Embed Size (px)
Citation preview
Induction of labour
Prepared by :Jomanah A.Hmood

Induction of labor is the artificial initiation of labour mechanism prior to its spontaneous onset.
Augmentation refers to stimulation of spontaneous contractions that are considered inadequate because of failed cervical dilation and fetal descent.

INDICATIONS Broadly speaking, an IOL is performed
when the risks to the fetus and/or the mother of the pregnancy continuing exceeds those of bringing the pregnancy to an end.

Common indications for induction of labour
Prolonged pregnancy Fetal growth restriction Pre-eclampsia and other maternal hypertensive
disorders Prelabour rupture of membranes Chorioamnionitis Placental abruption Diabetes mellitus Twin pregnancy continuing beyond 38 weeks Maternal iso-immunization Fetal malformations incompatible with life ‘Social’ reasons Risk of rapid labor, distance from
hospital, psychosocial indications
Common indications Prolonged pregnancy There is evidence that pregnancies extending
beyond 42 weeks gestation are associated with a higher risk of stillbirth, fetal compromise in labour, meconium aspiration and mechanical problems at delivery.
Prelabour rupture of membranes The longer the time delay between membrane
rupture and the delivery of the baby, the greater the risk of ascending infection (chorioamnionitis) and neonatal infectious morbidity
High Priority
Preeclampsia ≥ 37 weeks Significant maternal disease not
responding to treatment Significant but stable antepartum
hemorrhage Chorioamnionitis Suspected fetal compromise

CONTRAINDICATIONS
1. Major degree of Placenta praevia 2. Vasa praevia 3. Previous classical uterine incision4. significant prior uterine surgery (e.g. full
thickness myomectomy)5. Cephalopelvic disproportion because of
malpresentation or abnormal pelvic bone structure.
6. Active genital Herpes infection ,7. Invasive cervical carcinoma ,8. Hypersensitivity to cervical ripening
agents
Bishop score to quantify how far this process had
progressed prior to the IOL. High scores (a ‘favourable’cervix) are associated with an easier, shorter induction that is less likely to fail. Low scores (an ‘unfavourable’ cervix) point to a longer IOL that is more likely to fail and result in Caesarean section.

women with a score of > 9 were equally likely to deliver vaginally whether induced or allowed to labour spontaneously and could be delivered within 4 hours and most within 24 hours.
A favourable preinduction Bishop score of > 6 successful vaginal delivery.
The rate of failed induction was higher for women with a very low Bishop score (0 to 3)
Time, place & preparation
Time of induction: Preferably early morning
Place of induction: where facility for intervention and fetal monitoring is available
Preparation of Patient : Enema may be given to patients prior to induction

Factors to assess prior to induction
Maternal To confirm the indication Exclude the contraindication Assess Bishop score Assess pelvic adequacy Fetal Ensure fetal gestational age Ensure fetal presentation Confirm fetal well being

METHODS
Membrane Sweeping
Prostaglandins
Amniotomy
Oxytocin
Methods of induction of
labor

METHODS
Prostaglandins
PGE1Misoprostol
PGE2Dinoproston
e
ProstaglandinsLocal applications of PGs causes cervical ripening by:•Alteration of extracellular grounds substance of cervix by increasing collagenase , elastase, glycosaminoglycans ,•Relaxation of smooth muscle of cervix
Contraindications Previous uterine scar is relatively
contraindicated Established uterine activity, asthma, severe hepatic or renal impairment , known hypersensitivity to prostaglandins , active vaginal bleeding

PGE2 Dinoprostone
Intracervical PGE2 gel:
•Contains 0.5 mg of PGE2 •Bring the gel to room temperature before use and instill in the cervical canal below the internal os •The patient lies supine for 15-30 minutes after the insertion . •If no response occurs in one use a repeat insertion may be required after 6 hours .•Maximum of 1.5 mg \24 hours. •If required oxytocin is to used only after 6- 12 hours of the last insertion.
Intravaginal PGE2 gel: •Vaginal PG E2 gel : - contains 2.5 mg PGE2 - 2 doses 6 hours apart are used •Vaginal controlled release insert : (Cervidil ) - 10 mg insert which releases 0.3 mg / hr of the prostaglandin - The patient should lie supine for 2 hours following the insertion- The insert is to be removed after 12 hours or when active labor begins or in case of hyperstimulation.
•Intracervical use is technically more difficult •Vaginal route ( gel or insert ) is superior to intracervical route for cervical ripening but it causes higher uterine activity
•The overall incidence of hyperstimulation is 4.8% - same as with oxytocin. •the incidence is more when used in active labor (12.5 %)• more with vaginal gel (5%) than intracervical (1%) and least with controlled release insert

