Embed Size (px)
Citation preview

Prof. M.C.Bansal. MBBS;MS. FICOG. MICOG.
Founder Principal & Controller, Jhalawar Medical college , Jalawar.
Ex.Principal&Controller; Mahatma Gandhi Medical
College,sitapura , Jaipur.
IMAGING IN OBSTETRICS & GYNAECOLOGY
DR. RIDHI KATHURIAPG 2ND year
DEPTT OF OBS & GYNNIMS MEDICAL COLLEGE & HOSPITAL
JAIPUR

WHAT IS MEDICAL IMAGING?
MEDICAL IMAGING is the technique and process used to create images of
the human body (or parts and function thereof) for clinical purposes (medical
procedures seeking to reveal, diagnose, or examine disease) or medical science
(including the study of normal anatomy and physiology).

1. Ultrasonography.2. X-Ray.3. Hysterography.4. Hysteroscopy.5. CT Scan6. MRI.7. PET.
MODALITIES

Uses High-frequency broadband sound waves.
>20,000 Hz, i.e. 2 KHz.
Reflected by tissues upto varying degrees depending on the tissue content, type, consistency.
Receiving echoes.
Converting the echoes into electric signals.
Interpreting and displaying those signals
Can be snapshot or in real time.
ULTRASONOGRAPHY
ADVANTAGES
Can be directed in a beam
Obeys the laws of reflection and refraction
Reflected by objects of quite small size
Can be converted to analogue or digital signals for image production
No radiation exposure
Non Invasive
Fast
Relatively inexpensive.

DISADVANTAGES
Ultrasound waves;
o Travels poorly through gas
o The amount reflected depends on the degree of acoustic mismatch
o The piezoelectric crystals are quite delicate

The ultrasound beam & the receipt of echoes is achieved by PIEZOELECTRIC CRYSTALS
Mounted in an array on a probe. The probe can be fixed or oscillating. The wave of sound can be focused to a point of interest. The image is displayed on an oscilloscope or TV screen.
The image will be formed by-1) Direction of echo.2) Strength of echo.
3) Time taken for the echo to return.
These 3 characteristics determine which pixels on the screen will light up & with
what intensity.

DIA
GN
OST
IC
ULT
RASO
UN
Da. Typically involves frequencies of 2 – 15
mHz
b. Lower frequencies will give greater penetration
c. And thereby one can see further
d. Higher frequencies allow to see more detail
e. But the penetration is less
f. And very high frequencies have the potential for adverse biological effects

PROBES
Hand held Probes.
Contain the Piezoelectrical
Crystals.
Of varying types depending on shape,
usage, desired structure/area to be
visualised.

LINEAR PROBE
A Linear Array of Crystals
Produces parallel sound waves
And a rectangular image
Good for surface structures

CURVED PROBE
A Curved Array of Crystals
Will fit curved surfaces of the body
The density of scan decreases proportionally to the distance from the transducer

SECTOR PROBE
A Sector Scanning Probe
Produces a fan-like image
Can fit into narrow spaces
Has poor near-field resolution

TRANSVAGINAL
PROBE
A Sector Array of Crystals
Used to scan by placing it within the vaginal opening.
More detailed view of the structures.
Special emphasis for follicular monitering.


Ultrasound is no substitute for a good history & a thorough clinical (general & specific systemic)
examination .
ALWAYS do an abdominal scan before using the vaginal probe.
The trick is to build up a 3-dimensional picture in your mind using real-time imaging

TRANS ABDOMINAL
Full bladder Panaromic view For large masses Abdominal organs Lymphnodes
TRANS VAGINAL
Empty bladder In gynecology
diseases Uterus , ovaries,
follicles Pouch of Douglas
TRANS PERINEAL
Pelvic floor muscles
TRANS RECTAL Pubo-Rectalis Muscle Anal Sphincter
TYPES OF TECHNIQUES
& PRE
REQUISITES

