Embed Size (px)
DESCRIPTION
Conheça um pouco mais de nossos serviços de BOMBEIRO INDUSTRIAL em www.resgate.com
Citation preview

Always En Route At
MARCH 2013
ISSUE
tt
1303JEMS_C1 C1 2/26/13 2:43 PM

Macro. Mini. All Set.
When a patient requires intravenous therapy, EMS providers need to
administer care as quickly as possible. The AMSafe-3® IV Administration
Set features a 3-in-1 multi-drip chamber that allows providers to select a
10, 15 or 60 drop setting on the spot.
The AMSafe-3 drop setting can be adjusted without interrupting patient
care. Since the device combines three IV sets into one, it reduces inventory
and takes up less room on an ambulance or in an equipment bag.
�� !����������������������� ����������!�����������
�� ���������������������������������!��������������
�� ��������� �������������!�������
For more information or a product demonstration,
contact your dedicated Account Manager or call 800.533.0523
1712-30204
AMSafe-3 IV Set, 91”, 1 luer activated
injection site and 1 pre-pierced injection site,
���������������������������������������������
site and pre-pierced injection sites, slide
��� �� ����������������������������
1712-30304
AMSafe-3 IV set, 89” with backcheck valve,
1 pre-pierced injection site, 1 luer activated
������������������������������������ ����
��� �� ����������������������������
D38301
AMSafe-3 IV Set, 83”, 1 luer activated
injection site and 1 pre-pierced injection
������ ����������������������������
Ma
kin
g P
rec
iou
s M
inu
tes
Co
un
t™
800-533-0523 www.boundtree.com
Choose 11 at www.jems.com/rs
1303JEMS_C2 C2 2/26/13 4:39 PM

Choose 12 at www.jems.com/rs
1303JEMS_1 1 2/26/13 3:22 PM

Barbara Spoden Thanks to a dedicated EMS team and use of
the ResQPOD®, Barbara survived and was able to
return to playing with her granddaughter.
�� �������� �������
�������������� �
�������������������
��������� ���������������������������
��������������������������������
����������������������������������������� ���������
�/.����/�/���/����������/�"��#/� �/��00/������/$ %�0&!���
/ ��/'��������/�������/���������/(��/�/�������/���������/(��/����/��/�/�����/0���/)�0*/��/(��/�/��������/��������/��/�����/����������/�����'/����'����/����+/������+/������/
/ ���/���/����/�������/��/��'���'/��/�/�0/�/�������/�/���'&���/����,/�(/�/�������/(��/����������/������/�/������/��((����'/(���/�������/������/��/������/��(�������//
/ ���/���/��/�������/�/�����/�����,�/������&�����/������/��/��/�������/��/�/�0/-���
�������������������� �������������
Choose 13 at www.jems.com/rs
1303JEMS_2 2 2/26/13 3:22 PM

WWW.JEMS.COM MARCH 2013 JEMS 3
Contents
DEPARTMENTS & COLUMNS
5 I LOAD & GO I Now on JEMS.com
10 I EMS IN ACTION I Scene of the Month
12 I FROM THE EDITOR I ‘Special Stretchers’
By A.J. Heightman, MPA, EMT-P
14 I LETTERS I In Your Words
16 I PRIORITY TRAFFIC I News You Can Use
20 I LEADERSHIP SECTOR I Impact Ahead
By Gary Ludwig, MS, EMT-P
22 I TRICKS OF THE TRADE I Batteries
By Thom Dick
24 I CASE OF THE MONTH I Forward Fall
By Michael Orland, MD
80 I HANDS ON I Product Reviews from Street Crews
By Dominic Silvestro, EMT-P, EMS-I
82 I LIGHTER SIDE I The Slow Farewell
By Steve Berry
84 I EMPLOYMENT & CLASSIFIED ADS
87 I AD INDEX
88 I LAST WORD I The Ups & Downs of EMS
About the CoverThe driver of a vehicle involved in a multiple vehicle crash in Springfi eld, Mo., is being assessed prior to extrication by a Springfi eld Fire Department fi refi ghter. The issue of when to fully immobilize patients and on what devices is explored in-depth in this month’s issue of JEMS. Read more, p. 12 and pp. 28–39. IMAGE JOSEPH THOMAS
MARCH 2013 VOL. 38 NO. 3
I SPINAL IMMOBILIZATION I Time for a change
By Jim Morrissey, MA, EMT-P
28
40 I IN THE PATH OF DESTRUCTION I New Jersey EMS response to Superstorm Sandy aided by
pre-planning & preparedness
By Henry P. Cortacans, MAS, CEM, NREMT-P; & Terry Clancy, PhD, NREMT-P
50 I THE PREHOSPITAL CARE RESEARCH FORUM
PRESENTS ... I Selected abstracts for presentation at the 31st annual EMS
Today Conference & Exposition in Washington, D.C.,
March 5–9, 2013
58 I EXPANDING THE MISSION I Mission: Lifeline will incorporate EMS recognition in STEMI &
cardiac resuscitation systems of care
By Chris Bjerke, MBA, BSN; Gary Wingrove, EMT-P; Franklin Pratt, MD; J. Lee Garvey,
MD; & A. Gray Ellrodt, MD
60 I PLANNING LIKE AN OLYMPIAN I How London Ambulance Service successfully handled their
‘summer of sport’
By Jason Killens, MStJ, JP
70 I REVIVING FREEDOM HOUSE I How the storied ambulance company has been reborn
By Megan Corry, MA, EMT-P; Casey Keyes, BA, NREMT-B; & David Page,
MS, NREMT-P
76 I BUILT TO SHARE I The Bay Shore/Brightwaters Rescue Ambulance’s new vehicle will
respond to multiple incident types and provide mutual aid
By Bob Vaccaro
I 40
®
PREMIER MEDIA PARTNER OF THE IAFC, THE IAFC EMS SECTION & FIRE-RESCUE MED
I 60
1303JEMS_3 3 2/26/13 3:22 PM

uninterrupted hands-free compressions
featuring comprehensive CPR analytics
with capnography and CPR Metronome
Visit our booth #811 at EMS Today 2013 in Washington D.C. to see
CPR innovation in action and receive a T-shirt.
©2013 Physio-Control, Inc. Redmond, WA
The responsive
emergency team
delivers exceptional
CPR
Today’s responsive emergency team is always looking to elevate the
level of care they deliver, and they rely on evidence and data to get
them there. With the CPR Solution from Physio-Control, they have the
science-based, guidelines-consistent tools they need to respond better
to patients—and the demands of constant performance improvement.
And they choose Physio-Control
to help make it happen.
physio-control.com/CPR
Choose 14 at www.jems.com/rs
1303JEMS_4 4 2/26/13 3:23 PM

LIKE US
facebook.com
/jemsfans
FOLLOW US
twitter.com
/jemsconnect
GET CONNECTED
linkedin.com/groups?
about=&gid=113182
EMS NEWS ALERTS
jems.com/enews
BEST BLOGGERS
FireEMSBlogs.com
CHECK IT OUT
jems.com/ems-products
JEMS.com offers you
original content, jobs,
products and resources.
But we’re much more
than that; we keep
you in touch with
your colleagues
through our:
> Facebook fan page;
> JEMS Connect site;
> Twitter account;
> LinkedIn profile;
> Product Connect site; and
> Fire EMS Blogs site.
JEMSMSMSMSMS ccom offers you
FOLLOW US ON
LOAD & GO LOG IN FOR EXCLUSIVE CONTENT
A BETTER WAY TO LEARN
JEMSCE.COM ONLINE CONTINUING
EDUCATION PROGRAM
DATA WEBCASTCheck out our next webcast, which will be at 10 a.m. (Eastern
time) March 20. In this webcast, sponsored by ZOLL Data, fire-fighter/paramedic and EMS 10: Innovator in EMS Award-winner John Pringle will present, “Update on 360-degree Data: How to collect better data in the field.” He will give you prac-tical steps to successfully integrate new electronic tools into your emergency response systems.▲ jems.com/webcasts
THE JOURNEYI take for granted the things I do that make up most days; starting IV’s, admin-istering aspirin and nitro, assessing vital signs, stopping blood from leaving peoples bodies et al, but one of those mundane tasks I’ll never think of as busi-ness as usual again.
Last night, while talking with a group of friends, a meeting if you will, one of the members of the group, who struggles with addiction spoke of his recent
overdose, and subsequent revival and spiritual awakening.“I know how much I can do, and how much I can’t,” he explained. “Trust me, people who OD don’t
do so by accident.”
WWW.JEMS.COM MARCH 2013 JEMS 5
Where do you see EMS going in 2020?
That was the question put to four EMS
visionaries—James J. Augustine, MD, FACEP;
Matt Zavadsky, MS-HSA, EMT; David Page,
MS, NREMT-P; and moderator A.J. Heightman,
MPA, EMT-P. For hours, we f lmed them
while they created a new future. Join the
2020 EMS Visionaries LinkedIn group to get
engaged in the discussion.
Visit www.ems2020
vision.com to watch
the latest 2020 Vision
Leadership Series
video interviews.
JEMS.com
Setting our sights on the future of EMS
www.FernoEMS.com
http://linkedin.
ems2020vision.com
FEATURED BLOG: Rescuing Providence
Sponsored Product Focus
MULTI-PATIENT MONITORING SYSTEMThe new Multi-Patient Monitoring System (MPMS) from First Line Technology allows emergency personnel to stay connected and provide constant monitoring for up to 20 patients during triage, transport and care. The MPMS includes a roll and carry bag wired to charge both the (included) Wireless Vital SignsMonitor devices and a remote monitoring device.▲ Check out their ad on JEMS.com!
1303JEMS_5 5 2/26/13 3:23 PM

�
�
���������������������
•
•
•
•
•
EDITOR-IN-CHIEF I A.J. Heightman, MPA, EMT-P I [email protected]
MANAGING EDITOR I Jennifer Berry I [email protected]
ASSOCIATE EDITOR I Ryan Kelley I [email protected]
ASSISTANT EDITOR I Kindra Sclar I [email protected]
ONLINE NEWS/BLOG MANAGER I Bill Carey I [email protected]
ASSOCIATE WEB EDITOR I Nicole Reino I [email protected]
EDITORIAL DIRECTOR I Shannon Pieper I [email protected]
MEDICAL EDITOR I Edward T. Dickinson, MD, NREMT-P, FACEP
CONTRIBUTING EDITOR I Bryan Bledsoe, DO, FACEP, FAAEM
ART DIRECTOR I Liliana Estep I [email protected]
CONTRIBUTING ILLUSTRATORS
Steve Berry, NREMT-P; Paul Combs, NREMT-B
CONTRIBUTING PHOTOGRAPHERS
Vu Banh, Glen Ellman, Craig Jackson, Kevin Link, Courtney McCain, Tom Page, Rick Roach,
Steve Silverman, Michael Strauss, Chris Swabb
DIRECTOR OF ePRODUCTS/PRODUCTION I Tim Francis I [email protected]
PRODUCTION COORDINATOR I Matt Leatherman I [email protected]
PUBLICATION OFFICE
800/266-5367 I Fax 858/638-2601
ADVERTISING DEPARTMENT
800/266-5367 I Fax 858/638-2601
ADVERTISING DIRECTOR I Judi Leidiger I 619/795-9040 I [email protected]
WESTERN ACCOUNT REPRESENTATIVE I Cindi Richardson I 661/297-4027 I
SENIOR SALES COORDINATOR I Elizabeth Zook I 951/244-1245 I [email protected]
REPRINTS, ePRINTS & LICENSING I Rae Lynn Cooper I 918/831-9143 I [email protected]
VICE PRESIDENT, MARKETING SERVICES I Paul Andrews I 240/595-2352 I
SUBSCRIPTION DEPARTMENT I 888/456-5367
DIRECTOR, AUDIENCE DEVELOPMENT & SALES SUPPORT I Mike Shear I [email protected]
MARKETING & CONFERENCE DIRECTOR I Debbie Murray I [email protected]
MARKETING & CONFERENCE COORDINATOR I Vanessa Horne I [email protected]
CHAIRMAN I Frank T. Lauinger
PRESIDENT & CHIEF EXECUTIVE OFFICER I Robert F. Biolchini
CHIEF FINANCIAL OFFICER I Mark C. Wilmoth
SENIOR VICE PRESIDENT & GROUP PUBLISHER I Lyle Hoyt I [email protected]
VICE PRESIDENT/PUBLISHER I Jeff Berend I [email protected]
www.EMSToday.com
EXECUTIVE DIRECTOR I Jeff Berend
CONFERENCE DIRECTOR I Debbie Murray
EDUCATION DIRECTOR I A.J. Heightman
EVENT OPERATIONS MANAGER I Amanda Wilson
EXHIBIT SERVICES MANAGER I Raymond Ackermann
EXHIBIT SALES REPRESENTATIVE I Sue Ellen Rhine I 918/831-9786 I [email protected]
EXHIBIT SALES REPRESENTATIVE I Tracy Thompson I 918/832-9390 I [email protected]
FOUNDING EDITOR I Keith Griffiths
FOUNDING PUBLISHER
James O. Page (1936–2004)
®
Choose 15 at www.jems.com/rs
1303JEMS_6 6 2/26/13 3:23 PM

800-257-3810 | www.masimo.com
© 2013 Masimo Corporation. All rights reserved.
1 EMMA Users Manual.
World’s smallest portable self-contained capnometerEMMA™ (Emergency Mainstream Analyzer) is a fully self-
contained mainstream capnometer that requires no
routine calibration and virtually no warm up time.1 With
rapid measurement of end-tidal CO2 and respiration
rate, EMMA can help providers guide ventilation rates and
assess the effectiveness of CPR allowing them to make
adjustments in the course of treatment, breath by breath.
Accurate from the First Breath
Choose 16 at w ww.jems.com/rs
1303JEMS_7 7 2/26/13 3:23 PM

8 JEMS MARCH 2013
EDITORIAL BOARDWILLIAM K. ATKINSON II, PHD, MPH, MPA,
EMT-PPresident & Chief Executive Officer,
WakeMed Health & Hospitals
JAMES J. AUGUSTINE, MD, FACEPMedical Director, Washington Township (Ohio) Fire Department Associate Medical Director, North Naples (Fla.) Fire DepartmentDirector of Clinical Operations, EMP ManagementClinical Associate Professor, Department of
Emergency Medicine, Wright State University
STEVE BERRY, NREMT-PParamedic & EMS Cartoonist, Woodland Park, Colo.
BRYAN E. BLEDSOE, DO, FACEP, FAAEMProfessor of Emergency Medicine, Director, EMS Fellowship,
University of Nevada School of MedicineMedical Director, MedicWest Ambulance
CRISS BRAINARD, EMT-PDeputy Chief of Operations, San Diego Fire-Rescue
CHAD BROCATO, DHS, REMT-PAssistant Chief of Operations, Deerfield Beach (Fla.) Fire-Rescue Adjunct Professor of Anatomy & Physiology, Kaplan University
J. ROBERT (ROB) BROWN JR., EFOFire Chief, Stafford County (Va.) Fire & Rescue Department Executive Board, EMS Section,
International Association of Fire Chiefs
CAROL A. CUNNINGHAM, MD, FACEP, FAAEMState Medical Director,
Ohio Department of Public Safety, Division of EMS
THOM DICK, EMT-PQuality Care Coordinator,
Platte Valley (Colo.) Ambulance
BRUCE EVANS, MPA, EMT-P Deputy Chief, Upper Pine River Bayfield Fire Protection, Colorado District
JAY FITCH, PHDPresident & Founding Partner, Fitch & Associates
RAY FOWLER, MD, FACEPAssociate Professor,
University of Texas Southwestern School of MedicineChief of EMS, University of Texas Southwestern Medical Center Chief of Medical Operations,
Dallas Metropolitan Area BioTel (EMS) System
ADAM D. FOX, DPM, DOAssistant Professor of Surgery,
Division of Trauma Surgery & Critical Care,University of Medicine & Dentistry of New Jersey
Former Advanced EMT-3 (AEMT-3)
GREGORY R. FRAILEY, DO, FACOEP, EMT-PMedical Director, Prehospital Services, Susquehanna HealthTactical Physician, Williamsport (Pa.) Bureau of
Police Special Response Team
JEFFREY M. GOODLOE, MD, FACEP, NREMT-PProfessor & EMS Section Chief
Emergency Medicine, University of Oklahoma School of Community Medicine
Medical Director, EMS System for Metropolitan Oklahoma City & Tulsa
KEITH GRIFFITHSPresident, RedFlash GroupFounding Editor, JEMS
DAVE KESEG, MD, FACEPMedical Director, Columbus Fire Department Clinical Instructor, Ohio State University
W. ANN MAGGIORE, JD, NREMT-PAssociate Attorney, Butt, Thornton & Baehr PCClinical Instructor, University of New Mexico,
School of Medicine
CONNIE J. MATTERA, MS, RN, EMT-PEMS Administrative Director & EMS System Coordinator,
Northwest (Ill.) Community Hospital
MIKE MCEVOY, PHD, REMT-P, RN, CCRNEMS Coordinator, Saratoga County, N.Y.EMS Editor, Fire Engineering MagazineResuscitation Committee Chair, Albany (N.Y.) Medical College
MARK MEREDITH, MDAssistant Professor, Emergency Medicine and Pediatrics,
Vanderbilt Medical Center Assistant EMS Medical Director for Pediatric Care,
Nashville Fire Department
GEOFFREY T. MILLER, EMT-PDirector of Simulation Eastern Virginia Medical School,
Office of Professional Development
BRENT MYERS, MD, MPH, FACEPMedical Director, Wake County EMS SystemEmergency Physician, Wake Emergency Physicians PAMedical Director, WakeMed Health & Hospitals
Emergency Services Institute
MARY M. NEWMANPresident, Sudden Cardiac Arrest Foundation
JOSEPH P. ORNATO, MD, FACP, FACC, FACEPProfessor & Chairman, Department of Emergency Medicine,
Virginia Commonwealth University Medical CenterOperational Medical Director,
Richmond Ambulance Authority
JERRY OVERTON, MPAChair, International Academies of Emergency Dispatch
DAVID PAGE, MS, NREMT-PParamedic Instructor, Inver Hills (Minn.) Community CollegeParamedic, Allina Medical TransportationMember of the Board of Advisors,
Prehospital Care Research Forum
PAUL E. PEPE, MD, MPH, MACP, FACEP, FCCMProfessor, Surgery, University of Texas
Southwestern Medical CenterHead, Emergency Services, Parkland Health & Hospital SystemHead, EMS Medical Direction Team,
Dallas Area Biotel (EMS) System
DAVID E. PERSSE, MD, FACEPPhysician Director, City of Houston Emergency Medical Services Public Health Authority, City of Houston Department.
of Health & Human ServicesAssociate Professor, Emergency Medicine,
University of Texas Health Science Center—Houston
EDWARD M. RACHT, MDChief Medical Officer, American Medical Response
JEFFREY P. SALOMONE, MD, FACS, NREMT-PTrauma Medical Director, Maricopa Medical CenterProfessor of Surgery, University of Arizona College of Medicine—Phoenix
KATHLEEN S. SCHRANK, MDProfessor of Medicine & Chief,
Division of Emergency Medicine,University of Miami School of Medicine
Medical Director, City of Miami Fire RescueMedical Director, Village of Key Biscayne Fire Rescue
JOHN SINCLAIR, EMT-PInternational Director, IAFC EMS SectionFire Chief & Emergency Manager,
Kittitas Valley (Wash.) Fire & Rescue
COREY M. SLOVIS, MD, FACP, FACEP, FAAEMProfessor & Chair, Emergency Medicine,
Vanderbilt University Medical CenterProfessor, Medicine, Vanderbilt University Medical CenterMedical Director, Metro Nashville Fire DepartmentMedical Director, Nashville International Airport
WALT A. STOY, PHD, EMT-P, CCEMTPProfessor & Director, Emergency Medicine,
University of PittsburghDirector, Office of Education,
Center for Emergency Medicine
RICHARD VANCE, EMT-PCaptain, Carlsbad (Calif.) Fire Department
JONATHAN D. WASHKO, BS-EMSA, NREMT-P, AEMD
Assistant Vice President, North Shore-LIJ Center for EMSCo-Chairman, Professional Standards Committee,
American Ambulance AssociationAd-Hoc Finance Committee Member, NEMSAC
KEITH WESLEY, MD, FACEPMedical Director, HealthEast Medical Transportation
KATHERINE H. WEST, BSN, MED, CICInfection Control Consultant,
Infection Control/Emerging Concepts Inc.
STEPHEN R. WIRTH, ESQ.Attorney, Page, Wolfberg & Wirth LLC.Legal Commissioner & Chair, Panel of Commissioners,
Commission on Accreditation of Ambulance Services (CAAS)
DOUGLAS M. WOLFBERG, ESQ.Attorney, Page, Wolfberg & Wirth LLC
WAYNE M. ZYGOWICZ, BA, EFO, EMT-PEMS Division Chief, Littleton (Colo.) Fire Rescue
®
1303JEMS_8 8 2/26/13 3:23 PM

