Embed Size (px)
DESCRIPTION
Prepared by MD,PhD, Associate Professor, Marta R. Gerasymchuk Department of Pathophysiology, Ivano-Frankivsk National Medical University
Citation preview

INFLAMMATIONINFLAMMATION

1. Inflammation. Deffinition.
2. Signts of inflammation.
3. Etiological factors of inflammation.
4. Stages of inflammation.
5. Alteration. Mediators of inflammation.
6. Exudation. Mechanisms.
7. Phagocytosis. Disorders of phagocytosis.
8. Prolliferation.
9. Significance of inflammation.

The survival of all organisms requires that they eliminate foreign invaders, such as infectious pathogens, and damaged tissues. These functions are mediated by a complex host response called inflammationinflammation.
Inflammation Inflammation is a protective response intended to eliminate the initial cause of cell injury as well as the necrotic cells and tissues resulting from the original insult. Inflammation accomplishes its protective mission by diluting, destroying, or otherwise neutralizing harmful agents (e.g., microbes and toxins). It then sets into motion the events that eventually heal and repair the sites of injury.
Without inflammationWithout inflammation, infections would go unchecked and wounds would never heal. In the context of infections, inflammation is part of a broader protective response that immunologists refer to as innate immunityinnate immunity.
Inflammatory conditions are named by adding the suffix -itis -itis to the affected organ or system. For example, appendicitis refers to inflammation of the appendix, pericarditis to inflammation of the pericardium, and neuritis to inflammation of a nerve.

InflammationInflammation (“inflammatio” – from Latin)
It is a typical pathological process, It is a typical pathological process, which arises after damage of tissues and which arises after damage of tissues and
consists of three main vessel-tissues consists of three main vessel-tissues components: alteration, violation of components: alteration, violation of microcirculation with exudation and microcirculation with exudation and
emigration of leucocytes and emigration of leucocytes and proliferation.proliferation.
Not Not a synonym for a synonym for infection! infection!

Inflammations Inflammations classify:classify:
11) ) By clinical course:By clinical course: a) acute, b) subacute, c) chronic.2) By reason: 2) By reason: a) uninfectious origin (banal or unspecific) – caused uninfectious factors; b) infectious origin which includes for itself specific inflammations
(tuberculosis, syphilis, lepra, scleroma, glanders).3)3) By character of predominating phase of inflammation:By character of predominating phase of inflammation: a) alterative b) exudative, c) proliferative inflammation.4)4) In dependence on reactivity of organism of inflammation In dependence on reactivity of organism of inflammation
can be:can be: • a) normoergicnormoergic - adequate after the displays of factor which caused it; • b) hyperergichyperergic - is stormy (violent) course of inflammation, for example, on a
background (against a background) sensitizing; • c) hypoergichypoergic – with insignificant displays (for the children of 1th month of life,
in senile age, at considerable exhaustion of organism).
NeutrophilNeutrophil
acuteacute
LymphocyteLymphocyte
chronichroni
cc

Inflammation
Acute Inflammation Chronique InflammationFibrose
Cicatrisation
Phase vasculaire
Phase cellulaire
- allows inflammatory cells, plasma proteins - allows inflammatory cells, plasma proteins (e.g., complement), and fluid to exit blood (e.g., complement), and fluid to exit blood vessels and enter the interstitial spacevessels and enter the interstitial space
Characterized by the presence of edema and neutrophils in
tissue
Arises in response to infection Arises in response to infection (to eliminate pathogen) (to eliminate pathogen) or tissue or tissue necrosis necrosis (to clear(to clearnecrotic debris)necrotic debris)
Immediate response with
limited specificity (innate immunity)

Etiology of an inflammationEtiology of an inflammationThe external causesThe external causes of an inflammation are classified as of an inflammation are classified as
follows: follows: Physical factorsPhysical factors (foreign bodies, strong pressure on a (foreign bodies, strong pressure on a
tissue, high and low temperature, ionizing and ultra-tissue, high and low temperature, ionizing and ultra-violet rays, high and low barometric pressure, electrical violet rays, high and low barometric pressure, electrical current); current);
Chemical factorsChemical factors (acid, alkali, salts of heavy metals); (acid, alkali, salts of heavy metals); Biological factorsBiological factors (microorganisms – bacteria, viruses, (microorganisms – bacteria, viruses,
fungi; animal organisms – worms, insects). fungi; animal organisms – worms, insects).
The internal factorsThe internal factors are the factors, which arise in are the factors, which arise in organism, as the result of any other diseases, for example organism, as the result of any other diseases, for example cholic acids, complex antigen-antibody and others.cholic acids, complex antigen-antibody and others.

Local external signs of Local external signs of inflammationinflammation
The Roman The Roman CelsusCelsus in 1st century in 1st century A.D. named the famous four A.D. named the famous four cardinal signs of inflammation. cardinal signs of inflammation. The fifth sign added later The fifth sign added later by Virchow.by Virchow. 1) slight swelling – 1) slight swelling – tumortumor 2) reddening – 2) reddening – ruborrubor 3) increase of temperature3) increase of temperature (heat) – (heat) – calorcalor 4) pain – 4) pain – dolor dolor 5) loss of function – 5) loss of function – functio laesa.functio laesa.

Rubor (Rubor (rednessredness) ) andand calor (calor (heatheat) – ) – histaminehistamine-mediated -mediated vasodilatation of arterioles vasodilatation of arterioles

histaminehistamine-mediated-mediated in permeability of venules in permeability of venules
Synonyms with edema - Synonyms with edema - fluid in the interstitial space fluid in the interstitial space
Prostaglandin (Pg) E2Prostaglandin (Pg) E2 - - sensitizes sensitizes specialized nerve endings to the specialized nerve endings to the effects of effects of BRADYKININBRADYKININ and other and other pain mediators pain mediators

Pyrogens(e.g., LPS
from bacteria)
macrophages
perivascular cells of the
hypothalamus
PGE2
IL-1 and TNF
temperature set point
cyclooxygenase activity

Pathogenesis of inflammationPathogenesis of inflammation
The inflammation, as typical pathological The inflammation, as typical pathological process, consists of process, consists of three stagesthree stages: :
11st st is the is the alterationalteration stage; stage;
2nd2nd is violation of microcirculation with is violation of microcirculation with exudationexudation and emigration of leucocytes and emigration of leucocytes in the center of an inflammation in the center of an inflammation
3rd3rd – – proliferationproliferation. .

