Embed Size (px)
Citation preview
Infective Endocarditis
Download more documents and slide shows on The Medical Post [ www.themedicalpost.net ]
Dr. Kalpana MallaMBBS MD (Pediatrics)
Manipal Teaching Hospital
Definition
• Infective Endocarditis (IE): an infection of the heart’s endocardial surface
Classified into four groups: – Native Valve IE– Prosthetic Valve IE– Intravenous drug abuse (IVDA) IE– Nosocomial IE
Epidemiology
• The valves involved– Mitral 28-45%– Aortic 5-36%– Both 0-35%
– Tricuspid 0-6%– Pulmonary <1%
Epidemiology
• Incidence - varies according to location• Males > females• May occur at any age and increasingly
common in elderly• Mortality 20-30%

Predisposing Factors
Iv drug use
Central line
Prosthetic valve
Previous IE
Murmur
Dental procedure
Rheumatic disease
Miscellaneous

Risk for Endocarditis
• High risk– Prosthetic cardiac valve– Prior episodes of endocarditis– Complex congenital cardiac defect– Surgical systemic-pulmonary shunts
– Intravenous drug abuse – Intravascular catheters
Risk for Endocarditis
• Moderate risk– PDA, VSD, primum ASD– Co-Aorta– Bicuspid aortic valve– Hypertrophic cardiomyopathy– Acquired valvular dysfunction– MVP with mitral regurgitation
Risk for Endocarditis
• Low risk– Isolated secundum atrial septal defect– ASD, VSD, or PDA > 6 months past repair– “Innocent” heart murmur by auscultation in the
pediatric population
Further Classification
• Acute– Affects normal heart valves– Rapidly destructive– Metastatic foci– Commonly Staph.– If not treated, usually fatal within 6 weeks
• Subacute– Often affects damaged heart valves– Indolent nature– If not treated, usually fatal by one year
• The terms acute and subacute are used to define duration of infection, however are older terms and should not be used
• A classification based on organism is preferable
Pathophysiology
1. Turbulent blood flow disrupts the endocardium making it “sticky”
2. Bacteremia delivers the organisms to the endocardial surface
3. Adherence of the organisms to the endocardial surface
4. Eventual invasion of the valvular leaflets
Infecting Organisms
• Common bacteria in children– S viridans – 50% cases– S. aureus – 40% cases– S. fecalis ,Grp D sreptococcus (Enterococci)
Less common organisms
– P. aeruginosa, Staph epidemidis– Histoplasma, candida, Aspergillus– Coxiella burnetti, Brucella, chlamydia– HACEK grp – Hemophilus, Actinobacillus,
Cardiobacterium hominis, Eikenella, kingella
Symptoms• Acute
– High grade fever and chills
– SOB– Arthralgias/ myalgias– Abdominal pain– Pleuritic chest pain– Back pain
• Subacute– Low grade fever– Anorexia– Weight loss– Fatigue– Arthralgias/ myalgias– Abdominal pain
Signs• Fever • Heart murmur• Nonspecific signs – petechiae, subungal or
“splinter” hemorrhages, clubbing, splenomegaly, neurologic changes
• More specific signs - Osler’s Nodes, Janeway lesions, and Roth Spots
Petechiae
1.Nonspecific2.Often located on extremities
or mucous membranes
Splinter Hemorrhages
1.Nonspecific2.Nonblanching3.Linear reddish-brown lesions found under the nail
bed4.Usually do NOT extend the entire length of the nail
Osler’s Nodes
1.More specific2.Painful and erythematous nodules3.Located on pulp of fingers and toes4.More common in subacute IE
Janeway Lesions
1.More specific2.Erythematous, blanching macules 3.Nonpainful4.Located on palms and soles

