Embed Size (px)
Citation preview


Imaging of IPF
Gamal Rabie Agmy, MD, FCCP Professor of chest Diseases, Assiut university

• Interstitial compartment is the portion of the lung sandwiched between the epithelial and endothelial basement membrane
• Expansion of the interstitial compartment by inflammation with or without fibrosis – Necrosis
– Hyperplasia
– Collapse of basement membrane
– Inflammatory cells
What is the Pulmonary
Interstitium?


The interstitium of the lung is not normally visible radiographic-
ally; it becomes visible only when disease (e.g., edema,
fibrosis, tumor) increases its volume and attenuation.
The interstitial space is defined as continuum of loose
connective tissue throughout the lung composed of three
subdivisions:
(i) the bronchovascular (axial), surrounding the bronchi,
arteries, and veins from the lung root to the level of the
respiratory bronchiole
(ii) the parenchymal (acinar), situated between the alveolar
and capillary basement membranes
(iii) the subpleural, situated beneath the pleura, as well as in
the interlobular septae.
The Lung Interstitium

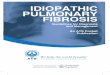
Secondary pulmonary lobular
anatomy
The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli.
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)

Ideal ILD doctor
Radiologist
Pathologist
Pulmonologist

Introduction
◙ Idiopathic pulmonary fibrosis (IPF) has
been defined by international guidelines as
a specific form of chronic, progressive,
fibrosing interstitial pneumonia of unknown
cause, occurring primarily in older adults,
limited to the lungs and associated with the
histopathological and/or radiological
pattern of usual interstitial pneumonia (UIP)

Diagnostic criteria
According to international guidelines , the
diagnosis of IPF requires the following:
1) exclusion of other known causes of interstitial lung
disease, e.g. domestic and occupational environmental
exposures, connective tissue disease and drug
toxicity;
2) the presence of a definite UIP pattern on HRCT in
patients not subjected to surgical lung biopsy; and
3) specific combinations of HRCT and surgical lung biopsy
patterns in patients subjected to surgical lung biopsy.

Radiography
Early in the disease, the most common radiographic changes are an
interstitial shadowing of small (1- to 2-mm), irregular opacities, which are
seen in about three fourths of patients. Less common are small, round
opacities, which are seen in one fifth of patients. This finding is generally
known as reticulonodular opacities. Septal lines are occasionally
observed. The distribution is predominantly basal.

Peripheral accentuation is also a
common feature, but it is more easily
appreciated on CT scans than on plain
chest radiographs.
The pattern is usually symmetrical.
Another common pattern is hazy, ground-
glass opacification, which is either
diffuse or patchy. Volume loss and a
raised diaphragm are seen in up to 60%
of patients. This may be accompanied by
basal discoid atelectasis.

Pleural disease is not typical of IPF. Its
presence should raise the possibility of
other conditions, such as asbestosis,
rheumatoid pulmonary disease, or
systemic lupus.
Pneumothorax, pneumomediastinum, or
both have been reported in a few patients;
these conditions have been associated
with bullae in the lung parenchyma.