NORMAL APPEARANCES
TRANSVERSE SECTION OF THE STRUCTURES, JUST ABOVE THE PUBIC SYMPHYSIS.(OVARIES SEEN CLEARLY AS HERE, MAY NOT BE POSSIBLE IN ALL CASES)


TRANS VAGINAL SCANNING
ANTEVERTED UTERUS:- Fundus faces the same
direction as bladder
RETROVERTED UTERUS:- Fundus faces the opposite direction as
bladder

ULTRASOUND IN GYNAECOLOGY

THE UTERUS
Normal Appearance

NORMAL MEASUREMENTS
Size - 7.5 x 5.0 x 2.5cmLength - Fundus to Cervix(7.5-8.0cm)Depth - Antero-posterior(4.5-5.0cm)Width - Coronal view (2.5-3.0cm)Myometrium –
HomogenousHypoechogenic
Endometrium-Changes during menstrual cycle1-4 mm after menses8-10 mm at ovulation(tri laminar)
When evaluating a suspected uterine mass, the practitioner should identify the appropriate anatomical structures.
The initial step is to identify the bladder anteriorly and the rectosigmoid posteriorly.
The position of the uterus depends on the distension of the bladder and rectosigmoid.
The normal uterus appears sonographically as a uniform structure.

CONGENITAL ANOMALIESBicornuate uterusSepatate uterusDidelphous uterus
MYOMASIrregular uterine contourHypo/iso/hyper echoic massesSize, number, location
ADENOMYOSISEnlarged uterusAsymmetric thickening of myometriumHeterogeneous echotexture
INDICATIONS

EN
DO
METR
IAL
AB
NO
RM
ALIT
IES
ABNORMAL UTERINE BLEEDINGPolypsSubmucosal fibroid
POSTMENOPAUSAL BLEEDINGEndo thickness- >5mm needs evaluation
ENDOMETRIAL CANCERMyometrial invasion
TAMOXIFEN THERAPYThick endometriumSubendometrial stromal vacuolation
MISSING IUCDBright echogenicPenetration to myometriumTranslocation to peritoneal cavity

ANOMALIES OF THE UTERUS

BICORNUATE UTERUS

DIDELPHUS UTERUS

SEPTATE
UTERUS
F < 2cm – Incomplete/Partial Septum
F > 2cm – Complete Septum

FIBROID UTERUS


With pregnancy a myoma can be seen better as the anechoic
amniotic fluid provides a good window.
Also as seen, cystic ill defined areas are suggesting ‘Red Degeneration Of
Pregnancy’.
Calcific changes may also be seen as ‘RING
CALCIFICATIONS’ seen as bright line encircling the
mass

POOR VASCULARITY OF THE MASS FURTHER CONFIRMS THE DIAGNOSIS
OF A FIBROID.

