% O2100% O2
ARTERIAL ARTERIAL HYPOXIAHYPOXIA HypoventilationHypoventilation
Arterial Arterial Pco2Pco2
Diffusion Diffusion limitationlimitation
Arterial Arterial Po2>600mmPo2>600mmHgHg
Physiologic Physiologic shuntshunt
Arterial Arterial Po2>600mmPo2>600mmHgHg
Anatomic shuntAnatomic shunt Arterial Arterial Po2<500mmPo2<500mmHgHg
STAGNANT STAGNANT HYPOXIAHYPOXIA
dissolved dissolved O2O2
ANEMIC ANEMIC HYPOXIAHYPOXIA
dissolved dissolved O2O2
HISTOTOXIC HISTOTOXIC HYPOXIAHYPOXIA
dissolved dissolved O2O2

OXYGEN THERAPYOXYGEN THERAPY• Oxygen is required for aerobic Oxygen is required for aerobic
metabolism to produce biological energymetabolism to produce biological energy
• With inadequate oxygenation, anaerobic With inadequate oxygenation, anaerobic metabolism sets in →→ decreased energy metabolism sets in →→ decreased energy and acidosisand acidosis
• Oxygen therapy is thus required Oxygen therapy is thus required whenever tissue oxygenation is whenever tissue oxygenation is impaired, to allow metabolic reactions to impaired, to allow metabolic reactions to occur and to prevent complications of occur and to prevent complications of hypoxemiahypoxemia

AARC CLINICAL PRACTICE AARC CLINICAL PRACTICE GUIDELINESGUIDELINES
• INDICATIONS:INDICATIONS:1.1. Documented hypoxemiaDocumented hypoxemia2.2. Severe traumaSevere trauma3.3. Acute MIAcute MI4.4. Acute care situations leading to Acute care situations leading to
hypoxemiahypoxemia5.5. Short term therapy e.g. post Short term therapy e.g. post
anesthesia recoveryanesthesia recovery• CONTRAINDICATION:CONTRAINDICATION: none specific when indications are none specific when indications are
presentpresent

Oxygen Delivery System: Oxygen Delivery System: Design and Performance.Design and Performance.
• 4 basic designs exist4 basic designs exist• Low flow,Reservoir,High flow and Low flow,Reservoir,High flow and
Enclosures.Enclosures.• Clinical performance is more important Clinical performance is more important
than the design.than the design.• Two key questions are important : Fio2 Two key questions are important : Fio2
range and whether the Fio2 remains fixed range and whether the Fio2 remains fixed or variable.or variable.

• LOW FLOW SYSTEMS : Fio2 less than 35%.LOW FLOW SYSTEMS : Fio2 less than 35%.
• MODERATE : Fio2 between 35% to 60%.MODERATE : Fio2 between 35% to 60%.
• High flow : Fio2 more than 60%.High flow : Fio2 more than 60%.
• Fixed or variable Fio2 depends on how Fixed or variable Fio2 depends on how much of the patients inspired gas the much of the patients inspired gas the system supplies.system supplies.

FIXED AND VARIABLE FIXED AND VARIABLE PERFORMANCE SYSTEMPERFORMANCE SYSTEM• Fixed performance system provides a Fixed performance system provides a
stable Fio2.stable Fio2.• Variable performance system -Inspired gas Variable performance system -Inspired gas
is a mixture of the delivered O2 diluted is a mixture of the delivered O2 diluted with a variable amount of air.with a variable amount of air.
• The more the patient breathes the more The more the patient breathes the more air dilutes the delivered O2 and lower is air dilutes the delivered O2 and lower is the Fio2. the Fio2.
• The Fio2 provided varies from min to min The Fio2 provided varies from min to min and even from breath to breath.and even from breath to breath.

• LOW FLOW SYSTEMS : Variable LOW FLOW SYSTEMS : Variable performance system.performance system.
• RESERVOIR SYSTEM : Can function as a RESERVOIR SYSTEM : Can function as a fixed performance system.fixed performance system.
The reservoir volume must exceed the The reservoir volume must exceed the patients tidal volume and no air leaks patients tidal volume and no air leaks should be present.should be present.
• HIGH FLOW SYSTEM : Fixed performance HIGH FLOW SYSTEM : Fixed performance system.system.

