Embed Size (px)
DESCRIPTION
Dr David Amor, Director, from Victoria Clinical Genetics Service has presented at the Obstetric Malpractice Conference. If you would like more information about the conference, please visit the website: http://bit.ly/10xh1iO
Citation preview

Implication of new genetic technologies on pre-pregnancy screening and prenatal testing
4th Annual Obstetric Malpractice Conference
David Amor
22nd June 2012
VCGS is a not for profit subsidiary of Murdoch Childrens Research Institute and the main provider of clinical and pathology genetics services in Victoria

All couples hope for a healthy baby, however human
reproduction is hazardous
• 4% of all babies are born with a congenital abnormality or genetic disorder that is evident at birth
• Most people have at least one recognised genetic disease
• All people are born with a genetic predisposition to various medical problems
• Every genome contains 50-100 variants that are expected to cause genetic disease
© Copyright 2012, VCGS. 2

Wrongful birth litigation may occur following birth of a child
with a genetic disorder when
1. A genetic risk was not identified prior to pregnancy
2. A genetic disorder was not detected during the pregnancy
© Copyright 2012, VCGS. 3
Inheritance Able to detect at risk couples prior to pregnancy
Able to detect during pregnancy
Inherited dominant + +
New dominant - +
Autosomal recessive + +
X-linked + +
Chromosomal +/- +
Polygenic - +/-
Epigenetic - +/-

Testing technologies and
practices relatively stable (and
limited) over last decade
• Taking a family history
• Down syndrome screening
• CVS and amniocentesis
• Ultrasound
Allowing various reproductive options to be exercised:
• TOP
• PGD
• Not have children
• Accept risk
© Copyright 2012, VCGS. 4
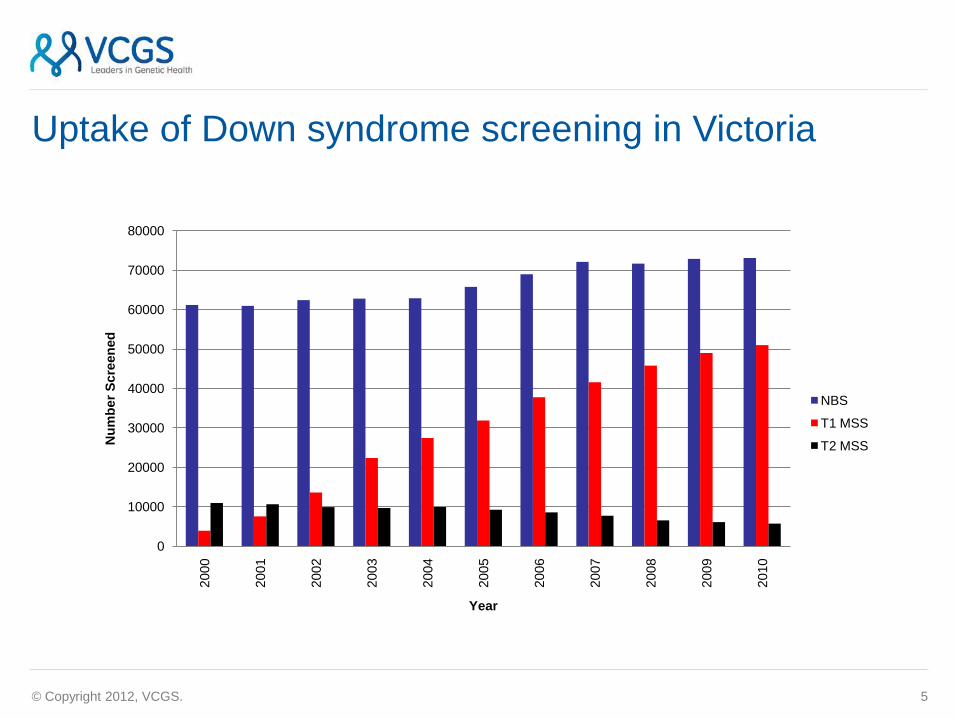
Uptake of Down syndrome screening in Victoria
© Copyright 2012, VCGS. 5
0
10000
20000
30000
40000
50000
60000
70000
80000
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
Nu
mb
er
Scre
en
ed
Year
NBS
T1 MSS
T2 MSS