SUB-MUCOUS FIBROID
The fibroid impinges within the uterine
cavity.
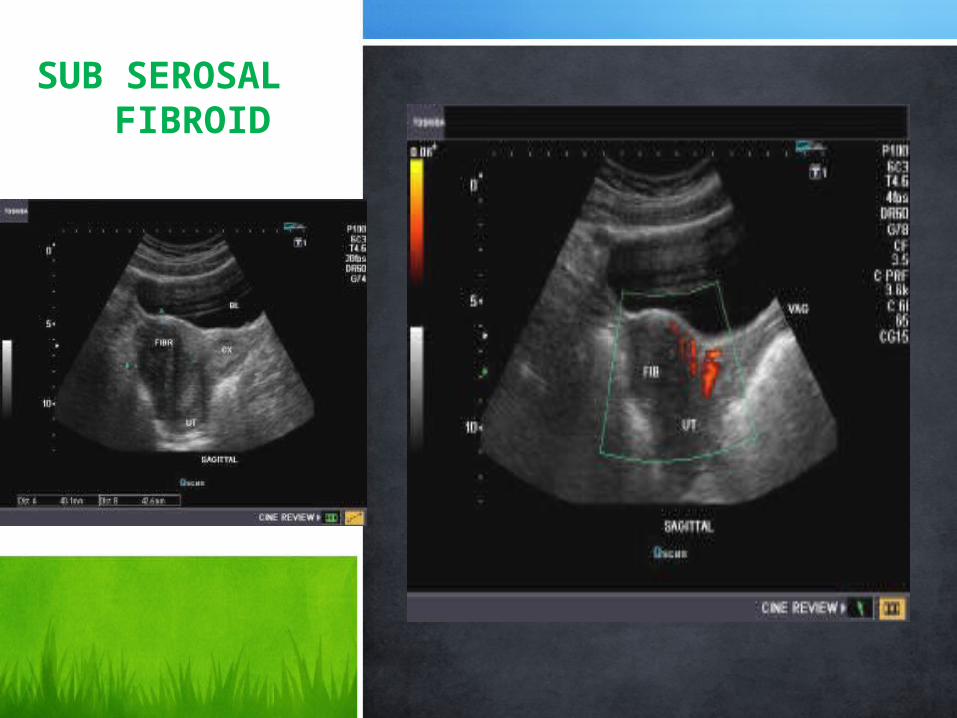
SUB SEROSAL FIBROID

PEDUNCULATED FIBROID
The fibroid stalk may twist on itself.
Get detached from the original area of attachment.
Hence, becoming a WANDERING FIBROID.

LIPOLEIOMYOMA
Brightness is due the fat (fatty degeneration) content of the
mass.

ADENOMYOSIS
A common benign condition that often co-exists with endometriosis and fibroids, often described as endometriosis within the uterus itself .
Endometrial tissue exists within the muscle of the uterus. During menstruation this degenerates and the blood cannot escape the uterine muscle causing pain; some blood may finally escape resulting in abnormal p.v. spotting

• MAY BE NORMAL
• Diffuse uterine enlargement with no alteration in echo-texture or uterine contour, often reported as a “bulky uterus” • Asymmetrically thickened uterus, usually posteriorly
• Poorly defined focal area of hypoechoic or hyperechoic texture within the myometrium, representing a focal adenomyoma (can be multiple) • Cystic hyperplasia of the endometrium • Myometrial cysts

DIFFUSE ADENOMYOSISThe loss of endometrial myometrial junction
when seen on images is characteristic.
Cystic appearance with thickened endometrium


DYSTROPHIC CALCIFICATION OF ENDOMETRIUM
• Deposition of calcium in abnormal tissues, without abnormal blood calcium levels.
• It may occur as a part of ageing process, or may follow an instrumentation or procedure like curettage
• Bright echogenic lesion with posterior shadowing is suggestive of calcification.
• The shadowing is due to complete reflection of the waves when they strike the lesion.

INTRA-UTERINE CONTRACEPTIVE DEVICE (IN SITU)



