Embed Size (px)
Citation preview

Intravascular Ultrasonography (IVUS)
PROFESSOR F. RAHMANMBBS (Dhaka), MCPS (Med), D-Card (DU), MD (Card)
FACC (USA), Fellow-in Interventional Cardiology (USA)Professor (Interventional Cardiology)
Department of Cardiology, UCCBangabandhu Sheikh Mujib Medical University.

Introduction
• Intravascular ultrasonography is an invasive imaging procedure that provides intravascular images of the coronary arteries (and other blood vessels).
• IVUS has played a critical role in-– coronary atherosclerosis pathophysiology– diagnostic and therapeutic strategies for various
vascular pathologies. – integral role in the evolution of interventional
cardiology.

Indications
• IVUS in CAG:Arterial wall thicknessAtheroma detection, assessment & characterization.Calcium contentDissectionAneurysm assessmentIn-stent restenosis

Indications• IVUS in PCI :
To plan interventional strategy & to optimize stent deployment.
Find reference lumen dimensions and lesion length for appropriate stent sizing;
Identification of superficial calcium by IVUS can lead to pre-stent rotational atherectomy

IVUS in PCI :Assess thrombus burden (Operators may
alter anticoagulant therapies or consider mechanical thrombectomy).
Post-stent IVUS assessment may detect complications of PCI and suboptimal stent deployment.

Contraindications
• Intravascular ultrasonography in interventional cardiology is an adjunct procedure to coronary angiogram.
• As such, any contraindication to coronary angiography applies to intravascular ultrasonography as well.

IVUS Equipment

IVUS Equipment

IVUS Equipment

IVUS Equipment

Technical Considerations
• A miniature ultrasound-mounted catheter is connected to an electronics console
• An electrical current is passed through the piezoelectric (pressure-electric) crystalline material of the transducer that expands and contracts when electrically excited.

Technical Considerations
• After reflection from tissue, part of the ultrasound energy returns to the transducer.
• The received signal is converted to electrical energy and sent to an external signal processing system for amplification, filtering, scan conversion, user-controlled modification, and graphic presentation.

Technical Considerations• The ultrasound beam upon reflection remains fairly
parallel for a distance (near field) and then begins to diverge (far field).
• The quality of ultrasound images is greater in the near field because the beam is narrower and more parallel.
• Therefore, larger transducers with lower frequencies are used for examination of large vessels because they create a deeper near field.

IVUS Technique• Prepare IVUS catheter Flush with saline Position imaging catheter across lesion Place distal marker minimum 3 cm beyond the
region of interest Set gain and field of view Image acquisition
Manual Automated pull back

IVUS Technique


Normal Arterial Wall
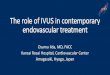
Normal anatomy by IVUS. In magnified image (right), thin intimal leading edge is highlighted by arrows.

Normal Arterial Wall

Normal Arterial Appearance
• A standard intravascular ultrasound image consists of three main components: catheter, lumen, and arterial wall.
• An ultrasound reflection is generated at a tissue interface if an abrupt change in acoustic impedance occurs.

Normal Arterial Appearance• In the normal artery, two such interfaces are usually
observed: I. One at the border between blood and the leading edge of the
intimaII. Second at the external elastic membrane, which is located at the
media-adventitia border. • In patients under 40 years of age, the reported normal value
for intimal thickness is typically between 0.15 mm and 0.25 mm.
• Most investigators use 0.25 to 0.50 mm as the upper limit of normal.

Quantitative Measurements
• Border identification• Lumen measurements

Border Identification
• Recognizing that all ultrasound techniques, including intravascular ultrasonography, require measurements to be performed at the leading edge of boundaries, never the trailing edge, is important.
• In muscular arteries such as the coronary arteries, frequently three layers exist.

Border identification1. The innermost layer consists of a complex of intima and internal
elastic membrane. I. This innermost layer is relatively echogenic compared with the
lumen and media. II. The trailing edge of the intima (which would correspond to the internal
elasticmembrane) cannot always be distinguished clearly.
2. Moving outward from the lumen, the second layer is the media.
3. The third and outer layer consists of the adventitia and periadventitial tissues. The boundary separating the true adventitia from surrounding perivascular tissues is less well defined on intravascular ultrasonography images.