The Essential Blood Test
• Blood Cultures– Minimum of three blood cultures– Three separate venipuncture sites– 5- 10mL in children– ½ to 1hr apart– Out of three one should be for anaerobic organisms
• Positive Result– Typical organisms present in at least 2 separate samples– Detects over 95% of cases
Negative blood culture
• Previous antibiotic• Technical errors• Unusual organisms- anaerobic
organisms,fungus
Additional supportive Labs
• CBC• ESR and CRP• Urinalysis-microscopic hematuria in 95%• Immunologic tests –• Increase in gamma globulins• Presence of cryoglobulin • Low Complement levels (C3, C4)• RF- positive (59%)

Imaging
• Chest x-ray – Look for multiple focal infiltrates and calcification
of heart valves• EKG
– Rarely diagnostic– Look for evidence of ischemia, conduction delay,
and arrhythmias• Echocardiography- diagnostic tool for culture
negative cases
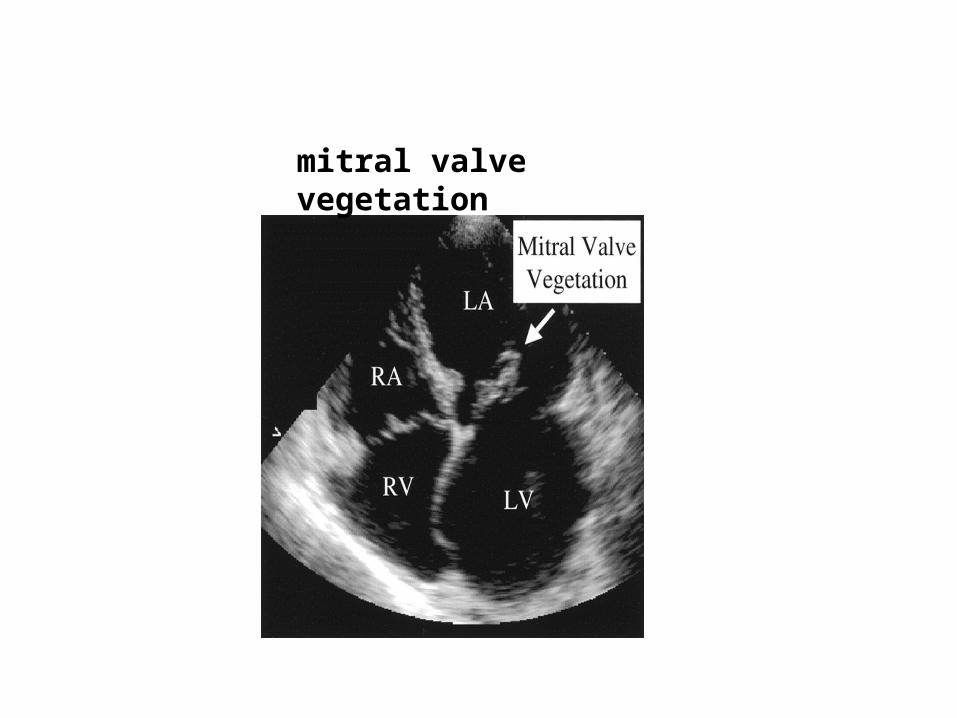
mitral valve vegetation

Making the Diagnosis
• Pelletier and Petersdorf criteria (1977)• Von Reyn criteria (1981)• Duke criteria (1994)• Modified Duke Criteria
Diagnostic (Duke) Criteria
• Major criteria– Positive blood culture for IE– Evidence of endocardial involvement