LOW FLOW SYSTEMSLOW FLOW SYSTEMS
• O2 delivered is always less than the O2 delivered is always less than the patients inspired flow(8L/min or less).patients inspired flow(8L/min or less).
• The remaining inspired flow comes The remaining inspired flow comes from the atmospheric air,diluting the from the atmospheric air,diluting the delivered O2.delivered O2.
• Thus they are Variable performance Thus they are Variable performance system.system.

Types of low flow delivery Types of low flow delivery systems.systems.• NASAL CANNULA : small bore oxygen NASAL CANNULA : small bore oxygen
supply tube connected to two short supply tube connected to two short prongs(approx 1cm long).prongs(approx 1cm long).
• Prongs are inserted to the patients nares Prongs are inserted to the patients nares and supply tubing either directly to the and supply tubing either directly to the flow meter or bubble humidifier.flow meter or bubble humidifier.
• Humidifier is used only if the input flow Humidifier is used only if the input flow exceeds 4L/min.exceeds 4L/min.

• Fio2 range is between 22% to 45%.Fio2 range is between 22% to 45%.
• Flows greater than 6 to 8L/min can Flows greater than 6 to 8L/min can cause patient discomfort including cause patient discomfort including dryness and bleeding.dryness and bleeding.
• In newborns and infants flows should In newborns and infants flows should be 2L/min or less.be 2L/min or less.

DISADVANTAGES OF NASAL DISADVANTAGES OF NASAL CATHETERCATHETER• They are unstable,easily dislodged.They are unstable,easily dislodged.• High flows are uncomfortable ; can High flows are uncomfortable ; can
cause dryness,bleeding;even when cause dryness,bleeding;even when they are used with a humidifier.they are used with a humidifier.
• Deviated septum,polyps,mouth Deviated septum,polyps,mouth breathing may reduce Fio2.breathing may reduce Fio2.

• Best used in the stable patients who need Best used in the stable patients who need low Fio2.low Fio2.
• Home care patient who needs long term Home care patient who needs long term therapy,low to moderate Fio2 while eating.therapy,low to moderate Fio2 while eating.
• Advantages: low cost, disposable,well Advantages: low cost, disposable,well tolerated.tolerated.
• Easy to use in adults,children,infants.Easy to use in adults,children,infants.

ESTIMATED FiO2 WITH ESTIMATED FiO2 WITH NASAL CANNULANASAL CANNULA• 1L/min - .241L/min - .24• 2L/min - .282L/min - .28• 3L/min - .323L/min - .32• 4L/min - .364L/min - .36• 5L/min - .405L/min - .40• Rule of thumb- for patients with normal Rule of thumb- for patients with normal
rate and depth of breathing,each litre per rate and depth of breathing,each litre per min of nasal oxygen increases the Fio2 by min of nasal oxygen increases the Fio2 by 4%.4%.

NASAL CATHETHERNASAL CATHETHER
• Soft plastic tube with several holes at the Soft plastic tube with several holes at the tip.tip.
• Inserted by advancing along the floor of Inserted by advancing along the floor of either nasal passage and visualizing it just either nasal passage and visualizing it just behind and above the uvula.behind and above the uvula.
• Once in position it is taped to the bridge of Once in position it is taped to the bridge of the nose.the nose.
• Can be inserted to a depth equal to the Can be inserted to a depth equal to the distance from the nose to the tragus of distance from the nose to the tragus of either ear.either ear.

• Flow – ¼ to 8L/min.Flow – ¼ to 8L/min.
• Fio2 range – 22% to 45%.Fio2 range – 22% to 45%.
• Variable performance system.Variable performance system.
• Low cost ,good stability,disposable.Low cost ,good stability,disposable.
• Best used in the procedures in which Best used in the procedures in which cannula is difficult to use(bronchoscopy).cannula is difficult to use(bronchoscopy).
• Long term care of infants.Long term care of infants.

DISADVANTAGES OF NASAL DISADVANTAGES OF NASAL CATHETERCATHETER• Difficult to insert.Difficult to insert.
• High flow increases back pressure.High flow increases back pressure.
• Needs regular changing(at least every Needs regular changing(at least every 8hrs).8hrs).
• Polyps,deviated septum can may block Polyps,deviated septum can may block insertion.insertion.
• May provoke gagging,air May provoke gagging,air swallowing,aspiration.swallowing,aspiration.

