Embed Size (px)
Citation preview

INVASION & METASTASISINVASION & METASTASIS
Dr.CSBR.Prasad, M.D.,Sri Devaraj Urs Medical College
Kolar-563101Karnataka
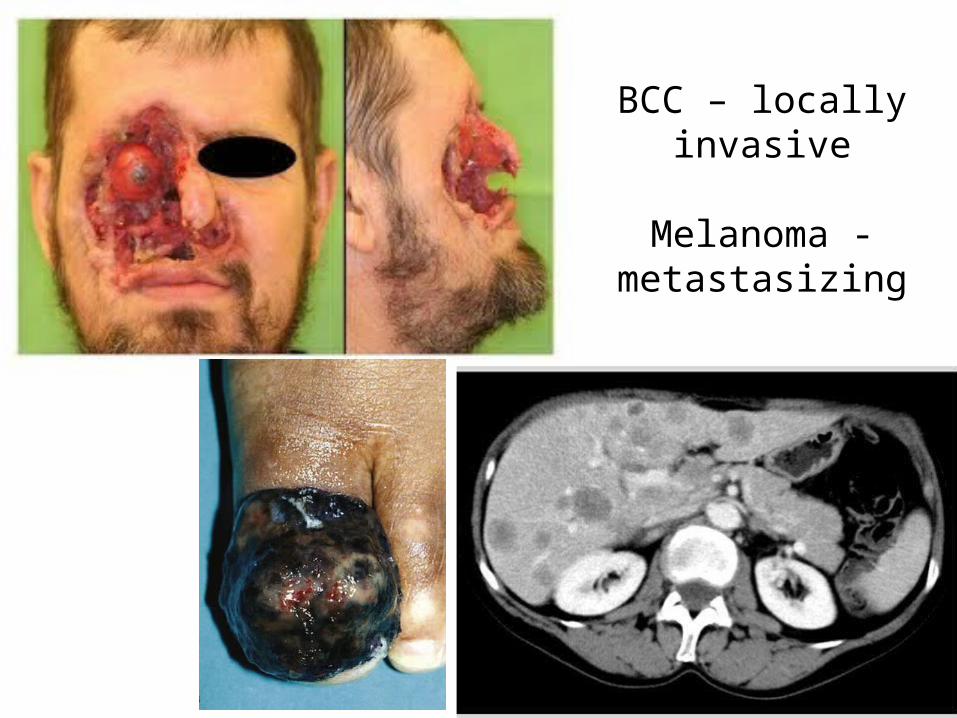
BCC – locally invasive
Melanoma - metastasizing
Invasion and metastasis are biologic Invasion and metastasis are biologic hallmarks of malignant tumorshallmarks of malignant tumors
• For tumor cells to break loose from a primary mass, enter blood vessels or lymphatics and produce a secondary growth at a distant site
• For this, they must go through a series of steps (the metastatic cascade)
The metastatic cascade is divided into two phases: 1. Invasion of the extracellular matrix (ECM)2. Vascular dissemination, homing of tumor cells,
and colonization

Metastasis
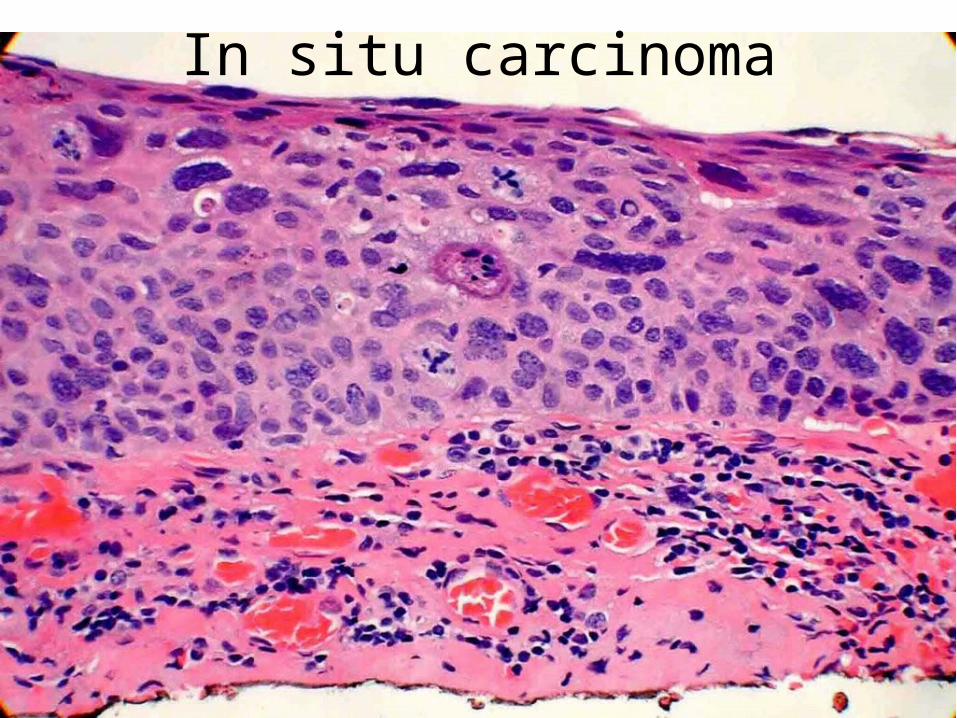
In situ carcinoma
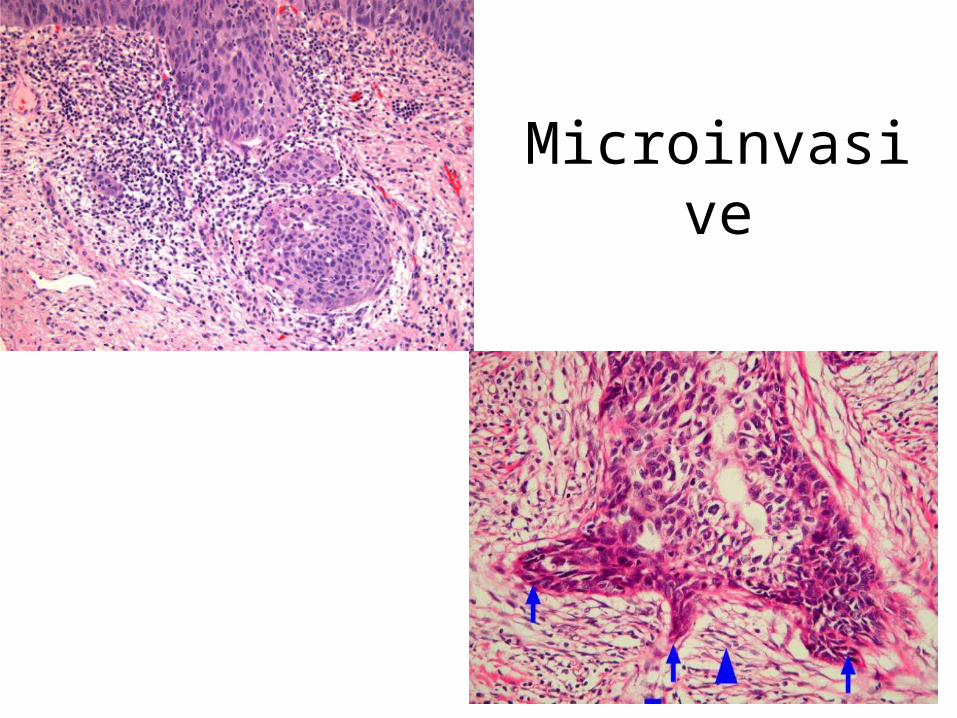
Microinvasive
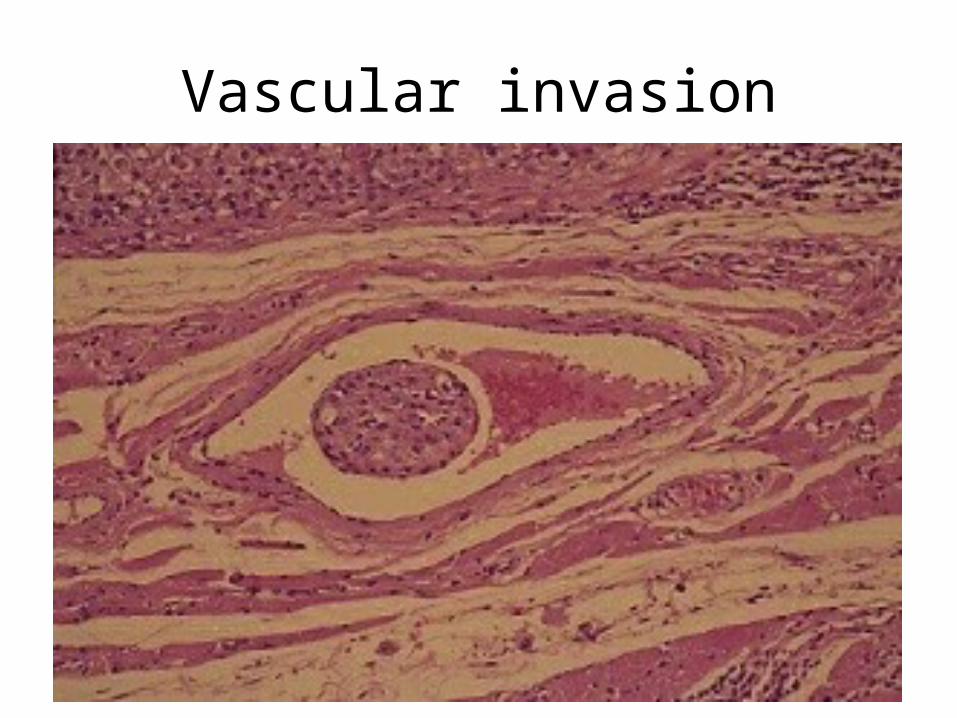
Vascular invasion
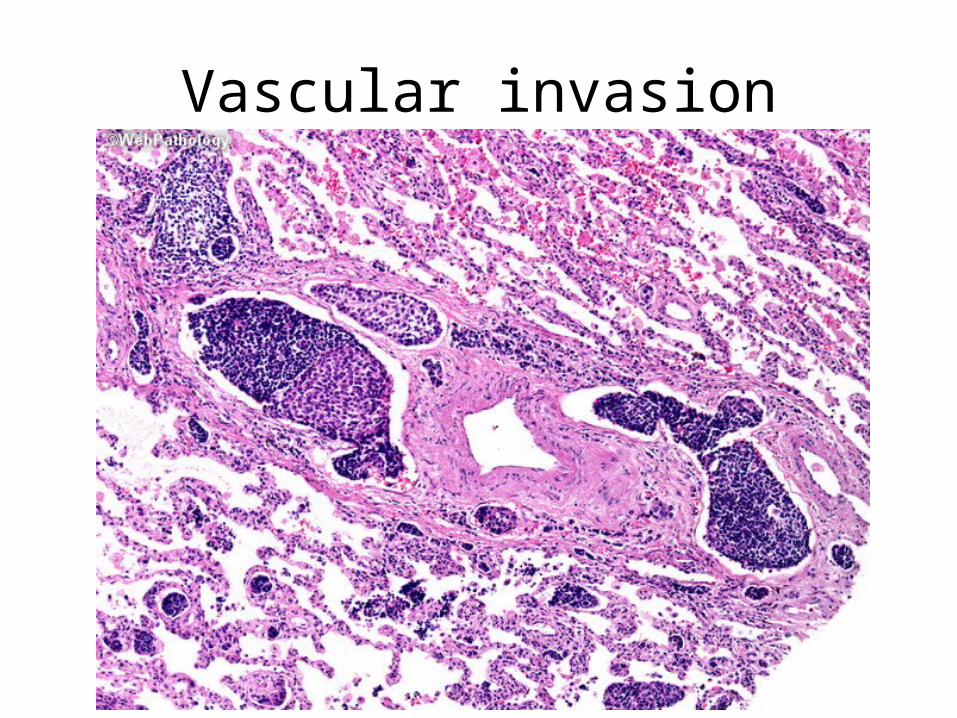
Vascular invasion
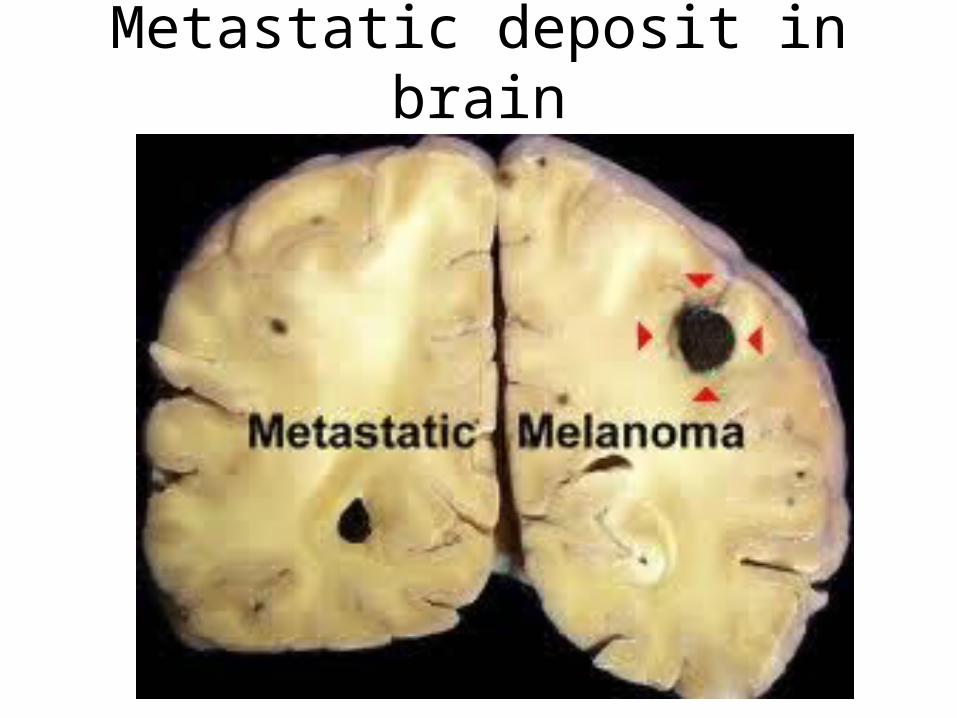
Metastatic deposit in brain
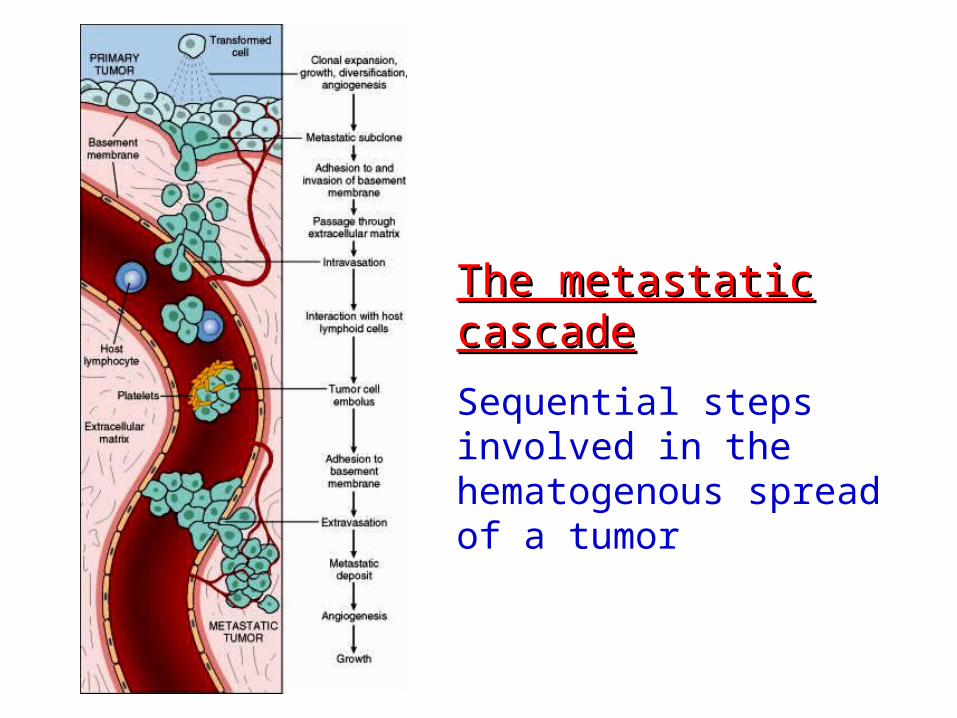
The metastatic cascadeThe metastatic cascade
Sequential steps involved in the hematogenous spread of a tumor
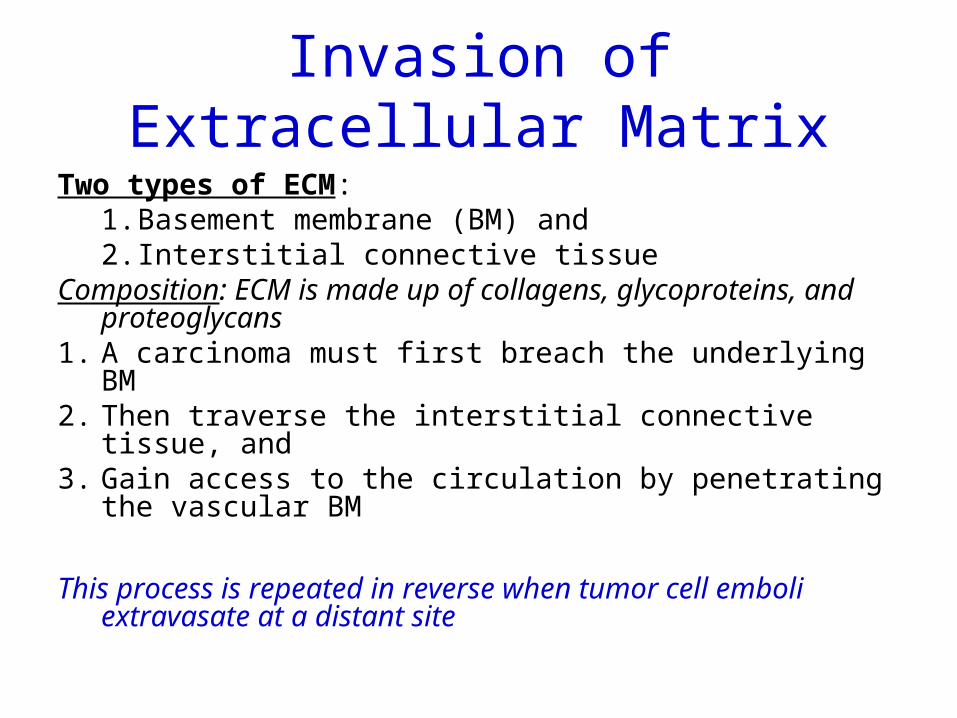