Choose 18 at www.jems.com/rs
When urgency and bravery are
essential job requirements, the
success of your business depends
on a commercial vehicle that won’t
back down from a challenge. With
an Adaptive Electronic Stability
Program®1 and both Best-In-Class*
payload capacity and standing
height, only the 2013 Freightliner
Sprinter is designed to answer the
call as boldly as you do every day.
freightlinersprinterusa.com
DRIVEN LIKE YOU.©2013 Daimler Vans USA, LLC *Based on a comparison of the
Automotive News classifi cation of full-size commercial vans.
1 No system, regardless of how advanced, can overcome the laws of
physics or correct careless driving. Please always wear your seat belt.
Performance is limited by available traction, which snow, ice and other
conditions can af ect. Always drive carefully, consistent with conditions.
Best performance in snow is obtained with winter tires. Choose 17 at www.jems.com/rs
1303JEMS_9 9 2/26/13 3:23 PM

10 JEMS MARCH 2013
>> PHOTOS JOSEPH THOMASEMS IN ACTIONSCENE OF THE MONTH
1303JEMS_10 10 2/26/13 3:23 PM

WWW.JEMS.COM MARCH 2013 JEMS 11
St. John’s/Mercy (Mo.) EMS Paramedic Christy Biram carries a 3-year-old female pedi-
atric patient on a pediatric backboard to a waiting ambulance at the scene of a crash
that involved two vehicles colliding at a stoplight. The vehicle the pediatric patient was in
was hit when another vehicle allegedly ran a red light. The girl was secured properly in a
child safety seat and had been extricated from the vehicle and car seat by her mother prior
to EMS arrival. Her only injuries were abrasions to her thighs and clavicles from the safety
seat restraints. She had been placed in spinal mobile restriction by Springfield Fire Depart-
ment prior to EMS arrival. She was transported to a Level 1 trauma center, where she was
treated and released. The driver of the other car collided with one of the stoplight posts,
causing the battery to fly out of the vehicle and hit a pedestrian who narrowly missed get-
ting hit by the vehicle. The pedestrian had a minor leg injury but refused care on scene, and
the driver of the vehicle that ran the light had to be extricated and was transported to an
emergency department. Note the crew’s professionalism, covering the patient’s body sur-
face with a turnout coat after exposing and assessing her lower torso.
PEDIATRIC IMMOBILIZATION
1303JEMS_11 11 2/26/13 3:23 PM

It’s amazing how committees, lim-
ited research and the omission of
a few words can change protocols
and affect the delivery of patient care
and comfort. Jim Morrissey’s article,
“Spinal Immobilization,” pp. 28–39,
is an epic piece of work, backed by
36 footnoted references that illustrate
we over-board patients, waste pre-
cious time at penetrating injury calls
and make patients uncomfortable by
placing them on hard surfaces that do
not fit their anatomy or support their
injuries without proper padding and
weight distribution.
I’m going to take you back to 1971,
when EMS got its “roots” in formal-
ized education with the release of the
initial EMT textbook, Emergency Care
and Transportation of
the Sick and Injured.
The first AAOS text-
book stated:
“Carefully splint the
injured spine, avoiding
abnormal or excessive
motion. Be sure that the
injured person is properly
splinted and transported
on a long backboard or
special stretcher with-
out bending or twisting
the spine in any direction.”
I call your attention to the important words “or special
stretcher” because those words were somehow omitted from
subsequent editions of the AAOS and most other textbooks.
Those omitted words resulted in decreased use of scoop and
canvas stretchers with slat supports, and SKED stretchers, in
some systems, and should be added back into our protocols and
textbooks to allow crews to use multiple devices to accomplish
spinal immobilization.
The “General Principles of Splinting” section in the 1971
AAOS textbook presented treatment considerations that still
hold true today:
“All fractures should be ‘splinted where they lie’; Apply the splint or ban-
dage before moving or transporting the patient; With some very important
exceptions, a severely angulated fracture should be straightened prior to
splinting; and pad the splint carefully to
prevent pressure points and discomfort to
the extremity [and the patient].”
Morrissey’s article gives you the
science, research and reasons to
allow your crews to use multiple
proven “special stretchers,” in addi-
tion to the traditional longboard,
to immobilize patients and “splint”
their injuries.
I spent a day with Poway (Calif.)
Fire Department Captain Andy Page
and crews from Engine 3711 and
Medic 3791. We applied, secured,
moved and transported paramedic/
firefighter Jon Maxwell up and down
stairways in some of the latest “spe-
cial stretchers” designed to properly
immobilize his spine.
We used: Conven-
tional scoop-style
stretchers; Full-body
vacuum platforms;
Vacuum splints and
a Ferno Flexible
Stretcher. We also used
Ferno’s EasyFix Vac-
uum Mattress/Stretcher
that is being used
throughout Europe
and was recently intro-
duced in the U.S.
Most of the devices
offered more comfort and security than a longboard without extra
padding. The vacuum devices were also durable, easily moldable to
the patient, and tended to better “cradle” the patient securely. We
used SSCOR and Laerdal suction devices to speed up the process.
Perhaps the most interesting finding was that vacuum mat-
tresses used in conjunction with the Ferno flexible stretcher and its
six conveniently-located handles, offered the best body mechanics
and positioning to maneuver our patient down stairways and
around tight corners, proving that some things haven’t changed
since 1971, when this type of flexible stretcher was first introduced
to EMS.
See a demo of the EasyFix Mattress at www.youtube.com/watch?v=-WF73wKdfZM
‘SPECIAL STRETCHERS’How two eliminated words impacted immobilization options
FROM THE EDITORPUTTING ISSUES INTO PERSPECTIVE
>> BY A.J. HEIGHTMAN, MPA, EMT-P
12 JEMS MARCH 2013
FERNO FULL-BODY VACUUM MATTRESS
HARTWELL MEDICAL EVAC-U-SPLINT
MATTRESS/STRETCHER USED ALONG
WITH A HARTWELL COMBICARRIER
FERNO’S EASYFIX VACUUM MATTRESS/STRETCHER
COMBINATION
FERNO’S MODEL 137 FLEXIBLE STRETCHER WITH BUILT-IN
RESTRAINTS USED IN TANDEM WITH A VACUUM SPLINT
1303JEMS_12 12 2/26/13 3:33 PM

The Safe Choice
NeedlesticksBlood Exposure
Catheter Complications
Introcan Safety® 3 Closed IV Catheterhelps shield against
From start to finish, Introcan Safety 3 provides:
�� Fully automatic safety shield that protects against needlesticks.
�� Multiple-access septum that helps prevent blood exposure.
�� Advanced stabilization that minimizes catheter movement to help
reduce irritation and associated restarts.
�� Lower cost and less waste from insertion through disposal.
introcansafety.bbraunusa.com
1-800-227-2862
The following is a list of supporting documents and reference material:1) Tosini, et al “Needlestick Injury Rates According to Dif erent Types of Safety-Engineered Devices: Results of a French Multicenter Study”, Infection Control and Hospital Epidemiology, Vol. 31, No. 4 April 2012 pp. 402-407 2) Bausone-Gazda D, et al, A Randomized Controlled Trial to Compare the Complications of 2 Peripheral Intravenous Catheter-Stabilization Systems, Journal of Infusion Nursing, 2012, Nov-Dec: 33(6):371 843) Shears G MD, Comparing an Intravenous Stabilizing Device to Tape, Journal of Infusion Nursing, Vol. 29, No. 4 July/August 20064) B. Braun Engineering Data on File5) B. Braun Introcan Safety 3 Cost Analysis Model6) McNeill, EE, et al, A Clinical Trial of a New All-in-one Peripheral Short Catheter, JAVA, 2009, Vol. 14, No. 1, pp. 46-50 7) Infusion Nurses Society (2011), Infusion Nursing Standards of Practice, Journal of Infusion Nursing Supplement, Vol. 34, No. 15, Std. 22, Std. 36 13-3611_2/13_JEMS_BB
Choose 18 at www.jems.com/rs
1303JEMS_13 13 2/26/13 3:33 PM

LETTERSIN YOUR WORDS
14 JEMS MARCH 2013
MECHANICAL CPR ADVANTAGES
We read the article “Are the Benefits of Mechanical CPR
Worth the Interruption Time?” (www.jems.com/arti-
cle/patient-care/are-benefits-mechanical-cpr-worth-
interr) with great interest. We participated in the NALE
project and submitted our data as part of the article
published in Resuscitation.
The authors of the review bring up some impor-
tant points about the findings, but we fear they do not
answer the question posed in the title of their article.
We have extensive experience using the mechani-
cal compression device with more than 1,200 uses to
date. One of the first things we learned when deploy-
ing the device was that crews put it as a priority and the
other, time-important interventions were delayed. We
had to put it into our protocols and train our people
to place it later in the event, after other interventions
were completed.
Next, we learned that placing the device tended
to cause everyone else to pause and help out. This
is much like our previous experience with intubation
where everyone stopped what they were doing until
the “vital” procedure was completed.
We changed our protocol again and trained our
staff how to place the device with no or minimal inter-
ruptions in other tasks. We now have a procedure
where the device is placed in stages and the maximum
interruption in compressions is 15 seconds.
The benefits of the device are many. We can see
in our cases that interruptions are minimal and short
once the device is placed. That may be the best argu-
ment when discussing whether the interruption is
worth it. We see it as accepting an early 15 second delay
which then prevents multiple delays later in the event.
During our quality assurance reviews, we see inter-
ruptions as providers tire and switch users, or as the
patient’s location is changed.
There is a real challenge in any research pertaining to
cardiac arrest right now. That challenge is trying to asso-
ciate one treatment with a definitive improvement in
outcome. This is a rapidly changing body of knowledge
and there is no agreed-upon protocol. So the question
of whether the delay in compressions when placing the
device is worth it is a difficult question to answer and
maybe should not be asked. A better question might
be “What are the advantages of using a mechanical
compression device, and how does it fit into a system
approach to care of the cardiac arrest victim?”
Our extensive experience is a resounding “yes,” it
is a vital part of our overall approach to improving the
community’s and emergency care system’s response to
cardiac arrest.
Charles Lick, MD
Paul Satterlee, MD
Allina Health EMS
PSYCH ISSUES
I am sorry Thom … while I’m
sure you are a great medic
and all, I just feel much of
this is bad advice. The main
reason being, why would/
should EMS be transport-
ing patients that are cur-
rently off their meds and/or
known to be diagnosed at the hospital as psychotic,
are potentially suicidal and/or homicidal, when we
have very little to no education in handling this? Isn’t
it enough that we have to occasionally deal with
potentially psychotic, suicidal or homicidal patients?
I read a story from a provider just last night who
described a situation where a psych patient, who
went nuts during an inter-facility transport, was able
to free themselves, threaten the provider and then
proceed to jump out of the ambulance and run away.
The truth is, as long as these patients don’t require
some sort of medical intervention en route to the
receiving medical/psychological treatment facility,
there is absolutely no reason whatsoever that they
should not be transported by law enforcement. Law
enforcement officers have the training and authority
to safely handle these patients, not EMS providers.
Jason M.
Via Facebook
Author Thom Dick, EMT-P, responds: Thanks, Jason,
for highlighting these issues. I think no matter who we
are or how great our skill, we don’t “know” very much
about most of the sick people we meet—certainly not
during the brief span of an ED visit. But even if we could
be sure somebody’s etiology is psychological, does that
somehow transform them into something less than a
sick person? I don’t think it does.
I agree with you that we all need and deserve to
understand more about behavioral disorders. The
Western medicine to which we all subscribe endorses
a pathetic approach to people with mental illness.
Your health insurance company will typically pay for
a 60-minute first visit with an internist. Care to guess
what they’ll allow for a first visit with a psychiatrist,
for a much more complex problem? On average,
they’ll pay a psychiatrist for 15 minutes.
What we call caring for mental patients basically
amounts to throwing drugs at them. It’s no wonder. The
standard Diagnostic and Statistical Manual (DSM) you’ll
find on the desk of every ED physician is republished
every few years as a means of classifying people with
psychiatric illnesses. The current edition, the DSM-IV,
lists six technical editors—all with published direct finan-
cial ties to pharmaceutical companies. Five of those six
are linked to the same pharmaceutical company (Eli Lilly).
As for bad advice, every one of the suggestions in
this article would have helped the crew you describe
to sense, predict and prevent the incident they expe-
rienced, as well as protect the patient and the public
who were also endangered.
It’s sad that, after all these years, the EMS texts
we trust either ignore this important part of field medi-
cine or recommend procedures that are sure to get us
injured along with the sick people we care for.
In my opinion, this is medicine we’re doing here.
Medicine is supposed to help people. We’re sup-
posed to help people. And a cage car is just not part
of that process.
ADDING TO THE
DISCUSSION
This month, we feature some
strong opinions from readers on
two recent articles. The first is a
response to a JEMS.com Street
Science column “Are the Ben-
efits of Mechanical CPR Worth
the Interruption Time?” by Keith
Wesley, MD, FACEP, and Mar-
shall J. Washick, BAS, NREMT-P,
that reviewed a study examining
interruption time in mechani-
cal CPR. The second comment is
from one of our Facebook fans,
who takes issue with Thom Dick’s
August “Tricks of the Trade” col-
umn advising on “Psych Trans-
fers: Know how to deal with these
types of patients.”
A
D
T
s
t
r
S
e
t
W
s
t
i
c
f
w
A
u
f
tPH
OT
O C
OU
RT
ESY
PH
YSIO
-C
ON
TR
OL
1303JEMS_14 14 2/26/13 3:33 PM

4660 La Jolla Village Drive, Suite 900 | San Diego, CA 92122 | 800-788-7999 | Fax 858-622-4130 | www.LMANA.com
Teleflex, LMA, LMA Airway Management, LMA Atomization, LMA Better by Design, LMA EMS, LMA MAD Nasal, LMA Pain Management, LMA Visualization
and MAD are trademarks or registered trademarks of Teleflex Incorporated or its affiliates.
©2013 Teleflex Incorporated. All rights reserved. 2013-1644.
SOFT CONICAL PLUG
The plug forms a seal
with the nostril preventing
expulsion of fluid.
ATOMIZATION SPRAY
The spray atomizes
drugs into a fine mist
of particles 30 - 100
microns in size.
FLEXIBLE STYLET
The flexible stylet
allows 180° positioning
of the nasal plug.
LMA FAMILY
LMA Atomization® | LMA EMS™ | LMA Airway Management™ | LMA Visualization™ | LMA Pain Management™
No shot. No needle. No risk of needle stick injury.
LMA®
MAD Nasal™
The LMA MAD Nasal™ atomization device
is the safe and painless way to deliver
medication into your patient’s blood
stream without an intravenous line.*
*For use with drugs approved for intranasal delivery
For more information contact your
LMA representative or visit LMANA.com.
Answer.
Your patient
requires urgent
pain medication.
How can you
administer this
less invasively?
Choose 19 at www.jems.com/rs
1303JEMS_15 15 2/26/13 3:33 PM

T he Newtown (Conn.)
school shooting and
Webster (N.Y.) ambush
of firefighters provide increased
awareness of violence against
emergency responders. East Hart-
ford (Conn.) Fire Chief John Oates,
writing for the National Fallen Fire
Fighters (NFFF), has provided nine
questions responders should ask:
1. Do you use risk/benefit analy-
sis for every call?
2. Do you have an effective rela-
tionship at all levels with the
law enforcement agencies in
your community?
3. How good is the information
you get from your dispatcher?
4. Do you allow members to
“first respond” directly to the
scene?
5. Does your law enforcement
agency use an incident man-
agement system?
6. When responding to a poten-
tially violent incident, do you
seek out a law enforcement
officer when you arrive?
7. Have you told your fire officers/per-
sonnel that it’s OK to leave the scene
if things start to turn bad?
8. Is there a point at which you don’t
respond or limit your response to vio-
lent incidents?
9. Is your uniform easily mistaken for
law enforcement?
These questions came from a March 2012
focus group of 35 participants representing
29 organizations. The NFFF-commissioned
report from this group, “Firefighter Life
Safety Initiative 12 Final Report: National
protocols for response to violent incidents
should be developed and championed,” is
part of a resource package covering 16 Fire-
fighter Life Safety Initiatives of the Everyone
Goes Home program.
PREVENTING LINE-OF-DUTY INJURY
Everyone Goes Home is a national pro-
gram by the National Fallen Firefighters
Foundation to prevent line-of-duty deaths
and injuries. In March 2004, a Firefighter
Life Safety Summit was held in Tampa,
Fla., to address the cultural, philosophi-
cal, technical and procedural problems
that affected safety within the fire service.
The most important domains were identi-
fied, resulting in 16 Firefighter Life Safety
Initiatives. Everyone Goes Home started
as a way of implementing initiatives at the
local level.
NFFF asked subject matter experts to
develop a white paper for each initia-
tive. Chief Oates provided the Initiative
12 report. The Novato, Calif., 2007 sum-
mit developed actionable objectives to
support each of the Firefighter Life
Safety Initiatives.
Noting that there was, “an absence
of response protocols for violent
incidents in many fire departments”
a focus group met in Anne Arun-
del County, Md., in 2012 to develop
an expanded report for Initiative 12,
including the nine questions.
There’s no enforcement author-
ity or funding to implement the
Firefighter Life Safety Initiatives.
Some feel that more effort should
be directed against those who
assault responders.
‘PARAMEDICS ARE
NOT PUNCHING BAGS’
New South Wales, Australia, ambu-
lance service acting Commissioner
Mike Willis announced a zero-toler-
ance policy toward violence against
EMS personnel, noting on the agen-
cy’s website that there were six
assaults against paramedics in early
December.
There’s a perception that sanctions
against those who assault EMS personnel
are inadequate. In Illinois it’s a felony to
assault a first responder; however, Chicago
paramedics claimed, in a WLS-TV ABC
News 7 report, that those who assault them
get trivial punishment.
One technique that has been used is to
fill a courtroom with emergency respond-
ers in uniform. In January, the New York
Post reported that two dozen EMS workers
filled a Manhattan courtroom to support
their colleague who was allegedly choked
by a drunken assistant district attorney.
— Michael J. Ward, MGA
PRIORITY TRAFFICNEWS YOU CAN USE
16 JEMS MARCH 2013
NFFF Response to Violent Incidents
For more of the latest EMS news, go to jems.com/news
Nine questions first responders should askIM
AG
E C
OU
RT
ESY
NA
TIO
NA
L F
ALLEN
FIR
E F
IGH
TER
S
Cover of the NFFF report “Firefighter Life Safety Initiative 12.”
Reports referenced in this article are available at: www.everyonegoeshome.
com/news/2013/initiative12_012913.html
1303JEMS_16 16 2/26/13 3:33 PM

