Embed Size (px)
Citation preview

Improvement in adherence to HAART: Best practices in adherence education by three model programs
Myriam Hamdallah, MS, MPH Center on AIDS & Community Health FHI 360

Session Objectives
– Provide a background/context of the study
– Describe the three agencies and their adherence education interventions
– Describe the study methodology
– Share findings
– Discuss implications and recommendations

Study Context – the ConnectHIV initiative
• ConnectHIV was a national initiative supported by the Pfizer Foundation through $7.5million in grants, technical assistance and networking resources over three years (2007-2010) to 20 mid-sized AIDS Service Organizations (ASOs) in the10 states with highest AIDS prevalence in the United States.

ConnectHIV Funding Categories
The 20 organizations differed in populations served & interventions implemented –
from prevention of infections among high-risk, HIV-negative persons, to promotion of adherence and delay of disease progression among persons living with HIV

Agency Characteristics
Characteristics ASO A ASO B ASO C Agency funds for HIV services
$2.17M $3.96M $2.80M
FTE staff in agency 47 36 24 FTE staff dedicated to program
2 1 4
PT staff dedicated to program
5 2 3
Volunteers dedicated to program
12 0 20

Agency Characteristics
Characteristics ASO A ASO B ASO C Staff to client ratio for AE intervention
1:26 1:26 1:21
HIV/AIDS services delivered in-house 13 5 6
% Clients substance abuse/addiction co-morbidity
30 66 75
% Clients - psychiatric co-morbidity
65 30 70

Characteristics of populations served
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Female Male Sex w persons of the opposite sex
Sex w persons of the same sex
ASO A
ASO B
ASO C

Age of the populations served
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
<= 19 20 - 29 30 - 39 40 - 49 50+
ASO A
ASO B
ASO C

Intervention Characteristics
ASO A ASO B ASO C
Obj
ectiv
es
To mobilize family, peer & social support as key elements in successful adherence.
To help clients needing additional assistance for stability in both housing and medical adherence.
To equip clients w. knowledge, skills to understand science behind HIV, care & treatment; prevent 2˚ infection; focus on compliance and adherence; become advocates
Stru
ctur
e
● Individual counseling ● 8-session women’s wellness HIV support groups ● Peers met 1X week, & face to face at intervals for one year ● MEMS cap –2 weeks
● Individual level intervention. ● Peers met with clients once a week for 12 weeks or about 3 months.
● 18-hour peer-led training (offered as a 3-day or a 6-day course) that includes 8 content specific education modules

Intervention Characteristics
ASO A ASO B ASO C
Cou
nsel
ing
Individual health counseling with HIV medication adherence specialist
Individual meeting with Peers; review medication regimen; create I-MAPs; problem solve barriers to adherence; provide HIV med education & adherence counseling.
Counseling is provided in house as needed but is not part of the intervention.
Educ
atio
n
Adherence education - Help clients understand illness; provide information on meds & regimen.
Personalized medication education; Review of medication regimen; Individual Medication Adherence Plans (I-MAPs), are completed.
Fundamentals of HIV biology med development, resistance, doc/patient relation, advocacy, nutrition, compliance & adherence to HIV in special popn, clin trials, co-infections

Intervention Characteristics
ASO A ASO B ASO C
Peer
Pie
ce Clients are assigned a
treatment adherence buddy; they can attend support groups.
Peers conduct the intervention with supervisory support.
Peers lead the training.
Trai
ning
One-hour training session, paid $40 to attend.
Peers received 2 month training serve as Peer Coordinator or Peer Interns.
18-hour peer-led training (offered as a 3-day or a 6-day course).
Ince
ntiv
e
$20 for treatment adherence buddy; $10 for joint coffee meeting.
$200/week $20 at conclusion of training; bus passes, meals.

Study Methods
• survey/interview designed in collaboration with the grantees and an Evaluation Advisory Committee
• IRB approval obtained
• 30 min individual interview with client
• baseline and two follow-up measures – 2-6 months from baseline for the second measure
– 6-12 months from baseline for the third measure

Variables
• HIV disease management knowledge
• Overall experience taking HIV medications
• Viral load
• CD4 count
• Perceived health score

Variables and Measures
• HIV disease management knowledge score 1. What happens when someone with HIV infection has a high
CD4 count?
2. What indicates that HIV infection has progressed to AIDS?
3. Typically, how often should a person with HIV have their viral load and CD4+ counts assessed?
4. In order for HIV medications to be effective, they should be taken…
5. If someone with HIV misses or skips taking some of their anti-HIV medications…
6. Anti-HIV medications can cause some health issues called "side-effects."