TRANSTRACHEAL CATHETERTRANSTRACHEAL CATHETER
• First described by Hemlich in 1982.First described by Hemlich in 1982.• Teflon catheter with a guide wire which is Teflon catheter with a guide wire which is
inserted directly into the trachea between inserted directly into the trachea between the 2the 2ndnd and 3 and 3rdrd tracheal rings. tracheal rings.
• Custom sized chain necklace secures the Custom sized chain necklace secures the catheter in position.catheter in position.
• No humidifier is needed as the flow is low.No humidifier is needed as the flow is low.

• Flow – ¼ to 4L/min.Flow – ¼ to 4L/min.• Fio2 range is 22% to 35%.Fio2 range is 22% to 35%.• Variable performance system.Variable performance system.• Lower oxygen use and cost.Lower oxygen use and cost.• Eliminates nasal and skin Eliminates nasal and skin
irritation;improved compliance.irritation;improved compliance.• Increased exercise Increased exercise
tolerance,enhanced image.tolerance,enhanced image.

DISADVANTAGESDISADVANTAGES
• High costHigh cost
• Surgical complicationsSurgical complications
• Infection,mucus plugging,lost tract.Infection,mucus plugging,lost tract.
• Best used in home care and ambulatory Best used in home care and ambulatory patients needing increased mobility.patients needing increased mobility.
• Those who dont accept nasal oxygen.Those who dont accept nasal oxygen.

Variables affecting the Fio2 Variables affecting the Fio2 of low flow oxygen systems.of low flow oxygen systems.• Increased Fio2 :Increased Fio2 :• Higher O2 input,mouth closed Higher O2 input,mouth closed
breathing(cannula only).breathing(cannula only).• Low inspiratory flow and low tidal Low inspiratory flow and low tidal
volume,high I:E ratio.volume,high I:E ratio.• Slow rate of breathing and small Slow rate of breathing and small
minute ventilation.minute ventilation.• Long inspiratory time.Long inspiratory time.

DECREASED FiO2DECREASED FiO2
• Lower O2 inputLower O2 input• Mouth open breathing.Mouth open breathing.• High inspiratory flow and high tidal High inspiratory flow and high tidal
volume.volume.• Fast rate of breathing.Fast rate of breathing.• Large minute ventilation,short Large minute ventilation,short
inspiratory time.inspiratory time.• Low I:E ratio.Low I:E ratio.

RESERVOIR SYSTEMSRESERVOIR SYSTEMS
• They incoporate a mechanism for They incoporate a mechanism for gathering and storing oxygen between gathering and storing oxygen between patients breaths.patients breaths.
• They extend the anatomic reservoir thus They extend the anatomic reservoir thus further increasing the Fio2.further increasing the Fio2.
• Air dilution is reduced and hence higher Air dilution is reduced and hence higher Fio2 is provided.Fio2 is provided.

RESERVOIR CANNULASRESERVOIR CANNULAS
• Designed to conserve oxygen.Designed to conserve oxygen.• FLOW : ¼ TO 4L/min.FLOW : ¼ TO 4L/min.• FiO2 range- 22% to 35%.FiO2 range- 22% to 35%.• Variable performance system.Variable performance system.• Lower oxygen use and cost,increased Lower oxygen use and cost,increased
mobility.mobility.• Less discomfort because of lower Less discomfort because of lower
flow.flow.

• RESERVOIR CANNULAS : Nasal reservoir RESERVOIR CANNULAS : Nasal reservoir and pendant reservoir.and pendant reservoir.
• Nasal reservoir cannula stores approx 20 Nasal reservoir cannula stores approx 20 ml of oxygen in a small membrane ml of oxygen in a small membrane reservoir during exhalation.reservoir during exhalation.
• The patient draws on this stored oxygen The patient draws on this stored oxygen during early inspiration.during early inspiration.
• The amount of O2 available increases with The amount of O2 available increases with each breath.each breath.

PENDANT RESERVOIRPENDANT RESERVOIR
• The reservoir is hidden under the The reservoir is hidden under the patients clothing on the anterior patients clothing on the anterior chest wall.chest wall.
• The device is less visible but the The device is less visible but the extra weight of the pendant can extra weight of the pendant can cause ear and facial discomfort.cause ear and facial discomfort.