®® TM
JEMS.com
eNewsletter
The JEMS eNewsletter gives you breaking news, articles and product information. It’s free to subscribe … stay ahead of the latest news!
Product
Connect
Giving you the detailed product information you need, when you need it. We collect all the information from manufacturers and put it in one place, so it’s easy for you to f nd and easy for you to read.
Go to www.jems.com/ems-products
JEMS, Journal of Emergency Medical ServicesWith content from writers who are EMS professionals in the f eld, JEMS provides the information you need on clinical issues, new products and EMS trends. Available in print and digital editions!
JEMS.com
Website
Your online connection to the EMS world, JEMS.com gives you information on:• Products
• Jobs
• Patient Care• Training• Technology
For more information on the JEMS Family of EMS Products: www.JEMS.com
Archived Webcasts• PEARS: Helping You Help Kids• Lessons From Our Battlef elds: New Approaches to Shock Management• Securing the Airway: The Expanding Role of Extraglottic Devices• Maximizing Your Revenue• Advances in Assisted Ventilation: Where have we come from &
where are we going?
The JEMS Family of Products:
Helping You Save Lives
Free … Available
24/7!
1303JEMS_17 17 2/26/13 3:33 PM

PRIORITY TRAFFIC>> CONTINUED FROM PAGE 16
18 JEMS MARCH 2013
SERVING THOSE WHO SERVE
Effectively treating military
personnel & veterans
First responders are a critical first con-
tact point for members of the armed
forces and veterans in crisis. Many EMS and
other emergency response agencies aren’t
effectively prepared to effectively serve those
who serve. For example, first
responders often don’t have
sufficient knowledge of mili-
tary culture and few know
how to de-escalate calls
involving military members
and veterans.
Special programming at
this year’s 2013 EMS Today
Conference & Exposition will focus on serv-
ing this special population. The conference
will feature presentations by a team from
Arizona’s Military/Veteran First Responder
Initiative. This effort, facilitated by the Ari-
zona Coalition for Military Families (ACMF),
brings together public and private sector
partners from the military, government and
community to focus on strengthening crisis
response for military members and veterans,
including those experiencing post-traumatic
stress and traumatic brain injury.
The training, which has
been developed by the ACMF
over the past four years, is
nationally recognized as a
best-practice approach to
improve the coordination of
care through training and net-
working personnel.
In the past year, through this
partnership, more than 2,200 first respond-
ers in Arizona have received training, with
plans for several hundred more this spring.
This initiative fits into a larger state effort to
build community capacity to care for and
support service members, veterans and their
families, including initiatives around behav-
ioral health, higher education, employment
and faith-based communities.
The Arizona Coalition for Military Fam-
ilies and partners are currently exploring
how to expand this training effort to reach
first responders across the country.
The presentation team at EMS Today
Conference & Exposition will include Cap-
tain Dean Pedrotti of the Phoenix Fire
Department, SSG (Ret.) Patrick Ziegert of
the Office of the Arizona Attorney Gen-
eral and Colleen Day Mach of the Arizona
Coalition for Military Families. The main
presentation is Friday, March 8, from 8–10
a.m. with a presentation on post-trau-
matic stress on Saturday, March 9, from
10–10:30 a.m. — Thomas Winkel, MA, LPC, NCC
DUTY TO ACT ARE YOU ALWAYS ON CALL?
Scenario: A medic stops at the grocery store after her shift. She’s still in her
company uniform and witnesses an older man drop to the floor, appar-
ently unconscious. Does the medic have a legal duty to act? Probably not. If
she chooses to walk on by, can she be held legally liable? Again, probably not.
Why? Because she doesn’t have a legal duty to act.
Tort law requires four elements for a plaintiff to hold a defendant legally
responsible for a personal injury. These elements are 1) a legal duty to act; 2) a
breach of that duty; 3) proximate causation (i.e., the defendant’s breach of duty
was the legal cause of the plaintiff’s harm); and 4) damages (i.e., losses or harm
that merits financial compensation). Unless an EMS provider has a legal duty to
the patient, they cannot be held liable in tort law.
In our scenario above, the medic was off duty, having completed her shift.
The fact that she was in uniform doesn’t change the analysis; your legal duty to
act isn’t dependent on your wardrobe.
To use the reverse of this example, if the medic was on duty, spilled grape
juice on her uniform at work and changed into a non-uniform shirt, she still has
a duty to respond when called. Certainly, the fact that the medic was in uni-
form while off duty at the grocery store, probably with a patch or some insignia
that identified her employer, still doesn’t create a legal duty to act when she
witnessed the man fall to the floor. Of course, it could raise a public relations
issue if the medic elects not to provide assistance to the patient, but it doesn’t
give rise to a legal duty.
As this scenario makes clear, there’s a difference between a legal duty and
a moral duty. Certainly, many EMS providers feel they may have a moral duty
to act in this scenario, though that is a personal decision that the law permits
each of us to make based on our own values and beliefs. In fact, this is why most
states have Good Samaritan laws: to incentivize people to act on behalf of a
fellow human being in peril even though they may have no legal duty to do so.
Can the medic’s employer be held liable for the medic’s failure to act?
They possibly can in the court of public opinion, but not in tort law. If the
agency is dispatched to respond, of course,
that’s a different story. But her employer
cannot be held liable simply because an off-
duty employee decided not to render aid as
a bystander.
What are the liability ramifications in this
case if the medic does choose to act and provides care to the patient? Can
the medic be held liable? Can her employer? Let’s start with the medic herself.
When she decided to act voluntarily, most states’ laws would hold her liable
only for harm that resulted from gross negligence, recklessness or intentional
misconduct—not for acts of ordinary negligence. (Gross negligence vs. ordinary
negligence is a threshold issue that is typically decided by the judge before the
case goes to trial.)
Some individual EMS providers choose to carry personal liability insurance
to address concerns about personal liability, though in truth it’s quite rare for
an EMS provider to have to pay out of their own pocket in a tort case. (In fact,
we haven’t encountered it in our nearly 20 years in the practice of law.)
Lastly, what is the liability of the medic’s employer if the medic chooses to
act, in her uniform, while off duty? That is a bit more complex. If the employer
has a policy (or even an unwritten expectation communicated to employees)
making it a job requirement to provide off-duty care as a bystander, then it
can possibly be held liable, because any errors or omissions committed by the
medic would then likely be found to have occurred in the course and scope
of her employment. However, in our experience, it’s unlikely (and inadvisable)
for an EMS agency to have such a policy, which means the agency itself could
most likely not be held liable for any acts or omissions committed by one of
its employees off duty.
The concept of a legal duty to act is a basic principle of tort law, and is the
threshold issue in determining whether an EMS provider can face liability for
their acts or omissions.
Pro Bono is written by
attorneys Doug Wolfberg
and Steve Wirth founding
partners of Page, Wolfberg &
Wirth, a national EMS indus-
try law firm. Visit the firm’s
website at
www.pwwemslaw.com.
Check out the most interesting and bizarre cases at jems.com/case
1303JEMS_18 18 2/26/13 3:33 PM

H M d JEMS / / PM
QUICK TAKEAWARD WINNERSFireEMS blogger, JEMS sister sites gain recognitionFire/EMSBlogs blogger Michael Morse,
who pens the Rescuing Providence blog,
was one of three Rhode Island writers
who received the prestigious MacColl
Johnson Fellowships from the Rhode
Island Foundation. Morse, who was one
of three writers to receive $25,000, writes
about his work as an EMT/firefighter
with the Providence Fire Department at
http://rescuingprovidence.com.
Two JEMS sister publications were
named Jesse H. Neal Awards com-
petition finalists. The Law Officer
Facebook page is up for Best Use of
Social Media, and FirefighterNation.
com is being considered for Best
Website. The American Business Media
considers the Neal Awards the indus-
try’s most prestigious and sought-after
editorial honors.
John P. Pryor, MD, FACS, former
trauma program director for the
Hospital of the University of Penn-
sylvania in Philadelphia, JEMS author
and JEMS Editorial Board member,
was killed by an enemy mortar
round in Mosul, Iraq on Christmas
morning of 2008. This posthu-
mous biography, penned by John’s
younger brother, Richard, is a mov-
ing and in-depth look into the life
of an EMT turned trauma surgeon.
It provides a rarely written view
of the motivation and dedication
behind heroic behavior.
John Pryor’s journey began as a humble EMT in
upstate New York. Like many JEMS readers, an inner
voice compelled John to serve his fellow man. Ulti-
mately, he decided that he wanted to be a surgeon.
This seemingly impossible dream led him to Grenada
in the Caribbean, Buffalo, N.Y., and Philadelphia as well
as onto the pile at the World Trade Center on Sept. 11,
2001. Reading this book helps one realize that anything
can be accomplished once you set your
mind to doing so. It’s also a powerful and
sometimes painful insight into the costs
involved in achieving these dreams.
Alright, Let’s Call it a Draw is an elo-
quently detailed compilation of stories
and incidents that became the pivotal
moments in the life of Dr. John Pryor. It
details the life events that made him a
man of conviction, a man of integrity, and
a family man. This book reveals the unique
characteristics of John’s life that resulted
in an exceptional individual whose family,
colleagues, friends and all who knew him
would ultimately be proud of.
Every EMS provider will see a little bit of themselves in
the life of John Pryor. Anyone who ever wondered what
medical school is like will gain an inside perspective. This
book is a must read for every emergency services pro-
vider. You won’t be able to put it down. To obtain a copy,
go to www.drjohnpryor.com.
—Mike McEvoy, PhD, REMT-P, RN, EMT-P
& A.J. Heightman, MPA, EMT-P
BOOK REVIEWAlright, Let’s Call it a Draw: The Life of John PryorBy Richard (and John) Pryor, based on the life and death of John Pryor, MD
Choose 20 at www.jems.com/rs
1303JEMS_19 19 2/26/13 3:33 PM

It’s final! In June 2011, the U.S. Supreme
Court upheld the Patient Protection and
Affordable Care Act (PPACA), com-
monly known as Obamacare. This past
November, President Barack Obama won
reelection and Democrats maintained a
majority control of the Senate. Any hopes
Republicans had of repealing the law went
away with those two opportunities. By the
end of Obama’s second term, many of the
PPACA’s core components will have been in
effect for three years or more. There’s really
no turning back; healthcare as we know it is
going to change.
The healthcare bill was 2,733 pages long
and EMS is only referenced a few times in the
document. But the effect on EMS will be dra-
matic. I suspect that many EMS systems will
look totally different in 10 years.
I know; you’ve heard this rhetoric before.
About 15 years ago, we heard that managed
care organizations would be the “gatekeep-
ers” that would keep people from unneces-
sarily calling 9-1-1 to go to an emergency
department (ED). We heard that call centers
for insurance providers would properly eval-
uate the caller and route them to the appro-
priate level of care instead of calling 9-1-1.
Those changes largely failed to materialize.
CHANGES TO MANAGED CARE
The problem with managed care is that it
was mainly an effort by some insurance
providers to control costs and profits, and
it was voluntary. The PPACA will be legally
required. Besides the 2,733 pages of the bill
itself, more than 14,000 pages of federal reg-
ulations have already been written.
In addition, the PPACA is partially funded
through tax reforms (e.g., a 2.3% tax on med-
ical devices costing more than $100). Expect
those manufacturers to pass that cost on
to you when you purchase devices costing
more than $100.
Although nobody truly knows how these
changes will affect healthcare, there’s one
thing we can be sure of: People are still
going to get shot, have heart attacks at the
ball game and get into auto accidents going
home from work. Our 9-1-1-based EMS sys-
tems will still be needed to address such
medical emergencies.
What’s most likely to change for EMS
is how we deal with chronically ill patients
who call 9-1-1 because they have waited
too long to address their medical problem
or because they lack health insurance and
use the ED as an entry into the healthcare
system to address their problem. For Medi-
care patients, these needs will most likely be
met through accountable care organizations
(ACOs), which are just starting to form.
The main function of an ACO is to moni-
tor and control reimbursements for health-
care providers while also monitoring the
quality of the care being provided. The
PPACA allowed for the establishment of a
Medicare Shared Savings Program (MSSP),
which allows for ACOs to contract with
Medicare. Under this type of scenario, the
ACO would need to be totally responsible
for the quality, cost, care and management of
at least 5,000 Medicare recipients.
An ACO can deny or reduce payment if
the provider isn’t meeting quality standards.
For example, reimbursement can be
denied when a patient is readmitted
to a hospital within three days for the
same problem. It’s therefore in that
hospital’s interest to make sure the
patient doesn’t get readmitted for the
same problem.
How does this affect EMS? To avoid such
readmittals and other quality of care issues,
hospitals may partner with the local EMS
system to perform a variety of services.
These can include checking on the patient
with home visits for the first three days, or if
complications arise, transporting the patient
to another level of care.
START PREPARING NOW
EMS managers should prepare now for the
changes that are coming. As patients with
insurance are moved to management sys-
tems and existing Medicare patients are
moved to ACOs, prepare for initial call load
increases. This should be followed by a level-
ing-off period. Start meeting with your local
hospital administrators to discuss partner-
ships that can come about with the imple-
mentation of the PPACA.
As the saying goes, “Chance favors the
prepared mind.” EMS systems that start
preparing for the long-term impacts of the
PPACA will no doubt reap the benefits.
IMPACT AHEADObamacare will transform future EMS systems
LEADERSHIP SECTORPRESENTED BY THE IAFC EMS SECTION
>> BY GARY LUDWIG, MS, EMT-P
Gary Ludwig, MS, EMT-P, is a deputy
fire chief with the Memphis (Tenn.) Fire
Department. He has 30 years of fire and
rescue experience. He’s chair of the EMS
Section for the International Association of Fire
Chiefs and can be reached at www.garyludwig.com.
20 JEMS MARCH 2013
GLOSSARY
The main function of an Accountable
Care Organization (ACO) is to monitor
and control reimbursements for health-
care providers while also monitoring the
quality of the care being provided. The
PPACA allowed for the establishment
of a Medicare Shared Savings Program
(MSSP), which allows for ACOs to con-
tract with Medicare. Under this type of
scenario, the ACO would need to be
totally responsible for the quality, cost,
care and management of at least 5,000
Medicare recipients.
PHO
TO
ALL
KIN
DZ
A/
IST
OC
KPH
OT
O.C
OM
1303JEMS_20 20 2/26/13 3:35 PM

Choose 21 at www.jems.com/rs
1303JEMS_21 21 2/26/13 3:35 PM

TRICKS OF THE TRADECARING FOR OUR PATIENTS & OURSELVES
>> BY THOM DICK, EMT-P
22 JEMS MARCH 2013
I survived a grade-school envi-
ronment where academic failure
meant physical pain. My teacher
would command me to put my hands
on my desk, and she would play rap
music on them with a maple pointer.
And that was nothing, compared to
what awaited me at home when my
dad returned from work.
My crime: not “applying” myself.
Nothing less than a B would do,
because in Pop’s view, non-achieve-
ment meant lack of effort.
Looking back, I don’t recall my
slightly neurotic teachers enjoying
their work any more than I did mine.
And not surprisingly, they sucked at it.
I loved auto shop, though; got straight
As in auto shop. Auto shop, music and writ-
ing. Grew up with Rochester QuadraJets,
235 and 327 Chevy engines, and VW bugs.
Listened to the Wolf Man every night, play-
ing Patsy Cline, Gene Pitney, The Righteous
Brothers, Motown, and later The Beach
Boys and Beatles. Idolized Walter Cronkite
and dreamed of being him someday. Then
in 1970, as a young journalism student, I
found a job as an ambulance attendant. I
instantly recognized my calling in life. Of
course, if you worked for an ambulance ser-
vice in those days, it was probably a small
one. And in small organizations, everybody
does more than one job.
One of my jobs between calls was man-
aging a fleet: tracking the licenses, buying
the batteries, checking the tires and log-
ging the maintenance. I was untaught, so I
made a lot of mistakes. But I loved ambu-
lances, and I learned a ton about what
makes them safe and reliable. I take care of
a fleet to this day.
There are two kinds of vehicle failures,
Life-Saver. One is the kind that takes you
out of service immediately. Most agencies
call those critical failures. The other kind, a
non-critical failure, needs to be fixed none-
theless. But it won’t keep you from run-
ning a call.
As you know, an ambulance can either
earn you a living or kill you on any day of
your career. It can kill other people, too. To
operate, it needs to be able to start, steer,
stop and stay running. It also needs to pro-
vide a stable interior environment, and its
safety restraints need to work. You don’t
need a mechanic or a supervisor to tell you
when any of those systems fails; and when
they do, you’re like a pilot. Nobody gets to
argue with your decision to put yourself
out of service.
I’ve learned to see critical failures not
just as events that prevent you from run-
ning calls, but as events that could pre-
vent you from running calls. So, an engine
that cranks hard or leaks fluids needs to
be taken out of service. So does a tire that
reveals excessive or unusual wear.
In fact, your ambulance will almost
always warn you before it fails. So you
probably deserve to understand how
it works and what it’s telling you.
Mechanical education is partly
your agency’s responsibility and
partly yours. Given your access to
the Internet, there’s no reason why
you shouldn’t know some of the
same stuff your vehicle tech knows. For
instance, that a cracked windshield can
defeat your airbag restraints. That your
late-model diesel depends on a sup-
ply of urea (and why). And that if
you’re having steering issues, the first
thing you should wonder about is
the air pressure in your tires. Think
of it the way you think about anat-
omy and physiology.
By far, the most common kinds of
critical failures I’ve seen are failures
to start. It turns out, they’re also the
easiest to prevent—partly by crews
who understand their instruments,
and partly by proactive agencies
that adhere to scheduled preventive
replacement of their batteries.
The thing about batteries is they
all eventually fail. A good commer-
cial ambulance-sized battery should cost
about $200, and the average ambulance
has two of those. They should be replaced
about once a year (even if they work just
fine), they should be protected from rapid-
charging, and their connections should be
kept tight and squeaky-clean. You know
what they’ll cost, so you can budget for
their replacement.
Now let’s think about the consequences
of a failure. When a battery fails, it’ll typi-
cally do so when you least expect it to.
You can’t project what it’ll cost. A pair of
dead ones is too big to jump-start, they
place unacceptable stress on alternators,
they generate towing bills and they’re sur-
rounded by three-sided billboards that
say “we screwed up.” And worst of all,
they interrupt our basic mission of help-
ing sick people.
Don’t think this is important? OK, Life-
Saver. Put your hands on the table
in front of you. ...
BATTERIESPreventing failures we can’t afford
Thom Dick has been involved in EMS
for 41 years, 23 of them as a full-time
EMT and paramedic in San Diego County.
He’s currently the quality care coordina-
tor for Platte Valley Ambulance, a hospital-based
9-1-1 system in Brighton, Colo. Contact him at
Batteries eventually fail, no matter what we do. Preventing failures to start is the key to making sure those failures don’t harm a patient.
PH
OT
O T
HO
M D
ICK
1303JEMS_22 22 2/26/13 3:35 PM

ADVANTAGE:
CPAP SYSTEM CONSUMES
50% LESS OXYGEN
CPAP conserves oxygen while
maintaining high FiO2 delivery
Increasing flow may be necessary when activating the nebulizer.
ADVANTAGE:
BUILT-IN
MANOMETER
& PRESSURE RELIEF VALVE
ADVANTAGE:
INTEGRATED NEBULIZER
Offers the capability of an in-line nebulizer.
∙ Uses only one oxygen supply source
∙ Easy Set-Up, Less Parts.
Neb
OffNeb
On
www.mercurymed.com
Visit Mercury Medicalʼs Booths #1431 & #1432 at the
2013 EMS Today Conference & Expo
Walter E. Washington Convention Center
Washington, D.C.
March 7 - 9, 2013
∙ CPAP & Nebulizer in One System ∙ Less Parts, Easy Set-Up
∙ Only One O2 Source
SAFE, SURE,SUPERIOR CPAP.
ADVANTAGE:
ADVANCED MASK DESIGN
∙ Quick Disconnect Clips
∙ Straight Rotating Port
∙ Soft Forehead Padding to reduce pressure on nose.
NEW DESIGN
EZ
A REVOLUTION IN EMERGENCY CARE
Clinicians can deliver aerosol & CPAP therapy with Only One oxygen source.
With so many advantages, it clearly puts you at an advantage.
Choose 22 at www.jems.com/rs
1303JEMS_23 23 2/26/13 3:35 PM