Three new genetic technologies will transform prenatal
diagnosis over the next five years
• Microarray
• Next generation gene sequencing
These two technologies are transformative because they offer the ability to simultaneously test for large numbers of genes in a cost effective manner
• Non-invasive prenatal diagnosis (NIPD)
© Copyright 2012, VCGS. 6

Microarray
(molecular karyotype)

Next generation DNA sequencing
• Currently able to sequence all genes in the body for approximately $2000 (HGP cost was $3 billion)
• Costs expected to be reduced to $100 per genome
• Data storage and analysis are considerable problems

Non invasive prenatal diagnosis (NIPD)
• Using fetal DNA from maternal blood
• Available in USA, China and Hong Kong
• Used as screening test because accuracy <100%
• Cost $1000-$2000
• Currently only capable of detecting DS and small number of other abnormalities
© Copyright 2012, VCGS. 9

Testing prior to pregnancy –
Screening for autosomal recessive disease
• AR diseases individually rare but collectively common
• >1000 known recessive genes (many more unknown)
• All people have some recessive genes
• Many variants of uncertain significance

Recessive genetic screening in Australia
In Australia, the main single gene conditions for which pre-pregnancy genetic carrier screening is undertaken are:
• Haemoglobinopathies (thalassaemia)
• Autosomal recessive diseases more common in the Ashkenazi Jewish community including Tay-Sachs disease
• Cystic fibrosis (conflicting guidelines and policy)

The ‘long tail’ of recessive genetic disease
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
Car
rie
r fr
eq
ue
ncy
Disease frequency

‘Counsyl’ genetic test
• Microarray-based approach
• Just test for specific known mutations
• Cost $350-$500
• Screens for 105 diseases (mostly rare)
• Substantial risk of false negative results
• Risk of false positive results
• 1 in 4 people receive abnormal result

New York Times January 29, 2010
“Firm Brings Gene Tests to Masses”
• A Silicon Valley start-up is making the bold claim that it can help eradicate more than 100 diseases by alerting parents-to-be who have the carrier genes.
• Counsyl is selling a test that it says can tell couples whether they are at risk of having children with a range of inherited diseases.
• Once informed, couples can take steps like using IVF with genetic testing of embryos, to avoid bearing children who would have the diseases.
“As a genetic counselor, I’ve been waiting for this for a really long time,”- Elena Ashkinadze genetic counselor.
• But some experts say the company’s Web site overstates the case. The company calls its product the Universal Genetic Test, for example, even though there are thousands of genetic diseases, not just the 100 Counsyl tests detect.
“Everyone hopes there is a test that will provide a perfect baby, but the reality is that that single magic bullet doesn’t exist,”
- Dr. Joe Leigh Simpson, a geneticist and obstetrician.
• Some experts say that such screening could save countless parents from heartache, and society from the millions of dollars it can cost to care for even one severely ill person over a lifetime.
• But some experts foresee new issues. So many people would be carriers for at least one disease that genetic counselors might be overloaded. Some critics, meanwhile, say such testing is a step toward designer babies.

Next generation sequencing approach
• Low cost (analytical cost $400)
• Test whole sequence of 437 (or more) genes
• All people will receive abnormal result therefore need to test both partners
• Interpretation of many results difficult
• Reliant on existing databases that are known to contain inaccuracies
© Copyright 2012, VCGS. 15
Testing in established pregnancies-
Chromosome microarray in prenatal diagnosis
• Introduced in Australia in 2011 but limited uptake to
date
• Expected to replace microscope analysis within 2
years
• Compared to microscope chromosome analysis, will
detect abnormalities in an additional
• 1.7% pregnancy with normal ultrasound
• 5.8% of pregnancies with abnormal ultrasound
• Also will detect abnormalities of:
• Unknown significance
• Uncertain significance
• Incidental findings
© Copyright 2012, VCGS. 16
New genetic technologies present many new challenges
• Testing capabilities have outstripped our ability to counsel and interpret information
• Pace of change is extremely rapid – when does a test become ‘standard of care’ and how will this be judged retrospectively?
• Multiple testing options replacing small numbers of mature tests
• Informed choice and consent
• Incidental findings and findings of uncertain significance
• Multiple testing brings increased risks of false positive results and risk of terminating a healthy pregnancy
• Interpretation of results is still evolving
• No funding mechanisms in place
• Insufficient resources for counselling
• Ethical issues
© Copyright 2012, VCGS. 17

The future?
© Copyright 2012, VCGS. 18

© Copyright 2012, VCGS. 19