AlterationAlteration is the first component of inflammation, which is characterized by the injury of structurally-functional unit of an organ.
Alteration is divided onis divided on PrimaryPrimary alteration is the result of the influence
of the pathological (flogogenic) agent on a tissue. Metabolic and structural changes arise therefore.
SecondarySecondary alteration is the self-injury which takes place under the action of biological active substances (BAS) which are produced in consequence of primary alteration.
primaryprimary
secondarysecondary

The signs of cells damage are the follows:The signs of cells damage are the follows: the the рО рО22; ; limitation or terminationlimitation or termination of О of О22 consumption by cells; consumption by cells; the the of АТР and АDР and the of АТР and АDР and the of the inorganic of the inorganic
phosphorus concentration; phosphorus concentration; the the intensificationintensification of glycolysis, which cause the of glycolysis, which cause the
accumulation of lactic acid and piruvate acidaccumulation of lactic acid and piruvate acid; ; the the of cells рН. of cells рН.
The The of АТР of АТР concentration: concentration: reduces the activity of ionic pumpsreduces the activity of ionic pumps of cells membranes, of cells membranes, the parity of Na, K, Ca and Mg in cytoplasm is violated, the parity of Na, K, Ca and Mg in cytoplasm is violated, the activity of biochemical systems of cells is violated the activity of biochemical systems of cells is violated
too. too. Then content of water in cells changes, the synthesis of Then content of water in cells changes, the synthesis of
protein protein , the density of cytoplasm raises, the amount of , the density of cytoplasm raises, the amount of Н+ Н+ , the outlines of the cell change. , the outlines of the cell change.
These changes are reversible!These changes are reversible!

Mediators of inflammation Mediators of inflammation – it is biologically active substances, which appear in the place of inflammation and determine the pathogenesis of inflammation.
Distinguish two main groups of mediators from their origin:
Cellular origin Cellular origin appear and activated in
different cells
Plasmatic origin Plasmatic origin appear in cells, but
activated in plasma of blood
ProinflammatoProinflammatoryry
AntiinflammatAntiinflammatoryory
MediatoMediatorsrs

Toll-like receptors (TLRs)Toll-like receptors (TLRs)1. Present on cells of the innate immune system : macrophages; dendritic cells.
2. Activated by pathogen-associated molecular patterns (PAMPs) that are commonly shared by microbes
CD14 (a TLR) on macrophages recognizes lipopolysaccharide (a PAMP) on the outer membrane of gram-negative bacteria.
3. TLR activation results in upregulation of NF-kB, a nuclear transcription factor that activates immune response genes leading to production of multiple immune mediators.4. TLRs are also present on cells of adaptive immunity (e.g., lymphocytes) and, hence, play an important role in mediating chronic inflammation.

Cellular mediators: Cellular mediators: 1) 1) Lysosomal factorsLysosomal factors 2) 2) Products of degranulation of tissue basophilesProducts of degranulation of tissue basophiles
(biogenic amine: histamine, serotonin)(biogenic amine: histamine, serotonin) 3) 3) Derivatives of arachidonic acidDerivatives of arachidonic acid 4) 4) Peptide and proteinsPeptide and proteins (leukokines, cytokines, (leukokines, cytokines,
enzymes)enzymes) 5) 5) NNeuropeptideeuropeptides, neuromediatorss, neuromediators (adrenalin, (adrenalin,
noradrenaline (norepinephrine), noradrenaline (norepinephrine), acetylcholineacetylcholine).). 6) 6) Oxygen-Derived free RadicalsOxygen-Derived free Radicals (O (O22-, HO-, -, HO-,
HH22OO22). ). These metabolites increased vascular These metabolites increased vascular permeability, injured of cells. permeability, injured of cells.
7) 7) Nitric Oxyde (NO)Nitric Oxyde (NO) – the endothelium-derived – the endothelium-derived relaxation factor. Also it caused damage of the relaxation factor. Also it caused damage of the foreign and hosts cells.foreign and hosts cells.

Mediators of Mediators of Humoral Humoral (plasmatic)(plasmatic) origin origin includes 3 groups:includes 3 groups:
• HumoralHumoral mediators are characterized by the widespread effectswidespread effects; ; spectrum of their influence is very wide.
• The effects of cellular mediatorscellular mediators are locallocal. .
Products of Products of kallikrein-kallikrein-kininkinin
systemsystem
Products of activating Products of activating of of complementscomplements
systemsystem
Products of activating of Products of activating of coagulaticoagulativeve and and
fibrinolytic systemsfibrinolytic systems of of blood, biogenic aminesblood, biogenic amines
(histamine, serotonine) (histamine, serotonine)

Products of tissue Products of tissue basophiles degranulationbasophiles degranulation
Vasoactive aminesVasoactive amines– HistamineHistamine: : Arterial vasodilatation and venular endothelial cell Arterial vasodilatation and venular endothelial cell
contraction, junctional widening; contraction, junctional widening; Released by mast cells, basophils, platelets in Released by mast cells, basophils, platelets in
response to injury (trauma, heat), immune response to injury (trauma, heat), immune reactions (IgE-mast cell FcR), anaphylatoxins (C3a, reactions (IgE-mast cell FcR), anaphylatoxins (C3a, C5a fragments), cytokines (IL-1, IL-8), C5a fragments), cytokines (IL-1, IL-8), neuropeptides, leukocyte-derived histamine-neuropeptides, leukocyte-derived histamine-releasing peptides releasing peptides
– SerotoninSerotonin: : vasodilatation effects similar to those of histamine; vasodilatation effects similar to those of histamine; platelet dense-body granules; platelet dense-body granules; release triggered by platelet aggregationrelease triggered by platelet aggregation

The inflammatory cells—neutrophils and monocytes, contain lysosomal granules which on release elaborate a variety of mediators of inflammation. These are as under: 1) 1) Granules of neutrophils. Granules of neutrophils. Neutrophils have 3 types of Neutrophils have 3 types of granules:granules:
Primary or azurophil Primary or azurophil granules are large granules are large azurophil granulesazurophil granuleswhich contain which contain functionally active functionally active enzymes. These are:enzymes. These are:- myeloperoxidase, - myeloperoxidase, - acid hydrolases, - acid hydrolases, - acid phosphatase,- acid phosphatase,- lysozyme, lysozyme, - defensin (cationic defensin (cationic protein), - protein), - phospholipase,phospholipase,- cathepsin G, - cathepsin G, - elastase, elastase, - protease.protease.
Secondary or Secondary or specific granules specific granules contain:contain:- alkaline alkaline phosphatase,phosphatase,- lactoferrin, lactoferrin, - gelatinase, gelatinase, - collagenase, collagenase, - lysozyme, lysozyme, - vitamin-B12 vitamin-B12 binding proteins, binding proteins, - plasminogen plasminogen activator.activator.
Tertiary Tertiary granules granules oror C particles C particles contain: contain: - gelatinase,gelatinase,- acid acid hydrolases.hydrolases.

2) Granules of 2) Granules of monocytes monocytes and tissue and tissue macrophages. macrophages. These These cells on degranulation also release cells on degranulation also release mediators of inflammation like:mediators of inflammation like:
- acid proteases, acid proteases, - collagenase, collagenase, - elastase, elastase, - plasminogen activator. plasminogen activator.
However, they are However, they are more active in chronic more active in chronic inflammationinflammation than acting as mediators of acute than acting as mediators of acute inflammation.inflammation.