It’s 2 a.m. on a Friday night and a
medic unit responds to a call of a
“pedestrian struck.”
On arrival, city law enforcement declares
the scene to be safe and directs the unit to
the opposite shoulder of the highway. EMS
providers find a 35-year-old male lying in
the prone position with a moderately dam-
aged mountain bike beside him.
ASSESSMENT & TREATMENT
The patient says he was riding home from
his friend’s house when he got “bumped” by
a passing car, hit a pothole and fell forward
off his bike. Although his breath indicates
recent alcohol intake, he’s able to answer
questions in a moderately slurred voice.
Initially the patient refuses medical evalu-
ation and transport to the hospital, but the
medics are able to convince him otherwise.
The airway is intact with no debris or
blood, and breath sounds are equal bilat-
erally. His respiratory rate is 22 and pulse
oximetry 96% on room air.
A cervical collar is placed on the patient,
and he is log-rolled and secured onto a
backboard. The heart rate is found to
be 110 mmHg with a blood pressure of
136/92. His helmet has an abrasion to the
front but is otherwise intact.
Your trauma exam is notable for a 2x3
cm round-shaped wound to the mid-
line epigastric region, just inferior to the
xiphoid process, with moderate non-pul-
satile bleeding. You note that when the
patient exhales following a deep inspira-
tion, there’s a small bulge in the wound
that subsequently resolves with the fol-
lowing inspiration. No air movement or
bubbling from the wound is detected.
The abdomen is mildly distended with
moderate diffuse tenderness and there are
multiple partial thickness abrasions to the
bilateral elbows, hands and lower extremi-
ties. Although he’s clinically intoxicated, his
Glasgow Coma Scale (GCS) is determined
to be 15.
Once in the mobile unit, you place the
patient on 4 lpm oxygen via nasal can-
nula and a cardiac monitor. You secure a
sterile abdominal gauze pad over the open
abdominal wound.
The total scene time is 12 minutes, and
transport time to the local trauma center
is 20 minutes. You place an 18-gauge IV
in the patient’s right antecubital fossa and
administer 500 ccs of normal saline en
route. The dressing controls the bleeding
from the abdominal wound, and there’s
no significant clinical change in the patient
during transport.
TRAUMA CENTER CARE
On arrival to the trauma center, the trauma
team repeats the primary and secondary
surveys. Vital signs arenít significantly
changed: Heart rate is 112, respiratory rate
is 18, blood pressure is 132/88, and pulse
oximetry is 100% on room air. The trauma
team also performs a focused assessment
with sonography for trauma (FAST) exam,
which demonstrates a small amount of free
fluid in the right upper quadrant, specifi-
cally Morrisonís pouch.
A FAST exam, which is regularly per-
formed during a trauma survey, uses four
different locations to place the ultrasound
and screen for free fluid in 10 distinct poten-
tial spaces. Free fluid, often blood in the
traumatic patient, is a strong indicator of
significant abdominal or thoracic injury, and
the FAST exam allows early identification of
these patients in order to expedite surgical
intervention. Morrison’s pouch is a potential
space between the inferior aspect of the liver
and superior aspect of the right kidney. It
is recognized as the most likely location to
identify free fluid associated with a serious
intra-abdominal injury.
Given the stable vital signs, a CT scan of
the head, cervical spine, chest, abdomen
and pelvis is performed to fully evaluate
the injuries. The CT scans demonstrate
FORWARD FALLGet a handle on handlebar injuries
CASE OF THE MONTHDILEMMAS IN DAY-TO-DAY CARE
>> BY MICHAEL ORLAND, MD
24 JEMS MARCH 2013
A deep breath by the patient produces a small bulge in the ring-shaped wound, indicating traumatic abdominal hernia.
PH
OT
OS C
OU
RT
ESY
ED
WA
RD
T. D
ICK
INSO
N
1303JEMS_24 24 2/26/13 3:59 PM

Choose 23 at www.jems.com/rs
1303JEMS_25 25 2/26/13 4:00 PM

CASE OF THE MONTH>> CONTINUED FROM PAGE 24
26 JEMS MARCH 2013
a 2 cm anterior abdominal wall hernia
at the site of the open wound, injury to
two areas of the small bowel with likely
perforation given the surrounding small
foci of free air and a grade 2 liver lacera-
tion. The patient is immediately taken to
the operating room, where he undergoes
an exploratory laporatomy with resection
of two portions of the small bowel, suture
repair of the liver laceration and primary
repair of the abdominal hernia with mesh.
His post-operative course is uneventful,
and the patient is discharged to home one
week later.
DISCUSSION
At first glance, a fall from a bicycle can
often be mistaken as a non-significant
mechanism. As is often the case with lat-
eral falls, a low level of energy is being dis-
tributed to a large area of the body or to an
extremity. However, forward falls from a
bicycle are frequently higher energy, which
is distributed to a smaller area of the body.
More specifically, the body can be
struck in the chest or abdomen by the
handlebars or the head by the ground or
stationary object. This focused impact in
combination with increased abdominal
pressure as a result of the initial impact of
the bicycle places the patient at significant
risk of injury to the abdominal wall and
anterior abdominal organs, including the
liver, spleen, stomach, bladder, colon and
small bowel. Therefore, any patient who
falls at a high rate of speed or falls forward
off of a bicycle should be considered to
have suffered a significant mechanism of
injury and treated as such.
Blunt traumatic injuries from a bicycle
handlebar are more common in the pedi-
atric population. A two-year retrospective
chart review at a major children’s hospital
found an average age of 8.8 years for this
injury, with 79% of patients in this popula-
tion being boys. Of the 14 patients who
presented for evaluation to the ED, 11 had
a ring-shaped ecchymotic area noted in the
abdomen with a variety of lacerations and
abrasions. After evaluation, it was found
that 21% had an intestinal perforation and
21% had an abdominal wall hernia, as
large as 5 cm.1 In the multiple case reports
published, traumatic abdominal wall her-
nias due to a handlebar injury more often
occur in the lower abdomen and appear
as a ring- or circular-shaped ecchymosis,
abrasion or open wound.
In the pediatric population, a handlebar
injury is the most common cause of a trau-
matic abdominal hernia and isn’t a reliable
indicator for more significant traumatic
injuries. In contrast, seatbelt trauma in a
motor vehicle collision is the more fre-
quent mechanism for abdominal hernias
in adults and is almost always associated
with other significant injuries.2
Clinically, a traumatic abdominal wall
hernia will appear as a discrete bulge on
abdominal exam that may expand and
reduce with a change in abdominal pres-
sure or remain constant. It’s important to
recognize this clinical sign and its associa-
tion with significant traumatic injuries, but
no other specific care should be performed
except for a sterile dressing application to
any open wounds. Application of manual
pressure or compression of any kind to the
mass isn’t advised because it may exacer-
bate other injuries.
CONCLUSION
In this case, the ALS unit provided prompt
and efficient care for their trauma patient;
starting with airway, breathing and circula-
tion (ABCs), and proceeding through spinal
immobilization and secondary examina-
tion. They recognized the significant mecha-
nism and were able to persuade the patient
to receive the care he required. Large-bore IV
access was obtained, fluid resuscitation was
initiated and appropriate wound care was
provided—all while expediting transport to
a trauma facility.
In summary, falling forward onto a bicy-
cle places a patient at risk of a handlebar
injury and should be considered a signifi-
cant traumatic mechanism that may cause
serious abdominal injuries with no major
outward signs of trauma on exam. A trau-
matic abdominal wall hernia will appear
as an area of ecchymosis or small wound
with an underlying bulge. Although this
doesn’t require specific care, it should be
recognized as a significant injury. In adults,
it may indicate additional serious abdomi-
nal injuries. As such, these patients should
be transported expeditiously to the closest
trauma center.
Michael Orland, MD, is a resident physician in emer-
gency medicine at the Hospital of the University of
Pennsylvania and a former EMT with the Pennington
First Aid Squad. He can be reached at Michael.Orland@
uphs.upenn.edu.
REFERENCES
1. Karaman I, Karaman A, Aslan M, et al. A hidden dan-
ger of childhood trauma: Bicycle handlebar injuries.
Surg Today. 2009;39(7):572–574
2. Haimovici L, Papafragkou S, Kessler E, et al. Handle-
bar hernia: Traumatic abdominal wall hernia with
multiple enterotomies. A case report and review of
the literature. J Pediatr Surg. 2007;42(3):567-569.
This CT scan demonstrates a 2 cm anterior fascial defect and associated abdominal wall hernia at the site of the open wound.
IMA
GE C
OU
RT
ESY
ED
WA
RD
T. D
ICK
INSO
N
1303JEMS_26 26 2/26/13 4:00 PM

Choose 24 at www.jems.com/rs
1303JEMS_27 27 2/26/13 4:00 PM

28 JEMS MARCH 2013
PH
OT
O B
Y C
HR
IS S
WA
BB
1303JEMS_28 28 2/26/13 4:01 PM

WWW.JEMS.COM MARCH 2013 JEMS 29
TIME FOR A CHANGE
rehospital spinal immobilization has long been
held as the standard of care for victims of blunt
or penetrating trauma who have experienced a
mechanism of injury (MOI) forceful enough to
possibly damage the spinal column. The majority
of EMS textbooks stress that any significant MOI, regardless of
signs and symptoms of spine injury, requires full-body immo-
bilization, which is typically defined as a cervical collar being
applied and the patient being secured to a backboard with head
stabilizers in place.
This approach to patient immobilization has been accepted
and implemented as the standard of care for decades with little
scientific evidence justifying the practice.1–3 In addition, scant
data shows that immobilization in the field has a positive effect
on neurological outcomes in patients with blunt or penetrating
trauma.1,4–6 In fact, several studies and articles show that spine
immobilization may cause more harm than good in a select
sub-set of trauma patients.5–7
Many experts question the current practice of prehospital
spinal immobilization.1,2,4–15 There are now some guidelines,
textbooks and an increasing number of EMS agencies that sup-
port a progressive, evidence-based approach in an effort to
lessen unnecessary spinal immobilizations in the field.
It’s problematic to use MOI alone as the key indicator for
prehospital spinal immobilization. In addition, the harmful
sequelae and potential dangers of spine immobilization need
to be considered in any field protocol. We need to examine
appropriate spine injury assessment guidelines and algorithms
that allow for the selective immobilization of injured patients.
We also should review immobilization devices and tech-
niques that are more appropriate for patients who do require
immobilization, or better termed, spinal motion restriction
(SMR), by EMS providers.
OUTDATED INDICATORS?
It typically takes several years for EMS textbooks to catch
up with new evidence and then additional time for the EMS
instructional community to modify curricula and change cur-
rent practice. For example, definitions of mechanisms that
require spinal immobilization found in most EMS textbooks
are outdated and problematic. Such indicators for potential
spine injury as fall, damage to the vehicle, injury above the clav-
icle and mechanism of injury involving motion, are not par-
ticularly helpful when determining the best course of action
in the field.
Especially troubling has been the lack of emphasis on the
assessment of the patient before making a decision about
immobilization. Historically, more emphasis has been placed
on what happened to the vehicle or the best guess on how far
someone may have fallen, instead of what actually happened
to the person.
It isn’t the fall that causes injury; it’s the sudden stop at
the end. The more sudden the stop, the more likely an injury
results, especially if the kinetic energy was transmitted to the
head and/or neck.
The physical condition of the patient must also be consid-
ered. A young, athletic person is able to withstand more forces
than an elderly patient. So the spectrum of potential injuries is
best determined through a detailed history and physical exam.
Vehicle damage has long been considered a strong indicator
of potential spine injury, yet improvements in vehicular design
and construction should change the way we look at vehicle
damage. Vehicle technology and passenger protection is far
superior to what it has been, particularly since the 70’s when
EMS textbooks began advocating back boarding of patients in
vehicles with significant damage.
Vehicle damage zones are now inherently built into newer
r
h
o
m
p
f b
>> BY JIM MORRISSEY, MA, EMT-P
1303JEMS_29 29 2/26/13 4:01 PM

SPINAL IMMOBILIZATION>> CONTINUED FROM PAGE 29
30 JEMS MARCH 2013
vehicles, designed to absorb and dissipate
the kinetic energy of a collision, and keep
the passenger cabin relatively isolated and
protected.16 An experienced paramedic once
said, “The cake box might be crumpled, but
the cake can be fine.”
Some textbooks accurately address this
issue. Even as far back as 1990, the Amer-
ican Academy of Orthopaedic Surgeons
addressed emergency medical responders
in an extended-care environment, stating,
“Patients with a positive mechanism of injury,
without signs and symptoms, and with a
normal pain response may be treated with-
out full spine immobilization, if approved by
your medical control physician.” 17
Emergency medical personnel who work
in extended-care, tactical, combat and wil-
derness environments have long realized the
need to safely and accurately assess and clear
patients regarding spinal injuries.18,19
New guidelines from Prehospital
Trauma Life Support and the National
Association of EMS Physicians have
diminished the emphasis on immobilizing
victims of penetrating trauma without
neurologic deficits.20
In the setting of drowning, the 2010 evi-
dence-based guidelines from the American
Heart Association state that “Routine c-spine
immobilization is a Class III (potentially
harmful) unless clear trauma is evident in the
history or exam, because it may unnecessar-
ily delay or impede ventilations. ”21
PRECAUTIONARY IMMOBILIZATION
It isn’t surprising that the term and practice
of “precautionary immobilization” has devel-
oped. It’s estimated that at least five million
patients are immobilized in the prehospital
environment in the U.S. each year. Most have
no complaints of neck or back pain or other
evidence of spine injury.3,11,12 (See Photo 2.)
EMS personnel historically have neither
been given the tools nor the authority to
make informed decisions about objectively
determining the need for prehospital spi-
nal immobilization. This may be because
the emergency medical community thought
immobilization was always safe, conserva-
tive and always in the best interest of the
patient. However, evidence now shows that,
in some cases, spinal immobilization may
not be in the patient’s best interest.1–3,7,8,10–13
Some prehospital care providers will
admit that they often immobilize patients
without evidence of spine injury because
they want to avoid being questioned on
arrival at the emergency department (ED).
This dynamic can (and must) change with
education and outreach.
BACKBOARD-BASED IMMOBILIZATION
In addition to patient discomfort and anxi-
ety associated with backboard-based immo-
bilization, there are several potentially
significant consequences. Standard immo-
bilization requires the patient’s body to con-
form to a flat, hard surface. In addition, EMS
secures a cervical collar around the patient’s
neck and uses tape to secure the patient’s
head to the board.
This practice often increases patient
anxiety and has the potential to aggravate
underlying injuries. Standard spinal immo-
bilization techniques can also take away the
patient’s ability to effectively protect their
own airway thus significantly increasing the
risk of aspiration.3–6,11,13
Patient vomiting, bleeding, airway drain-
age and swelling are common problems
associated with trauma patients. Even with
one EMS provider dedicated to the manage-
ment of the airway and patient suction, it
cannot be assumed that a suction catheter
can handle the job when significant bleeding
and/or vomiting is presented.
The continued spinal stability of a patient
who is turned on their side to facilitate airway
drainage and control is also questionable.
Patients typically experience a significant
There are many situations (hostile environment, life threatening injuries) where spinal immobiliza-tion may be detrimental to good patient care. This training scenario emphasizes rapid extrication.
PH
OT
O C
OU
RT
ESY
JIM
MO
RR
ISSEY
/JO
SH
KEN
NED
Y
Assessment is still the key to determining the need for spinal immobilization.
PH
OT
O A
.J. H
EIG
HT
MA
N
1303JEMS_30 30 2/26/13 4:01 PM

Choose 25 at www.jems.com/rs
Choose 26 at www.jems.com/rs
1303JEMS_31 31 2/26/13 4:01 PM

32 JEMS MARCH 2013
shift in body weight and distribution, causing more movement to
the spine than the immobilization process was intended to prevent.
In a comprehensive review published in Prehospital and Disas-
ter Medicine, healthy volunteers who were immobilized on a back-
board were found to be “significantly more likely to complain of
pain when compared with immobilization on a vacuum mattress.”
Adverse effects of backboard-based immobilization documented in
this study include increased ventilatory effort, pain and discomfort.
In addition to pressure injury, the backboard may also be the
cause of pain—even in otherwise healthy volunteers. The resultant
posterior surface/back pain of immobilized patients has been docu-
mented to result in unnecessary radiographs and potential clinical
ambiguity regarding the cause of the pain.3,22 There’s an increased
cost associated with some of these complications.
It has been documented that supine patient immobilization
results in a 15–20% reduction in respiratory capacity, and that respi-
ratory effectiveness is markedly reduced by the strapping systems
typically used.3,9,13 Patients are often either strapped securely, thus
having diminished respiratory capacity, or loosely secured, facilitat-
ing easier breathing. Neither scenario is ideal.
The challenge is exacerbated in obese patients, the elderly and
patients with such underlying diseases as congestive heart failure,
COPD, asthma and pneumonia.
Done properly, immobilization in the field takes time and mul-
tiple personnel. Time delay to the ED or trauma center arrival has
been cited as a significant problem for critical trauma victims. Sev-
eral studies have looked at the risk vs. benefit of prehospital immo-
bilization, with several authors and researchers questioning the
value of current practices.1,2,7,8,11,15
SPINAL IMMOBILIZATION>> CONTINUED FROM PAGE 30
Patients with penetrating trauma (ex., gunshots and stabbings) to the head and torso usually do not benefit from spine immobilization.
PH
OT
O C
OU
RT
ESY
JIM
MO
RR
ISEY
/JO
SH
KEN
NED
Y
Choose 27 at www.jems.com/rs
1303JEMS_32 32 2/26/13 4:01 PM

WWW.JEMS.COM MARCH 2013 JEMS 33
Studies have also shown limited or no benefit of prehospital
immobilization of penetrating trauma patients. (See photos on
pages 32 and 33.) Unnecessary immobilization of this subset of
trauma patients can result in prolonged on-scene time and delayed
transport to definitive care, which may increase morbidity and
mortality.4–6,14,18,23–25
Several studies show that cervical collars by themselves aren’t
without risk or significant consequences.4,26–28 One study concludes
that cervical collars frequently increase intracranial pressure and
may be particularly harmful if used on head-injured patients.26
Another researcher observed that cervical collars “can result in
abnormal distraction within the upper cervical spine in the pres-
ence of severe injury.”28 In addition, cervical collars hide areas of
the head and neck, resulting in the increased possibility of missing
injuries or evolving problems, such as swelling, hematoma and
tracheal deviation.27,28
In addition, the longer a patient is immobilized, the more likely
that cutaneous pressure ulcers will develop, most notably in the
occipital, sacral or heel areas.9,12,22,29,30 This is especially true in elderly,
unconscious and neurologically impaired patients. This problem
may be significantly reduced with padding or use of a vacuum
mattress. Unfortunately, the vast majority of the patients who are
immobilized don’t get padding in voids or areas of significant body
weight/pressure or a vacuum mattress that distributes beads/pad-
ding in voids and uneven body surface areas.
THE PENETRATING TRAUMA PATIENT
As referenced earlier, there is a growing body of evidence that sug-
gests penetrating trauma victims shouldn’t be routinely immobi-
lized. Immobilization has been associated with higher mortality in
patients with penetrating trauma.4–6,14,23–25
Independent studies show that whether the penetrating trauma is
to the head, neck or torso, immobilization is unnecessary, interferes
Tactical teams often use compact, flexible extraction devices.
PH
OT
O C
OU
RT
ESY
JIM
MO
RR
ISSEY
/JO
SH
KEN
NED
Y
Choose 28 at www.jems.com/rs
BEGIN THE CHALLENGE AT:
heart.org/acls-ep
1303JEMS_33 33 2/26/13 4:01 PM