DISADVANTAGES OF DISADVANTAGES OF RESERVOIR CANNULASRESERVOIR CANNULAS• They are unattractive,cumbersome.They are unattractive,cumbersome.• Poor compliance.Poor compliance.• Must be regularly replaced(every 3 Must be regularly replaced(every 3
weeks).weeks).• Breathing pattern affects performance.Breathing pattern affects performance.• Best used in home care or ambulatory Best used in home care or ambulatory
patients who need increased mobility.patients who need increased mobility.

RESERVOIR MASKSRESERVOIR MASKS
• Most commonly used reservoir Most commonly used reservoir systems.systems.
• 3 main types : 3 main types :
• Simple mask.Simple mask.
• Partial rebreathing mask.Partial rebreathing mask.
• Non rebreathing mask.Non rebreathing mask.

SIMPLE FACE MASKSIMPLE FACE MASK
• Basic reservoir system.Basic reservoir system.• Flow : 5 – 12L/minFlow : 5 – 12L/min• Fio2 – 35% - 50%Fio2 – 35% - 50%• Variable performance system.Variable performance system.• Flow rate must exceed 5L/min to Flow rate must exceed 5L/min to
replace exhaled gas with fresh replace exhaled gas with fresh oxygen otherwise rebreathing of CO2 oxygen otherwise rebreathing of CO2 will occur.will occur.

SIMPLE FACE MASKSIMPLE FACE MASK
• Disposable plastic unit designed to cover Disposable plastic unit designed to cover both the mouth and the nose.both the mouth and the nose.
• Gathers and stores O2 between the Gathers and stores O2 between the patients breaths.patients breaths.
• The patient exhales directly through open The patient exhales directly through open holes or ports in the mask body.holes or ports in the mask body.
• If O2 input flow cease,the patient can draw If O2 input flow cease,the patient can draw in air through these holes and around the in air through these holes and around the mask edge.mask edge.

Advantages and Advantages and DisadvantagesDisadvantages• Advantages : quick,easy to apply, Advantages : quick,easy to apply,
disposable, inexpensive.disposable, inexpensive.• Disadvantages : uncomfortable,must be Disadvantages : uncomfortable,must be
removed for eating.removed for eating.• Prevents radiant heat loss.Prevents radiant heat loss.• Blocks vomitus in unconscious patient.Blocks vomitus in unconscious patient.• Best used in emergencies,short term Best used in emergencies,short term
therapy requiring moderate FiO2.therapy requiring moderate FiO2.

ESTIMATED FiO2 WITH FACE ESTIMATED FiO2 WITH FACE MASKMASK
• 5 – 6L/min - .405 – 6L/min - .40
• 6 – 7 L/min- .506 – 7 L/min- .50
• 7 – 8 L/min - .607 – 8 L/min - .60

PARTIAL REBREATHING MASK PARTIAL REBREATHING MASK AND NON REBREATHING MASKAND NON REBREATHING MASK
• Both have got the similar design.Both have got the similar design.
• Each has a 1 L flexible reservoir bag Each has a 1 L flexible reservoir bag attached to the oxygen inlet.attached to the oxygen inlet.
• The bag increases the reservoir volume The bag increases the reservoir volume and hence provide higher FiO2 than face and hence provide higher FiO2 than face mask.mask.
• The key difference between these designs The key difference between these designs is the use of valves.is the use of valves.

• Partial rebreather has no valves.Partial rebreather has no valves.• O2 flows into the mask during inspiration O2 flows into the mask during inspiration
and passes directly to the patient.and passes directly to the patient.• During exhalation, source O2 enters the During exhalation, source O2 enters the
bag.bag.• Since there is no valves, some of the Since there is no valves, some of the
patients exhaled gas also enters the patients exhaled gas also enters the bag( approx first one third).bag( approx first one third).
• It contains mainly O2 and little CO2.It contains mainly O2 and little CO2.