Invasion of Extracellular MatrixTwo types of ECM:
1. Basement membrane (BM) and 2. Interstitial connective tissue
Composition: ECM is made up of collagens, glycoproteins, and proteoglycans
1. A carcinoma must first breach the underlying BM2. Then traverse the interstitial connective tissue, and 3. Gain access to the circulation by penetrating the
vascular BM
This process is repeated in reverse when tumor cell emboli extravasate at a distant site
Invasion of Extracellular Matrix
Invasion of the ECM initiates the metastatic cascade:
1. Changes (“loosening up”) of tumor cell-cell interactions
2. Degradation of ECM 3. Attachment to novel ECM components 4. Migration of tumor cells
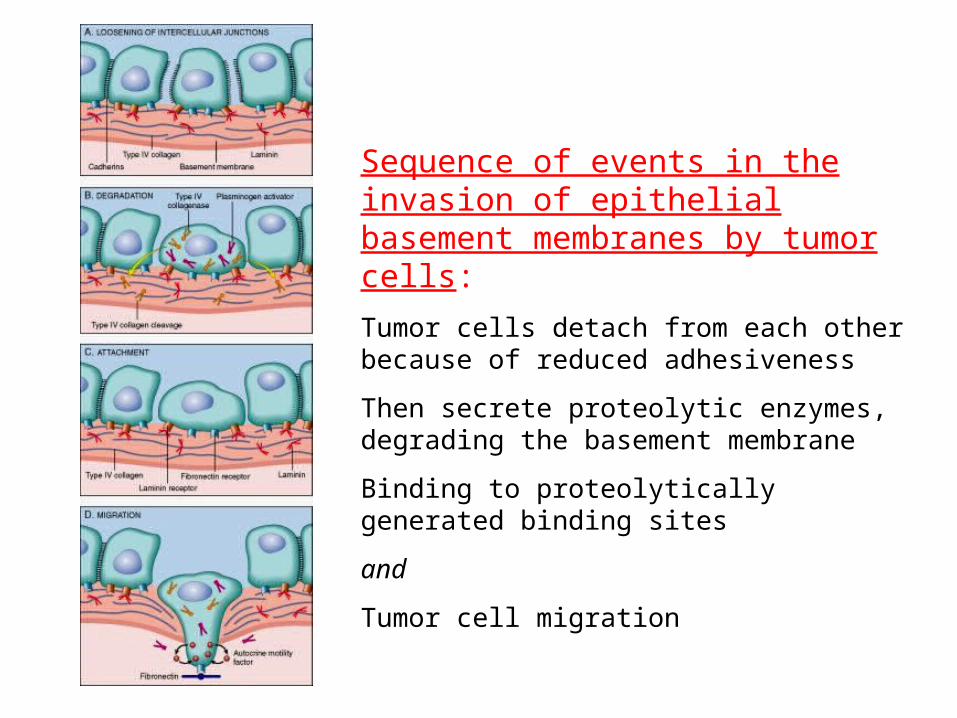
Sequence of events in the invasion of epithelial basement membranes by tumor cells: Tumor cells detach from each other because of reduced adhesiveness
Then secrete proteolytic enzymes, degrading the basement membrane
Binding to proteolytically generated binding sites
and
Tumor cell migration
Invasion of Extracellular Matrix
Invasion of the ECM initiates the metastatic cascade and is an active process that can be resolved into several steps
1. Changes (“loosening up”) of tumor cell-cell interactions