Monocytes and macrophagesMonocytes and macrophages

Derivatives of Arachidonic AcidDerivatives of Arachidonic Acid Arachidonic acid metabolites Arachidonic acid metabolites
(eicosanoids)(eicosanoids) ☼☼CyclooxygenaseCyclooxygenase produces produces
prostaglandins (PG).prostaglandins (PG). aa. . PGIPGI22, PGD, PGD22 and and PGEPGE22 mediate mediate
vasodilation vasodilation and and increased vascularincreased vascular permeabilitypermeability.. bb. . PGEPGE22 also mediates pain.also mediates pain. ☼☼ LipoxygenaseLipoxygenase produces produces
leukotrienes (LT).leukotrienes (LT). aa. . LTBLTB44, , attractsattracts and and activates activates
neutrophilsneutrophils.. bb. . LTC4, LTD4LTC4, LTD4, and , and LTE4 LTE4 (slow (slow
reacting substances of anaphylaxis) reacting substances of anaphylaxis) mediate vasoconstriction, mediate vasoconstriction, bronchospasmbronchospasm, and , and increased increased vascular permeabilityvascular permeability..
COXCOX blocked by blocked by aspirinaspirin and and NSAIDSNSAIDS
PAFPAF (platelet activating factor) (platelet activating factor)Derived also from cell membrane Derived also from cell membrane phospholipid, causes phospholipid, causes vasodilationvasodilation,, increasedincreased vascular permeability vascular permeability, , increasesincreases leukocyte adhesion leukocyte adhesion (integrin conformation)(integrin conformation)
CORTICOSTEROIDS
NSAIDs

CYCLOOXYGENASE
LIPOOXYGENASE

Peptide and ProteinsPeptide and Proteins Cytokines Cytokines are polypeptide substances produced by activated are polypeptide substances produced by activated
lymphocytes lymphocytes (lymphokines) and activated (lymphokines) and activated monocytes monocytes (monokines).(monokines). IL-1, TNF-IL-1, TNF- (formed by activated macrophages)(formed by activated macrophages) and and TNF-TNF-, IFN-, IFN- (produced by activated T cells) are especially (produced by activated T cells) are especially
important in inflammation.important in inflammation. The actions of various cytokines as mediator of inflammation are as The actions of various cytokines as mediator of inflammation are as
under:under: 1) IL-1 and TNF-α, TNF-β induce endothelial effects in the 1) IL-1 and TNF-α, TNF-β induce endothelial effects in the form form
of increased leucocyte adherence, thrombogenicity, elaboration of of increased leucocyte adherence, thrombogenicity, elaboration of other cytokines, fibroblastic proliferation and acute phase reactions.other cytokines, fibroblastic proliferation and acute phase reactions.
2) IFN-γ causes activation of macrophages and neutrophils 2) IFN-γ causes activation of macrophages and neutrophils and is associated with synthesis of nitric acid synthase.and is associated with synthesis of nitric acid synthase.
3) Chemokines are a family of chemoattractants for 3) Chemokines are a family of chemoattractants for inflammatory cells (as discussed above) and include:inflammatory cells (as discussed above) and include:
IL-8 IL-8 chemotactic for neutrophils;chemotactic for neutrophils; platelet factor-4 chemotactic for neutrophils, monocytes and platelet factor-4 chemotactic for neutrophils, monocytes and
eosinophils;eosinophils; MCP-1 MCP-1 chemotactic for monocytes; chemotactic for monocytes; eotaxin chemotactic for eosinophils.eotaxin chemotactic for eosinophils.



NeuropeptidesNeuropeptides• Another class of vasoactive amines is Another class of vasoactive amines is
tachykinin neuropeptides, such as: tachykinin neuropeptides, such as: • substance P, substance P, • neurokinin A, neurokinin A, • vasoactive intestinal polypeptide(VIP), vasoactive intestinal polypeptide(VIP), • somatostatin.somatostatin.• These small peptides are produced in the central and peripheral nervous systems.These small peptides are produced in the central and peripheral nervous systems.• The major proinflammatory The major proinflammatory actions of these neuropeptides actions of these neuropeptides is as follows:is as follows:• a) a) Increased vascular permeability.Increased vascular permeability.• b) b) Transmission of pain stimuli.Transmission of pain stimuli.• c) c) Mast cell degranulation.Mast cell degranulation.

Nitric Oxide (NO)Nitric Oxide (NO) short-acting soluble free-radical gas short-acting soluble free-radical gas
with many functionswith many functionsProduced by endothelial cells, Produced by endothelial cells, macrophages, causes:macrophages, causes:
Vascular smooth Vascular smooth muscle relaxation muscle relaxation and vasodilationand vasodilation
Kills microbes in Kills microbes in activated activated macrophagesmacrophages
Counteracts Counteracts platelet adhesion, platelet adhesion, aggregation, and aggregation, and degranulationdegranulation

Humoral MediatorsHumoral Mediators There are three most important blood systems, which There are three most important blood systems, which
play main role during inflammation: kinines, play main role during inflammation: kinines, hemostasis/fibrinolysis and complement’s systems. hemostasis/fibrinolysis and complement’s systems.
The The ХХII factorII factor of blood coagulation activates of blood coagulation activates derivation derivation such kinines such kinines as theas the bradykinine bradykinine and and kallidinekallidine. .
Their main effects are:Their main effects are: pain, pain, dilatation of vessels, dilatation of vessels, rise of vascular wall permeability, rise of vascular wall permeability, activation of hemostasic and fibrinolysis systems. activation of hemostasic and fibrinolysis systems. The The system of hemostasis and fibrinolysissystem of hemostasis and fibrinolysis directly directly
participate in the generation of highly active participate in the generation of highly active mediators. mediators.
The The appearance of fibrinopeptidesappearance of fibrinopeptides promotes the promotes the increase of microvessels permeability, activation increase of microvessels permeability, activation of chemotaxisof chemotaxis. . PlasminePlasmine plays the main role in the plays the main role in the system of fibrinolysis; it system of fibrinolysis; it promotespromotes the derivation of the derivation of biological active substances, which biological active substances, which increase of vessels increase of vessels permeability.permeability.

1. Inactive proinflammatory protein produced in liver
2. Activated upon exposure to subendothelial or tissue collagen; in turn, activates:
I. Coagulation and fibrinolytic systems II. Complement III. Kinin system — Kinin cleaves high-
molecular-weight kininogen (HMWK) to bradykinin, which mediates vasodilation and increased vascular permeability (similar to histamine), as well as pain.


Kinin systemKinin system• Leads to formation of bradykininbradykinin
from cleavage of precursor • Vascular permeability
– Arteriolar dilation– Non-vascular smooth muscle
contraction (e.g., bronchial smooth muscle)
– Causes pain– Rapidly inactivated (kininases)

Complement systemComplement systemComplement systemComplement system The system of complement is a group of 20 plasma proteins The system of complement is a group of 20 plasma proteins
(C1-C9). (C1-C9). Components C1-C9 present in inactive form. Components C1-C9 present in inactive form. Their Their main functionmain function is the is the destruction of alien and own destruction of alien and own
changed cellschanged cells. . Activated via Activated via classic (C1)classic (C1) or or alternative (C3)alternative (C3) pathways to pathways to
generate generate MACMAC (C5 – C9)(C5 – C9) that that punch holes in microbe punch holes in microbe membranesmembranes
Activated Activated СС22 operates as kinines; operates as kinines; СС33 raisesraises vascular permeability and vascular permeability and stimulates the motionstimulates the motion of of
phagocytes; phagocytes; СС55 has properties of has properties of СС33 (but is (but is more activemore active) and stimulates ) and stimulates
the selection of leucocytes of lysosomic enzymes; the selection of leucocytes of lysosomic enzymes; СС55 stimulates the splitting of arachidonic acid and the stimulates the splitting of arachidonic acid and the
synthesis of leucotriens, promotes the forming of oxygen synthesis of leucotriens, promotes the forming of oxygen radicals and hydroperoxides of lipids;radicals and hydroperoxides of lipids;
СС5b-5b-СС99 (MAC) (MAC) is provided by the reactions of alien and own is provided by the reactions of alien and own cells lysis. cells lysis.