Lumen Measurements
Lumen measurements are performed using the interface between the lumen and the leading edge of the intima.
Generally, the leading edge of the innermost echogenic layer should be used as the lumen boundary.
The following basic measurements can be recorded depending upon the operator’s preference

Lumen Measurements
• Lumen cross sectional area (CSA): The area bounded by the luminal border Minimum lumen diameter: The shortest diameter through the center
point of the lumen Maximum lumen diameter: The longest diameter through the center
point of the lumen Lumen eccentricity: 1 [(Maximum lumen diameter – minimum lumen
diameter)/maximum lumen diameter] Lumen area stenosis: (Reference lumen CSA – minimum lumen
CSA)/reference lumen CSA

Special Measurements• Further special measurements facilitated by
intravascular ultrasonography are as follows:External elastic membrane measurements Atheroma measurements Calcium measurements Stent measurements (a post deployment minimal stent
area of 5 mm2 predicts increased likelihood of angiographic restenosis)
Remodeling Length measurements

Qualitative Assessment
Atheroma morphology
Evaluating dissections and other complications
after intervention
Unstable lesions and ruptured plaques
Unusual lesion morphology
Ambiguous lesions

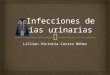
Atheroma Morphology by IVUS:Soft (left), mixed fibrous and calcified (center), and heavily calcified atheromas (right) are illustrated.

Atheroma Morphology
• Although intravascular ultrasonography cannot be used to detect and quantify specific histologic contents, certain image patterns can be very useful in estimating the morphology and content of the atheroma.
I. Soft (echolucent) plaques refer to the acoustic signal that arises from low echogenicity instead of plaque’s structural characteristics. Although a zone of reduced echogenicity generally results from high lipid content in a mostly cellular lesion, it could also result from a necrotic zone within the plaque, an intramural hemorrhage, or a thrombus.

Atheroma Morphology• Fibrous plaques have an intermediate echogenicity between soft
(echolucent) atheroma and highly echogenic calcific plaques.
• Generally, the greater the fibrous tissue content, the greater the echogenicity of the tissue.
• Ultrasound imaging is more sensitive than fluoroscopy for coronary calcification detection.[Large calcifications may be associated with lesion stability. In contrast, micro calcifications are frequently found in lipid-rich necrotic core areas of unstable plaques and may not be well reflected in intravascular ultrasonography images.

Atheroma Morphology
• Plaques frequently contain more than one acoustical subtype.
• A thrombus is usually recognized as an intraluminal mass, often with a layered, lobulated, or pedunculated appearance.
• However, in vitro studies have revealed limitations of intravascular ultrasonography in the diagnosis of thrombi (sensitivity of 57% and specificity of 91%), considerably inferior to conventional angiogram.

Atheroma Morphology
• The intimal hyperplasia characteristic of early in-stent restenosis often appears as tissue with very low echogenicity, at times less echogenic than the blood speckle in the lumen.
• Appropriate system settings are critical to avoid suppressing this relative nonechogenic material. The intimal hyperplasia of late in-stent restenosis often appears more echogenic.

Dissection After Balloon Angioplasty.

Evaluating Dissections And Other Complications After Intervention
• Intravascular ultrasound is commonly used to detect and direct the treatment of dissections and other complications after intervention.
• IVUS allows for detailed classification of dissection and assessing the severity of the dissection.
• Important characteristics of a dissection are identified distinctly by intravascular ultrasonography such as- – Presence of a false lumen, – Identification of mobile flap(s), – Presence of calcium at the dissection border, – Dissections in close proximity to stent edges

Stable And Vulnerable Plaques.

Unstable Lesions And Ruptured Plaques
• Although no definitive features define a plaque as vulnerable on IVUS , a hypoechoic plaque without a well-formed fibrous cap is presumed to represent potentially vulnerable atherosclerotic lesions because this represents a lipid-rich with a thin fibrous cap.[26]
• In patients studied after an acute coronary syndrome, ultrasound imaging may reveal ulceration, often with remnants of the ruptured fibrous cap evident at the edges of the ulcer. Various other appearances are common, including fissuring or erosion of the plaque surface.

Ruptured Plaque With Positive Remodelling.

Unusual Lesion Morphology
• Intravascular ultrasonography can be used to characterize unusual lesion morphology, such as aneurysms, pseudo-aneurysms, and true versus false lumens.

Ambiguous lesions• IVUS lends itself to the identification of technically difficult
lesions, such as intermediate lesions of uncertain stenotic severity or ostial stenosis and disease at branching sites.
• IVUS can also be helpful for delineating lesions involving tortuous vessels and left main stem lesions.
• IVUS has a particularly important role in defining areas with intraluminal filling defects, angiographically hazy lesions, sites with plaque rupture, and lesions with local flow disturbances.
• IVUS can be used to determine vein graft morphology in situ as well.

Special Disease Considerations
• In-stent Restenosis• Assessment of transplant vasculopathy• Aortic, carotid, and peripheral vascular
disease

“Candy wrapper” restenosis after placement of radioactive stent.

Some Snapshots

Angiographic Underestimation Of Disease.

Views Of Different Arterial Segments