34 JEMS MARCH 2013
with and delays emergent care, and should be seriously reconsidered
as the standard of care.4–6,14,23
A Journal of Trauma article concluded, “Indirect spinal injury
does not occur in patients with gunshot wounds to the head.” The
authors state, “Protocols mandating cervical spine immobilization
after a gunshot wound to the head are unnecessary and may com-
plicate airway management.”14
Another retrospective study showed similar concerns about the
use of a cervical collar with patients who have penetrating injuries
to the neck. This study suggests that avoiding the collar should be
the rule, and that a provider who chooses to apply a cervical collar
should have good justification. The authors also suggest that fre-
quent examination of the underlying structures and tissue is war-
ranted if a cervical collar is used.4
A comprehensive retrospective analysis of gunshot injuries to
the torso found that immobilization was of little or no benefit, even
if an unstable spine fracture was present. The authors argue that air-
way management, including intubation, is far more complicated
and problematic with prehospital spinal immobilization in place.5,6
In fact, failed airway management was reported to be the second-
leading error preceding death of trauma patients, accounting for
16% of mortality in one study. This study also highlights the poten-
tial delay to definitive surgical treatment and the lack of neurologic
improvement after gunshot injury to the spinal cord, suggesting
that prehospital spinal immobilization is unjustified.5,6
PROPER SPINE INJURY ASSESSMENT
For many trauma patients, a vetted field assessment criterion that
focuses on the assessment of the patient rather than the mecha-
nism of injury would obviate unwarranted immobilization.3,11,31
Many emergency medicine specialists believe an accurate, reli-
able, simple-to-perform spinal injury assessment could reduce spine
immobilizations drastically. Thankfully, there is a trend in this direc-
tion across the nation.
The idea of “clearing” a patient of spinal injury in the field has
been, and continues to be debated. However, there are prehospital
spine assessment protocols that safely and accurately allow EMTs
and paramedics to omit prehospital spinal immobilization in cer-
tain patients.
Some EMS experts prefer the term “selective immobiliza-
tion” to “clearing” the c-spine, but the end result is the same.
The end result is the reduction of the incidence of unwarranted
spinal immobilizations.
For example, the Maine spine injury assessment guidelines,
developed by Peter Goth, MD, in the 1990s, have been shown
to be accurate and safe.10,31,32 Several states and EMS systems
around the nation use this, or a similar protocol, to help decrease
the number of trauma patients being subjected to prehospital
spinal immobilization.
The origin of this type of spinal assessment was initially intended
to help ED physicians clinically decide if they can safely clear
patients from prehospital spinal immobilization and reduce or elim-
inate unnecessary radiographic studies. It has been shown that the
proper clinical exam and history is more accurate at predicting spine
injuries than X-ray review.10,32–35
The spine injury assessment guidelines that have been adopted
SPINAL IMMOBILIZATION>> CONTINUED FROM PAGE 33
AIRPOWER® R8
Lower profile zipper Station/EMS boot
> Built in Arch Support
> Steel toe protection
> Chemical/bloodborne
pathogen protection
> Waterproof & breathable
Quality shoes for law enforcement, fire
and rescue services, hunting, work wear,
and leisure time
HAIX® North America Inc.
2320 Fortune Drive, Suite 120,
Lexington KY 40509
Phone 859-281-0111,
Fax 859-281-0113,
Toll free 866-344-HAIX (4249)
www.haix.com
Visit us at
EMS TODAY
Booth 1049
Choose 29 at www.jems.com/rs
1303JEMS_34 34 2/26/13 4:01 PM

WWW.JEMS.COM MARCH 2013 JEMS 35
by multiple prehospital systems are based on the Canadian C-spine
rule and the National Emergency X-Radiography Utilization Study
(NEXUS) low-risk criteria. Each has similar parameters, requiring
that the patient be awake, alert, conversant and without significant
distracting injury or intoxication.
In addition, the guidelines further state that the physical exam
should reveal no pain or tenderness to the posterior neck and back
and the neurologic exam must find normal motor and sensory func-
tion in the extremities.10,18,31,33–35
Studies show that prehospital care providers can safely apply
spine injury assessment criteria and not miss any clinically
significant spine injuries.10,31,32 Although these guidelines are
PH
OT
O C
OU
RT
ESY
JIM
MO
RR
ISEY
/JO
SH
KEN
NED
Y
Some patients, such as pediatric patients, require special spinal immo-bilization consideration.
Children have been immobilized acceptably in specialized spinal devices for decades.
PH
OT
O C
HR
IS S
WA
BB
Choose 30 at www.jems.com/rs
1303JEMS_35 35 2/26/13 4:01 PM

SPINAL IMMOBILIZATION>> CONTINUED FROM PAGE 35
36 JEMS MARCH 2013
available, training and practice is needed to
become proficient at using these criteria.
Alameda County (Calif.) EMS has revised
its spine injury assessment protocol to
accurately reflect the current literature and
research. (See Figure 1, p. 38). Its goals in
2012 were to reduce unnecessary immobili-
zation, and use treatment modalities in the
best interest of and provide the most comfort
to the patient. In some cases, this meant for-
going prehospital spinal immobilization to
expedite transport to a trauma center.
However, long-established norms are
hard to break, and extensive training was
required to make this new policy success-
ful. EMS schools, fire departments and other
EMS providers, as well as emergency depart-
ment staff, needed to be exposed to the litera-
ture and trained in the new protocol. Initial training and outreach has been
well received and the early indicators have
shown a significant reduction in spine
immobilizations. The end result is:
>> A better understanding of the need
for expeditious care under specific cir-
cumstances, in particular, the need
to move rapidly when penetrating
trauma is present;
>> All involved are empowered to break
the paradigm of “board them all” as
a result of understanding the impor-
tance of proper spinal/neurological
assessment and assessment parame-
ters that allow crews to assess for seri-
ous spinal indications and perform
selective immobilization. We did the
same process decades ago when we
adopted rapid removal techniques for
patients in lieu of spending precious
minutes placing splints and half back-
boards on critical patients. Little or no
untoward results occurred with that
change in procedure;
>> More attention to patient comfort and
pain instead of routine placement of
trauma patients on a hard, uncomfort-
able platform that often put them in
anatomically-incorrect positions for
extended time periods, made patients
unnecessarily claustrophobic lying
supine and immobile and exacerba-
tion of respiratory distress in patients
due to the supine position, strap place-
ment, and existing conditions such as
CHF, COPD or morbid obesity; and
>> The ability to deploy and maximize
the usage of alternative immobiliza-
tion and transfer devices and stretch-
ers such as vacuum mattresses, scoop
or CombiCarriers and flexible stretch-
ers such as Ferno and SKED stretchers
and others that feature lateral patient
support slats and multiple handles for
convenient movement and transfer
of patients. Many of these devices are
better suited to patient movement in
tight spaces and crew body mechan-
ics when carrying and transferring
patients down stairways and other dif-
ficult environments.
Of course, crews have to take special
caution when dealing with and manag-
ing high-risk patients, including pediatric
patients, the elderly and those with such
degenerative bone disorders as osteopo-
rosis. Field personnel need to be conser-
vative while evaluating these patients and
should provide spinal motion restriction
when in doubt.33,34
UNCONVENTIONAL OPTIONS
Even with appropriate application of spine
injury assessment guidelines, some patients
still require some degree of prehospital spinal
motion restriction. Vacuum mattresses and
other break-away and flexible stretchers have
been used successfully throughout Europe
for years. They score well in several criti-
cal areas, including patient comfort, secure
immobilization, insulation, lack of pressure
A vacuum splint can be used as a highly moldable and comfortable cervical immobilization device.
PH
OT
O A
.J. H
EIG
HT
MA
N
This patient is securely immobilized in a FERNO Germa Easyfix vacumm mattress – stretcher.
Vacuum mattresses and stretchers pad voids and distribute a patient’s weight evenly.
Patients can be immobilized safely and comfortably via a combination of a backboard or other flexible or scoop-type stretcher, such as shown here with a Hartwell Combi-Carrier/vacuum mattress combination.
PH
OT
O A
.J. H
EIG
HT
MA
N
PH
OT
O A
.J. H
EIG
HT
MA
N
PH
OT
O E
D D
OER
R
1303JEMS_36 36 2/26/13 4:01 PM

Choose 31 at www.jems.com/rs
Visit www.HealthEMS.NET or call 877.506.2747 for Demo
#1 EMS Software as a Service (SaaS) Solution – Over 25% Top EMS Agencies Use HealthEMS®
Sansio 11 East Superior Street, Suite 310 Duluth, MN 55802
HealthEMS® Mobile• Industry–Leading ePCR
Secure field data collection using your hardware of choice
• HealthEMS® FlexFields Unique functionality creates customized ePCR
• HealthEMS® Integrates to CAD and EKG
Wireless data exchange eliminates manual entry improving accuracy
• HealthEMS® XchangER
Two-way wireless communication of ePCR data to/from hospital
HealthEMS® EHR• Industry-Leading EHR Advanced QA solution supports CQI
• HealthEMS® Xchange NEMSIS Gold compliant, v3 development in process
• HealthEMS® is CARES Compliant;
Sansio is the IT partner of the CARES network
• myPatientEncounters™
Provides patients with secure, online access to their EHR
• EMS Web-Based Revenue Cycle Management Solution! Improved efficiency with ePCR system integrated to billing system
• Accurate/Automatic ICD-9/10 coding, medical necessity, service level, loaded mileage, eligibility checking
• HIPAA Compliant Transactions 4010/5010 electronic claims and remittances
• Complete AR Management Workload management/change management and reporting
NEW
Choose 32 at www.jems.com/rs
1303JEMS_37 37 2/26/13 4:02 PM

SPINAL IMMOBILIZATION>> CONTINUED FROM PAGE 36
38 JEMS MARCH 2013
sore development and, in the case of some
vacuum device configurations, allow crews
to utilize them without a cervical collar.12,29,30
When considering adding vacuum mat-
tresses, vacuum stretchers or other immobi-
lization devices to your arsenal, keep in mind
that they don’t require more effort or training
than using backboards. Vacuum mattresses
can also effectively pad voids, distribute
weight evenly and immobilize patients on
their side because the device can be “molded”
around the patient to best package them
safely. (See photos on page 36.)
However, keep in mind that backboards
still have a place, especially to restrain or
slide a patient out of an extrication mess.
There is also nothing that precludes you
from utilizing a combination of devices such
as a backboard or scoop-type stretcher to
remove a patient and transfer them to a
more moldable or comfortable secure sur-
face such as a vacuum mattresses. Many
systems use this combination or deploy vac-
uum mattresses in conjunction with flexible
stretchers. (See photo, top of page 36.)
Another emerging school of thought
questions the need for traditional prehos-
pital spinal immobilization at all—even for
patients who have positive evidence of a
spinal column or spinal cord injury. One
group of researchers who compared vari-
ous extrication tools and methods found
that allowing a patient to self-extricate from
a vehicle with a cervical collar alone caused
less movement of the spine than the use of
cervical collar, KED extrication device and
standard extrication techniques.36 This trig-
gers a series of questions that are beyond
the scope of this article. Groups such as the
National Association of EMS Physicians and
the U.S. Metropolitan Municipalities Medical
Directors and Global Affiliates Consortium
> Age > 65> Meet Trauma Patient Criteria
for Mechanism of Injury (Section 3)> Axial load to the head (e.g. diving injury)> Numbness or tingling in extremitiesIf any one of the high-risk factors above are present, strongly consider spinal motion restriction (SMR).
A reliable patient is cooperative, sober and alert without:
Significant Distracting Injuries Language Barrier
SPINAL PAIN/TENDERNESS Palpate vertebral column thoroughly
MOTOR/SENSORY EXAM Wrist or finger extension (both hands)
Plantarflexion (both feet) Dorsiflexion (both feet) Check gross sensation in all extremities
Check for abnormal sensations to extremities (e.g. parathesias)
Low-risk factors:> Simple rear-end MVC> Ambulatory at any time on scene> No neck pain at scene> Absence of midline cervical spine
tendernessThe low-risk factors above allow safe omission of SMR.
RELIABLE PATIENT? NORMAL SPINE EXAM? NORMAL MOTOR/SENSORY?
POTENTIAL FORUNSTABLE SPINAL
INJURY?
POSSIBLE SPINE INJURY
APPLY SMR
OMIT SMR
YES
YES
NO
Figure 1: Alameda County (Calif.) 2012 Spinal Immobilization Procedure
To obtain a copy of the complete
Alameda County Spinal Injury Assessment Procedure,
go to the web version of this article at jems.com/journal
1303JEMS_38 38 2/26/13 4:02 PM

WWW.JEMS.COM MARCH 2013 JEMS 39
are carefully discussing these options and
revisions to our traditional approaches to
neck and spine immobilization
CONCLUSIONIt’s appropriate for emergency person-
nel to immobilize certain trauma patients.
However, many other trauma patients are
unnecessarily immobilized by EMS. Spinal
immobilization isn’t always a benign inter-
vention. It can result in increased scene time,
delay of delivery to definitive care, problem-
atic airway management, increased patient
pain or dyspnea, and unnecessary radio-
graphic testing.
Many trauma patients can be safely and
accurately assessed and treated without
immobilization if they meet all criteria in
prehospital spinal assessment guidelines.
Extensive initial training and ongoing review
is necessary for an effective selective immobi-
lization protocol.
Science, research and multiple validated
articles have changed the way EMS practices.
If good patient care is the goal, it’s time that
prehospital spinal immobilization be criti-
cally examined.
Jim Morrissey, MA, EMT-P, is the terrorism preparedness
coordinator for Alameda County (Calif.) EMS. He is a tacti-
cal paramedic for the San Francisco FBI SWAT team, and
a medical intelligence officer for the Northern California
Regional Intelligence Center. He holds a master’s degree in
homeland security from the Naval Postgraduate School.
He can be reached at [email protected].
REFERENCES1. Hauswald M, Ong G, Tandberg D, et al. Out-of-hos-
pital spinal immobilization: Its effect on neurologic
injury. Acad Emerg Med. 1998;5(3):214–219.
2. Baez AA, Schiebel N. Evidence-based emergency
medicine/systematic review abstract. Is routine spi-
nal immobilization an effective intervention for
trauma patients? Ann Emerg Med. 2006;47(1):110–112.
3. Kwan I, Bunn F. Effects of prehospital spinal immo-
bilization: a systematic review of randomized tri-
als on healthy subjects. Prehosp Disaster Med.
2005;20(1):47–53.
4. Barkana Y, Stein M, Scope A, et al. Prehospital
stabilization of the cervical spine for penetrat-
ing injuries of the neck: Is it necessary? Injury.
2000;31(5):305–309.
5. Haut ER, Kalish BT, Efron DT, et al. Spine immobiliza-
tion in penetrating trauma: More harm than good? J
Trauma. 2010;68(1):115–120; discussion 120–121.
6. Brown JB, Bankey PE, Sangosanya AT, et al. Prehospi-
tal spinal immobilization does not appear to be ben-
eficial and may complicate care following gunshot
injury to the torso. J Trauma. 2009;67(4):774–778.
7. Smith JP, Bodai BI, Hill AS, et al. Prehospital stabiliza-
tion of critically injured patients: A failed concept. J
Trauma. 1985;25(1):65–70.
8. Seamon MJ, Fisher CA, Gaughan J, et al. Prehospital
procedures before emergency department tho-
racotomy: ‘Scoop and run’ saves lives. J Trauma.
2007;63(1):113–120.
9. Chan D, Goldberg R, Tascone A, et al. The effect of
spinal immobilization on healthy volunteers. Ann
Emerg Med. 1994;23(1):48–51.
10. Domeier RM, Frederiksen SM, Welch K. Prospec-
tive performance assessment of an out-of-hospital
protocol for selective spine immobilization using
clinical spine clearance criteria. Ann Emerg Med.
2005;46(2):123–131.
11. Kwan I, Burns F. Spinal immobilization for trauma
patients (Cochrane Review). Cochrane Review;
2009; 11 http://summaries.cochrane.org/CD002803/
spinal-immobilisation-for-trauma-patients.
12. McHugh TP, Taylor JP. Unnecessary out-of-hospital
use of full spinal immobilization. Acad Emerg Med.
1998;5(3):278–280.
13. Totten VY, Sugarman DB. Respiratory effects
of spinal immobilization. Prehosp Emerg Care.
1999;3(4):347–352.
14. Kaups KL, Davis JW. Patients with gunshot wounds
to the head do not require cervical spine immobili-
zation and evaluation. J Trauma. 1998;44(5):865–867.
15. Hauswald M. A re-conceptualisation of acute spinal
care. Emerg Med J. Sept. 8, 2012. [Epub ahead of print].
16. Centers for Disease Control and Prevention (Sept. 6,
2012). Guidelines for Field Triage of Injured Patients.
2011; Retrieved from www.cdc.gov/Fieldtriage.
Accessed Sept. 24, 2012, 2012.
17. Worsing R. Basic Rescue and Emergency Care. First
Edition. Ed: American Academy of Orthopaedic Sur-
geons, Park Ridge, IL; 1990; 253 .
18. Goth P. Spine Injury, Clinical Criteria for Assessment
and Management. Augusta, ME: Medical Care Devel-
opment Publishing; 1994.
19. Morrissey J. Field Guide of Wilderness Medicine and
Rescue. Third Edition Ed: Wilderness Medical Associ-
ates, Portland, ME; 2000; 30-33.
20. Stuke LE, Pons PT, Guy JS, et al. Prehospital spine
immobilization for penetrating trauma: Review and
recommendations from the Prehospital Trauma
Life Support Executive Committee. J Trauma.
2011;71(3):763–769; discussion 769–770.
21. Berg RA, Hemphill R, Abella BS, et al. Part 5: Adult
basic life support: 2010 American Heart Associa-
tion Guidelines for Cardiopulmonary Resuscitation
and Emergency Cardiovascular Care. Circulation.
2010;122(18 Suppl 3):S685–S705.
22. March JA, Ausband SC, Brown LH. Changes in physi-
cal examination caused by use of spinal immobiliza-
tion. Prehosp Emerg Care. 2002;6(4):421–424.
23. Kennedy FR, Gonzalez P, Beitler A, et al. Incidence of
cervical spine injury in patients with gunshot wounds
to the head. South Med J. 1994;87(6):621–623.
24. Chong CL, Ware DN, Harris JH, Jr. Is cervical spine
imaging indicated in gunshot wounds to the cra-
nium? J Trauma. 1998;44(3):501–502.
25. Arishita GI, Vayer JS, Bellamy RF. Cervical spine
immobilization of penetrating neck wounds in a hos-
tile environment. J Trauma. 1989;29(3):332–337.
26. Davies G, Deakin C, Wilson A. The effect of a rigid col-
lar on intracranial pressure. Injury. 1996;27(9):647–649.
27. Kolb JC, Summers RL, Galli RL. Cervical collar-induced
changes in intracranial pressure. Am J Emerg Med.
1999;17(2):135–137.
28. Ben-Galim P, Dreiangel N, Mattox KL, et al. Extri-
cation collars can result in abnormal separation
between vertebrae in the presence of a dissociative
injury. J Trauma. 2010;69(2):447–450.
29. Cordell WH, Hollingsworth JC, Olinger ML, et al. Pain
and tissue-interface pressures during spine-board
immobilization. Ann Emerg Med. 1995;26(1):31–36.
30. Luscombe MD, Williams JL. Comparison of a long spi-
nal board and vacuum mattress for spinal immobili-
sation. Emerg Med J. 2003;20(5):476–478.
31. Muhr MD, Seabrook DL, Wittwer LK. Paramedic use
of a spinal injury clearance algorithm reduces spinal
immobilization in the out-of-hospital setting. Pre-
hosp Emerg Care. 1999;3(1):1–6.
32. Domeier RM, Evans RW, Swor RA, et al. The reliability
of prehospital clinical evaluation for potential spinal
injury is not affected by the mechanism of injury.
Prehosp Emerg Care. 1999;3(4):332–337.
33. Stroh G, Braude D. Can an out-of-hospital cervical
spine clearance protocol identify all patients with
injuries? An argument for selective immobilization.
Ann Emerg Med. 2001;37(6):609–615.
34. Barry TB, McNamara RM. Clinical decision rules and
cervical spine injury in an elderly patient: a word of
caution. J Emerg Med. 2005;29(4):433–436.
35. Burton JH, Dunn MG, Harmon NR, et al. A state-
wide, prehospital emergency medical service selec-
tive patient spine immobilization protocol. J Trauma.
2006;61(1):161–167.
36. Shafer JS, Naunheim RS. Cervical spine motion dur-
ing extrication: a pilot study. West J Emerg Med.
2009;10(2):74–78.
A special note of thanks to Karl Sporer,
MD, Alameda County medical director,
and Edward Dickinson, MD, JEMS medi-
cal editor, for their critical and helpful
review of this article, and to Peter Goth,
MD, for insight, fortitude and ground-
breaking efforts to shift the paradigm.
1303JEMS_39 39 2/26/13 4:02 PM