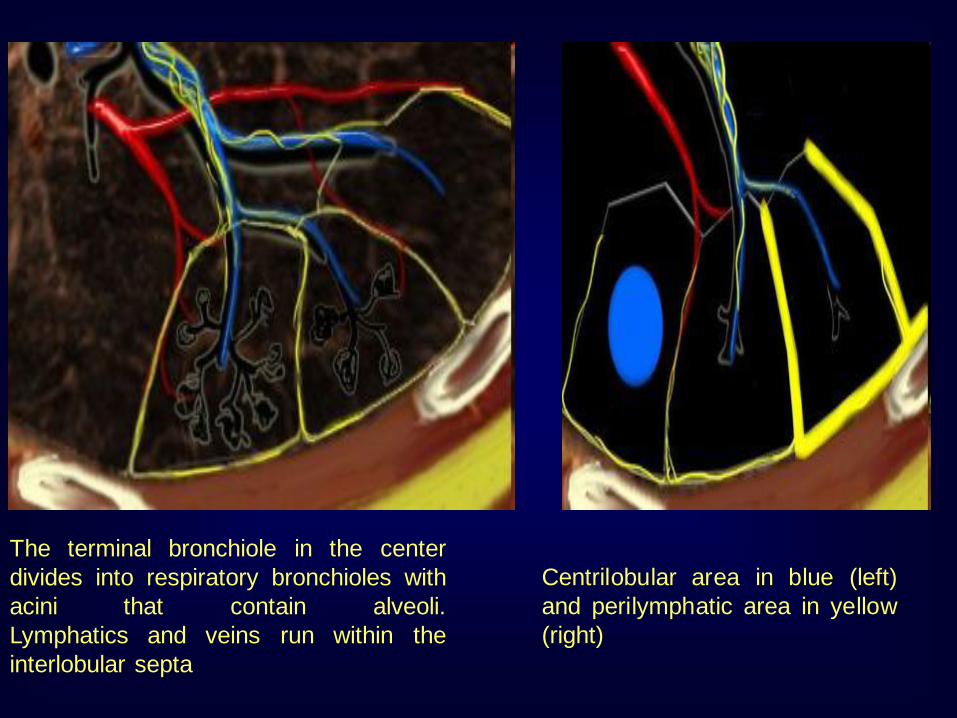
With progression of alveolitis to fibrosis, the
initial fine lines become coarse, and small (2-
mm) cysts appear. These cysts coalesce and
increase to 5-7 mm in diameter; they appear as
ring opacities within the honeycomb lung.
As fibrosis worsens, the honeycombing
becomes coarser with larger honeycomb
cysts, and further volume loss occurs. In
advanced stages, there is radiographic
evidence of pulmonary arterial hypertension.

False positives/negatives
For symptomatic patients in whom the
diffusion capacity is abnormal, results of
chest radiography may be normal.
For other patients, the radiographic
appearances are abnormal before clinical
symptoms appear. Results of HRCT scanning
are abnormal for most patients with IPF.

Computed Tomography

Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
•Upper or mid lung
predominance
•peribronchovascular
predominance
•extensive ground glass abnormality (extent >
reticular abnormality)
•profuse micronodules
(bilateral, predominantly
upper lobes) •discrete cysts (multiple
bilateral, away from areas of
honeycombing)
•diffuse mosaic
attenuation/air trapping (bilateral in three or more
lobes)
•subpleural basal
predominance
•reticular abnormality
•Absence of features listed as inconsistent
with UIP pattern
•subpleural basal
predominance
•reticular abnormality
•honeycombing with
or without traction
bronchiectasis
•Absence of features
listed as inconsistent
with UIP pattern

The Fleischner Society glossary provides both
radiological and pathological definitions for
honeycombing
Radiologically, honeycombing is characterised by
‘‘clustered cystic air spaces, cysts of comparable
diameters, and cyst diameters typically ,10 mm
surrounded by well-defined walls’’
The pathology is defined as ‘‘destroyed and fibrotic
lung tissue containing numerous cystic airspaces
with thick fibrous walls, representing the late stage
of various lung diseases, with complete loss of
acinar architecture’’

Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP


Mosiac pattern

Bronchiolitis
obliterans


Chronic EAA

Young woman Dry mouth Smoker
LAM LIP Histiocytosis



Using HRCT to prognosticate IPF and
monitor disease progression
1-Traction bronchiectasis
2-Honeycombing
3-Decreases DLCo
the extent of honeycombing at baseline and its progression on
follow-up HRCT were both found to be important predictors of
mortality in patients with fibrosing interstitial pneumonia.
Subjects who demonstrated progression of fibrosis extent on
HRCT over a period of 6 months and a decline in forced vital
capacity were identified as a particular sub-group of IPF
patients with the poorest outcomes. In fact this was shown to
be a superior predictor of outcome compared to baseline
HRCT fibrosis scores

False positives/negatives
One third of all cases of IPF are missed on
HRCT; a confident diagnosis of IPF is made
in about two thirds of cases

Nuclear Imaging In cases of IPF, perfusion lung scintigraphy shows
nonspecific, subsegmental mismatched perfusion defects.
These are not correlated with clinical severity.
Gallium-67 imaging has not proven to be of value in cases
of established IPF.
Technetium-99m diethylenetriamine penta-acetic acid
(DTPA) is cleared more rapidly when capillary permeability
is increased than when it is not, and the findings may
provide an index of lung inflammation.
Fluorodeoxyglucose (FDG) positron-emission tomography
(PET) may show FDG accumulation in the lung bases; such
findings correlate with the honeycomb fibrosis seen on
high-resolution HRCT