Embed Size (px)
Citation preview

‘Effect of anti-hypertensive drugs and other modifiable factors on systolic blood pressure (SBP) in elderly population: a study
from a tertiary care hospital in Delhi’
CO-SUPERVISORRazi AhmadMD,DCH Associate Professor PharmacologySupervisor of HAH Centenary Hospital Pharmacy, Jamia Hamdard, New Delhi
PRESENTED BY:NIKHIL SINGHM.PHARMPHARMACY PRACTICENIPER-H
SUPERVISORDr. Shridhar DwivediMD, PhD (Cardiology), FAMS,FRCP (London), FIACS,Dean and Principal of HIMSR & HAH Centenary HospitalJamia Hamdard, New Delhi

Flow of Seminar• Introduction
• Complications of Hypertension
• Aim & Objective
• Methodology
• Inclusion Criteria & Exclusion Criteria
• Results
• Conclusion

INTRODUCTION• Hypertension (HTN) or high blood pressure, sometimes called arterial hypertension, is
a chronic medical condition in which the blood pressure in the arteries is elevated.
• In elderly population, systolic hypertension is the commonest form of hypertension
and it is a better predictor of cardiovascular events, end-stage renal disease , as
compared to diastolic blood pressure.
• Isolated systolic hypertension is more often seen in the elderly than in the young.
• Population older than 50 years, systolic blood pressure (SBP) over 140 mm Hg is an
important risk factor for stroke and heart disease.
• Most cases of uncontrolled hypertension in the United States are due to systolic
hypertension among elder.
• Therefore, prevention and treatment of systolic hypertension (SBP) may be helpful in
the growing epidemic of kidney & heart dysfunction among elderly persons.

COMPLICATIONS OF HYPERTENSION

AIM & OBJECTIVESAIM:
The overall aim is to evaluate the effect of anti-hypertensive drugs on systolic blood
pressure (SBP) in elderly population. More specifically, the following objectives will be
achieved:
Objectives:
1) To study the effect of antihypertensive drugs on systolic blood pressure (SBP) in
elderly patients (≥50 years men and in ≥45 years females, menopausal).
2) To find out relation between various factors (smoking/red meat/junk food) and systolic
blood pressure (SBP) in elderly population.
3) To analyze the effect of Visceral Adiposity Index on systolic blood pressure (SBP) in
elderly patients.

Methodology
Type: It is the prospective study of the elderly patients with hypertension.
Site: The study was conducted at Hakeem Abdul Hameed Centenary Hospital, Jamia Hamdard , New Delhi – 110062, India.
Study population: 220 patients with their follow-up
Duration of study: 11 months
Source of data: Patients registered in OPD/IPD & ICU
Follow up have taken after every 1 to 2 month

Inclusion Criteria
Elderly patients (male ≥50 yr. and female ≥ 45yr. , Post Menopausal)
Patients with > 140/90 mm of Hg
All menopausal female with BP > 140/90 mm of Hg
Systolic blood pressure >140 mm of Hg

Exclusion Criteria
Patient with age of Male < 50 yrs. and female < 45yrs (or non-menopausal)
Patients with ≤ 140/90 mm of Hg
Patients with other chronic diseases ( Except T2DM)

Results
• Out of total 230 patients enrolled, 220 (96%) were followed and completed study (9 were left and 1 died).
Gender wise Distribution of Patients
Gender Frequency Percentage (%)
MALE 108 49%
FEMALE 112 51%
TOTAL 220 100%

MALE; 108; 49%
FEMALE; 112; 51%
The study includes more female patients as compared to male patients. A total of 51% patients were female while 49% patients were male. There is significant correlation between gender and SBP (P˂0.05).
Gender wise distribution of patients

(Years) 45-55 55-65 65-75 75-85 85-950
20
40
60
80
100
120
45-55; 73
55-65; 98
65-75; 37
75-85; 1285-95; 1
Age wise distribution of patients
There is significant correlation between age and SBP (P<0.05)

Socioeconomic Status (modified kuppuswamy scale 2014)
IV III II0
20
40
60
80
100
120
14056%
30%
14%
The study reveals that 123 (56%) patients belongs to IV socioeconomic status patients followed by 66 (30%) to III socioeconomic status patients. There is negative correlation between Socioeconomic Status and SBP (P<0.05).

Religion wise distribution
HINDU MUSLIM CHRISTIAN 0
20
40
60
80
100
120
140
160
180 HINDU , 157, 72%
MUSLIM , 60, 27%
CHRISTIAN , 2, 0.09%
The maximum number of patients belongs to Hindu group, 157 patients (72%) of total population followed by Muslim group, 60 patients (27%) of total population. There is negative correlation between religion and SBP (P<0.05).