40 JEMS MARCH 2013
NEW JERSEY EMS RESPONSE TO SUPERSTORM
SANDY AIDED BY PRE-PLANNING &
PREPAREDNESS
Casino Pier in Seaside Heights was destroyed by Superstorm Sandy.
A new inlet carved out by Superstorm Sandy washed out a portion of a bridge and numerous homes in Mantoloking, N.J.
PH
OT
O C
OU
RT
ESY
OC
EA
N C
OU
NT
Y
1303JEMS_40 40 2/26/13 4:02 PM

It was Sept. 16, 1903, more than 100
years ago, when an unnamed hurricane
made landfall in New Jersey. Dubbed the
“Vagabond Hurricane,” the storm struck
Atlantic City with 80 mph winds and
caused $8 million in damage (equivalent
to $200 million today after inflation).
The Vagabond Hurricane destroyed doz-
ens of buildings, piers, barns and boats, scat-
tering debris all along the beachfront. Strong
winds downed telegraph and telephone
wires all up and down the coastline. Moder-
ate damage was reported from Cape May to
Monmouth County, with Atlantic County
encountering the most severe damage. One
person was killed.
Fast forward to October 2012, when
another unprecedented storm took place. But
this time, it wasn’t just a hurricane; it was the
first of its kind—a “Superstorm” named Sandy,
the largest storm ever recorded in the Atlantic
Ocean. Sandy led to at least 40 deaths in New
Jersey and left damage totaling in the billions
of dollars.
The New Jersey EMS Task Force (NJEMSTF),
formed in 2004, was ready. The NJEMSTF was
born from the Sept. 11, 2001, terror attacks
and designed to prepare New Jersey’s EMS for
large scale disasters and high impact events by
providing three critical needs: project man-
agement for major regional EMS planning
and preparedness initiatives, the procurement
of specialized equipment and resources to
support those initiatives, and a team of more
than 300 people, trained and ready to mobi-
lize those resources and staff critical areas of
operation.
We will highlight some of the major areas
of operation, share some lessons learned and
best practices, and suggest areas where others
can learn and adapt from our experiences.
FRAMEWORK FOR PREPAREDNESS
On Oct. 21, 2012, nine days before the storm
arrived, a computer weather forecast model
showed a hurricane hitting New Jersey. Our
colleagues and I were in disbelief, and we
shared the forecast with EMS stakeholders.
Subsequent forecasts continued to confirm the
storm’s path and its imminent landfall.
On Oct. 26, 2012, the State of New Jersey’s
“Tropical Storm/Hurricane Management Plan
for EMS” was activated. This document pro-
vides a framework for the effective coordi-
nation of EMS resources should the state be
threatened with a tropical system or major
coastal storm. It was produced in 2008 after it
was recognized that EMS agencies and organi-
zations would be better prepared to respond to
the overwhelming demands of such a natural
disaster if a guidance document was available.
When Sandy invaded the N.J. coastline, it had
been implemented four times already.
The plan provides:
>> Detailed standard operating procedures
when a tropical system (or equivalent
WWW.JEMS.COM MARCH 2013 JEMS 41
>> BY HENRY P. CORTACANS, MAS, CEM, NREMT-P; & TERRY CLANCY, PHD, NREMT-P
PH
OT
O C
OU
RT
ESY
OC
EA
N C
OU
NT
Y
1303JEMS_41 41 2/26/13 4:02 PM

42 JEMS MARCH 2013
significant, major coastal storm) has
the potential to impact New Jersey;
>> Procedures for EMS at the state,
county and local levels when the
National Weather Service issues a
tropical storm or hurricane watch/
warning for any portion of the New
Jersey coast;
>> Procedures for the evacuation
of healthcare facilities using
EMS resources;
>> Procedures for the acquisition
of mutual aid out-of-state EMS
resources to support New Jersey
operations through the Emergency
Management Assistance Compact
(EMAC) and the Federal Emergency
Management Agency’s (FEMA)
National Ambulance Contract;
>> Guidance on the suspension of
EMS operations (response) during
increased, hazardous winds;
>> Integration of EMS resources
within the New Jersey Office of
Emergency Management’s (OEM)
Contraflow Plan;
>> Regulatory waivers to increase EMS
capability and response during
such a disaster; and,
>> A statewide EMS communications
and demobilization strategy.
SUPPORTING DOCUMENTS
The tropical storm/hurricane management
plan references several other guidance docu-
ments that were used:
New Jersey EMS Staging Area Management
Plan: This plan defines specific, pre-identi-
fied locations that have been designated as
regional EMS staging areas able to accom-
modate large numbers of resources. It also
gives an overview of the staging process and
identifies the resources and trained person-
nel that will support the plan.
For Superstorm Sandy, two regional
EMS staging areas were established. Before
and continuing to operate early in the
storm, a facility was set up in Egg Har-
bor Township, Atlantic County. A sec-
ond location was established at MetLife
Stadium in East Rutherford, N.J., two
days after the storm hit. The NJEMSTF
deployed staging area management trailers
and teams to manage these locations. EMS
assets were organized into strike teams,
task forces and single resources, and each
was deployed to various locations around
the state for missions.
New Jersey Helibase Helicopter EMS (HEMS)
Management Plan: This plan defines specific,
pre-identified locations that have been des-
ignated as HEMS helibases where large
amounts of rotary wing air medical services
can be coordinated during a regional disas-
ter. The plan also provides an overview of
helibase management and lists the resources
and trained personnel that the NJEMSTF
uses to support the plan.
A helibase was established at Trenton-
Mercer Airport. Additional New Jersey
aircraft were placed into service. It was antic-
ipated that search and rescue missions by air
were going to be widespread after the storm
passed. As it turned out, most of the missions
were done by ground; however, this facility
was prepared to coordinate large amounts of
IN THE PATH OF DESTRUCTION>> CONTINUED FROM PAGE 41
Figure 1: Similar paths of the 1903 “Vagabond Hurricane” and Hurricane Sandy in 2012.
IMA
GE H
EN
RY
P. C
OR
TA
CA
NS/
GO
OG
LE E
AR
TH
Regional EMS staging area at MetLife Stadium, home of the N.Y. Giants and N.Y. Jets, in northern New Jersey with ambulance strike teams ready for deployment.
PH
OT
O H
EN
RY
P. C
OR
TA
CA
NS
1303JEMS_42 42 2/26/13 4:02 PM

medevac aircraft to various locations around
the state should they be needed.
New Jersey Multi-Agency Coordination
System (MACS) Plan for EMS: This plan
provides a flexible framework for estab-
lishing multi-agency coordination of EMS
resources to support a large scale inci-
dent when a regional emergency situation
threatens or significantly impacts mul-
tiple jurisdictions. This plan establishes
a coordinated net-
work for providing
information, plan-
ning, logistics and
other operational support to EMS provid-
ers within the region.
Sandy was forecasted to have a state-
wide impact, so a MACS was established
and coordinated the tracking of hundreds
of mission assignments. This allowed for the
prioritization and assignment of resources
to multiple, simultaneous areas of operation
to include emergency evacuation, mass casu-
alty surge, continuity of 9-1-1, search and
rescue, mobile satellite emergency depart-
ment and shelter support.
WWW.JEMS.COM MARCH 2013 JEMS 43
N.J. EMS Task Force Coordinator Terry Clancy briefs mutual aid crews to use caution due to extremely hazardous conditions.
A convoy of ambulances from Philadelphia arrive at the N.J. staging area.
PH
OT
O C
OU
RT
ESY
BO
B K
RA
NE
PH
OT
O C
OU
RT
ESY
BO
B K
RA
NE
� Emergency Medical Services� Operations� NIMS / ICS
� Exercise / Drills
� Human Patient Simulator
� Rescue
� HazMat
� Fire
�� WMD
� US&R
� Ambulance Strike Team
� Emergency Operations Training Center
Specialized training can be tailored to meet your needs in:Specialized training can be tailored to meet your needs in:gp
EMERGENCY RESPONSETEXAS A&M ENGINEERING EXTENSION SERVICE/EMERGENCY SERVICES TRAINING
pppp edzeizaliiaciepSpS inratrd t
Schedule these or any of our 130+ courses today!�����������������������������
Choose 33 at www.jems.com/rs
1303JEMS_43 43 2/26/13 4:02 PM

IN THE PATH OF DESTRUCTION>> CONTINUED FROM PAGE 43
44 JEMS MARCH 2013
AP P
HO
TO
/JU
LIO
CO
RT
EZ
PH
OT
O C
OU
RT
ESY
BR
IAN
DIE
CK
PH
OT
O C
OU
RT
ESY
IN
DIA
NA
EM
S T
ASK
FO
RC
E
HOSPITAL EVACUATIONSTwo emergency evacuations of hospitals took place,
both in Hudson County, N.J. The night before the storm,
Hoboken University Medical Center issued an emer-
gency evacuation order. The Hudson County OEM EMS
coordinator Mickey McCabe, with the assistance of the
NJEMSTF, mobilized more than 40 ambulances from
eight counties, including three medical ambulance buses
(MABs) to transport more than 140 patients to other des-
tinations. This was a good decision by hospital adminis-
trators, because Hoboken was under water and without
power for more than a week. The second hospital evacu-
ation took place at dawn, the morning after Sandy struck.
Palisades General Medical Center in North Bergen is
located adjacent to the Hudson River; water penetrated
their emergency generators and disabled them. Four
MABs from the NJEMSTF were deployed to rescue and
relocate 83 patients in between tidal cycles.
CONTINUITY OF OPERATIONSShore towns and urban areas were greatly affected. The
urban cities of Jersey City and Hoboken both had their
EMS headquarters destroyed by storm surge flooding
and 10 ambulances were destroyed. This area had, severe
fuel shortages and a population of more than 300,000
desperate people and no power. Dozens of the shore
communities within Monmouth, Ocean and Atlantic
counties also lost their buildings, ambulances and equip-
ment. Houses lay where roads used to be, and remaining
roads were buckled and looked like beaches. Call vol-
ume into the dispatch center was extremely high. EMTs
and paramedics worked tirelessly throughout the storm
with the remaining resources they had, despite, in many
cases, losing their own homes and personal property.
More than 1,000 mutual aid 9-1-1 missions were coor-
dinated from the Regional EMS Staging Areas, the EMS
divisions that were established and the MACS through-
out the event.
NS
A Hoboken University Medical Center patient is transported into an ambu-lance during a mandatory evacuation.
Hoboken EMS was severely impacted by record storm surge tidal flooding. They lost two ambulances, a communications trailer and a special operations truck.
The morning after Sandy, the first mutual aid convoy of ambulances is deployed for search and rescue operations along the barrier islands in Ocean County.
1303JEMS_44 44 2/26/13 4:02 PM

WWW.JEMS.COM MARCH 2013 JEMS 45
SEARCH & RESCUEUnion Beach and the “Bayshore Region”—the Barrier Islands and Atlantic City—and
many more locations received mutual aid ambulance strike teams (ASTs) and other
task forces to assist with search and rescue operations. At one point during the
storm, Mike Bascom, the Monmouth County OEM EMS coordinator made a request
for five ASTs to assist with 500 trapped or missing people in the community of Union
Beach. In Ocean County, the EMS coordinator, Steve Brennan, also used numerous
strike teams to canvas the barrier islands while more than 20 structure fires burned
and smoldered. In Atlantic City, residents were trapped in their homes and apart-
ments because they didn’t heed evacuation recommendations. These and other
search and rescue missions went on for days.
PH
OT
O C
OU
RT
ESY
AN
DY
CA
RU
SO
Off-road, all-wheel drive ambulances from the N.J. EMS Task Force proved effective in navigating difficult terrain in Ocean County.
PH
OT
O H
EN
RY
P. C
OR
TA
CA
NS
Five ambulance strike teams assisted in search and rescue operations in Union Beach, which was devastated by the storm.
Scan and get
your APP.
Download the EZ-IO app and have powerful information at your fingertips.
ANSWERS AS FAST AS OUR VASCULAR ACCESS
Choose 34 at www.jems.com/rs Choose 35 at www.jems.com/rs
1303JEMS_45 45 2/26/13 4:02 PM

46 JEMS MARCH 2013
EMERGENCY MANAGEMENT ASSISTANCE COMPACT (EMAC)Knowing ahead of time that NJEMSTF
would be overwhelmed, and following the
guidance in the previously mentioned plans,
Ken Christensen, the N.J. Department of
Health State EMS coordinator activated
the EMAC system, the nation’s state-to-
state mutual aid system.
The initial request was for 75 ambu-
lances to be deployed to N.J. before the
storm. Indiana sent the first wave of
ambulances. It had to come from that far
away initially because Superstorm Sandy
was going to potentially impact the entire
northeast quadrant of the U.S. A total of
136 ambulances, as well as staff, and sup-
port and specialty vehicles, arrived from
Indiana, Pennsylvania, Maryland and Ver-
mont. Not only did these teams bring
resources, but they brought experienced
EMS providers, which was critical to the
success of the operation. Dealing with a
catastrophe of this type required “relief”
and more staff to fill management roles.
Additionally, many of these out-of-state
professionals filled critical “leadership
positions”—from assisting with stag-
ing area and camp operations to staffing
critical roles at the MACS. The so-called
“EMAC ambulances” remained in New
Jersey through Nov. 11, 2012—almost
two weeks after the storm hit.
SPECIALIZED EMS RESOURCESAlmost every piece of the 100-plus NJEMSTF
apparatus fleet was used in some type of
capability in regards to the response to
Sandy. We’ll touch on two critical resources:
Mobile Satellite Emergency Department
(MSED): Through a partnership with
Hackensack University Medical Center,
the NJEMSTF deployed a “mobile hos-
pital system” four times. The complete
MSED system consists of three tractor-
trailers and several support vehicles, and
is equipped to function as a mobile emer-
gency department.
Mission 1 was deployed to Somerset
County ahead of the storm as a result of
lessons learned from Tropical Storm Irene.
This area of the state was expected to be cut
off significantly from river flooding based
on rainfall forecasts. Its mission was to be
a temporary field hospital to support area
communities until flood waters receded,
roads were cleared from debris and power
was restored. They treated four patients
during the three-day deployment, which
included the delivery of a healthy baby boy
during the height of the storm.
Mission 2 was deployed to Ocean
County after the storm as a result of a mas-
sive surge of patients flooding emergency
rooms. The mission was to decompress
hospitals by establishing such a facility.
Patients were transported via MABs to this
temporary location, triaged/treated and
discharged or admitted to a fixed facil-
ity. Approximately 150 patients were seen
over several days.
Mission 3 was a “mobile hospital”
deployed to Jersey City Medical Center to
allow for extra capacity so that the dam-
aged areas of the hospital could be repaired
after being surrounded by five feet of water.
This mission saw 1,301 patients.
Mission 4 was deployed through EMAC
to Long Beach, N.Y., in Nassau County
at the request of the state of New York.
It served as a “mobile hospital” to serve
the residents and surrounding commu-
nities after Long Beach Medical Center
was severely damaged and inoperable as a
result of the storm surge flooding. This mis-
sion lasted 17 days, and nearly 160 patients
were treated.
Medical Ambulance Buses (MABs): The
NJEMSTF maintains a fleet of 12 MABs.
These resources served as “force multipliers”
IN THE PATH OF DESTRUCTION>> CONTINUED FROM PAGE 45
The N.J. EMS Task Force and Hackensack Medical Center deployed their “mobile hospital system” in Ocean County to decompress swelling area emergency departments. This site treated more than 150 patients in the first few days after the storm.
Superstorm Sandy wrought significant damage to shore communities in Ocean County.
PH
OT
O H
EN
RY
P. C
OR
TA
CA
NS
PH
OT
O C
OU
RT
ESY
ST
AT
E O
F P
EN
NSY
LV
AN
IA E
MS T
ASK
FO
RC
E
1303JEMS_46 46 2/26/13 4:02 PM

WWW.JEMS.COM MARCH 2013 JEMS 47
when it came to evacuation of healthcare
facilities, relocation of non-ambulatory
medical needs patients, transport of sick
people to the mobile hospital to alleviate
the jam-packed emergency rooms, a place
to rehab and continued MCI operations.
During the storm, 10 of these resources
were available, and the MABs transported
close to 1,000 people since being were
placed in-service.
LESSONS LEARNED
As you would expect with an incident of this
size, lessons came through during the event
and after evaluation.
Incident management assistance should be
established early and continue until operations cease.
Although New Jersey had an Incident Man-
agement Team through an EMAC request,
this resource came in several days after the
disaster took place. With a catastrophe of
this magnitude anticipated, EMS leaders will
need additional support for the long-term –
especially when the impact is statewide and
“all-hands” are continuously operating.
The MSED experienced, at times, a short-
fall of available physicians. Once again, in
a “statewide” disaster, pulling these types
of resources from surrounding, non-
impacted states would have solved our
manpower shortages.
Understand the scope of practice of all response
levels and how they will integrate into the existing
EMS system. Although the state doesn’t nor-
mally recognize EMT-Intermediates, during
the disaster the state acknowledged (via the
EMAC) that EMT-Intermediates could prac-
tice to the level at which they were trained.
This created some confusion within our
own EMS system at times and was mitigated
with a quick explanation explaining what
EMT-Intermediates do.
Critical incident stress management (CISM)
is crucial during and after the event. We believe
the integration of CISM is paramount to
ensure the mental well-being of respond-
ers, especially when they are also person-
ally impacted.
Long deployments can stress respond-
ers, especially those with personal or family
commitments. States sending agencies via
an EMAC should ensure that all responders
can stay beyond the agreed EMAC request
should an extension be granted. This ensures
continuity of operations and does not create
a hardship for the sending state.
Activate the EMAC system early. This was
only the second time New Jersey requested
out-of-state EMS resources. N.J. learned
during Tropical Storm Irene that activat-
ing this system early ensures resources are
An emotional farewell as Union Beach EMS Chief Carlos Rodriguez (right) thanks Pennsylvania EMS task force leaders for their help during the weeklong operation.
PH
OT
O H
EN
RY
P. C
OR
TA
CA
NS
Choose 36 at www.jems.com/rs Choose 37 at www.jems.com/rs
1303JEMS_47 47 2/26/13 4:02 PM