2. Degradation of ECM 3. Attachment to novel ECM components 4. Migration of tumor cells
1-Dissociation of cells from one another(“loosening up”) of tumor cell-cell interactions
As a result of alterations in intercellular adhesion molecules
Normal cells are bound together by adhesion molecules
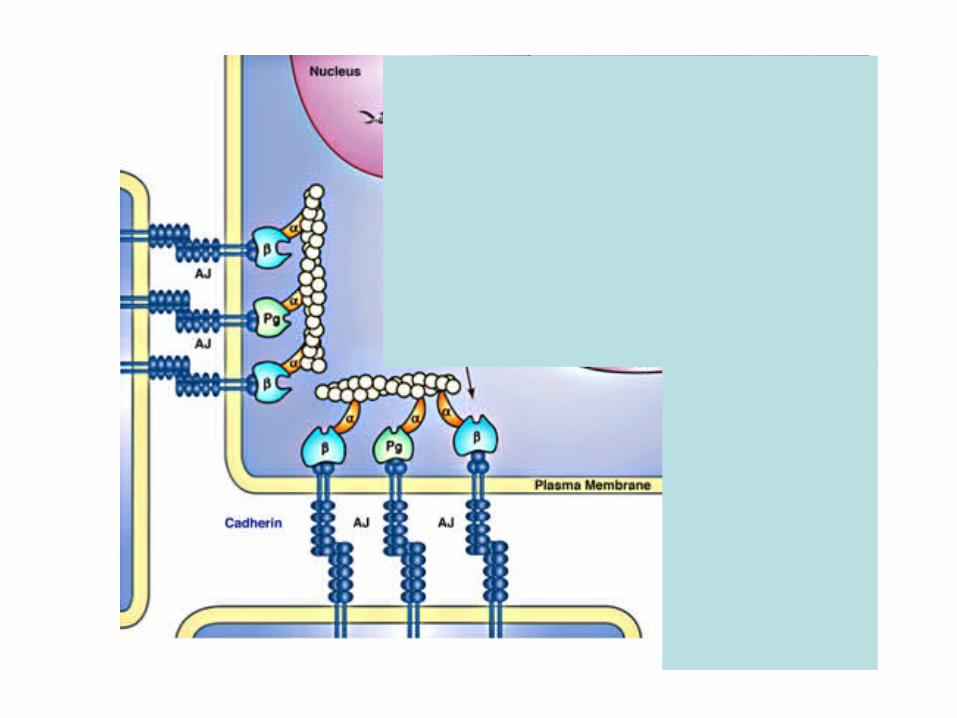
• Cell-cell interactions are mediated by the cadherin family of transmembrane glycoproteins
• Intracellularly the E-cadherins are connected to β-catenin and the actin cytoskeleton
Tumors with down-regulated E-cadherin expression
Seen in several epithelial tumors, including adenocarcinomas of the colon and breast
• This down-regulation reduces the ability of cells to adhere to each other and facilitates their detachment from the primary tumor
• The normal function of E-cadherin is dependent on its linkage to catenins
• In some tumors E-cadherin is normal, but its expression is reduced because of mutations in the gene for α catenin
Invasion of Extracellular Matrix
Invasion of the ECM initiates the metastatic cascade and is an active process that can be resolved into several steps
1. Changes (“loosening up”) of tumor cell-cell interactions
2. Degradation of ECM 3. Attachment to novel ECM components 4. Migration of tumor cells