• The last two thirds of exhalation escapes The last two thirds of exhalation escapes out the exhalation ports of the mask.out the exhalation ports of the mask.
• CO2 rebreathing is negligible as long the CO2 rebreathing is negligible as long the O2 input flow keeps the bag from O2 input flow keeps the bag from collapsing.collapsing.
• Flow – 6 -10L/minFlow – 6 -10L/min• Fio2 range – 35% - 60%.Fio2 range – 35% - 60%.• Variable performance system.Variable performance system.

NONREBREATHING MASKNONREBREATHING MASK
• It prevents rebreathing with one way It prevents rebreathing with one way valves.valves.
• An inspiratory valve sits atop the An inspiratory valve sits atop the bag,expiratory valves cover the exhalation bag,expiratory valves cover the exhalation ports on the mask body.ports on the mask body.
• During inspiration,the valve atop the bag During inspiration,the valve atop the bag opens providing O2.opens providing O2.
• The expiratory valves close due to the The expiratory valves close due to the negative pressure preventing air dilution.negative pressure preventing air dilution.

• During exhalation,slight positive pressure During exhalation,slight positive pressure closes the inspiratory valve which closes the inspiratory valve which prevents exhaled gas from entering the prevents exhaled gas from entering the bag.bag.
• Concurrently the one way expiratory Concurrently the one way expiratory valves open and divert exhaled gas out.valves open and divert exhaled gas out.
• Flow – 6 to 10L/minFlow – 6 to 10L/min• FiO2 Range – 55% to 70%FiO2 Range – 55% to 70%• Variable performance system.Variable performance system.

• Large air leaks the major problem.Large air leaks the major problem.• Air leakage occurs both around the Air leakage occurs both around the
mask body and through the mask body and through the exhalation port.exhalation port.
• The open exhalation port is common The open exhalation port is common safety feature.safety feature.
• This also causes air dilution.This also causes air dilution.

NON REBREATHING NON REBREATHING RESERVOIR CIRCUITRESERVOIR CIRCUIT• Basically a CLOSED SYSTEM.Basically a CLOSED SYSTEM.• Blending system premixes air and O2;full Blending system premixes air and O2;full
range of FiO2 is provided.range of FiO2 is provided.• The gas mixture is warmed and humidified The gas mixture is warmed and humidified
and flows into an inspiratory volume and flows into an inspiratory volume reservoir.reservoir.
• The patient breathes through the closed The patient breathes through the closed airway appliance such as a mask with one airway appliance such as a mask with one way valve.way valve.

• A valved T tube can also be used in the A valved T tube can also be used in the care of a patient with an endotracheal or care of a patient with an endotracheal or tracheostomy tube.tracheostomy tube.
• FLOW – 3 times Ve.( prevent bag collapse FLOW – 3 times Ve.( prevent bag collapse on inspiration).on inspiration).
• FiO2 range – 21% to 100%.FiO2 range – 21% to 100%.• Fixed performance system.Fixed performance system.• Main advantage – provides full range of Main advantage – provides full range of
FiO2.FiO2.

• Disadvantage – potential suffocation Disadvantage – potential suffocation hazard,blender failure is common.hazard,blender failure is common.
• Best used in patients who need Best used in patients who need precise FiO2 at any level(21% to precise FiO2 at any level(21% to 100%).100%).

FIXED PERFORMANCE SYSTEMSFIXED PERFORMANCE SYSTEMS
(Fio(Fio22 is independent of patient factors) is independent of patient factors)
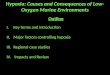
HIGH-FLOW VENTURI MASKHIGH-FLOW VENTURI MASKThese masks give an accurate FioThese masks give an accurate Fio2 2 which which
depends on their construction & the Odepends on their construction & the O22 flow flow rate (which is written on the mask with the rate (which is written on the mask with the OO22 percentage percentage

They are colour-coded & acc. ‘Bernoulli’ principleThey are colour-coded & acc. ‘Bernoulli’ principle
However, these masks may not deliver the However, these masks may not deliver the intended Fiointended Fio22 if severe dyspnoea is present if severe dyspnoea is present
FiOFiO2 2 is increaqsed by increasing the size of jet orifice or decreasing the size of side ports , both of which decrease the amount of room air entrained.