C3a, C5aC3a, C5a – – anaphylatoxinsanaphylatoxins vascular permeability/vasodilation (via vascular permeability/vasodilation (via histamine), mast cell degranulationhistamine), mast cell degranulation C5aC5a – chemotactic for PMN, monocytes, basophils, increase – chemotactic for PMN, monocytes, basophils, increase adhesion to endothelium (activates WBC), increases integrin avidityadhesion to endothelium (activates WBC), increases integrin avidity C3b, C3biC3b, C3bi – as an – as an opsoninopsonin, increases phagocytosis, increases phagocytosis



Disturbance of the microcirculation in Disturbance of the microcirculation in the inflammation areathe inflammation area
The first stagefirst stage is the short-term spasmshort-term spasm of vessels (arterioles), the secondsecond is the arterial hyperemiaarterial hyperemia, the third stagethird stage is the venous hyperemiavenous hyperemia, the fourth stagefourth stage is the prestasisprestasis, and the stasisstasis is the fifth stagefifth stage.
1. Irrespective of the type of injury, immediate vascular response is of transient vasoconstriction of arterioles. With mild form of injury, the blood flow may be re-established in 3-5 seconds while with more severe injury
2. Next follows persistent progressive vasodilatation which involves mainly the arterioles, but to a lesser extent, affects other components of the microcirculation like venules and capillaries. This change is obvious within half an hour of injury. Vasodilatation results in increased blood volume in microvascular bed of the area, which is responsible for redness and warmth at the site of acute inflammation the vasoconstriction may vasoconstriction may last for about 5 minutes. last for about 5 minutes.

3. Progressive vasodilatation, in turn, may elevate the 3. Progressive vasodilatation, in turn, may elevate the local local hydrostatic pressure resulting in transudation of fluid into hydrostatic pressure resulting in transudation of fluid into the extracellular space. This is responsible for swelling at the the extracellular space. This is responsible for swelling at the local site of acute inflammation.local site of acute inflammation.
4. 4. Slowing or stasis of microcirculation follows which Slowing or stasis of microcirculation follows which causes increased concentration of red cells, and thus, raised causes increased concentration of red cells, and thus, raised blood viscosity.blood viscosity.
5. 5. StasisStasis or slowing is followed by or slowing is followed by leukocytic margination leukocytic margination or or peripheral orientation of leukocytes (mainly neutrophils) along peripheral orientation of leukocytes (mainly neutrophils) along the vascular endothelium. The leukocytes stick to the vascular the vascular endothelium. The leukocytes stick to the vascular endothelium briefly, and then move and migrate through the endothelium briefly, and then move and migrate through the gaps between the endothelial cells into the extravascular space. gaps between the endothelial cells into the extravascular space. This process is known as This process is known as emigration emigration (discussed later in detail).(discussed later in detail).

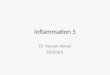
Fluid interchange between blood and Fluid interchange between blood and extracellular fluid extracellular fluid (ECF). (ECF).
(HP = hydrostatic pressure, OP = osmotic (HP = hydrostatic pressure, OP = osmotic pressure).pressure).
The appearance of inflammatory The appearance of inflammatory oedema due to increased vascular oedema due to increased vascular permeability of microvascular bed is permeability of microvascular bed is explained on the basis of explained on the basis of Starling’s Starling’s hypothesishypothesis. In normal . In normal circumstances, circumstances, the fluid balance is the fluid balance is maintained by two opposing sets of maintained by two opposing sets of forces:forces:
1) Forces that cause 1) Forces that cause outward outward movement of fluid from movement of fluid from microcirculation are microcirculation are intravascular intravascular hydrostatic pressure and colloid osmotic hydrostatic pressure and colloid osmotic pressure of interstitial fluid.pressure of interstitial fluid.
2) Forces that cause 2) Forces that cause inward inward movement of interstitial fluid movement of interstitial fluid into into circulation are circulation are intravascular colloid intravascular colloid osmotic pressure and hydrostatic osmotic pressure and hydrostatic pressure of interstitial fluid.pressure of interstitial fluid.

Mechanism Microvasculature Response Type Pathogenesis Examples
1Endothelial cell contraction
VenulesImmediate transient
(15-30 min)Histamine,
bradykinin, othersMild thermal injury
2Endothelial cell retraction
VenulesSomewhat delayed (in 4-6 hrs) prolonged (for
24 hrs or more)IL-1, TNF-α In vitro only
3Direct endothelial cell injury
Arterioles, venules, capillaries
Immediate prolonged (hrs to days), or
delayed (2-12 hrs) prolonged (hrs to
days)
Cell necrosis and detachment
Moderate to severe burns, severe
bacterial infection,radiation injury
4
Leukocyte-mediated endothelial injury
Venules, capillaries Delayed, prolongedLeukocyte activation
Pulmonary venulesand capillaries
5 Neovascularisation All levels Any type
Angiogenesis, VEGF (vascular
endothelialgrowth factor)
Healing, tumors

Exudative processesExudative processes The increase of vascular wall permeability provokes exudation (penetration of a liquid from the blood into the tissue), emigration of leucocytes. The permeability of microvessels increases first of all (especially of venules).

There are three ways penetration of fluid through the vessel wall (exudation).
The 1st way is interendotelial (between nearby endotheliocytes). Histamine promotes contraction of endothelial cells, the slots between nearby endotheliocytes extend, and basal membrane is exposed.
The 2nd way of exudation is transendotelial (through the endoteliocytes cytoplasm). Vesicles pinocytosis activity (the catch of fluid) of the endoteliocytes increases. The blood plasma is inside vesicles, which move through the cell and some time form channels. Various substances
can pass without any control through channels (microvesicle transport). The 3rd way of the exudation is the vessels wall area, where are injured endoteliocytes.

The main cause of the exudation is mediators of inflammation, but amplifying disorder of the metabolism, the injury cells and leucocytes promotes other pathological mechanisms, which increase vascular permeability.
They are lysosomes hydrolytic enzymes of various phagocytes and parenchimal cells (collagenase, collagenase, elastaseelastase) and bacterial enzymes (hyaluronidasehyaluronidase), lactic acid and piruvate acidlactic acid and piruvate acid, other non-oxidated substances, which are the result of tissues hypoxia, adenosine, Н+ and K+, especially during the decrease of Са2+ level. First of all albumins, than globulins and fibrinogen, which promotes the formation of fibrins clots, penetrate outside the vessels.