Education
This study reveals that illiterate patients are more hypertensive as compare literate patients. There is negative correlation between SBP and education (P<0.05)
Illiterates 10th 12th Graduate & above
Total 0
50
100
150
200
250
85
3667
29
220
LITRACY
PATI
ENTS

OBESITY
The study depicts that obese patients (134) were more hypertensive as compared to non-obese patients (86). Among the 134 obese patients female patients were 88(65.67%) and male patients were 46 (34.32%) There is significant relation between obesity and SBP (P<0.05).
Male Female Total 0
20406080
100120140160
46
88
134
62
24
86
Obese Patients Linear (Obese Patients )Non-obese Patients
GENDER
PATI
ENTS

Tobacco user
The study documented that among the 220, hypertensive patients, 40.90% (90) patients were tobacco. The habits of tobacco were seeing more in male patients (31.36%) as compared to female patients (9.54%). There is positive correlation between tobacco and SBP (P<0.05).
Smokers user (%) Non-smoker0
20
40
60
80
100
120
140
69
39
21
9190
130
Male Female Total
GENDER
NO
. OF
PATI
ENTS

Non-vegetarians
Male Female Total0
20406080
100120140
14 1024
7256
128
Non-veg eater (n=152) Non-red meat (n1) Non-veg eater (n=152) Red meat (n2)
Axis Title
Axi
s Titl
e
In this study 152 (69.09%) patients were non-veg eater out of 220 elevated systolic blood pressure patients and among the non-veg eater 128 (58.18%) were red meat eater while only 24 (10.90%) non-red meat eater. The occurrence of male patients (39.09%) was found comparatively higher than female patients (30%). There is significant correlation was found between non-veg eater and SBP (P<0.05).

Junk Food Eater
Male Female Total 0
50
100
150
200
250
108 112
220
100 90
190
822 30
Total no Junk food Non-junk food eater
GENDER
PATI
ENTS
The study leads to conclude that out of 220 hypertensive patients, 190 (86.36%) patients were junk food eater and 30 (13.63%) patients were non-junk food eater. The habit of junk food eating was more in male patients 100(45 %%) as compared to female patients, 90 (40.90%). There is positive correlation between junk food eater and SBP (P<0.05).

Type-II Diabetes Mellitus
Male Female Total 0
20
40
60
80
100
2541
66
36
58
94
T2DM Non- T2DM
Axis Title
Axi
s Ti
tle
This study leads the conclusion that only 66 (30%) patients were having T2DM out of 220 hypertensive patients and among the T2DM patients female patients were more 41(18.63%) as compared to male patients 25(11.36%)There is no significant correlation between T2DM and SBP (P> 0.05).

MONO DRUG THERAPY
TELMISARTAN (4
0Mg)
RAMIPRIL
(5Mg)
AMLODIPIN
E(5Mg)
METOPROLOL (50Mg)
CARVEDILOL(3.125Mg)
CHLORTHALIDONE (1
2.5 Mg)
INDAPAM
IDE ( 2
.5 Mg)
SPIRONLACTONE (5
0Mg)
ATENOLOL (50Mg)
0.00%
5.00%
10.00%
15.00%
20.00%
25.00% 21.61%19.37%
17.15%15.01%
12.50% 11.76%
6.66%2.75%
0.09%
DRUGS
RED
UC
TIO
N IN
SB
P
This study reveals that among the single drug therapy telmisartan (40mg) shows 21.61% reduction in systolic blood pressure followed by ramipril (5mg) shows 19.3% reduction, amlodipine (5mg) shows 17.15% reduction, metoprolol (50mg) shows 15.01% reduction & carvedilol (3.125mg) shows 12.5% reduction.

TWO DRUG THERAPY
0.00%
10.00%
20.00%
30.00% 27.21% 26.70% 24.57%19.03% 18.72%
DRUGS
RED
UC
TIO
N IN
SB
P
This study reveals that among the dual drug therapy α1 & β1 blocker + diuretic shows 27.21% reduction in systolic blood pressure followed by CCB+ diuretics shows 26.7% reduction, CCB+ β1 blocker shows 24.57%reduction, ARBS + CCB shows 19.03% reduction & thiazide + ARBS shows 18.72%reduction.

TRIPLE DRUG THERAPIES
0.00%
10.00%
20.00%
30.00% 23.91% 21.60%14.44% 13.88%
2.85%
DRUGS
% R
ED
UC
TIO
N IN
SB
P
This study depicted that among the triple drug therapy CCB+ β1 blocker + ARBs shows 23.91% reduction in systolic blood pressure followed by CCB+ ACEI+ diuretic shows 21.60%reduction, ARBs + Diuretic + CCB shows 14.44% reduction and diuretic +diuretic + α1 & β1 blocker shows 13.88%reduction