IUCD PENETRATING THE MYOMETRIAL WALL
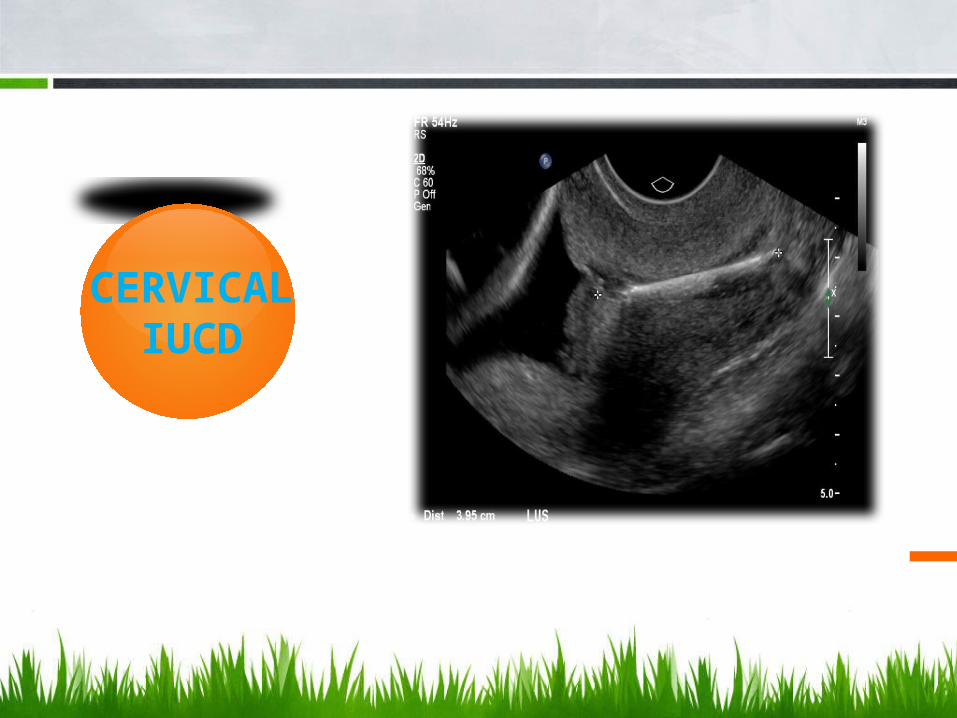
CERVICAL
IUCD

IUCD IN BLADDER

PERFORATED IUCD
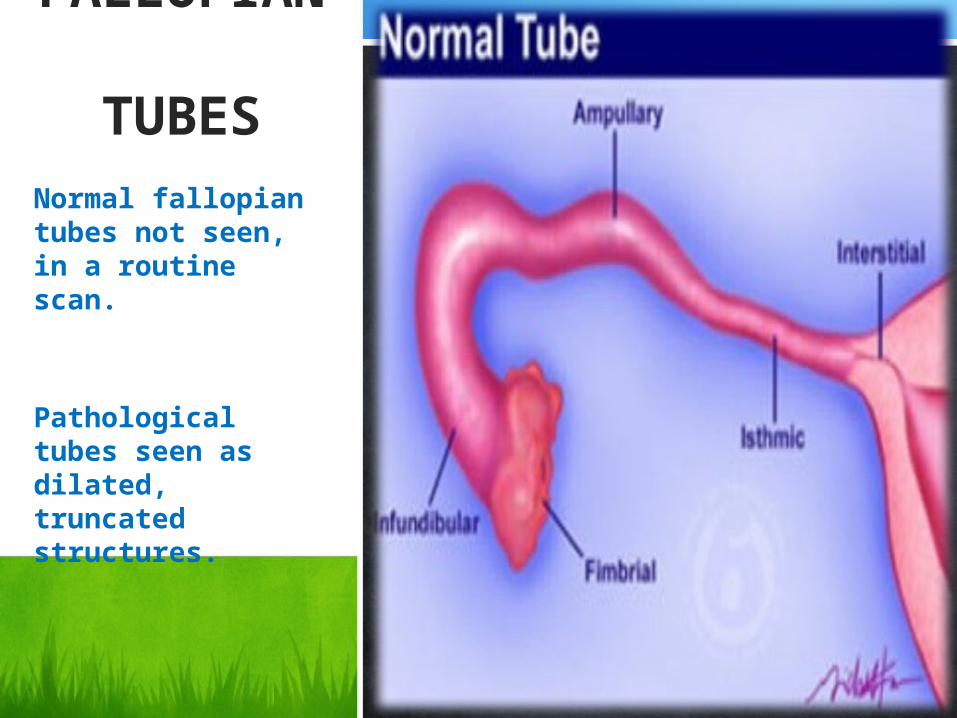
FALLOPIAN
TUBESNormal fallopian tubes not seen, in a routine scan.
Pathological tubes seen as dilated, truncated structures.

