Embed Size (px)
DESCRIPTION
This is a presentation I gave at Texas A&M University in November 2012. It is a talk that summarizes this publication: http://rd.springer.com/article/10.1007/s10708-011-9445-3
Citation preview

P. JOHNELLE SPAR KS, P HDDEPARTMEN T OF DEMOGR APHY
THE U N I VER SI TY OF TEXAS AT SAN AN TON I O
COR EY S. SPAR KS, PHDDEPARTMEN T OF DEMOGR APHY
THE U N I VER SI TY OF TEXAS AT SAN AN TON I O
JOSEPH CAMPBELL , PHDU SAA
MODELI N G SECTI ON
An Application of Bayesian Spatial Statistical Methods to the Study of
Poverty Segregation and Infant Mortality Rates in the United States

Outline
IntroductionInfant Mortality in the US
Risk factors at the individual level Risk factors at the population level
Linking Residential Segregation Methods and DataResultsFurther Issues to discuss

Introduction
The United States has an Infant Mortality Rate (IMR) higher than one would expect, given the stature of our economy and access to advanced medical resources
Numerous studies have examined this phenomena from both individual and population-level perspectives Disparities exist by race, ethnicity, birth weight,
environmental conditionsHere, we explore the connection between
residential segregation and infant mortality from a population perspective

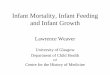
Iceland Austria Cuba Albania Ukraine Thailand Libya Nicaragua Nepal Comoros Sudan Burundi0
20
40
60
80
100
120
140
160
180
Infant Mortality Rate, 2008
IMR
US: Ranked 48th
In the world
31st Among OECD Countries

Infant Deaths by Cause, 2008
Congressional Research Service R41378

Infant Mortality in the US
Contributing Factors: Inconsistent recording of births
Are we just bad at counting? We use the WHO standard, like other nations
Unfavorable rates of LBW and short gestational age births US rate of LBW and short for gestational age births is
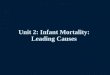
double that of some European nations Our IMR would be 39 if this was adjusted! These risk factors also varies widely by race/ethnicity of
mother Racial and ethnic disparities

US IMR by Race/Ethnicity of Mother, 2007
NCHS Data Brief #74, Sept 2011

Infant Mortality in the US
In summary, the US has several conditions that puts infants and mothers in an unfavorable position
Most of these are related to socioeconomic inequality within the population
One potentially important factor, related to inequality is residential location More to the point, the spatial arrangement of
racial/ethnic minorities and low-income individuals relates to that of the majority group

Residential Segregation
Racial and socioeconomic residential segregation generally exposes minority groups to negative structural, social, economic, material, and individual level resources. More specifically, poor housing quality, environmental
contaminants, lower educational and employment opportunities, access restrictions to social services, limited access to healthy and fresh food options, high crime rates, low investment in infrastructure, and poor access to medical services
Some authors go on to say that segregation leads to higher levels of economic inequality among racial/ethnic groups Minorities are isolated from employment opportunities and
social services available in more white areas

Residential Segregation
Less work has focused on the explicit role of poverty segregation on infant health Outside of using the poverty rate
This is often because poverty rates and minority concentration are highly correlated
However it may be the relative differences in economic resources for minority residents that impact infant mortality chances Persons living in areas with better than expected
economic circumstances, also noted as positive income incongruity, may benefit from certain forms of residential segregation

Residential Segregation
Regardless of whether segregation is racial or economic, it is multidimensional It is not clear how certain dimensions of residential
segregation are protective or harmful against infant mortality risks, particularly when measuring both racial and poverty residential segregation in a spatial context.
Some authors have found that residential isolation led to poorer infant health outcomes, while racial clustering led to better outcomes
In terms of poverty segregation, we might expect that areas with higher interaction (integration) might lead to lower infant mortality rates

Spatial is Special
When considering health outcomes, policy makers work at a local level
Knowing more about the location of ones’ constituents may help public officials serve them better
Being able to visualize where levels of risk differ is a powerful policy tool Translates the statistical skull drudgery into real
world context Spatial methods help with this

Methods and Data
Data Source 2008 Area Resource File
Outcome: 3 Year count of infant deaths in each county 24,487 total deaths 4,041,042 live births in the period Equates to a rate of 60.6 deaths per 10,000 live births
Control variables Rural population Income inequality Neighborhood deprivation

Methods and Data
Segregation Measures 3 dimensions Evenness -> Dissimilarity Index Exposure -> Interaction Index Spatial Clustering -> Spatial Proximity Index
Refer to Reardon and O’Sullivan (2004) Sociological Methodology and Massey and Denton (1988) Social Forces
•Measured Black-White and Poor-Non Poor segregation•6 total measures

Bayesian Estimation
When we combine the likelihood and the prior, we form what is called the posterior distribution
Thus we have Bayes Theorem which in the continuous case is:
Which states, the posterior distribution of θ, conditional on y is the product of the likelihood and the prior distribution of θ

The denominator in Bayes theorem is a constant, and this is generally written as:
Which says the posterior is proportional to the likelihood times the prior

Models
The model we used is the convolution model, or the Besag, York and Mollie model yi
| θi ~Pois(ei θi) log(θi)=α+ X’β + ui + vi
θi is commonly thought of as the Standardized Mortality Ratio (SMR)
Where ui is a correlated heterogeneity (CH) term and vi is an Uncorrelated Heterogeneity (UH) term
ui is given a Conditionally Autoregressive Normal prior~ ( , / )i j ju N u n

Model Estimation
OpenBUGS 150,000 MCMC samples, 100k burn in 2 parallel chains Thinned every 50th sample to reduce autocorrelation Gelman-Rubin diagnostics revealed convergence of
the models12 Models were fit
6 just considered segregation 6 considered segregation, controlling for the SES
variables Models are compared with Deviance Information
Criterion (DIC)

Results: SMR Observed

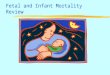
Results: SMR Smoothed

Results
Racial Segregation Without controlling for county SES, dissimilarity
increases the IMR, Interaction decreased the IMR and Spatial clustering increased the IMR
After controlling for SES, the effects of segregation are diminished, except for interaction, but maintain significant effects
Poverty Segregation Similar trends are found for poverty segregation in
the baseline models After controlling for SES, poverty dissimilarity
becomes insignificant in the model

Discussion
Results show the utility of Bayesian models for modeling unstable rates Smoothed risk profile
Interaction between both blacks and white and poor/non-poor residents tends to decrease infant mortality Net of SES controls
However, the more spatially concentrated both blacks and residents below the poverty line, the higher the infant mortality risk

Future Issues
We should consider a spatio-temporal approach instead of the purely spatial one taken here Cross sectional associations are weaker
Ideally, we could emulate this work with individual level data using similar hierarchical models
Currently we are applying these methods to a variety of health outcomes Ethnic differences in cancer incidence Cardiovascular disease Crime rates

Acknowledgements
My two co-authorsUTSA COPPThe TAMU Census RDC