Misoprostol:•Mioprostol is a synthetic PG E1 analogue which has been used as a gastric cytoprotective agent since 1988 for patients of peptic ulcer.•How to give Misoprostol? Dose of 25 micro gram every 4hrly to a maximum of 6
doses can be given intravaginally into the posterior vaginal fornix ,
Dose of 50micro gram every 3hrs to a maximum of 6 doses can be given orally
Dose of 25micro gram every 2hrs can be given orally Other routes of administration: 1.Buccal 2.rectal 3.sublingual

Oral Vs vaginal Misoprostol
oral
Less effective when compared to vaginal PG
Chance of fetal distress is less
vaginal
More effective when compared to oral route
Chance of fetal distress is more
Misoprostol Vs Dinoprostone Cheap & cost
effective Stable at room
temp
Costly Need refrigeration
Oxytocin It’s synthetised in the hypothalamus. Half life of 3-4 mins and duration of
action 20 mins Oxytocin is used very commonly to
achieve induction of labour. The objective is to produce uterine
contractions that effectively produce cervical change and descent of the presenting part.
Mode of Action
1.It acts through the receptor and voltage gated calcium channelmyometrial contraction
2.It stimulates amniotic and decidual PG production
Routes of administration: I.V infusion Intra muscular Buccal tablets Nasal spray
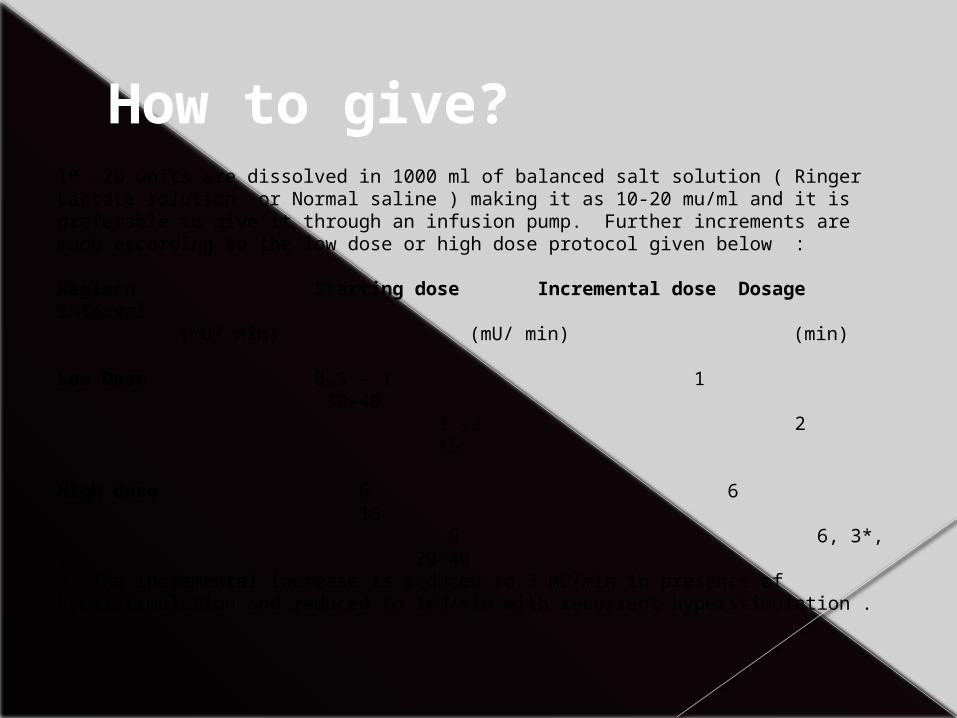
How to give?10 –20 units are dissolved in 1000 ml of balanced salt solution ( Ringer Lactate solution or Normal saline ) making it as 10-20 mu/ml and it is preferable to give it through an infusion pump. Further increments are made according to the low dose or high dose protocol given below : Regimen Starting dose Incremental dose Dosage interval
(mU/ min) (mU/ min) (min) Low Dose 0.5 – 1 1 30-40 1 –2 2 15 High dose 6 6 15 6 6, 3*, 1* 20-40 * The incremental increase is reduced to 3 mU/min in presence of hyperstimulation and reduced to 1mU/min with recurrent hyperstimulation .
Oxytocin should be used with extreme caution in multiparous women.
Oxytocin should not be started for six hours following administration of vaginal prostaglandins
Oxytocin should be used with caution with a previous uterine scar.
Oxytocin should always be used in conjunction with the partogram once in established labour.
Hazards of oxytocin Uterine hyperstimulation: (>5 contractions in 10mins each
lasting for 1min) Water intoxication:It due to anti diuretic action(30-
40IU/ml) .Manifested by hyponatremia ,confusion ,coma
Fetal distress Uterine rupture
When to interrupt? When there is hyperstimulation of
uterus Fetal distress Signs of water intoxication.(Occurs
with the max dose of 100 IU in the interval of less than 24hrs .clinically Manifested after 24hrs)
Oxytocin Vs Misoprostol Safe,cheap and
effective Unstable at room temp Easily titrable Chance of fetal
distress is less More effective near
term Less effective with less
Bishop score and in IUD
Tablet form is cheap& effective
Stable at room temp,PGE1-unstable
Not titrable Chance of fetal
distress is more Effective irrespective
of gestation