TTransudate – ransudate –
is is no no
inflammatory inflammatory
effusion. effusion.

Exudate kindsExudate kinds The inflammation is named the exudativeexudative if this
component is expressed stronger than others. The exudate type determines type of an inflammation.
There are next types of the exudates and inflammation: serous, fibrinous, purulent, decaying, hemorrhagic combination. The serous inflammation develops in mucous and
serous coats, interstitial tissue, skin, and kidneys glomes capsules. The amount of cells in the serous exudate is not large.


The fibrinous exudate contains a plenty of fibrinogen, which forms clots of fibrin in tissuesfibrin in tissues.
Such inflammation occurs when an organism is affected by corinebacterium diphtheriae, pneumococcus, Fridlander's bacillus, Frencel's diplococcus, streptococcus, and mycobacterium of tuberculosis.
Such type of an inflammation occurs on mucous or serous coats more often. Porcine Heart/Pericardium - fibrinous exudate (Mulberry Heart Disease)

The causes of purulent inflammation are staphylococcus, streptococcus, gonococcus, meningococcus, and Frenkel’s diplococcus.
Purulent exudate consists of many viable leukocytes and purulent bodies (perishing leukocytes), cells detritus, microorganisms, plenty of proteins (especially globulines)

• The decaying inflammation develops after the invasion of decaying microflora into the purulent inflammation site. During this type of inflammation necrosis of injurious tissues progresses, the inflammation area doesn’t localize, and this provokes the arrival of alien and toxic products into vessels and the development of intoxication due to which the patients usually dies.

The The hemorrhagichemorrhagic inflammationinflammation, as the form of , as the form of the serous, the fibrinous or the the serous, the fibrinous or the purulent inflammation, is purulent inflammation, is characterized by erythrocytes characterized by erythrocytes impurity to the exudate (Siberian impurity to the exudate (Siberian ulcer, natural ulcer, natural smallpoxsmallpox, , influenza). influenza).

The The combination combination formsforms of inflammation of inflammation are characterized by are characterized by connection of one type connection of one type of exudateof exudate to another to another. . Any combinations are Any combinations are possible. possible.
Such forms usually Such forms usually develop as the result develop as the result of connection of a new of connection of a new infection to the lasting infection to the lasting process. The tissues process. The tissues damage and the damage and the process of process of inflammation cause inflammation cause the restoring of broken the restoring of broken structure and function structure and function ((reparative reparative regeneration). regeneration).

Chronic OsteomyelitisChronic Osteomyelitis

The The uniqueunique featurefeature of the of the inflammatory process is inflammatory process is the the reaction of blood reaction of blood vessels, leading to the vessels, leading to the accumulation of fluid and accumulation of fluid and leukocytes in leukocytes in extravascular tissues.extravascular tissues.

In In most cases of acute inflammationmost cases of acute inflammation neutrophyles neutrophyles emmigrate the firstemmigrate the first (that process lasts (that process lasts 6-24 hours6-24 hours). ). In In 24-48 hours24-48 hours monocytes emigrate most activelymonocytes emigrate most actively..Lymphocytes Lymphocytes emigrate a little bit lateremigrate a little bit later. . Lymphocytes emmigrate first time during virus Lymphocytes emmigrate first time during virus infection and tuberculosis, and eosinophiles – during infection and tuberculosis, and eosinophiles – during allergic reactions. allergic reactions. Leukocytes regulate of the cells cooperation and Leukocytes regulate of the cells cooperation and delete the alien agents or the detritus of defective delete the alien agents or the detritus of defective tissues. tissues. The The neutrophilesneutrophiles ( (microphagesmicrophages) destroy pathological ) destroy pathological agents due to the following properties: agents due to the following properties:
the the absorptionabsorption of the foreign agent ( of the foreign agent (phagocytosisphagocytosis),), the the microbicydity and cytotoxicitymicrobicydity and cytotoxicity ( (these are the these are the
mechanisms of the foreign agent destroy by such mechanisms of the foreign agent destroy by such biooxidants as superoxide anions, hydroxyl- radicals, biooxidants as superoxide anions, hydroxyl- radicals, singlet oxygen, peroxide),singlet oxygen, peroxide),
the the intra-intra- and extracellular and extracellular lysislysis. .

Step 1 — MarginationStep 1 — Margination
1. Vasodilation slows blood flow in postcapillary venules.1. Vasodilation slows blood flow in postcapillary venules.
2. Cells marginate from center of flow to the periphery.2. Cells marginate from center of flow to the periphery.
Step 2 — RollingStep 2 — Rolling
1. Select in "speed bumps" are upregulated on endothelial cells.1. Select in "speed bumps" are upregulated on endothelial cells.
a) a) P-selectinP-selectin release from Weibel-Palade bodies is release from Weibel-Palade bodies is mediated by histamine.mediated by histamine.
b) b) E-selectin E-selectin is induced by TNF and IL-1.is induced by TNF and IL-1.
2. Selectins bind 2. Selectins bind sialylated carbohydrate groups sialylated carbohydrate groups related to the related to the Lewis XLewis X on leukocytes. on leukocytes.
3. Interaction results in rolling of leukocytes along vessel wall3. Interaction results in rolling of leukocytes along vessel wall

Step 3 — AdhesionStep 3 — Adhesion
1.1. Cellular adhesion molecules (Cellular adhesion molecules (ICAMICAM and and VCAMVCAM) are ) are
upregulated on endothelium by TNF and IL-1upregulated on endothelium by TNF and IL-1
2. 2. Integrins are upregulated on leukocytes by C5a and Integrins are upregulated on leukocytes by C5a and LtBLtB44
3.3. Interaction between CAMs and integrins results in firm adhesion of Interaction between CAMs and integrins results in firm adhesion of leukocytes to the vessel wall,leukocytes to the vessel wall,
4. 4. Leukocyte adhesion deficiency Leukocyte adhesion deficiency is most commonly is most commonly due to an autosomal due to an autosomal recessive defect of integrins recessive defect of integrins (CD18 subunit).(CD18 subunit).
• LAD type 1 is a deficiency of CD11 a:CD18 (LAD type 1 is a deficiency of CD11 a:CD18 (LFA-1 and Mac-1 subunit defects lead to impaired adhesion))
• LAD type 2 is a deficiency of a selectin that binds neutrophils (LAD type 2 is a deficiency of a selectin that binds neutrophils (Absence of sialyl-Lewis X, and defect in E- and P-selectin sugar epitopes).).
• Clinical featuresClinical features include: include: • Delayed separation of the umbilical cord (~1 month), (Delayed separation of the umbilical cord (~1 month), (neutrophil enzymes are
important in cord separation))• Increased circulating neutrophils (due to impaired adhesion of marginated pool of Increased circulating neutrophils (due to impaired adhesion of marginated pool of
leukocytes), leukocytes), • recurrent bacterial infections that lack pus formation (recurrent bacterial infections that lack pus formation (severe gingivitis, poor wound
healing)