48 JEMS MARCH 2013
in position and mission ready when you
need them.
Establish inter-state relationships before
a disaster occurs. Knowing who your out-
of-state partners are ahead of time only
enhances the coordinated response when
disaster strikes. These previous relation-
ships established can make a big difference.
Healthcare facility evacuations should always
take place prior to an anticipated disaster.
This is especially true for the most vulner-
able locations.
Carbon monoxide illnesses and fatalities need
to be included in the plan. A large amount of
carbon monoxide illnesses and fatalities
took place after Sandy struck. This was due
to the incorrect use of generators and dam-
aged utilities. EMS responders should be
equipped with personal carbon monoxide
detectors when providing 9-1-1 services to
areas that don’t have power.
Be careful about what you eat. A num-
ber of EMS responders fell ill after eating
“donated food.” Although intentions from
the public are generally good, EMS crews
have no way of knowing if donated food
was properly stored or contaminated.
It’s best to stick with meals, ready to eat
(MREs) products or food supplied from
trusted sources. Also, maintaining public
health and hygiene are important to pre-
vent outbreaks, such as norovirus.
Fuel shortages in a regional disaster should be
anticipated. Have a backup plan with several
other potential suppliers should the pre-
ferred ones not be able to meet your needs.
The lack of widespread power is accompanied
by a widespread loss of technology. If your com-
puter email servers and backup systems
are all affected, you’ll have to wait until
they are restored. Some EMS leaders were
without email services for several days. It’s
a good plan to use a backup email during
disasters, such as Yahoo Mail or Gmail.
Both are alternative options because they
have redundant systems worldwide.
Anticipate the need to change or waive regula-
tions. The N.J. Department of Health issued
two waivers of regulations during the storm.
The first waiver was for ALS and permit-
ted mobile intensive care units (MICU) to
be staffed by one EMT and one paramedic,
instead of the standard staffing protocol,
which requires a minimum of two para-
medics. The second waiver issued permitted
licensed BLS agencies to use one EMT and
one first responder as minimum staffing as
opposed to two EMTs per regulation. This
increased the state’s capabilities during the
disaster where resources were limited.
Establish a plan; exercise your plan and
improve your plan. Every time you exercise
or use your plan, you will find ways to
enhance or improve it.
PLANNING & TEAMWORK
In the end, the New Jersey EMS
community and our out-of-state
partners pulled off an incredible
feat. Sure, there were challenges
at times; however, because of
all the pre-existing relationships,
plans, resources, procedures
and people that were in place,
it all paid off. Today, New Jer-
sey is not just known for its 127
miles of picturesque shoreline
and beaches, but it’s also known
for its dedicated and prepared
EMTs and paramedics, who
went above and beyond the call
of duty during the largest EMS
response in state history.
Henry P. Cortacans, MAS, CEM, NREMT-P,
serves as the state planner assigned to the
Urban Areas Securities Initiative of the N.J.
EMS Task Force. He has been involved in EMS and emer-
gency management for more than 20 years. He holds a
master’s degree from Fairleigh Dickinson University spe-
cializing in terrorism/securities studies and emergency
management administration. He is also a certified emer-
gency manager through the International Association of
Emergency Managers.
Terry Clancy, PhD, MA, NREMT-P, currently serves as the
New Jersey EMS Task Force coordinator overseeing the task
force’s day-to-day activities within the Office of EMS. She
has more than 20 years of experience in the field of EMS,
public health and healthcare initiatives at the local, county
and state levels. She is a licensed N.J. Health Officer, holds
a Bachelor’s Degree in healthcare administration, a Mas-
ter of Arts in health education, and a PhD in public health.
IN THE PATH OF DESTRUCTION>> CONTINUED FROM PAGE 47
N.J. EMS Task Force medical ambulance buses stand at the ready. These valuable, high-capacity assets were used heavily and transported hundreds of patients.
Table 1: Superstorm Sandy response by the numbers
INCIDENT NUMBER OF OCCURENCES
Hospital evacuations 2
State shelter openings 5
Acute care hospitals that lost power 39
Long-term care facility evacuations 16
Healthcare facilities that lost power 196
Healthcare facility resident evacuations More than 1,700
Out-of-state EMAC ambulances supporting N.J. 136
Mutual aid mission assignments More than 1,000 (still evaluating)
N.J. EMS headquarter buildings damaged/destroyed 23
Households in N.J. without power during the height of the storm More than 2.6 million
Deaths as a result of Sandy 40
Injuries/illnesses that occurred directly due to Sandy More than 1,000
Homes damaged/destroyed 300,000
Dollars in damages $38 billion
PH
OT
O C
OU
RT
ESY
CH
AR
LES M
ON
DA
RO
1303JEMS_48 48 2/26/13 4:02 PM

WWW.JEMS.COM MARCH 2013 JEMS 49
“ Pinnacle is where
change is happening
... where change is
being defined.”
CHIEF BRUCE EVANS
Upper Pine River
Fire Protection District
Bayfield, Colo.
EXPERIENCE Pinnacle this year and gain not just an
understanding of important topics, but critical insight into
the trends you need to know about as an EMS leader. For
complete program details, faculty information, registration
discounts and more, visit pinnacle-ems.com or call
816-431-2600 today.
A REMARKABLE EVENT
FOR EMS LEADERS
AUGUST 5–9, 2013
OMNI PLANTATION
AMELIA ISLAND
JACKSONVILLE, FL
PINNACLE-EMS.COM
Experience something unique. Experience something inspiring. EXPERIENCE PINNACLE.
TM
Copyright © Fitch & Associates Choose 38 at www.jems.com/rs
1303JEMS_49 49 2/26/13 4:02 PM

50 JEMS MARCH 2013
THE PREHOSPITAL CARE RESEARCH FORUM PRESENTS ...
FOUNDING PARTNERSUCLA Center for Prehospital CareJEMS
FRIENDFISDAP
DONORArmstrong Medical
AFFILIATESNational Association of EMS EducatorsNational Association of EMTs
Selected abstracts for presentation at the 31st annual EMS Today Conference & Exposition in Washington, D.C.,March 5–9, 2013
BOARD OF ADVISORSScott Bourn, PhD, RN, NREMT-P Lawrence H. Brown, MPH, TMMegan Corry, MA, EMT-P Edward Dickinson, MD, FACEP, EMT-PWilliam J. Koenig, MD, FACEPTodd F. LeGassick, MPHGregg Margolis, PhD, NREMT-PDavid Page, MS, NREMT-P
ADVISOR EMERITUSMarv Birnbaum, MD, PhDElizabeth Criss, RN, MEd
DIRECTORBaxter Larmon, PhD, MICP
EMS RESEARCH FELLOWS Melissa Bentley, BS, NREMT-P Jennifer Purcell, MS, CHES, NREMT-P, CCEMT-P
ASSOCIATESPaul Bishop, MPA, EMT-P Dwayne Clayden, MEM, BHSc, EMT-P Twink Dalton, RN, MS, CNS, NREMT-P Robert A. De Lorenzo, MD, FACEP, MSMRobert Delagi, MA, NREMT-P Philip Dickison, MD, NREMT-P, FACEP Thomas Dunn, PhD, EMT-B Scott Eamer, BS Antonio R. Fernandez, MS, NREMT-P Mic Gunderson, EMT-P Nancy Hays, MPH Christopher Shane Henderson, AS, EMT-P David Hostler, PhD, NREMT-P, CSCS Billy James, PhD, EMT-P Todd LeDuc, MS, CFO, CEM Jeffrey Lindsey, PhD, EMT-P, CFO, EFO Mark Marchetta, BS, RN, NREMT-PMary Kay Margolis, MHA, MPH Richard Narad, DPA, JD Madeleine O’ Donnell, BNg, BEd, MEd Robert J. Philip, MPH, NREMT-P Louise Reynolds, PhD
Chris T. Ryther, MS, NREMT-P Andrew Stern, MPA, MA, NREMT-P Ronald Stewart, MD Walt Alan Stoy, PhD, EMT-P, CCEMT-P Johathan Studnek, PhD, NREMT-P Mike Taigman, EMT-P Wiliam F. Toon, MEd, NREMT-P Attila Üner, MD, MPH, FAAEM Donald Walsh, PhD, EMT-P Paul Werfel, NREMT-P , MSDavid M. Williams, PhD
1303JEMS_50 50 2/26/13 4:02 PM

WWW.JEMS.COM MARCH 2013 JEMS 51
Letter to Our Readers
The Prehospital Care Research Forum at UCLA believes that it’s the responsibility of emergency medical professionals worldwide to develop a body of evidence that examines prehospital emergency care. Our mission is to assist, recognize and disseminate prehos-
pital care research conducted at all provider levels.Each year, we acknowledge those authors who have contributed to the science of EMS through the publication of this supplement and
their subsequent presentations. As part of our ongoing pledge, the Prehospital Care Research Forum at UCLA continues to educate the medical community through a variety of seminars, lectures and workshops throughout the country. These presentations are designed to demystify the research process and provide participants with the tools to conduct research in their community.
I would like to thank our volunteer Board of Advisors and Associates. Without the dedication of these volunteers none of this would be possible.
In addition to the hard work of many, many people, much of our success can be attributed to the commitment of several organiza-tions dedicated to research in prehospital care. I would like to acknowledge our Founding Partners: Jems Communications (now known as PennWell Public Safety), Friend: FISDAP and Donor: Armstrong Medical. The generous support of these fine organizations and our affiliation with the National Association of EMS Educators and the National Association of EMTs are what enable the Research Forum to fulfill our mission.
The future of EMS depends on the quality and quantity of research we produce. We invite you to take a stand, conduct research in your community and submit it in 2013 for the greater benefit of EMS.
Sincerely,
Baxter Larmon, PhD, MICP
Director, Prehospital Care Research Forum at UCLA
52 Decreasing Mortality of Cryptic Septic Shock in EMS Patients—Oral &
Poster; Ryan T. Mayfield, MS, NREMT-P; & Mary Meyers, MHA, EMT-P
52 Probability of ROSC as a Function of Timing of Vasopressor
Administration—Oral & Poster; Christopher Johnson, EMT-B; Michael W. Hubble,
PhD, NREMT-P; Jamie N. Blackwelder, EMT-B; William P. Bozeman, MD; Kevin T. Collopy,
BA, CCEMT-P, FP-C; Sara Houston, BS, EMT-P; Melisa D. Martin, MHS, EMT-P; Delbert S.
Wilkes, EMT-P; & Jonina D. Wiser, EMT-B
52 The Accuracy of Emergency Medical Dispatcher-Assisted Layperson-
Caller Pulse Check Using the Medical Priority Dispatch System
Protocol—Oral & Poster; Greg Scott, MBA, EMDQ-I; Jeff Clawson, MD; Mark Rector;
Dave Massengale; Mike Thompson; Brett Patterson; & Christopher Olola, HO, PhD
53 Probability of a Shockable Presenting Rhythm as a Function of EMS
Response Time—Oral & Poster; Ginny O’Brien, BS, EMT-P; Michael W. Hubble, PhD,
NREMT-P; Daniel R. Wesley, AS, EMT-B; Patricia A. Dorian, EMT-B; Matt J. Losh, EMT-B;
Robert Swain, EMT-P; & Stephen Taylor, BS, EMT-P
53 Estimates of Cost-Effectiveness of a Comprehensive Influenza
Vaccination Program for Emergency Medical Services Personnel—
Poster; John Deal, BS, NREMT-P, FP-C; Michael W. Hubble, PhD, NREMT-P
53 Influence of Vasopressin on Achieving Out-of-Hospital Return of
Spontaneous Circulation—Poster; Brittany McCormick, EMT-B; Casey Schmidt,
EMT-B; Emily Wilkes, DH, AA, AS, NREMT-P; Kim Woodward, BS, BA, EMT-P; Benjamin
Young, EMT-B; Evelyn Wilson, MHS, NREMT-P; Melisa Martin, MHS, EMT-P; & Michael
Hubble, PhD, NREMT-P
54 Estimation of Patient Weight and Laryngoscopic Grade of View
Achieved By Paramedics Performing Endotracheal Intubation—Poster;
Bradley Demeter, MD; Emily Guhl, BA; Peter Lazzara, BS, EMT-P; Leslee Stein-Spencer, RN,
MS; James Walter, MD; & Eric Beck, DO, EMT-P
54 Work Exhaustion Associated with Personal and Work-Related
Characteristics among NREMTs—Poster; Jennifer Eggerichs, MS, CHES,
NREMT-P; & Melissa A. Bentley, MS, NREMT-P
55 Out-of-Hospital Cardiac Arrest in North Carolina: Epidemiology and
Patient Factors Associated With Return of Spontaneous Circulation—
Poster; Emily Wilikins, EMT-B; Stephen Taylor, BS, EMT-P; Caitlyn Boyles, EMT-B; Doran A.
Grossman-Orr, EMT-B; Lennie Cooper, EMT-P; & Michael W. Hubble, PhD, NREMT-P
55 Physiologic and Clinical Management Factors Associated with
Patients Experiencing Cardiac Arrest after EMS Contact—Poster; Mark
Pinchalk, MS, EMT-P; & Ronald N. Roth, MD
55 Short Board MVC Extrications: Current Practices and Opinions of
New Hampshire EMS Providers—Poster; Angela Shepard, MD, MPH; & Chief
Clay Odell, NRP, RN
56 Paramedics’ Perceptions of Mechanical Chest Compression Devices
for Use in Adult Out-of-Hospital Cardiac Arrest—Poster; Darren Figgis,
MSc, DIMC; Brian Carlin; Dr. Cathal O’Donnell; & Dr. Niamh Cummins
56 Aspirin Administration by Emergency Medical Dispatchers Using a
Protocol-Driven Aspirin Diagnostic and Instruction Tool —Poster; Greg
Scott, EMD-QI, MBA; Tracey Barron, BSc; Jeff Clawson, MD; Brett Patterson, EMD-I;
Ronald Shiner, AAS; Donald Robinson, BCA; Fenella Wrigley, FCEM; James Gummett; &
Christopher Olola, PhD
TABLE OF CONTENTS
1303JEMS_51 51 2/26/13 4:03 PM

PCRF ABSTRACTS>> CONTINUED FROM PAGE 51
52 JEMS MARCH 2013
1. Decreasing Mortality of Cryptic Septic Shock in EMS
Patients >> By Ryan T. Mayfield, MS, NREMT-P; & Mary Meyers, MHA,
EMT-P
Introduction: Patients in septic shock have been shown to have
a high mortality rate. Patients who fall into the subset of cryptic
septic shock—patients with a systolic blood pressure above 90
mmHg but with an elevated blood lactate—are at an even higher
risk of mortality. Previous research has shown that EMS treatment
can lower blood lactate levels before hospital arrival, but no stud-
ies to date have looked at the impact early identification by EMS
might have on patient mortality
Hypothesis: The mortality rate of patients in cryptic septic
shock identified by EMS before hospital arrival will be lower than
if it is identified after hospital arrival.
Methods: This prospective study was IRB approved and given a
waiver of informed consent. In November 2008, about 950 EMTs
and paramedics were trained on identifying patients with septic
shock and evaluating blood lactate levels. To measure blood lac-
tate levels, the paramedics were provided with the Lactate Pro©
blood lactate meter by Arkray Inc. Between May 1, 2009, and Dec.
31, 2011 patients more than 18 years old who were not pregnant
with suspected septic shock underwent blood lactate readings by
EMS. Septic patients with a lactate reading of ≥ 4.0 mmol/l were con-
sidered to be in cryptic septic shock if their corresponding systolic
blood pressure was above 90 mmHg.
Results: During the study period, 167 patients with cryptic sep-
tic shock, confirmed by an emergency department physician diag-
nosis were transported by EMS. Out of the 167 patients, 82 (49.1%)
were identified by EMS before arrival and 9 (0.5%) died in the hospi-
tal (Crude OR=0.061, CI 0.024 to 0.140, p=0.001). Of the 85 patients
who were not identified, 57 (67.1%) died in the hospital (Crude
OR=16.51, CI 6.78 to 41.41, p=0.001).
Conclusion: Many studies state the key to surviving septic shock is
early identification. In this sample of cryptic septic shock it appears
there is an almost 16 times greater chance of survival if patients are
identified by EMS before arrival at a hospital. Further studies must be
conducted to know if this can be replicated.
2. Probability of ROSC as a Function of Timing of Vasopressor
Administration >> By Christopher Johnson, EMT-B; Michael W. Hubble,
PhD, NREMT-P; Jamie N. Blackwelder, EMT-B; William P. Bozeman, MD; Kevin
T. Collopy, BA, CCEMT-P, FP-C; Sara Houston, BS, EMT-P; Melisa D. Martin,
MHS, EMT-P; Delbert S. Wilkes, EMT-P; & Jonina D. Wiser, EMT-B
Introduction: Vasopressors (epinephrine and vasopressin) have
been associated with return-of-spontaneous circulation (ROSC)
but not long-term survival. A recent retrospective study reported a
greater likelihood of ROSC when vasopressors were administered
within the first 10 minutes of arrest. However, it is unlikely that the
relationship between ROSC and the timing of vasopressor admin-
istration is a binary function (i.e., <10 vs. >10 minutes). More likely,
this relationship is a function of time measured on a continuum,
with diminishing effectiveness even within the first 10 minutes of
arrest, and potentially, some lingering benefit beyond 10 minutes.
However, this relationship remains undefined.
Objective: To develop a model describing the likelihood of ROSC
as a function of the time interval between call-receipt and first vaso-
pressor administration measured on a continuum.
Methods: This retrospective study of cardiac arrest was con-
ducted using the North Carolina Prehospital Care Reporting Sys-
tem (PREMIS). Inclusionary criteria were all adult patients suffering
witnessed, non-traumatic arrests between Jan. 1, 2012, and June 30,
2012. Chi-square and t-tests were used to analyze the relationships
between ROSC and call receipt-to-vasopressor-interval (CRTVI);
patient age, race, and gender; endotracheal intubation; AED use; first
presenting cardiac rhythm; and bystander CPR. A multivariate logis-
tic regression model calculated the odds ratio of ROSC as a function
of CRTVI while controlling for statistically significant variables from
the univariate analyses.
Results: Of the 1,150 patients meeting inclusion criteria, 518
(45.0%) experienced ROSC. ROSC was less likely with increas-
ing CRTVI (OR=0.95,p<0.01). Compared to patients with shock-
able rhythms, patients with asystole (OR=0.36,p<0.01) and PEA
(OR=0.57,p<0.01) were less likely to achieve ROSC. Bystander CPR
was a predictor of ROSC (OR=2.4,p<0.01), whereas race, age and
AED were not.
Conclusion: The study found that time to vasopressor admin-
istration is significantly associated with ROSC, and that for every
one-minute delay between call-receipt and vasopressor administra-
tion, the odds of ROSC declined by 5%. Similar to previous studies,
the study observed an increased likelihood of ROSC among patients
presenting with shockable rhythms and receiving bystander CPR.
These results support the notion of a time-dependent function of
vasopressor effectiveness across the entire range of administration
delays rather than just the first 10 minutes.
3. The Accuracy of Emergency Medical Dispatcher-Assisted
Layperson-Caller Pulse Check Using the Medical Priority
Dispatch System Protocol >> By Greg Scott, MBA, EMDQ-I; Jeff
Clawson, MD; Mark Rector; Dave Massengale; Mike Thompson; Brett Pat-
terson; & Christopher Olola, HO, PhD
Introduction: Knowing the pulse rate of a patient in a medi-
cal emergency can help determine patient acuity and the level of
medical care required. Little evidence exists regarding the ability of a
layperson 9-1-1 caller to accurately determine a conscious patient’s
pulse rate.
Hypothesis: When instructed by a trained emergency medical
dispatcher (EMD) using the scripted Medical Priority Dispatch Sys-
tem protocol Pulse Check Diagnostic Tool, a layperson-caller can
detect a carotid pulse and accurately determine the pulse rate in a
conscious person.
Methods: This nonrandomized and noncontrolled prospective
study was conducted at three different public locations in the state
of Utah. A healthy, mock patient’s pulse rate was obtained using an
electrocardiogram monitor. Laypeople initiated a simulated 9-1-1
phone call to an EMD call-taker who provided instructions for
determining the pulse rate of the patient. Layperson accuracy was
assessed using correlations between the layperson’s finding and the
ECG reading.
Results: Two hundred sixty-eight laypeople participated; 248
1303JEMS_52 52 2/26/13 4:03 PM