• PID• Tuberculosis• Chlamydia/
Gonorrhoea infection
• Traumatic• Cryptomenorrho
ea• Ectopic
Pregnancy• Tubal Carcinoma• Endometriosis
HEMATOSALPINXHYDROSALPINX
Ciliae of the inner lining (endosalpinx) of the fallopian tube beat towards the uterus, tubal fluid is normally discharged via the fimbriated end into the peritoneal cavity from where it is cleared. If the fimbriated end of the tube becomes agglutinated, the resulting obstruction does not allow the tubal fluid to pass; it accumulates and reverts its flow downstream, into the uterus, or production is curtailed by damage to the endosalpinx.
TUBAL PHIMOSIS refers to a situation where the tubal end is partially occluded, in this case fertility is impeded,
and the risk of an ectopic pregnancy is increased.

HYDROSALPINX


HEMATOSALPINX
Thick echogenic homogen
ous material filling the lumen is s/o blood

PYOSALPINXEchogenic debris seen within the lumen is s/o
pus.

OVARIES

NORMAL APPEARANCE

Position
The normal ovary in the resting (menstrual) phase is moderately echogenic, well marginated and located at the lateral edge of the broad ligament.
Because it is mobile, it may be found from the pelvic cul-de-sac to the lower abdomen ( often displaced superiorly by distended urinary bladder, coming to lie anterior and lateral to the iliac vessels).
Despite this variability, it is typically found lateral to the fundus of the uterus.

PREMENARCHAL (Vol. = 0-8 ml)Ovaries are small, and often show a uniform moderately echogenic solid structure. It is typical to note scattered antral follicles (small 3-6 mm cysts) during the years 9-13 preceding menarche.Follicles in younger patients however are not necessarily evidence of endocrine dysfunction. Size of premenarchal ovaries is quite variable, making conclusions based on size alone unreliable.
PUBERTY THROUGH MIDDLE AGE (Vol. = 0-18 ml)Solid background with scattered antral follicles (3-6 mm cysts). This pattern is punctuated by the regular cyclic development of graafian follicles.
POST-MENOPAUSAL (Vol. = 0-8 ml)Solid background, antral follicles may persist 4 -5 years following clinical menopause. Ovarian size is smaller.

PRE- MENARCHAL APPEARANCE
Uterus Cervix & Vagina
Endometrium

Small Multifollicular Ovary Unilocular Ovary


1. Because of the ovary has a variable, usually oval shape, size is best
expressed as an estimated volume.
Volume (ml.) = Length (cm) x Width (cm) x Depth (cm) x 0.52
2. The Ratio of larger to smaller ovary should normally be less then 2:1.
Age (yrs) Volume (ml) Mean (ml)
0-10 0.2 - 4.9 1.7
11-20 1.7 - 18.5 7.8
21-30 2.6 - 23.0 10.2
31-40 2.6 - 20.7 9.5
41-50 2.1 - 20.9 9.0
51-60 1.6 - 14.2 6.2
61-70 1.0 - 15.0 6.0Values ; 95% confidence level

Introduction:
• Although the hormonal background of follicular development is among the more complex endocrine events, the resulting sequence of gross morphologic changes visualized by ultrasound is a simple sequence of enlarging cysts.
• Using measures of size, number, and temporal progression, ultrasound can verify normal sequences, or in many cases, diagnose ovulation failure by recording at what point follicular development is arrested.

Normal Development:• The resting ovary contain a women's full complement of
potential follicles.
• The resting primordial follicles are too small to be seen grossly or on a scan.

Follicular PhaseInitial follicular development occurs during the proliferative (follicular) phase of the menstrual cycle, approximately days 1-14 counting from the first day of menstrual flow, and ends with ovulation.
During the follicular phase, a small subset of the primordial follicles are stimulated to develop, andaccumulate follicular fluid, with enlargement ultimately visible by ultrasound.
Developing Follicles are first seen by ultrasound as a group of 4-8 antral follicles 3-5mm size by
day 6-7 .