Step 5 — PhagocytosisStep 5 — Phagocytosis
1.1. Consumption of pathogens or necrotic tissue; Consumption of pathogens or necrotic tissue;
2.2. Phagocytosis is enhanced byPhagocytosis is enhanced by
opsonins (opsonins (IgG and C3bIgG and C3b).).
3. 3. Pseudopodias extend from Pseudopodias extend from leukocytes to form phagosomes, which leukocytes to form phagosomes, which are internalized and merge with are internalized and merge with lysosomes to produce lysosomes to produce phagolysosomes.phagolysosomes.
Step 4 — Transmigration (diapedesis) and ChemotaxisStep 4 — Transmigration (diapedesis) and Chemotaxis1. 1. Leukocytes transmigrate across the endothelium of Leukocytes transmigrate across the endothelium of postcapillary venules and move toward chemical attractants postcapillary venules and move toward chemical attractants ((chemotaxischemotaxis).).2. 2. Neutrophils are attracted by bacterial products, IL-8, C5a, Neutrophils are attracted by bacterial products, IL-8, C5a, and LtBand LtB44..

Phagocytosis and Degranulation
• Once at site of injury, leukocytes:– Recognize and
attach– Engulf (form
phagocytic vacuole)
– Kill (degrade)1. Adhesion (chemotaxis)2. Attachment3. Engulfment4. Digestion

Chediak-Higashi syndrome Chediak-Higashi syndrome is a is a protein protein trafficking defect trafficking defect (microtubular defect), (microtubular defect), autosomal recessive, characterized by autosomal recessive, characterized by impaired phagolysosome formationimpaired phagolysosome formation. . Clinical features includeClinical features include1. 1. risk of risk of pyogenic infectionspyogenic infections2. 2. NeutropeniaNeutropenia (due to intramedullary (due to intramedullary death of neutrophils)death of neutrophils)3. 3. Giant granulesGiant granules in leukocytes (due to in leukocytes (due to fusion of granules arising from the Golgi fusion of granules arising from the Golgi apparatus)apparatus)4. 4. Defective primary hemostasis Defective primary hemostasis (due to (due to abnormal dense granules in platelets)abnormal dense granules in platelets)5. 5. AlbinismAlbinism (melanocytes can’t release (melanocytes can’t release melanin for ceratinocytes)melanin for ceratinocytes)6. 6. Peripheral neuropathyPeripheral neuropathy

Step 6 — Destruction of phagocytosed materialStep 6 — Destruction of phagocytosed material
1. 1. OO22-dependent killing -dependent killing is the most effective mechanism.is the most effective mechanism.
2. 2. HOCl HOCl generated by oxidative burst in phagolysosomes generated by oxidative burst in phagolysosomes destroys phagocytosed microbes.destroys phagocytosed microbes.
1)1) OO22 is converted to O is converted to O22▪‾▪‾by by NADPHNADPH oxidase oxidase
(oxidative burst!)(oxidative burst!)..Positive NBT test Positive NBT test (blue)(blue)..2) 2) OO22▪‾ ▪‾ is converted to His converted to H22OO22
by by superoxide dismutase superoxide dismutase (SOD).(SOD).
3) H3) H22OO22 is converted to is converted to HOCl▪ (HOCl▪ (bleachbleach) by ) by myeloperoxidasemyeloperoxidase (MPO). (MPO).

CGD is characterized by poor OCGD is characterized by poor O22-dependent killing.-dependent killing.
1). Due to 1). Due to NADPH oxidase defect ; NADPH oxidase defect ; X-linked or autosomal recessive;X-linked or autosomal recessive;
2). Leads to recurrent infection and 2). Leads to recurrent infection and granuloma formation granuloma formation with with catalase-catalase-positive organismspositive organisms, particularly:, particularly:
Staphylococcus aureus, Pseudpmonas cepacia,Staphylococcus aureus, Pseudpmonas cepacia, Serratia marcescens, Nocardia, Serratia marcescens, Nocardia, and and AspergillusAspergillus
3). Nitrobiue tetrazolium test (NBT) is used to screen for CGD. Leukocytes 3). Nitrobiue tetrazolium test (NBT) is used to screen for CGD. Leukocytes are incubated with NBT dye, which are incubated with NBT dye, which turns blue turns blue if NADPH oxidase can if NADPH oxidase can convert Oconvert O22 to O to O22▪‾, but remains ▪‾, but remains colorless if NADPH oxidase is detectivecolorless if NADPH oxidase is detective..

Results in defective Results in defective conversion of Hconversion of H22OO22, to HOCI▪., to HOCI▪.
1). 1). risk for Candida risk for Candida infections infections (most patients are(most patients are
asymptomatic).asymptomatic). 2). 2). NBT is normalNBT is normal; respiratory ; respiratory
burst (Oburst (O22 to H to H22OO22 is intact. is intact.
OO22-independent killing -independent killing is is less effectiveless effective than O than O22-dependent -dependent killing and killing and occurs via enzymes occurs via enzymes present in present in leukocyte secondary leukocyte secondary granules granules (e.g., lysozyme in macrophages and major basic (e.g., lysozyme in macrophages and major basic protein in eosinophils).protein in eosinophils).
Step 7 — ResolutionStep 7 — Resolution Neutrophils Neutrophils undergo apoptosis and disappear within 24 hours undergo apoptosis and disappear within 24 hours after resolution of the inflammatory stimulus.after resolution of the inflammatory stimulus.

1) return to normal vascular 1) return to normal vascular permeability; permeability;
2) drainage of edema fluid 2) drainage of edema fluid and proteins into lymphatics and proteins into lymphatics oror
3) by pinocytosis into3) by pinocytosis into macrophages; macrophages; 4) phagocytosis of apoptotic 4) phagocytosis of apoptotic
neutrophilsneutrophils 5) phagocytosis of necrotic 5) phagocytosis of necrotic
debris; debris; 6) disposal of macrophages. 6) disposal of macrophages.
Macrophages Macrophages also produce also produce growth factors that initiate growth factors that initiate the subsequent process of the subsequent process of repair. repair.
Note Note the central role of the central role of macrophages in resolution. macrophages in resolution.

The inflammation The inflammation proliferative proliferative phasephase• The inflammation proliferative phase is simultaneously a phase
of the reparatory regeneration. The restoring of the damaged tissues structure depends on the interaction of connective tissues cells among themselves (fibroblasts, macrophages, labrocytes, lymphocytes, endotheliocytes), on the interaction of connective tissues cells with the intercellular matrix (collagen, proteoglicans, fibronectine), on the interaction of connective tissue cells with blood cells and parenchymal ones.