FOUR DRUGS THERAPY
% REDUCTION IN SBP0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%11.54%
DRUGS
% R
ED
UC
TIO
N IN
SB
P
This study reveals that the four drugs therapy ACEI+ CCB+ diuretics + β1 blocker shows 11.54% reduction in systolic blood pressure.
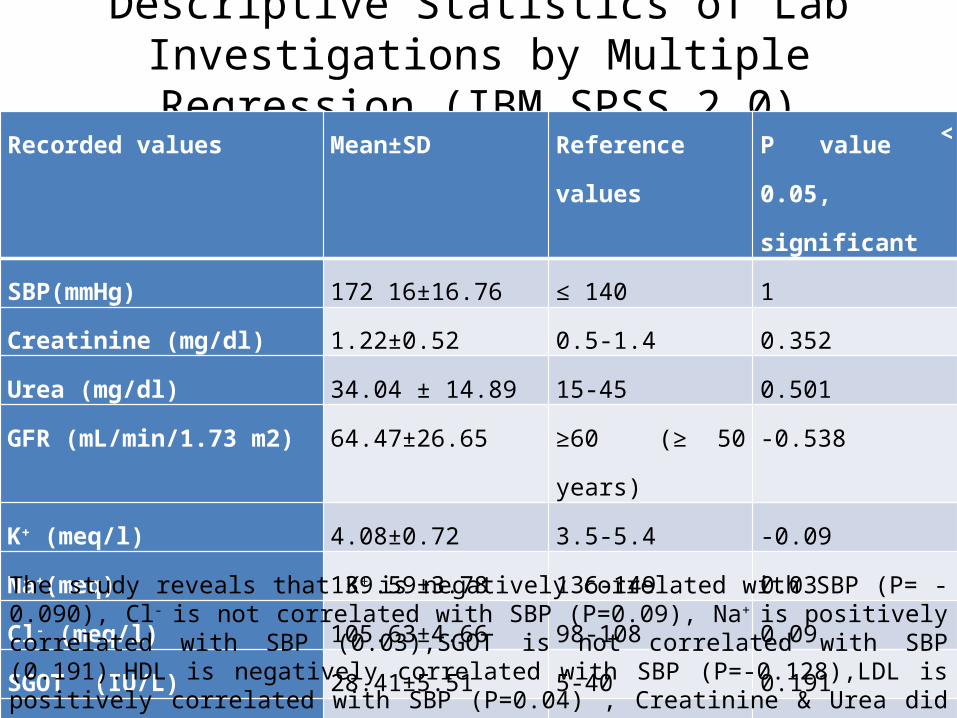
Descriptive Statistics of Lab Investigations by Multiple Regression (IBM SPSS 2.0)
Recorded values Mean±SD Reference values P value ˂ 0.05,
significant
SBP(mmHg) 172 16±16.76 ≤ 140 1
Creatinine (mg/dl) 1.22±0.52 0.5-1.4 0.352
Urea (mg/dl) 34.04 ± 14.89 15-45 0.501
GFR (mL/min/1.73 m2) 64.47±26.65 ≥60 (≥ 50 years) -0.538
K+ (meq/l) 4.08±0.72 3.5-5.4 -0.09
Na+(meq) 139.59±3.78 136-149 0.03
Cl- (meq/l) 105.63±4.66 98-108 0.09
SGOT (IU/L) 28.41±5.51 5-40 0.191
LDL (mg/dl) 86.34±20.74 150-190 0.04
HDL (mg/dl) 53.06±20.74 30-70 -0.128The study reveals that K+ is negatively correlated with SBP (P= -0.090), Cl- is not correlated with SBP (P=0.09), Na+ is positively correlated with SBP (0.03),SGOT is not correlated with SBP (0.191).HDL is negatively correlated with SBP (P=-0.128),LDL is positively correlated with SBP (P=0.04) , Creatinine & Urea did not show significant correlation, GFR is negatively correlated with SBP, C-RP is positively correlated with SBP.

CONCLUSION• This study concluded that prevalence of elevated SBP is highest in the age group of 55-65
years among elderly patients.• This study also reveals that age, obesity, non-veg eater and junk food eaters are positively
correlated with elevated SBP, while socioeconomic status and education are negatively correlated with SBP.
• Tobacco showed significant correlation with elevated SBP and this habit was seen more in male patients as compared to female patients
• Waist circumference is positively correlated with elevated SBP although visceral adiposity index has no significant correlation with SBP.
• In pharmacological treatment of telmisartan as single drug therapy provides good control of SBP followed by ramipril and amlodipine but combination of two drugs carvedilol with thiazide diuretic or CCB with diuretics provides better control of systolic hypertension as compared to monotherapy in elderly population.
• Carvedilol did not show good control in elevated SBP as a single drug therapy but with diuretics (combination) showed better control in elevated SBP. In this study combination of carvedilol with thiazide were given to very few patients so further study on this combination needed. According to available evidence it is clearly depicted that carvedilol could be a valuable tool for the management of hypertension.
• In addition some previous studies are supporting our results whereas some are not, so considering the findings; this study opens the door for further research in this regard.