Duke’s Major Criteria
• positive blood culture for IE– typical microorganism (strep viridans, strep bovis, HACEK
group, staph aureus or enterococci in the absence of a primary locus) for endocarditis from two separate blood cultures
– persistently positive blood culture from:• blood cultures drawn more than 12 hr apart, or• all of 3 or a majority of 4 or more separate blood
cultures, with first and last drawn at least 1 hr apart
Duke’s Major Criteria
• Evidence of endocardial involvement– positive echocardiogram for endocarditis
Duke’s Minor Criteria
• Predisposing heart condition or iv drug use• Fever of 100.40F or higher• Vascular phenomena : - major arterial emboli - septic pulmonary infarcts - mycotic aneurysm - intracranial hemorrhage - conjunctive hemorrhages - Janeway lesions
Duke’s Minor Criteria• Immunologic phenomena: - Glomerulonephritis - Osler’s nodes - Roth spots - Rheumatoid factor)• Microbiologic evidence: - positive blood culture not meeting major
criteria or serologic evidence of active infection with organism consistent with IE)
• Echocardiogram -consistent with IE but not meeting major criteria)
Modified Duke Criteria• Definite IE
– Microorganism (via culture or histology) in a valvular vegetation, embolized vegetation, or intracardiac abscess
– Histologic evidence of vegetation or intracardiac abscess
• Possible IE– 2 major– 1 major and 3 minor– 5 minor
Modified Duke Criteria
• Rejected IE–Resolution of illness with four days or
less of antibiotics
Treatment
• Parenteral antibiotics
• Surgery– Intracardiac complications
• Surveillance blood cultures
Antimicrobial Therapy• Antibiotics IV for 2-6 weeks
1. Penicillin-susceptible streptococcal (PSSE) on native cardiac valves:
• Penicillin G - 4 weeks or• Penicillin G or ceftriaxone + gentamicin - 2 wks2. Penicillin-resistant streptococcal (PRSE) on native
cardiac valves – • Penicillin, ampicillin, or ceftriaxone for 4 weeks +
gentamicin for the first 2 weeks
Antimicrobial Therapy
3.PSSE on prosthetic valve-• penicillin, ampicillin, or ceftriaxone - 6 wks +
gentamicin for the first 2 wks.4. PRSE on prosthetic valve – penicillin, ampicillin, or ceftriaxone for 6 weeks
+ gentamicin for first 2 wks
Antimicrobial Therapy
5. Enterococcal infection on native valves - penicillin or ampicillin + gentamicin for 4-6 weeks
Antimicrobial Therapy
6.Methicillin-susceptible S aureus (MSSA) on native valves :
- Nafcillin or oxacillin for at least 6 weeks + gentamicin for 3-5 days is optional
7. Methicillin-resistant S aureus (MRSA) on native valves:
- vancomycin for at least 6 weeks, with or without 3-5 days of gentamicin
Antimicrobial Therapy
8. MSSA infection on prosthetic valve :- Nafcillin or oxacillin + rifampin for at least 6
weeks, in combination with gentamicin for 2 weeks.
9. MRSA infection on prosthetic valve:- Vancomycin + rifampin for at least 6 weeks, in
combination with gentamicin for 2 weeks
Antimicrobial Therapy
10. Gram negative endocarditis caused by HACEK organisms: - ceftriaxone or ampicillin plus gentamicin for 4 weeks
Culture Negative Endocarditis
• Intracellular organisms– Bartonella henselae– Coxiella burnetti– Mycoplasma pneumonia– Legionella pneumophila
• Diagnosis is made by checking IgM/IgG serologies
Culture Negative Endocarditis Treatment
• One should cover for the HACEK organisms, alpha streptococci & last slide
• Ceftriaxone 2 grams IV daily + vancomycin 1 g q 12 - 6 weeks
New Treatments
• Right-sided infective endocarditis due to methicillin-susceptible S aureus (MSSA) in IV drug users– 2-wk therapy with a penicillinase-resistant penicillin and
an aminoglycoside– 2-wk monotherapy with IV cloxacillin– short-term therapy is inappropriate if complicated by
ostomyelitis, meningitis, myocardial abscess, or concomitant left-sided involvement
New Treatments
• Highly penicillin-susceptible Streptococcus viridans or bovis– Once-daily ceftriaxone for 4 wks
• cure rate > 98%• easily administered as outpatient, avoid hospitalization, offers
significant cost savings
– Once-daily ceftriaxone 2 g for 2wks followed by oral amoxicillin qid for 2 wks
– Once-daily ceftriazone and netilmicin for 2 wks
New Treatments
• Prosthetic valve endocarditis due to fluconazole-susceptible Candida species– many are due to bloodstream invasion– chronic oral suppressive therapy with fluconazole for
inoperable disease
Surgical Treatment• 15-25% of patients with IE are treated
surgically• Indications -
– Antibiotic therapy fails – Persistent vegetation after systemic
embolization– Increase in vegetation size after antimicrobial
therapy– Valvular dysfunction– Fungal endocarditis
Complications of Endocarditis
• Cardiac 33-50%
• Neurologic 25-35%
• Emboli 15-35%
• Metastatic Abscesses <5%
Neurologic Complications
• Acute encephalopathy• Meningitis• Embolic stroke• Cerebral hemorrhage • Brain abscess