Reparation and regenerationReparation and regeneration

WOUND HEALINGWOUND HEALING
BASIC PRINCIPLES I. Healing is initiated when inflammation begins. II. Occurs via a combination of regeneration and repair

The process of The process of cells proliferationcells proliferation is regulated by is regulated by substances, which can substances, which can stimulate (mitogens)stimulate (mitogens) or or oppress oppress (keilones)(keilones) the reproduction of cells. the reproduction of cells.
Cambial Cambial cells are the tissues source of regeneratory cells are the tissues source of regeneratory material. The damage of tissues material. The damage of tissues causes intensive causes intensive proliferation trunk cellsproliferation trunk cells. .
The reparative The reparative stage of inflammation begins when stage of inflammation begins when phagocytephagocytess actively swallow the microorganisms or the actively swallow the microorganisms or the tissuestissues detritus detritus. .
At that time At that time labrocyteslabrocytes activate interaction activate interaction with with macrophagemacrophagess, , fibroblastsfibroblasts, , and intercellular matrixand intercellular matrix, , clottingclotting blood system and promote the excretion and the synthesis of blood system and promote the excretion and the synthesis of substances, which substances, which stimulate stimulate proliferativeproliferative processes processes. .
ThrombocytesThrombocytes produce produce substances, which substances, which strengthen the strengthen the proliferationproliferation and the and the chemotaxis of fibroblastschemotaxis of fibroblasts to the to the injurious area: injurious area: the the thrombocytalthrombocytal growth factor growth factor of of fibroblastsfibroblasts, the , the factor of epidermis factor of epidermis and and fibroblasts growthfibroblasts growth, , the the peptidepeptide, which activates connective tissue, which activates connective tissue etc. etc.

1.1. Replacement of damaged tissue Replacement of damaged tissue with native tissue; dependent on with native tissue; dependent on regenerative capacity of tissueregenerative capacity of tissue
2. Tissues are divided into three types 2. Tissues are divided into three types based on regenerative capacity: based on regenerative capacity: • labile, labile, • stable, and stable, and • permanent.permanent.
3.3. Labile tissues Labile tissues possess possess stem cells stem cells that continuously cycle to regenerate that continuously cycle to regenerate the tissue.the tissue.
1). Small and large bowel (1). Small and large bowel (stem cells in mucosal cryptsstem cells in mucosal crypts))
2). Skin (2). Skin (stem cells in basal layerstem cells in basal layer))
3). Bone marrow (3). Bone marrow (hematopoietic stem cells, CD34+hematopoietic stem cells, CD34+))
4. Stable tissues 4. Stable tissues are comprised of cells that are quiescent, but can reenter are comprised of cells that are quiescent, but can reenter the cell cycle to regenerate tissue when necessary.the cell cycle to regenerate tissue when necessary.
Classic example Classic example is regeneration of liver by compensatory hyperplasia after is regeneration of liver by compensatory hyperplasia after partial resection. Each hepatocyte produces additional cells and then partial resection. Each hepatocyte produces additional cells and then reenters quiescence.reenters quiescence.
5. Permanent tissues 5. Permanent tissues lack significant regenerative potential lack significant regenerative potential (e.g., myocardium, skeletal muscle, and neurons).(e.g., myocardium, skeletal muscle, and neurons).

1. Replacement of damaged tissue with fibrous scarfibrous scar2. Occurs when regenerative stem cells are lost (e.g.,
deep skin cut) or when a tissue lacks regenerative capacity (e.g., healing after a myocardial infarction)
3. Granulation tissue formation is the initial phase of repair
Consists of fibroblastsfibroblasts (deposit type III collagen), capillaries capillaries (provide nutrients), myofibroblastsmyofibroblasts (contract wound)4. Eventually results in scar formation, in which type III
collagen is replaced with type I collagen1). Type III collagen Type III collagen is pliable and present in granulation tissue, embryonic tissue, uterus, and keloidskeloids;2). Type I collagen Type I collagen has high tensile strength and is present in skin, bone, tendons, and most organs;3). Collagenase Collagenase removes type III collagen and requires zinc as a cofactor.

Tissue granulation

I. Mediated by paracrine signaling via growth factors I. Mediated by paracrine signaling via growth factors (e.g., (e.g., macrophages secrete growth factors that target fibroblasts)macrophages secrete growth factors that target fibroblasts)
II. Interaction of growth factors with receptors II. Interaction of growth factors with receptors
(e.g.. epidermal growth factor with growth factor receptor) (e.g.. epidermal growth factor with growth factor receptor) results in gene expression and cellular growth.results in gene expression and cellular growth.
III. Examples of mediators includeIII. Examples of mediators include 1. 1. TGFTGFαα—epithelial and fibroblast growth factor—epithelial and fibroblast growth factor 2. 2. TGFTGFββ — important fibroblast growth factor; also inhibits — important fibroblast growth factor; also inhibits
inflammation;inflammation; 3. 3. Platelet-derived growth factor (Platelet-derived growth factor (PDGFPDGF))—growth factor for —growth factor for
endothelium, smooth muscle, and fibroblast growth factor;endothelium, smooth muscle, and fibroblast growth factor; 4. 4. Fibroblast growth factor (Fibroblast growth factor (FGFFGF) ) — important for — important for
angiogenesis; also mediates skeletal developmentangiogenesis; also mediates skeletal development 5. 5. Vascular endotheIial growth factor (Vascular endotheIial growth factor (VEGFVEGF)) — important — important
for angiogenesisfor angiogenesis

I. I. Cutaneous healing Cutaneous healing occurs via primary or secondary intention.occurs via primary or secondary intention.
1. Primary intention 1. Primary intention — wound edges are brought together (e— wound edges are brought together (e.g., suturing of .g., suturing of a a surgical incision); leads to minimal scar formation.surgical incision); leads to minimal scar formation.
2. Secondary intention 2. Secondary intention — edges are not approximated. — edges are not approximated.
Granulation tissue fills the defect; myofibroblasts then contract the wound, Granulation tissue fills the defect; myofibroblasts then contract the wound, forming a scar.forming a scar.
II. Delayed wound healingII. Delayed wound healing occurs in: occurs in:
1. Infection1. Infection (most common cause (most common cause S.aureusS.aureus is the most common offender)is the most common offender)
2. Vitamin C, copper, or zinc deficiency2. Vitamin C, copper, or zinc deficiency
1) 1) Vitamin CVitamin C is an important cofactor in the is an important cofactor in the hydroxylation of hydroxylation of prolineproline and and lysine procollagen residueslysine procollagen residues; ; hydroxylationhydroxylation is necessary for eventual collagen is necessary for eventual collagen cross-linking.cross-linking.
2) 2) CopperCopper is a cofactor for is a cofactor for lysyl oxidaselysyl oxidase, which cross-links lysine and , which cross-links lysine and hydroxy lysine to form stable collagen.hydroxy lysine to form stable collagen.
3) 3) ZincZinc is a cofactor for is a cofactor for collagenasecollagenase, which replaces the , which replaces the type III collagentype III collagen of of granulation tissue with stronger type I collagen.granulation tissue with stronger type I collagen.
3. Other causes include foreign body, ischemia, diabetes, and malnutrition.