2-Local degradation of the basement membrane and interstitial connective tissue
Elaboration of proteases by– Tumor cells themselves or– Stromal cells [induced by tumor cells]
Many different families of proteases– Matrix metalloproteinases (MMPs) – Cathepsin D & – Urokinase plasminogen activator
MMPsTumors either elaborate large quantities of MMPs or they
may reduce the concentrations of MMP-inhibitors
They regulate tumor invasion by:• Dissolving components of the BM & interstitial matrix • Releasing ECM-sequestered growth factors
– Cleavage products of collagen and proteoglycans also have chemotactic, angiogenic, and growth-promoting effects
• Eg: MMP9 is a gelatinase that cleaves type IV collagen of the epithelial and vascular basement membrane and also stimulates release of VEGF from ECM-sequestered pools
Eg: Benign tumors of the breast, colon, and stomach show little type IV collagenase activity, whereas their malignant counterparts overexpress this enzyme
Invasion of Extracellular Matrix
Invasion of the ECM initiates the metastatic cascade and is an active process that can be resolved into several steps
1. Changes (“loosening up”) of tumor cell-cell interactions
2. Degradation of ECM 3. Attachment to novel ECM components 4. Migration of tumor cells
3 - Attachment to novel ECM components
• Normal epithelial cells have receptors, such as integrins, for basement membrane laminin and collagens that are polarized at their basal surface– These receptors help to maintain the cells in a resting,
differentiated state• Loss of adhesion in normal cells leads to induction of
apoptosis [tumor cells are resistant to this form of cell death]
• The matrix itself is modified in ways that promote invasion and metastasis– Eg: cleavage of the basement membrane proteins collagen IV
and laminin by MMP2 or MMP9 generates novel sites that bind to receptors on tumor cells and stimulate migration
Invasion of Extracellular Matrix
Invasion of the ECM initiates the metastatic cascade and is an active process that can be resolved into several steps
1. Changes (“loosening up”) of tumor cell-cell interactions
2. Degradation of ECM 3. Attachment to novel ECM components 4. Migration of tumor cells
4 – Migration of tumor cells - Locomotion
• Tumor cells propel themselves through the degraded basement membranes and zones of matrix proteolysis
• It involves many families of receptors and signaling proteins that eventually impinge on the actin cytoskeleton– Cells must attach to the matrix at the leading edge, detach from the
matrix at the trailing edge, and contract the actin cytoskeleton to ratchet forward - Ameboid migration
• Such movement are potentiated by tumor cell–derived cytokines– Cleavage products of matrix components (e.g., collagen, laminin) and
some growth factors (e.g., IGFs I and II) have chemotactic activity for tumor cells
• Stromal cells also produce paracrine effectors of cell motility– HGF–scatter factor, which bind to receptors on tumor cells– HGF–scatter factor is elevated at the advancing edges of the highly
invasive brain tumor glioblastoma multiforme
Ameboid migration• In this type of migration the cell squeezes
through spaces in the matrix instead of cutting its way through it
• This ameboid migration is much quicker• Tumor cells are capable of switching
between the two forms of migration, perhaps explaining the disappointing performance of MMP inhibitors in clinical trials
Molecular Genetics of Metastasis Development
Malignant tumors have varied metastatic potential
Cancer with Low metastatic potential– Basal cell carcinoma
Cancer with high malignant potential– Malignant melanoma
•Why this variation?•What genetic changes bring about metastatic potential?
Several THEORIES have been proposed to explain how the metastatic phenotype arises?