Embolic Phenomena
• Stroke• Ischemic extremities• Pulmonary emboli• Paralysis due to embolic infarction of
either the brain or spinal cord• Hypoxia from pulmonary emboli• Abdominal pain (splenic or renal infarction
Metastatic Spread of Infection
• Metastatic abscess – Kidneys, spleen, brain, soft tissues
• Meningitis and/or encephalitis• Vertebral osteomyelitis• Septic arthritis
Local Spread of Infection
• Heart failure– Extensive valvular damage
• Paravalvular abscess (30-40%)– Most common in aortic valve, IVDA, and S. aureus– May extend into adjacent conduction tissue causing
arrythmias– Higher rates of embolization and mortality
• Pericarditis• Fistulous intracardiac connections
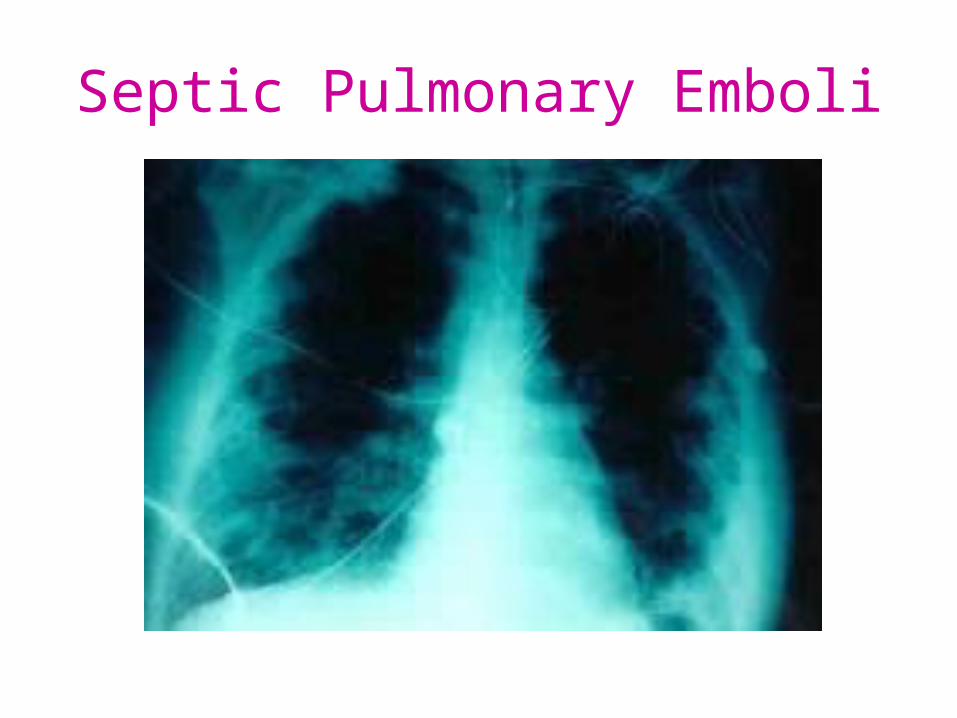
Septic Pulmonary Emboli
Poor Prognostic Factors
• Female• S. aureus• Vegetation size• Aortic valve • Prosthetic valve• Older age
• Diabetes mellitus• Low serum albumen • Apache II score• Heart failure• Paravalvular abscess• Embolic events
Thank youDownload more documents and slide shows on The Medical Post
[ www.themedicalpost.net ]