By Ultrasound, early antral follicles are 2-4mm in size. Developing follicles range between 5-10 mm.
The dominant (selected) follicle will continue to grow, reaching 10mm on day 8-9 and reaching final mature
size of 18-24 mm, on day 14 prior to ovulation.
Typically subordinate (non-dominant follicles) reach 10 mm and then become atretic.
Follicles 11 mm or larger are usually dominate follicles.

Secretory (Luteal) PhaseOn about day 14, the mature follicle expels the oocyte. In most cases, loss of fluid associated with expulsion of the oocyte results in disappearance or substantial decrease in size of the mature follicle.
This abrupt change in size represents the Ultrasound sign of ovulation.
Free Fluid seen in POD, is also arbitrarily taken as a sign of ovulation
In the 1st scan, the star marked follicle is the selected dominant follicle.
It is seen approaching the margin of the ovarian cortex & also is the largest of all
others.

The defect in the follicle heals in 2-5 days.
The wall thickens as cells are "luteinized"( lining cells enlarge and fill with lipid), and in most cases, the antrum fills with blood to form a "Corpus Hemorrhagicum”.
The follicle becomes a "Corpus Luteum", contributing hormone secretion, particularly progesterone to support the Secretory Phase.
On ultrasound, the corpus luteum reappears in in several forms.• 1/3 are a typical cyst of similar size to the mature follicle or larger. • 1/3 are more echogenic, forming a nearly "solid" ultrasound appearance.• 1/3 are not apparent at ultrasound examination.
If pregnancy occurs, HCG secreted by the trophoblast maintains the corpus luteum through the 10 week of gestation. If pregnancy does not occur, the Corpus Luteum usually disappears within a day or two of the onset of menses.

Because almost all functional ovarian cysts disappear by the 5th day of the subsequent cycle, concerns regarding neoplastic origin of unusually large functional of cysts can usually be dispelled by demonstrating their disappearance by 3-5 days into the next cycle.
For the same reason, screening for early ovarian tumors must be done during the first 5 days of the cycle to avoid needless confusion with physiologic cysts.
CLINICALIMPORTANCE
ABNORMAL FOLLICULAR CYCLES
Sporadic Anovulatory Mechanisms
Chronic Ovulation Failure•FO
LLICULAR ATRESIA
•EMPTY FOLLICLE
SYNDROME
•LEUTINIZED
UNRUPTURED FOLLICLE
SYNDROME
•HYPER-GONADOTROPISM
•HYPO-
GONADOTROPISM
•POLY CYSTIC
OVARIAN DISEASE/SYNDRO
ME

FOLLICULAR ATRESIA
In these cycles, the proliferative maturing effects of E2 (estrogen) are not properly synchronized with the the LH (luteinizing hormone).
The resulting follicle does not reach full size or ovulate.
Ultrasound shows a dominate follicle which does not reach full mature size (16-24mm.) and become rapidlyatresic. This is the morphologic pattern most frequently observed in patients taking oral contraceptives.
EMPTY FOLLICLE SYNDROME
Follicular development is grossly normal, but aspiration or natural ovulation does not produce an oocyte.
Failure to demonstrate a cumulus oophorus with a mature follicle on very high resolution ultrasound may beseen. However visualization of the cumulus is difficult under optimal conditions, the accuracy of ultrasoundin demonstrating the syndrome in probably low. Under routine study, these cycles are likely to appear normal.
LEUTINIZED UNRUPTURED FOLLICLE
SYNDROME
In this syndrome, an apparently normal mature luteinized follicle fails to rupture and ovulate. It goes on to behave as a luteinized follicle.
The syndrome can be recognized as a follicle which fails to collapse inassociation with the expected LH peak.
Ultrasound findings cant be taken as conclusive.