1. The clonal evolution model– As mutations accumulate in cancer cells, the tumor become
heterogeneous
2. Metastasis is the result of multiple abnormalities that occur in most of the cells in a primary tumor– “Metastasis signature”
• It may involve the cancer cells or in the microenvironment
3. Background genetic variation in gene expression contributes to the generation of metastases
4. Tumors derive from rare tumor stem cells, metastases require the spread of the tumor stem cells themselves
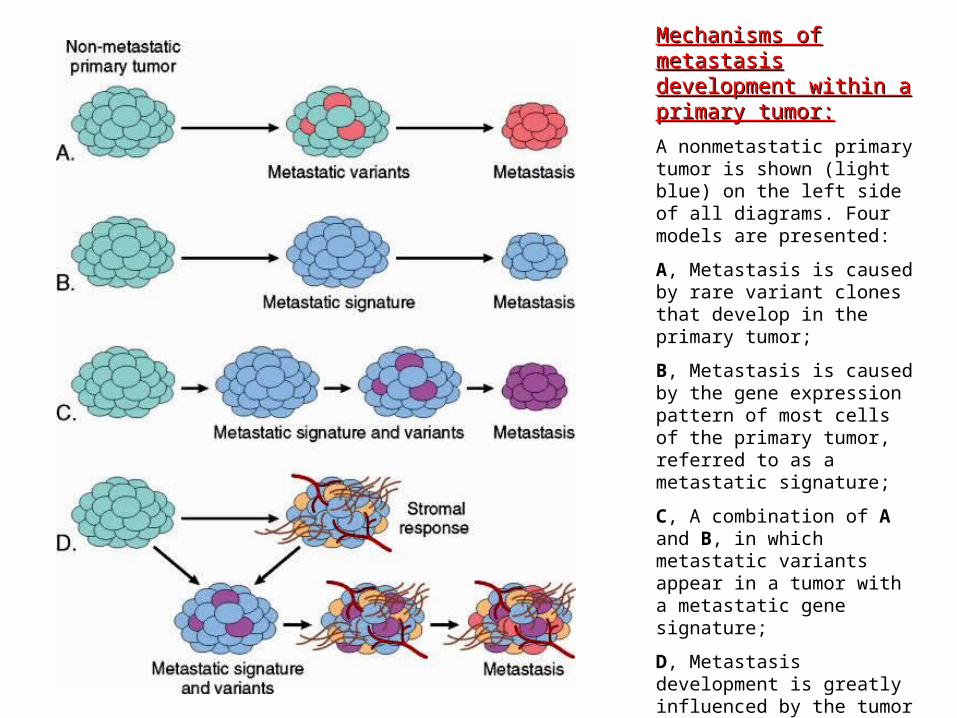
Mechanisms of metastasis Mechanisms of metastasis development within a development within a primary tumor:primary tumor:
A nonmetastatic primary tumor is shown (light blue) on the left side of all diagrams. Four models are presented:
A, Metastasis is caused by rare variant clones that develop in the primary tumor;
B, Metastasis is caused by the gene expression pattern of most cells of the primary tumor, referred to as a metastatic signature;
C, A combination of A and B, in which metastatic variants appear in a tumor with a metastatic gene signature;
D, Metastasis development is greatly influenced by the tumor stroma, which may regulate angiogenesis, local invasiveness, and resistance to immune elimination, allowing cells of the primary tumor, as in C, to become metastatic.
Are there genes whose principal or sole contribution to tumorigenesis is to control
metastasis?
• Genes that function as “metastasis oncogenes” or “metastatic suppressors” are rare
• At least a dozen genes lost in metastatic lesions have been confirmed to function as “metastasis suppressors”
• Their molecular functions are varied and not yet completely clear; however, most appear to affect various signaling pathways
• Recent work has suggested that two miRNAs, mir335 and mir126, suppress the metastasis of breast cancer, while a second set (mir10b) promotes metastasis