amniotomy
Ideally amniotomy or ARM is performed when the cervix is effaced and 2 cm dilated but it can be performed with minimal cervical dilatation. Methodology of ARM:•Auscultate the FHR •Evaluate the cervix and station of head. The cervix should be well applied to the head •Introduce two fingers into the cervix , sweep away the membranes from the cervix •Pass an Allis or Kocher’s forceps in between the groove of your two fingers , hook the membranes and rupture them ; look for the clarity of liquor
•Risks: Cord prolapse FHR deceleration Bleeding through vasa praevia Fetal injury Maternal and fetal infection Advantages: - It shortens duration of labor - Allows for early diagnosis of meconium staining of amniotic fluid,specially in high risk pregnancy - Facilitates invasive fetal monitoring

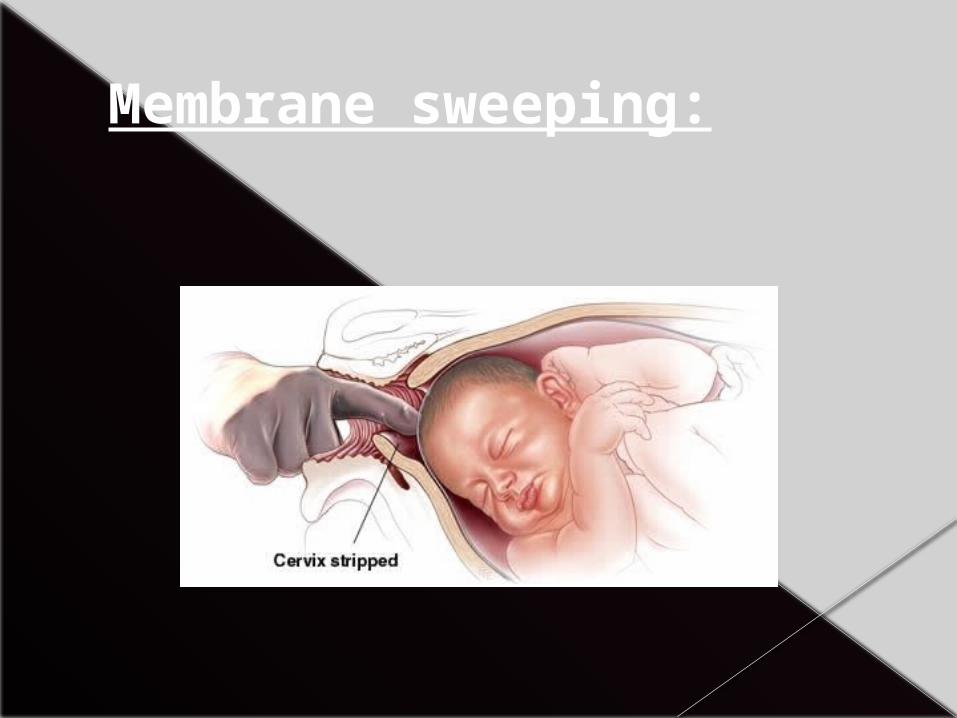
Membrane sweeping: Its possible only if the cervix has ripened to
allow the passage of one finger. Insertion of a gloved finger through the
cervix and it’s rotation against the wall of the uterus.
Its strips off the chorionic membrane from the underlying decidua releases PGS
Placenta previa should be excluded, Accidental amniotomy is a disadvantage and can be uncomfortable for the woman.
Membrane sweeping:

Balloon Devices: Foley Catheter
For a single balloon catheter, a no. 18 Foley is introduced under sterile technique into the intracervical canal past
the internal os. The bulb is then inflated with 30 to 60 cc of water. The catheter is left in place until either it falls out spontaneously or 24 hours have elapsed.
Low-lying placenta is an absolute contraindication to the use of a Foley catheter.
Relative contraindications to its use include antepartum hemorrhage, rupture of membranes, and evidence of lower tract genital infection.

There is an increased need for oxytocin when Foley catheters are used.
In comparison with prostaglandins, Foley catheters cause much less uterine tachysystole.
Foley catheters are not associated with increased rates of maternal infection (chorioamnionitis and endometritis) or neonatal infection.

Hygroscopic dilators: These are natural or synthetic rods inserted through the cervical os and left in situ for a particular time wherein because of their osmotic properties they
absorb endocervical and local tissue fluids . This swelling causes a controlled dilatation of the cervix along with releasing prostaglandins.

Castor Oil
It is known to stimulate gut peristalsis and labor most likely is stimulated due to release of prostaglandins.
Other methods like : Nitric Oxide , Mifepristone (an anti-progesterone), Intercourse , Herbal supplements, Acupuncture and TENS( Transcutaneous electric nerve stimulation)
COMPLICATIONS 1.Greater pain in labour 2. Long labours augmented with oxytocin
predispose to postpartum haemorrhage secondary to uterine atony.
3. Cord prolapse If ARM is performed while the fetal head is high then cord prolapse may occur, precipitating the need for emergency delivery by Caesarean section.

COMPLICATIONS 4. Uterine hyperstimulation and fetal
compromise : Fetal compromise is more common during induced labours and this is due to uterine hyperstimulation caused by the injudicious use of prostaglandins and oxytocin.
A contraction frequency of 5 per 10 minutes should be treated by stopping the oxytocin and the administration of a tocolytic drug, most commonly the subcutaneous injection of the β2-agonist terbutaline.
Uterine hyperstimulation may precipitate a fetal bradycardia and the need for emergency Caesarean section if the fetal heart rate fails to resolve promptly.
5. Greater risk of uterine rupture:Women with a previous Caesarean section scar, or some other form of old uterine injury, are at greater risk of uterine rupture if they are induced. The risk of scar rupture increases from one in 200 in a spontaneous labour, to as high as one in 70 if induction of labour is performed using prostaglandins.
6. Increased need for Caesarean or instrumental delivery : The rates of instrumental delivery and Caesarean section are higher following induction, and not all of this increase can be explained by the underlying problems which necessitated the induction in the first place.

7. FAILURE this is said to have occurred if an ARM
is still impossible after the maximum number of doses of prostaglandin have been given,
or if the cervix remains uneffaced and less than 3 cm dilated after an ARM has been performed and oxytocin has been running for 6–8 hours with regular contractions.
When induction fails: When an induction fails, the options include attempting induction again at some point in the
future, or performing a Caesarean section. Delaying delivery further is only acceptable if
there is no major threat to fetal or maternal condition.This may be the case with a failed social induction,for example.
Failed induction in the setting of preeclampsia or fetal growth restriction will usually necessitate Caesarean delivery.
during Induction of Labor, B enefits should be weighed, R isks should be assessed, A lternatives should be considered, N ecessity of intervention adjudged & D ecision should be taken accordingly BUT INJUDICIOUS USE of Labor Inducing agents
should be avoided

THANK YOU