III. Dehiscence is rupture of a wound; III. Dehiscence is rupture of a wound; most commonly seen after abdominal surgery
IV. Hypertrophic scarIV. Hypertrophic scar is excess production of scar tissue that is localized to the wound
V. Keloid V. Keloid is excess production of scar tissue that is out of proportion to the wound
1. Characterized by excess type III collagen2. Genetic predisposition (more common in African Americans)3. Classically affects earlobes, face, and upper extremities

The The influence of endocrine systeminfluence of endocrine system on the inflammation is on the inflammation is proved by numerous clinical observations. proved by numerous clinical observations.
HyperthyroidismHyperthyroidism amplifies manifestations of the amplifies manifestations of the inflammation and inflammation and hypothyroidismhypothyroidism is characterized by the is characterized by the insignificant sings. insignificant sings.
MineralocorticoidsMineralocorticoids promote the development of promote the development of inflammatory reactioninflammatory reaction and and glucocorticoidsglucocorticoids weaken weaken itit. .
The ability of The ability of glucocorticoidsglucocorticoids to weaken the to weaken the inflammationinflammation is constantly used in clinics because they: is constantly used in clinics because they:
reduce the amount of tissues basophiles, reduce the amount of tissues basophiles, increase the activity increase the activity of histaminaseof histaminase ( (enzymeenzyme, which , which
destroys destroys histaminehistamine), ), reduce reduce serotonine formationserotonine formation, , stabilize stabilize lysosomelysosome membranes and membranes and inactivateinactivate their their
enzymesenzymes.. GlucocorticoidsGlucocorticoids induce synthesis of proteinsinduce synthesis of proteins, , which which
block block prostaglandinesprostaglandines and and leucotriensleucotriens synthesis synthesis. . MineralocorticoidsMineralocorticoids are capable to are capable to strengthen the strengthen the
exudationexudation, to , to accelerate the reproduction of cellsaccelerate the reproduction of cells, the , the derivation of new capillariesderivation of new capillaries, and , and synthesis of the synthesis of the connective tissueconnective tissue..

BASIC PRINCIPLESBASIC PRINCIPLES
I. I. Characterized by the Characterized by the presence of lymphocytes presence of lymphocytes and plasma cellsand plasma cells in tissue. in tissue.
II. II. Delayed response, but more specific (adaptive Delayed response, but more specific (adaptive immunity) than acute inflammationimmunity) than acute inflammation
III. III. Stimuli include:Stimuli include:1)1) persistent infection (most common cause); persistent infection (most common cause); 2) 2) infection with viruses, mycobacteria, parasites infection with viruses, mycobacteria, parasites
and fungi; and fungi; 3) 3) autoimmune disease; autoimmune disease; 4) 4) foreign material; foreign material; 5) 5) some cancers.some cancers.

I. Subtype of chronic inflammationI. Subtype of chronic inflammation II. Characterized by granulomaII. Characterized by granuloma, which is a , which is a collection of collection of epithelioid epithelioid
histiocyteshistiocytes ((macrophages with abundant pink cytoplasmmacrophages with abundant pink cytoplasm), usually ), usually surrounded by surrounded by giant cellsgiant cells and a and a rim of lymphocytesrim of lymphocytes
III. Divided into noncaseating and caseating subtypesIII. Divided into noncaseating and caseating subtypes1. 1. Noncaseating granulomasNoncaseating granulomas lack central necrosis.lack central necrosis. Common etiologies includeCommon etiologies include reaction to foreign material, sarcoidosis, reaction to foreign material, sarcoidosis,
beryllium exposure, Crohn disease, and cat scratch disease,beryllium exposure, Crohn disease, and cat scratch disease,2. 2. Caseating granulomas Caseating granulomas exhibit central necrosis and are exhibit central necrosis and are
characteristic of tuberculosis and fungal infections,characteristic of tuberculosis and fungal infections, IV. Steps involved in granuloma formationIV. Steps involved in granuloma formation 1. 1. MacrophagesMacrophages process and present antigen via MHC class II to process and present antigen via MHC class II to
CD4 helper T cells.CD4 helper T cells.2. Interaction leads macrophages to secrete IL-12, inducing CD4
helper T cells to differentiate intoTh1 subtype.3. Th1 cells secrete IFN-γ, which converts macrophages to
epithelioid histiocytes and giant cells.

FEATURE ACUTE INFLAMMATION CHRONIC INFLAMMATION
Pathogenesis Microbial pathogens, trauma, burns
Persistent acute inflammation, foreign bodies (e.g., silicone, glass), autoimmune disease, certain types of infection (e.g., tuberculosis, leprosy)
Primary cells involved NeutrophilsMonocytes/macrophages (key cells), B and T lymphocytes, plasma cells, fibroblasts
Primary mediatorsHistamine (key mediator), prostaglandins, leukotrienes
Cytokines (e,g., IL-1), growth factors
Necrosis Present Less prominentScar tissue Absent Present
Onset Immediate Delayed
Duration Few days Weeks, months, years
OutcomeComplete resolution, progression to chronic inflammation, abscess formation
Scar tissue formation, disability, amyloidosis
Main immunoglobulin IgM IgG
Serum protein electrophoresis effect
Mild hypoalbuminemiaPolyclonal gammopathy; greater degree of hypoalbuminemia
Peripheral blood leukocyte response
Neutrophilic leukocytosis Monocytosis

• Inflammation came on changing of sepsis which is a Inflammation came on changing of sepsis which is a general process;general process;
• development of necrosis of tissue during development of necrosis of tissue during alterationalteration promote stopping of blood stream and result in promote stopping of blood stream and result in limitation of infection spreadinglimitation of infection spreading;;
• ExudationExudation::– dilution of toxins;dilution of toxins;– proteins absorb the toxins;proteins absorb the toxins;– phagocytosis;phagocytosis;– limitationlimitation of toxins matters and mediators of toxins matters and mediators spreadingspreading
in an organism. in an organism. • ProliferationProliferation the regeneration of organ or tissue, the regeneration of organ or tissue,
recover of structure and function take place.recover of structure and function take place.

Negative significance of inflammation:
• alteration is the injury → dysfunction of organs;
• exudate results in compression of arterial, venous and lymphatic vessels → hypoxia;
• the fibroplasia results in the organ dysfunction.

Literature• Copstead Lee-Ellen C. Pathophysiology / Lee-Ellen C. Copstead, Jacquelyn L.
Banasic // Elsevier Inc. – 2010. • Robbins and Cotran Pathologic Basis of Disease 8th edition./ Kumar, Abbas,
Fauto. – 2007. – Chapter 2 – 3. • Pathophysiology, Concepts of Altered Health States, Carol Mattson Porth,
Glenn Matfin.– New York, Milwaukee. – 2009. • Essentials of Pathophysiology: Concepts of Altered Health States (Lippincott
Williams & Wilkins), Trade paperback (2003) / Carol Mattson Porth, Kathryn J. Gaspard. Chapters 9
• General and clinical pathophysiology. Edited by prof. A.V. Kubyskin. Simferopol. – 2011.
• Symeonova N.K. Pathophysiology / N.K. Symeonova // Kyiv, AUS medicine Publishing. – 2010.
• Gozhenko A.I. General and clinical pathophysiology / A.I. Gozhenko, I.P. Gurcalova // Study guide for medical students and practitioners. Edited by prof. Zaporozan, OSMU. – Odessa. – 2005.