HYPER-GONADOTROPISM
Primary ovarian failure leads to small ovaries and low secretion of estrogen.
The anestrogenic state leadsto lack of feedback on gonadotrophin secretion and Hypergonadotropism.
Causes include primary failure, autoimmune damage, and chromosomal mosaicism.
Ultrasound shows small or absent ovaries without follicles.
Except in autoimmune causes, this group of patients do not respond to treatment.
HYPO-GONADOTROPISM
FSH and LH levels are found to be low, and evaluation for pituitary tumor is indicated.
Ovarian function is often normal and may be recovered through correction of pituitary problems, or exogenous FSH and HCG (LH replacement).
Due to inadequate stimulation, these patients also have lowestrogen levels.

POLY CYSTIC OVARIAN DISEASE / SYNDROME
On ultrasound, these patients ovaries may be "normal", but are more often enlarged ( > 6ml), and tend to have an increased number of small incompletely developed follicles (>11) and no dominant size follicles.
The stroma in the central part of the ovary is usually abundant and hyperechoic.
Doppler blood flow has been reported to be faster in PCOS.


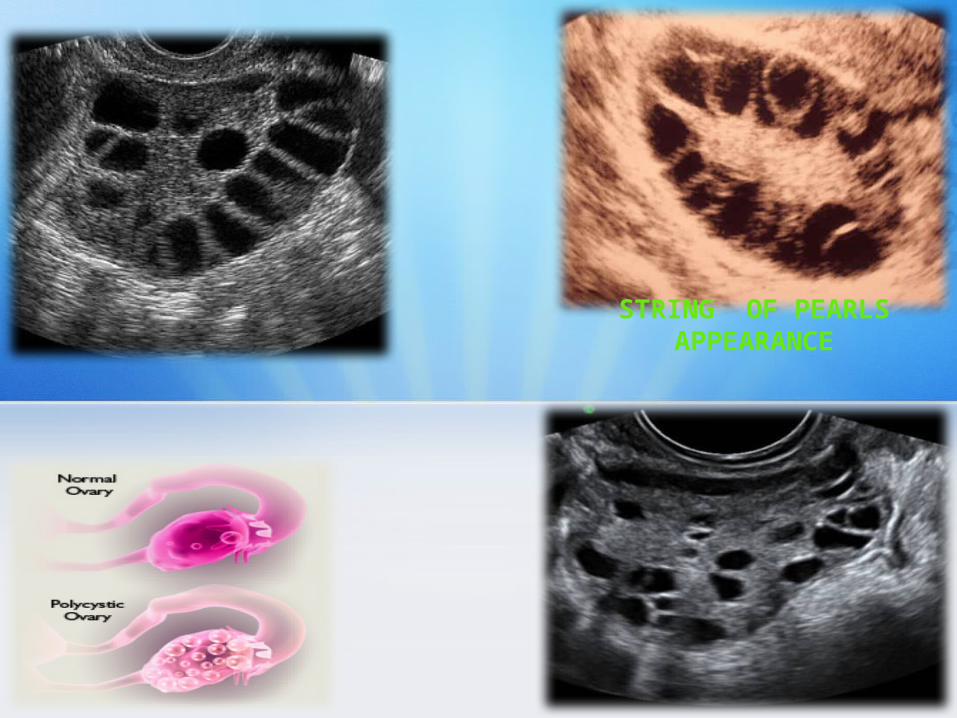
STRING OF PEARLS APPEARANCE

• May show features of polycystic ovaries – Bilateral enlarged ovaries with multiple small
follicles : 50%• Increased ovarian size (> 10 cc)• 12 or more follicles measuring 2 - 9 mm• Follicles of similar size• Peripheral location of follicles : which can give a
String Of Pearl Appearance• Hyperechoic central stroma• Ovarian outline may be slightly irregular
• Hypo-echoic ovary without individual cysts : 25%
• Normal ovaries : 25%• Endometrium – may appear as proliferative

OVARIAN HYPERSTIMULATION
SYNDROMEOvarian
Hyperstimulation
Syndrome (OHSS) is a complication from some forms
of fertility medication.