AdvantagesAdvantages- delivery of predictable FiO- delivery of predictable FiO2
-useful in patients in whom delivery of -useful in patients in whom delivery of excessive oxygen could depress the excessive oxygen could depress the respiratory driverespiratory drive
DisadvantagesDisadvantages- limited access for - limited access for
eating ,drinking ,expectoratingeating ,drinking ,expectorating -claustrophobia-claustrophobia -irritation to eyes because of high flow -irritation to eyes because of high flow
ratesrates

Approximate OApproximate O22 concentration related to concentration related to flow rates of semi venturi devicesflow rates of semi venturi devices
FiOFiO22 Flow rateFlow rate
(l/min)(l/min)Air:oxygenAir:oxygen
entrainmeentrainmentnt
Total gas Total gas
Flow Flow (l/min)(l/min)
0.240.24 44 25:125:1 104104
0.280.28 66 10:110:1 6666
0.350.35 88 5:15:1 4848
0.400.40 88 3:13:1 3232
0.600.60 1212 1:11:1 Twice oTwice o22
flowflow

TRACHEOSTOMY MASKSTRACHEOSTOMY MASKS These are small plastic masks placed over the These are small plastic masks placed over the
tracheostomy tube or stomatracheostomy tube or stoma The pt will inspire less OThe pt will inspire less O22 than delivered, as than delivered, as
dilution by room air occursdilution by room air occurs Otherwise, they perform similarly to simple Otherwise, they perform similarly to simple
facemaskfacemask

FACE TENTFACE TENT
This is a large, semi-rigid plastic half mask which This is a large, semi-rigid plastic half mask which wraps around the chin & cheekswraps around the chin & cheeks
The OThe O22 mixture is delivered from the bottom of mixture is delivered from the bottom of the mask & the gases are exhaled through the the mask & the gases are exhaled through the open upper part.open upper part.
It is used to provide added humidification from a It is used to provide added humidification from a
heated humidifierheated humidifier Otherwise it has no advantages over the simple Otherwise it has no advantages over the simple
facemaskfacemask

OO22 HEADBOX HEADBOX
OO22 is delivered into a box encasing is delivered into a box encasing the child’s neckthe child’s neck
The FioThe Fio22 depends on the fresh gas depends on the fresh gas flow, size of box, flow, size of box,

It is a useful method in infants & small children, It is a useful method in infants & small children,
but high flow rates should be supplied & but high flow rates should be supplied & monitoring of Omonitoring of O22 concentration near the face is concentration near the face is essentialessential
INCUBATORINCUBATOR It provide OIt provide O2 2 as well as a neutral thermal as well as a neutral thermal
environmentenvironment Pt access & recovery of OPt access & recovery of O2 2 concentration after concentration after
opening incubator are problemsopening incubator are problems

HYPERBARIC OHYPERBARIC O2 2 THERAPYTHERAPY
HBO therapy is indicated in compromised OHBO therapy is indicated in compromised O2 2 carrying carrying capacity of Hb (e.g in CO poisoning) or if extra tissue capacity of Hb (e.g in CO poisoning) or if extra tissue OO2 2 is required (e.g severe burns & tissue infection)is required (e.g severe burns & tissue infection)
This uses the ability of plasma & tissue fluid to accept This uses the ability of plasma & tissue fluid to accept an increased amount of Oan increased amount of O2 2 that is dissolved under that is dissolved under pressurepressure
HBO therapy delivers 100% OHBO therapy delivers 100% O2 2 at a pressure above at a pressure above atm, in a pressurized multi or one-person chamberatm, in a pressurized multi or one-person chamber
Complications of HBO therapy include barotrauma to Complications of HBO therapy include barotrauma to ears, sinuses & lung, Oears, sinuses & lung, O2 2 toxicity,grand mal fits & toxicity,grand mal fits & reversible visual changes.reversible visual changes.

PRECAUTIONS AND PRECAUTIONS AND COMPLICATIONSCOMPLICATIONS1.1. PaO2 > 60mmHg in patients with PaO2 > 60mmHg in patients with
chronic hypercapnia may cause chronic hypercapnia may cause depression of ventilationdepression of ventilation
2.2. FiO2 >0.5 may cause atelectasis, FiO2 >0.5 may cause atelectasis, oxygen toxicity and ciliary depressionoxygen toxicity and ciliary depression
3.3. In premature infants PaO2 >80mmHg In premature infants PaO2 >80mmHg may cause Retinopathy of prematuritymay cause Retinopathy of prematurity
4.4. Fire hazard is increased in presence of Fire hazard is increased in presence of high FiO2high FiO2