Metastasis oncogenes• Genes: SNAIL and TWIST• Their primary function: is to promote epithelial-
to-mesenchymal transition (EMT)In EMT:• Some epithelial markers like E-cadherin is down
regulated and certain mesenchymal markers (e.g., vimentin and smooth muscle actin) are up-regulated – This favors the development of a promigratory
phenotype that is essential for metastasis
Modes of Spread
• Seeding the body cavities– The cavity most often involved is peritoneal cavity
(Krukenberg tumor, pseudomyxoma peritonei)• Lymphatic spread
– Most carcinomas– Deposits will be in the regional or distant nodes
• Hematogenous (through blood stream)– most sarcomas and some carcinomas
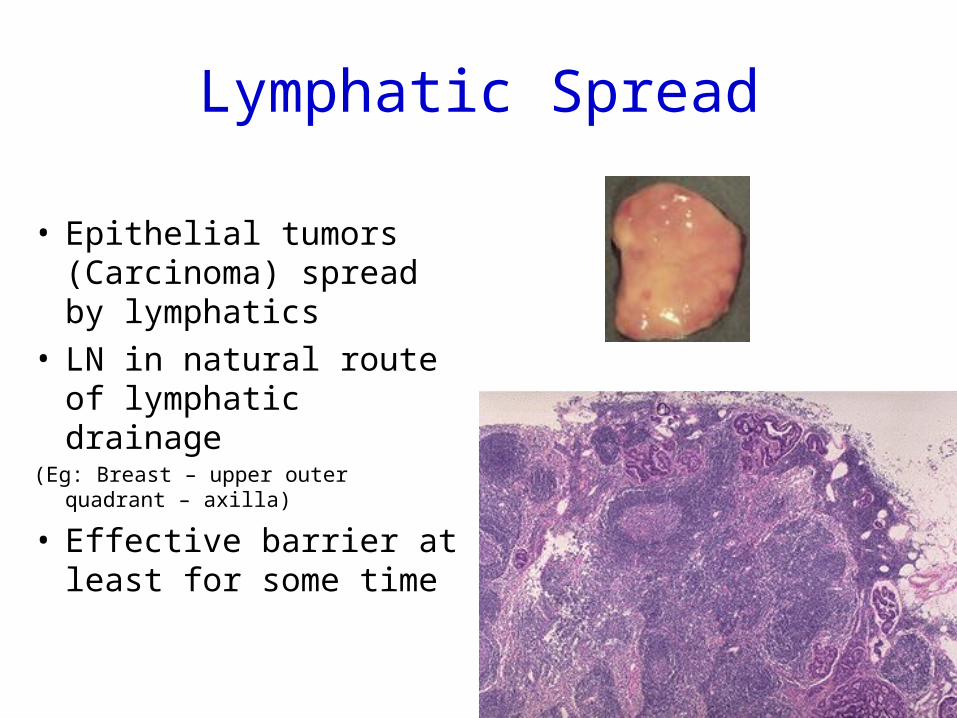
Lymphatic Spread
• Epithelial tumors (Carcinoma) spread by lymphatics
• LN in natural route of lymphatic drainage
(Eg: Breast – upper outer quadrant – axilla)
• Effective barrier at least for some time
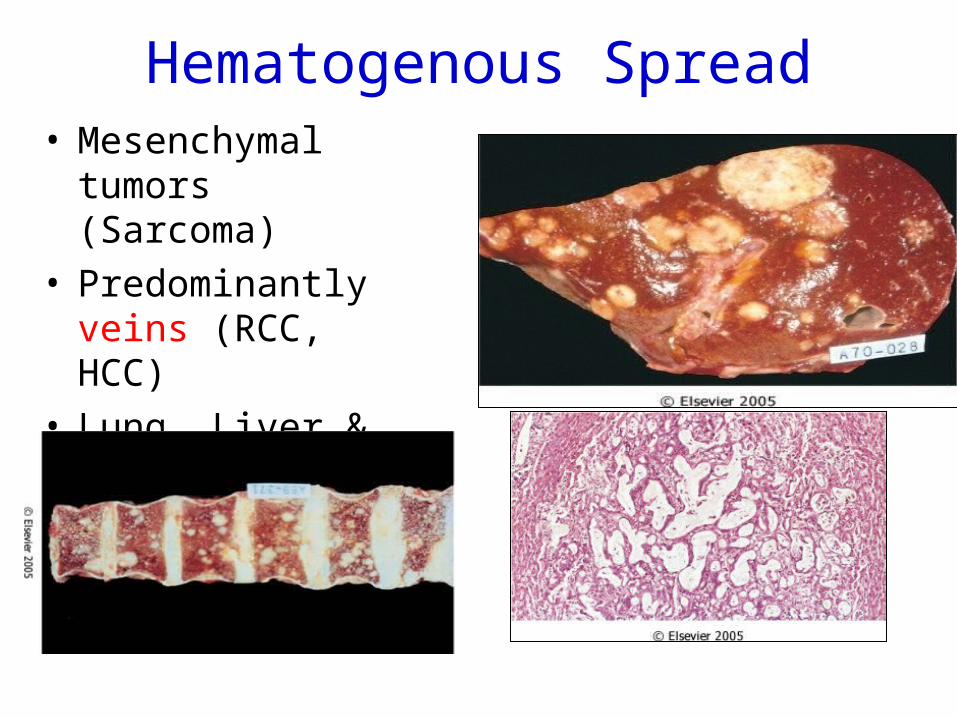
Hematogenous Spread• Mesenchymal
tumors (Sarcoma)• Predominantly veins
(RCC, HCC)• Lung, Liver &
Vertebra
Common sites of metastatic deposits (hematogenous spread)
• Liver
• Bones
• CNS
• Lung
Some tumors prefer certain sites
• Adrenals prefered by Bronchogenic.ca (Lung carcinoma)
• Bone metasizing tumors:– BK.Patil
• Liver & bone by Neuroblastoma
Rare sites for mets
• Skeletal muscle• Spleen• Pancreas
Other mechanisms of spread
• Direct extension
• Surgical or procedural transplantation (iatrogenic)
Unusual modes of spread
• Carcinomas arising close to vertebral column spread via paravertebral venous plexus giving rise to early bone metastasis
• Renal cell carcinoma grows inside renal vein in a snake like fashion
• Carcinoma of lung gives rise to metastatic deposit in adrenals very frequently
E N D