Variables and Measures
• Overall experience taking HIV medication
• Over the last 30 days, which of the following best describes your general experience taking your HIV medications? – 1. I never take my pills
– 2. I take my pills less than 50% of the time
– 3. I take my pills between 50 and 90% of the time
– 4. I take my pills at least 90% of the time
– 5. I take them exactly as prescribed, never missing a dose.

Variables and Measures
• Viral load
• Categorical variable developed from actual viral load data or self-reported viral load data (if clinical data was not available) with the following Likert-style categories: – 1. Undetectable (<400 or <40 depending on test)
– 2. Detectable, but less than 1,000
– 3. Between 1,000 and 9,999
– 4. Between 10,000 and 55,000
– 5. More than 55,000

Variables and Measures
• CD4 count – What was your most recent CD-4 or T-cell count?’ A
continuous variable was developed from the actual CD4 data or self-reported CD4 data (if clinical data was not available).
• Perceived health score – On a scale from 1 to 100, how would you rate your
overall health?
– Worst Health = 1; Perfect Health = 100

Data Analysis
• Generalized Estimated Equations (GEE) models were created to determine change over time (taking into account repeated measures over individuals –measures at baseline, post and follow-up)
• N=386
• The models controlled for client level confounders - age and gender
• Significance was reported at a < 0.05 level.

Findings
Outcome
Mean Scores Level of Significance
Baseline
1st FU
2nd FU
Baseline vs. 1st FU
Baseline vs. 2nd FU
1st FU vs. 2nd FU
Knowledge of HIV disease management (1-14) (N=386)
11.36 11.98 12.14 <.001 <.001 NS
Overall experience taking HIV medication (1-5) (N=356)
4.36 4.52 4.58 <.001 <.001 NS
Viral load (1-5) (N=374) 1.82 1.54 1.48 <.001 <.001 NS CD4 count (N=367) 517 543 554 <.05 <.01 NS
Perceived health score (1-100) (N=384)
76 81 83 <.001 <.001 NS
Change Across Mean Scores of Client Outcomes from Baseline to 1st to 2nd Follow-up

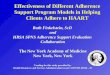
Findings
75 79
79
73
80
77
77
84
88
70
75
80
85
90
95
100
Baseline Post Followup
Aver
age
Hea
lth S
core
(1-1
00)
Overall Health Score by Period "How would you rate your health (1-100)?"
ASO A
ASO B
ASO C

Interactions
• Gender was significantly (p<.01) associated with knowledge of HIV disease management; males tended to score higher than females
• Gender was significantly (p<0.01) associated with HIV medication experience; men took their medications more consistently than women
• Age was significantly associated with viral load; clients 50 years and older had significantly lower viral load compared to those younger than 30 (p <0.05)

Interactions
• Gender significantly associated with overall health score, with males scoring higher than females (P<0.001)
• Age significantly associated with overall health score, with persons under 30 years of age scoring significantly higher than older persons (p<.001)

Discussion
• Significant positive change from baseline to post, & baseline to follow-up across all client outcomes
• All 3 interventions accomplished goal of improving adherence to HIV medications
• Two ASOs (A and B) reviewed individual regimens; B developed IMAPs (Individual Medication Adherence Plans); C’s intense training focused on adherence

Discussion
• Peers were key element in ASO B’s & C’s and a component of ASO A’s intervention – Rationale for peer support/peer-led interventions
• Social support theory (positive relations; emotional & other support)
• Experiential knowledge (practical experience)
• Social learning theory (learning in social context & role modeling)
– CDC’s compendium/adherence chapter includes two interventions with peer components

Discussion
• Knowledge of disease mgmt – Men scored higher than women; & Adherence – Men had higher adherence than women (stigma; child care; adverse drug effects reported)
• Viral load – older had lower VL than younger (increased virologic suppression in older adults reported in literature)
• Health score – Men scored higher than women

Implications & Recommendations
• Patient education, imparting knowledge on HIV management & importance of adherence; review of regimens; problem solving to reduce barriers
• Strong, well supported peer components with structured training and incentives
• Consider competing priorities for women, in addition to managing potential adverse drug effects and stigma

Authors:
• Myriam Hamdallah
• Stacey Little
• Dave Nimmons
• Lisa Rizzano
Unpublished Manuscript and Acknowledgements
• Derek Worley
• Caitlin Corcoran
• Susan J. Rogers
• Acknowledgements: The authors would like to thank Evany Turk and Warren Reich as well as other staff from the ConnectHIV grantee agencies and their clients for their contribution to the manuscript and to Atiya Ali Weiss at the Pfizer Foundation, David Holtgrave at Johns Hopkins University and to Sally Munemitsu and Janice Brown at TCC.

Contact Information & Thank you!
• Myriam Hamdallah
• 202 884 8858