5. During laser bronchoscopy, minimal 5. During laser bronchoscopy, minimal FiO2 should be used to avoid intra FiO2 should be used to avoid intra tracheal ignitiontracheal ignition
6. Bacterial contamination can occur if 6. Bacterial contamination can occur if nebulizers or humidifiers are used nebulizers or humidifiers are used

MONITORINGMONITORING• CLINICAL ASSESSMENTCLINICAL ASSESSMENT
• PHYSIOLOGIC PARAMETERS – ABG PHYSIOLOGIC PARAMETERS – ABG PaO2, SaO2 AT :-PaO2, SaO2 AT :-
1.1. Initiation of therapyInitiation of therapy
2.2. Within 12 hours if initial FiO2 >0.6Within 12 hours if initial FiO2 >0.6
3.3. Within 72 hours in acute MIWithin 72 hours in acute MI
4.4. Within 2 hours in COPD patientsWithin 2 hours in COPD patients
5.5. Within 1 hour for neonatesWithin 1 hour for neonates

EQUIPMENT MONITORINGEQUIPMENT MONITORING• All oxygen delivery systems should be All oxygen delivery systems should be
checked at least once a daychecked at least once a day
• More frequent checks for systems More frequent checks for systems which are :which are :
1.1. Susceptible to variation in FiO2 Susceptible to variation in FiO2 e.g.hood, high flow blending systemse.g.hood, high flow blending systems
2.2. Applied to patients with artificial Applied to patients with artificial airwaysairways
3.3. Delivering a heated gas mixtureDelivering a heated gas mixture
4.4. Applied to clinically unstable patients Applied to clinically unstable patients requiring FiO2 >0.5requiring FiO2 >0.5

HAZARDS OF OXYGEN THERAPYHAZARDS OF OXYGEN THERAPY OXYGEN TOXICITYOXYGEN TOXICITY• PRIMARILY AFFECTS LUNGS AND CNSPRIMARILY AFFECTS LUNGS AND CNS
• 2 MAJOR DETRMINANTS :2 MAJOR DETRMINANTS :
1.1. PaO2PaO2
2.2. Exposure timeExposure time
• CNS effects – tremors, twitching & CNS effects – tremors, twitching & convulsions occur with hyperbaric convulsions occur with hyperbaric oxygen pressuresoxygen pressures
• Pulmonary effects can occur at Pulmonary effects can occur at clinical PaO2clinical PaO2

PHYSIOLOGIC RESPONSE OF PHYSIOLOGIC RESPONSE OF EXPOSURE TO 100EXPOSURE TO 100% O% O22
EXPOSUREEXPOSURE• 0 - 12 0 - 12 hrshrs
• 12 - 14 hrs12 - 14 hrs
• 24 - 30 24 - 30 hrshrs
• 30-72hrs30-72hrs
PHYSIOLOGIC RESPONSEPHYSIOLOGIC RESPONSE• Normal pulmonary functionNormal pulmonary function• Substernal pain Substernal pain
TracheobronchitisTracheobronchitis
Decreasing vital capacityDecreasing vital capacity
• Decreasing lung complianceDecreasing lung compliance• Increasing P(A-a)O2 gradientIncreasing P(A-a)O2 gradient• Decreasing exercise PaO2Decreasing exercise PaO2
• Decreasing diffusing capacityDecreasing diffusing capacity

•Patients exposed to high Po2 for Patients exposed to high Po2 for prolonged period has signs prolonged period has signs similar to broncho-pneumoniasimilar to broncho-pneumonia
•CXR- patchy infiltrates prominent CXR- patchy infiltrates prominent in lower lung fieldsin lower lung fields
•Underlying the gross clinical Underlying the gross clinical signs is a major alveolar injurysigns is a major alveolar injury

PATHOGENESIS OF OPATHOGENESIS OF O22 TOXICITYTOXICITY
Exposure to ↑ Po2 damages capillary Exposure to ↑ Po2 damages capillary endotheliumendothelium
Interstitial oedema & alveolar thickening Interstitial oedema & alveolar thickening followsfollows
Type-1 alveolar cells are destroyed & Type-1 alveolar cells are destroyed & Type-2 cells proliferateType-2 cells proliferate