Ovarian hyperstimulation syndrome is particularly associated with injection of a hormone called human chorionic gonadotropin (hCG) which is used for inducing final oocyte maturation and/or triggering oocyte release.
The risk is further increased by multiple doses of hCG after ovulation and if the procedure results in pregnancy.
Using a GnRH agonist instead of hCG for inducing final oocyte maturation and/or release results in an elimination of the risk of ovarian hyperstimulation syndrome, but a slight decrease of the delivery rate of approximately 6%

Classification
Based upon the clinical manifestation and imaging findings, OHSS can be classified into
• Mild OHSS : Characterised by bilateral multicystic ovarian enlargement;
• Moderate OHSS : If there is associated ascites and abdominal distension;
• Severe OHSS : Characterised by hypovolemia, haemoconcentration, thrombosis, oliguria, pleural and pericardial effusion.

Typically shows bilateral symmetric enlargement of ovaries (often > 12 cm) with multiple cysts of varying sizes, giving the classic WHEEL - SPOKE APPEARANCE.
Associated ascites, pleural + / pericardial effusion (which is due to capillary leak) may also be present.


DERMOID• Ultrasound is the preferred imaging
modality. Typically an ovarian dermoid is seen as a cystic adnexal mass with some mural components. Most lesions are unilocular.
• Rokintansky Nodule / Dermoid Plug
• Diffusely or partially echogenic mass with posterior attenuation owing to sebaceous material and hair within the cyst cavity : TIP OF THE ICEBERG Sign
• Echogenic, shadowing calcific or dental (tooth) components
• Presence of fluid-fluid levels
• Multiple thin, echogenic bands caused by hair in the cyst cavity : DOT & DASH PATTERN.

TIP OF ICEBERG SIGN
Sebaceous material/hair/ calcified
material within the cyst.
Acoustic mismatch
Attenuation of the rays passing through the
above contents.
Behind these structures, all appears dark (sono-opaque)

CYSTIC VS MIXED APPEARANCE
Rokitansky nodule or Dermoid plug refers to a solid protuberence
projecting from an ovarian cyst in the context of a mature teratoma. It often contains calcific, dental, adipose, hair and / or sebaceous
components

THECA LUTEIN CYST
• A Theca Lutein Cyst is a type of bilateral functional ovarian cyst filled with clear, straw-colored fluid.
• To be classified a functional cyst, the mass must reach a diameter of at least three centimeters.
• These cysts originate when abnromally high Beta-HCG are elevated, which can occur due to multifetal gestations or molar pregnancies.

B/L THECA CYSTS

CORPUS LUTEAL CYST
CORPUS LUTEAL (CL) cyst is a type of functional ovarian cyst which results when a corpus luteum fails
to regress following the release of an ovum.
Such a cyst is complicated further by hemorrhage
occurring within the cyst.
When associated with pregnancy, it is the most
common pelvic mass encountered within the
1st trimester.

Colour Doppler shows either no vascularity within the cyst or at times show low
resistance blood flow around the cyst

ENDOMETRIOMAEctopic
Endometrium when present
within the ovaries,
proliferates under the
influence of hormones, during the
normal cycles.
Seen here, is the classical
GROUND GLASS APPEARANCE

Transabdominal ultrasound shows a multiloculated right ovarian endometrioma with low level
echoes




























![1 Estrategiadeempresayrhunr 131116113703 Phpapp01[1]](https://img.pdfslide.net/doc/110x75/577c81001a28abe054ab1236/1-estrategiadeempresayrhunr-131116113703-phpapp011.jpg)