Exudative phase followsExudative phase follows
Low V/Q ratio,Physiologic shunting & Low V/Q ratio,Physiologic shunting & hypoxemiahypoxemia
Hyaline membrane forms in alveolar regionsHyaline membrane forms in alveolar regions
Pulmonary fibrosis & hypertension developsPulmonary fibrosis & hypertension develops

•AS LUNG INJURY WORSENS AS LUNG INJURY WORSENS BLOOD OXYGENATION BLOOD OXYGENATION DETERIORATESDETERIORATES
• If this progressive hypoxemia is If this progressive hypoxemia is managed with additional oxygen, managed with additional oxygen, the toxic effect worsensthe toxic effect worsens
•A vicious cycle sets inA vicious cycle sets in

OXYGEN TOXICITYOXYGEN TOXICITY
INCREASEDINCREASED FiOFiO22
LOW PaOLOW PaO22
INCREASED
SHUNTING

•Toxicity is caused by overproduction Toxicity is caused by overproduction of oxygen free radicals which of oxygen free radicals which damages cellsdamages cells
•Normally superoxide dismutase Normally superoxide dismutase enzyme and Anti-oxidants can enzyme and Anti-oxidants can defend against free radical damagedefend against free radical damage
• BUT in presence of high PaO2 ANTI BUT in presence of high PaO2 ANTI OXIDANT SYSTEMS ARE INEFFECTIVEOXIDANT SYSTEMS ARE INEFFECTIVE
•Cell damage occurs and provoke Cell damage occurs and provoke immune response → worsens injuryimmune response → worsens injury

•Exactly how much oxygen is safe is Exactly how much oxygen is safe is debatabledebatable
•TheThe GOAL GOAL should be to use lowest should be to use lowest possible FiOpossible FiO22 with adequate with adequate oxygenationoxygenation
•Limit patient exposure to 100% OLimit patient exposure to 100% O22 to to less than 24 hours.less than 24 hours.
•High FiOHigh FiO22 is acceptable if is acceptable if concentration can be decreased to concentration can be decreased to 70% within 2 days and 50% or less in 70% within 2 days and 50% or less in 5 days5 days

RETINOPATHY OF PREMATURITYRETINOPATHY OF PREMATURITY
•RETROLENTAL FIBROPLASIARETROLENTAL FIBROPLASIA
•Affects LBW &infants <1 monthAffects LBW &infants <1 month
•High PaO2 causes retinal High PaO2 causes retinal vasoconstriction which leads to vasoconstriction which leads to necrosis of blood vesselsnecrosis of blood vessels
•Keeping an infants arterial PaO2 Keeping an infants arterial PaO2 <80mmHg is best way of <80mmHg is best way of preventionprevention

ABSORPTION ATELECTASISABSORPTION ATELECTASIS
• FiO2 >0.5 presents a significant risk.FiO2 >0.5 presents a significant risk.
High FiO2 rapidly depletes body High FiO2 rapidly depletes body nitrogennitrogen
Total pressure of venous gases declineTotal pressure of venous gases decline
Gases that exists in body cavities Gases that exists in body cavities rapidly diffuse inrapidly diffuse in bloodblood

Alveolar O2 rapidly diffuses in bloodAlveolar O2 rapidly diffuses in blood
If no source of gas repletion total If no source of gas repletion total gas pressure in alveolus rapidly gas pressure in alveolus rapidly declines until alveoli collapse e.g. declines until alveoli collapse e.g. obstructionobstruction
Because collapsed alveoli are Because collapsed alveoli are perfused but not ventilated →V/Q perfused but not ventilated →V/Q mismatchmismatch

•The risk of absorption atelectasis The risk of absorption atelectasis is greatest in patients breathing is greatest in patients breathing at low tidal volumes e.g. sedation, at low tidal volumes e.g. sedation, surgical pain, CNS dysfunction.surgical pain, CNS dysfunction.
• In these cases poorly ventilated In these cases poorly ventilated alveoli become unstable when alveoli become unstable when they loose oxygen faster than it they loose oxygen faster than it can be replaced.can be replaced.
•Result is gradual shrinking of Result is gradual shrinking of alveoli to complete collapse.alveoli to complete collapse.

THANK YOUTHANK YOU