WWW.JEMS.COM MARCH 2013 JEMS 53
(92.5%) found the pulse of the mock patient. There was a high cor-
relation between pulse rates obtained using the ECG monitor and
those found by the laypeople , overall (94.6%, P<.001), and by site,
gender, and age.
Conclusions: Laypeople, when provided with expert, scripted
instructions from a trained 9-1-1 dispatcher over the phone, can
accurately determine the pulse rate of a conscious and healthy per-
son. Improvements to the 9-1-1 instructions may further increase
layperson accuracy.
4. Probability of a Shockable Presenting Rhythm as a Func-
tion of EMS Response Time >> By Ginny O’Brien, BS, EMT-P;
Michael W. Hubble, PhD, NREMT-P; Daniel R. Wesley, AS, EMT-B; Patricia
A. Dorian, EMT-B; Matt J. Losh, EMT-B; Robert Swain, EMT-P; & Stephen
Taylor, BS, EMT-P
Introduction: Survival from cardiac arrest is associated with hav-
ing a shockable presenting rhythm (VF/pulseless VT) on EMS arrival.
A concern is that several studies have reported a decline in the inci-
dence of SPR over the past few decades. One plausible explanation
is that contemporary cardiovascular therapies, such as increased use
of statin and beta blocker drugs, may shorten the duration of VF/VT
after arrest. As a result, EMS response time would become an increas-
ingly important factor in the likelihood of a shockable presenting
rhythm, and consequently, cardiac arrest survival.
Objective: To develop a model describing the likelihood of
shockable presenting rhythm as a function of EMS response time.
Methods: This study conducted a retrospective observational
study of cardiac arrest using the North Carolina Prehospital Care
Reporting System (PREMIS). Inclusionary criteria consisted of all
adult patients suffering nontraumatic cardiac arrest witnessed by
a layperson between Jan. 1, 2012, and June 30, 2012. Patients defi-
brillated before EMS arrival were excluded. Chi-square and t-tests
were used to analyze the relationship between shockable presenting
rhythm and patient age, gender and race; response time measured
as elapsed minutes between 9-1-1 call receipt and scene arrival and
the presence of bystander CPR. A multivariate logistic regression
model was used to calculate the odds ratio of a shockable presenting
rhythm as a function of response time while controlling for statisti-
cally significant variables identified by the univariate analyses. Due to
the risk of bias from small sample sizes, all response time categories
with less than five patients were excluded.
Results: A total of 563 patients met inclusion criteria. Overall, a
shockable presenting rhythm was observed in 159 patients (28.2%).
A shockable presenting rhythm was less likely with increasing EMS
response time (OR=0.92,p<0.01) and age (OR= 0.98,p<0.01), while
males were more likely to have a shockable presenting rhythm
(OR=1.87,p<0.01). Race and bystander CPR were not associated with
a shockable presenting rhythm, although EMS response time was
longer among patients with bystander CPR compared to those with-
out bystander CPR (9.83 vs. 8.83 minutes, p<0.01).
Conclusions: This study found that for every 1 minute of added
ambulance response time, the odds of a shockable presenting
rhythm declined by 8%. This information could prove useful for EMS
managers tasked with developing EMS system response strategies
for cardiac arrest management.
5. Estimates of Cost-Effectiveness of a Comprehensive Influ-
enza Vaccination Program for Emergency Medical Services
Personnel >> By John Deal, BS, NREMT-P, FP-C; Michael W. Hubble,
PhD, NREMT-P
Introduction: Because of their frequent contact with vulnerable
patients, vaccination against influenza is recommended for all health
care workers. Vaccination has been shown to decrease influenza
transmission to patients as well as reduce worker illness and absen-
teeism. However, the vaccination rate among EMS workers remains
low and most EMS agencies are reluctant to mandate vaccination
because of the unknown economic consequences of mandatory,
employer-provided vaccination programs.
Objective: To estimate the cost-effectiveness of a manda-
tory, employer-provided influenza vaccination program for EMS
personnel.
Methods: Using estimates from published reports on influenza
vaccination, a cost-effectiveness model of an employer-provided
vaccination program in an urban EMS system of 100 employees was
developed from the perspective of the EMS employer. Model inputs
included vaccination costs, vaccination rate, infection rate, and costs
associated with absenteeism, lost productivity due to working while
ill (presenteeism), and medical care for treating illness (medical office
visits and prescription drugs). To assess the robustness of the model,
a series of univariate and multivariate sensitivity analyses were per-
formed on the input variables.
Results: In the base case scenario, the proportion of employ-
ees contracting influenza or influenza-like illness was estimated
to be 19% (19) among vaccinated employees compared to 26%
among nonvaccinated employees. The costs of vaccine, consum-
ables and employee time for vaccination totaled $40.86 per vacci-
nated employee. For a theoretical EMS system of 100 employees, the
cost of mandatory vaccination was estimated to be $4,086. Com-
pared to no vaccination, a mandatory vaccination program would
save $20,122 (or $16,036 in net savings). The total savings were 4.9
times the cost of the vaccination program as derived from avoided
absenteeism ($7,241), avoided presenteeism ($10,963), and avoided
medical costs of treating influenza/influenza-like illness ($1,918).
Through sensitivity analyses the model was verified to be robust
across a wide range of input variable assumptions. The net mon-
etary benefits were positive across all ranges of input assumptions,
but cost savings were most sensitive to the vaccination uptake rate.
Conclusions: This cost-benefit analysis suggests that an employer-
provided influenza vaccination program is a cost-effective strategy
for reducing EMS employee absenteeism, presenteeism, and influ-
enza/influenza-like illnesss health care costs.
6. Influence of Vasopressin on Achieving Out-of-Hospital
Return of Spontaneous Circulation >> By Brittany McCormick,
EMT-B; Casey Schmidt, EMT-B; Emily Wilkes, DH, AA, AS, NREMT-P; Kim
Woodward, BS, BA, EMT-P; Benjamin Young, EMT-B; Evelyn Wilson, MHS,
NREMT-P; Melisa Martin, MHS, EMT-P; & Michael Hubble, PhD, NREMT-P
Introduction: Epinephrine has been used since 1906 in the treat-
ment of cardiac arrest. However, recent clinical trials have not been
able to demonstrate a clear benefit compared to a placebo. More
1303JEMS_53 53 2/26/13 4:03 PM

PCRF ABSTRACTS>> CONTINUED FROM PAGE 53
54 JEMS MARCH 2013
recently, vasopressin has been suggested as an alternative to epineph-
rine. However, previous investigations of vasopressin have provided
mixed and inconclusive results when compared to epinephrine.
Objective: To compare the rate of return of spontaneous cir-
culation (ROSC) between patients receiving vasopressin plus epi-
nephrine vs. epinephrine alone in out-of-hospital cardiac arrest.
Methods: This study conducted a retrospective observational
study of cardiac arrest using the North Carolina Prehospital Care
Reporting System (PREMIS), a statewide EMS patient database.
Inclusionary criteria consisted of all adult patients suffering non-
traumatic cardiac arrests in North Carolina between Jan. 1, 2012,
and June 30, 2012, who received at least one dose of vasopressin
and/or epinephrine. Chi-square and t-tests were used to analyze
the relationship between ROSC and vasopressin use; patient age,
gender, and race; witnessed arrest; EMS response time; shockable
presenting rhythm; endotracheal intubation; and the presence of
bystander CPR. A multivariate logistic regression model was used
to calculate the odds ratio of ROSC as a function of vasopressin
use while controlling for statistically significant variables identi-
fied by the univariate analyses.
Results: A total of 1,831 patients met the inclusion criteria,
of which 19.6% (359) received vasopressin. Overall, 28.2% (516)
achieved ROSC. Vasopressin was not associated with increased
rate of ROSC (OR1.0,p=0.74). ROSC was more likely among
females (OR=1.3,p=0.01), witnessed arrests (OR=1.6,p<0.01), and
shockable presenting rhythm (OR1.9,p<0.01), endotracheal intu-
bation (OR=0.5,p<0.01) and bystander CPR (OR=0.6,p<0.01) were
negatively associated with ROSC, although EMS response time
was longer among patients with bystander CPR compared to
those without (10.5 vs. 8.7 minutes, p<0.01).
Conclusion: In this statewide, retrospective analysis, vasopres-
sin made no difference in the rate of ROSC compared to epineph-
rine alone.
7. Estimation of Patient Weight and Laryngoscopic Grade of
View Achieved By Paramedics Performing Endotracheal
Intubation >> By Bradley Demeter, MD; Emily Guhl, BA; Peter Lazzara,
BS, EMT-P; Leslee Stein-Spencer, RN, MS; James Walter, MD; & Eric Beck,
DO, EMT-P
Introduction: Field intubations are frequently complicated by
challenging patients, austere environments and limited equip-
ment, although as with hospital intubations, safe and expeditious
airway management is expected. A common metric in the litera-
ture for such a standard is the “first pass” success rate.
Objective: To identify demographic, environmental and tech-
nical variables that might predict first-pass success of field endo-
tracheal intubation
Method: This study retrospectively reviewed 137 field intuba-
tions reported by paramedics in a large, urban, fire-based EMS sys-
tem for variables that might predict first pass success, including a
provider’s estimation of patient weight and a novel data point in
the literature on prehospital airway management: the Cormack-
Lehane laryngoscopic grade of view.
Results: The maximal grade of view achieved on first attempt
was significantly greater in cases of first pass success compared
to intubation that required a second attempt (C-L Grade 1.41±0.6
v. 3.47±0.7, p<0.01). The care providers’ estimation of patient
weight also correlated with first pass success (mean 82.1±31.3kg
v. 97±34.9, p=0.05). There was a stepwise progression in mean
weight from an unimpeded view of the glottic opening (C-L Grade
1, 79.7±32.1kg, n=69); to visualization of some of the vocal cords
(C-L Grade 2, 82.2±21, n=29); to visualization of only the epiglot-
tis (C-L Grade 3, 89.9±40.5; n=14; to inability to visualize either the
glottis or epiglottis (C-L Grade 4, 102±30.2, n=11).
Conclusion: These data suggest that an estimation of patient
weight might correlate with airway difficulty, as increases in
weight appear to predict less favorable views of the glottis dur-
ing direct laryngoscopy and correspond with lower rates of first
pass success.
8. Work Exhaustion Associated with Personal and Work-
Related Characteristics among NREMTs >> By Jennifer Egg-
erichs, MS, CHES, NREMT-P; & Melissa A. Bentley, MS, NREMT-P
Introduction: Work exhaustion is the depletion of emotional
and mental energy needed to meet job demands, and the impact
of work exhaustion in EMS is a growing concern. The objectives
of this study were to characterize work exhaustion in a cohort of
nationally certified EMS professionals and to determine if work
exhaustion was associated with personal and work-related charac-
teristics among nationally certified EMS professionals.
Hypothesis: There are personal and work-related characteris-
tics associated with work exhaustion among EMS professionals.
Methods: In 2010, a questionnaire was sent to all nationally cer-
tified EMS professionals eligible for recertification. A 3-item work
exhaustion scale was used to assess work exhaustion (Strongly
Agree=1 to Strongly Disagree=6). A summation of all three items
divided by three was used to compute the outcome variable. This
questionnaire also contained previously validated demographic
and work-life characteristics. Multivariable linear regression mod-
eling was used to test the study hypothesis (á=0.05).
Results: A total of 24,586 (33.9%) people completed the ques-
tionnaire. The majority of respondents were EMT-Basics (50.9%;
12,514), male (73.3%; 18,021) and had an average age of 40
(SD=10.5). Respondents reported high disagreement of work
exhaustion (mean=5.28, SD=0.93). Statically significant predictors
of work exhaustion included highest level of education completed
(high school diploma/GED â=1; some college â= -0.006, SE=0.02;
Associates or Bachelors â=-0.053, SE=0.02; Graduate Degree
â=-0.057, SE=0.03); excellent overall health (agree â=1; disagree
â=-.127, SE=0.03); excellent overall physical fitness (agree â=1; dis-
agree â=-.388, SE=0.02); years of experience (less than 1 year â=1;
1-4 years â=-0.041, SE=0.19; 5-10 years â=-0.198, SE=0.19; 11-20
years â=-0.346, SE=0.19; 21 or more years â=-0.458, SE=0.19);
volunteering (yes â=1; no â=0.039, SE=0.01); and job satisfaction
(agree â=1; disagree â=-1.385, SE=0.03). The overall model fit was
R2=0.195.
Conclusion: This is the first study that has assessed work
exhaustion in EMS professionals. As years of experience increased
and job satisfaction decreased, work exhaustion increased in
this population. Likewise, those people who did not volunteer
1303JEMS_54 54 2/26/13 4:03 PM

WWW.JEMS.COM MARCH 2013 JEMS 55
reported less work exhaustion. Key EMS stakeholders should
focus attention on these predictors to monitor those people at a
higher risk of work exhaustion.
9. Out-of-Hospital Cardiac Arrest in North Carolina: Epidemi-
ology and patient factors associated with return of spon-
taneous circulation >> By Emily Wilikins, EMT-B; Stephen Taylor, BS,
EMT-P; Caitlyn Boyles, EMT-B; Doran A Grossman-Orr, EMT-B; Lennie Coo-
per, EMT-P; & Michael W. Hubble, PhD, NREMT-P
Introduction: Although the epidemiology and outcome of out-
of-hospital cardiac arrest are known to vary geographically, pub-
lished descriptions of out-of-hospital cardiac arrest are limited to
those of EMS systems in urbanized areas. Larger-scale studies are
needed to better describe the epidemiology of out-of-hospital car-
diac arrest and factors associated with return of spontaneous cir-
culation (ROSC) in nonurban areas.
Objective: To perform a statewide, population-based, retro-
spective study of the epidemiology of out-of-hospital cardiac
arrest and patient factors associated with ROSC.
Methods: The PREMIS system, a comprehensive and mandated
data collection system for all North Carolina EMS systems, was
queried for out-of-hospital cardiac arrest occurring between Jan.
1, 2012, and June 30, 2012. Descriptive statistics, Chi-square and
t-tests were used to summarize the epidemiology of out-of-hos-
pital cardiac arrest.
Results: During the study period, North Carolina EMS agencies
responded to 4,111 out-of-hospital cardiac arrests, of which 5.6%
(230) were of traumatic origin, 39.1% (1,607) were female patients,
and 3.8% (156) were pediatric patients (<18 years). Arrests were
witnessed by laypeople in 49.4% (2,030) of cases, 18.0% (740) pre-
sented with a shockable rhythm on EMS arrival, and 44.7% (1,838)
achieved ROSC. Males were more likely to present with a shock-
able rhythm (21.2% vs. 13.1%, p<0.01) and more likely to experi-
ence a traumatic arrest (7.3% vs. 3.1%, p<0.01). Those with ROSC
were more likely to be female (47.7% vs. 42.6%, p<0.01), present
with a shockable rhythm (62.4% vs. 41.9%, p<0.01), have a wit-
nessed arrest (50.3% vs. 41.6%, p<0.01), and experience a nontrau-
matic arrest (48.0% vs. 29.2%, p<0.01). There was no difference in
age (61.9 vs. 60.7 years, p=0.10) or EMS response time (10.4 vs.
10.0 minutes, p=0.14) between patients with and without ROSC.
Conclusion: Compared to reports from mostly urbanized EMS
systems, out-of-hospital cardiac arrest s in North Carolina were
similar in terms of age, gender, cause of arrest, frequency of wit-
nessed arrest, and rate of ROSC, while EMS response times were
comparatively longer and fewer patients presented with a shock-
able rhythm. Patient factors associated with ROSC included being
female, witnessed arrest, nontraumatic arrest, and shockable pre-
senting rhythm. These findings describe out-of-hospital cardiac
arrests in North Carolina which includes a mixture of urban, sub-
urban and rural areas and offers a broader depiction of OHCA
than some other studies.
10. Physiologic and Clinical Management Factors Associated
with Patients Experiencing Cardiac Arrest after EMS Con-
tact >> By Mark Pinchalk, MS, EMT-P; & Ronald N. Roth, MD
Hypothesis: Cardiac arrest occurring in prehospital patients
after EMS contact is associated with measurable physiological
deraignment and the failure of EMS providers to provide key pre-
hospital interventions.
Methods: Retrospective chart review in a single urban ALS EMS
system of medical patients who experienced a cardiac arrest after
EMS contact and on whom an advanced airway (endotracheal
intubation or King Airway) was attempted. Trauma cases were
excluded. This was a retrospective chart review that only included
cases in which advanced airway placement was attempted.
Results: Forty-four cases were identified from Jan, 1, 2010, to
Sept. 30, 2012. The mean time from EMS contact to the patient
arresting was 15.8 +/- 7.8 minutes. The mean Glasgow Coma
Score was 10.1 +/- 5.0. The ECG was abnormal (tachycardia or bra-
dycardia) 50% (22/44) of the time. In all, 57.7% (15/26) of patients
had an initial SpO2 of < 90% and 44.8% (13/29) were hypotensive
with a systolic blood pressure of < 90. For clinical management,
75.0% (33) of the patients were moved to the ambulance before the
arrest. Of the patients, 72.7% (32) were documented to have been
placed on oxygen; 26.3% (5/19) of patients with respiratory com-
plaints were placed in CPAP; 40.9% (18) received positive pres-
sure ventilation via bag valve mask (BVM); 25.0% (11) of patients
had a successful IV or IO line placed; 46.2% (6/13) of hypotensive
patients received an fluid bolus; and 31.6% (6/19) of respiratory
patients received a respiratory medication.
Conclusion: Altered mental status, hypoxia, initial tachycar-
dia or bradycardia, and hypotension appear to be physiological
findings associated with cardiac arrest after EMS patient contact.
Early movement of the patient to the ambulance; failure to man-
age respiratory problems with CPAP or BVM ventilation; failure
to obtain IV access; and failure to administer fluids for hypoten-
sion appear to be clinical management issues associated with car-
diac arrest after EMS contact. An educational program targeted to
early identification of dangerous physiological findings and criti-
cal clinical early interventions might improve patient outcomes.
11. Short Board MVC Extrications: Current Practices and Opin-
ions of New Hampshire EMS Providers >> By Angela Shepard,
MD, MPH; & Chief Clay Odell, NRP, RN
Introduction: Many currently accepted practices in EMS are
supported only by historical practice or professional consensus.
Spinal immobilization is one area in which long-held beliefs are
being called into question. Anecdotal evidence implies that short
board devices are used less frequently than EMS training programs
teach and many protocols direct. To assess practice patterns and
opinions in New Hampshire, the New Hamphsire Bureau of EMS
surveyed providers about their use of short boards during motor
vehicle collision extrications.
Methods: A short survey was distributed at two regional EMS
conferences and a required EMS instructor training. Participation
was voluntary and anonymous.
Results: Two hundred and three completed surveys were
returned.
Most providers reported using short boards infrequently during
MVC extrications that met standard criteria for short board use. Of
1303JEMS_55 55 2/26/13 4:03 PM

PCRF ABSTRACTS>> CONTINUED FROM PAGE 55
56 JEMS MARCH 2013
respondents who reported a short board usage rate, 62.6% (127) of
the responses were for rates of 25% or lower. In fact the most fre-
quently chosen response, selected by 45.8% (93) of respondents,
was 0 to 5%. Only 14.3% (29) of respondents reported using a short
board 95 to 100% of the time.
While 78.8% (160) of respondents were “very confident” in their
ability to apply a short board during extrication, their confidence
in the device itself was significantly lower. Only 23.6% (48) of
respondents indicated they were “very confident” the device effec-
tively immobilized the spine during extrication.
One hundred and four respondents (51.2%) chose to write com-
ments. Most frequent comments included: time consuming, diffi-
cult to apply in many cars, and application increases movement
of patient. Many respondents questioned the value in MVCs not-
ing the lack of evidence to support its use or preferring to use only
c-collar and manual stabilization. Nine respondents voiced strong
support for short board usage in MVC extrications.
Conclusion: Short board usage for MVC extrication is low
among New Hampshire EMS providers responding to our survey.
Providers feel confident in their ability to apply the device but are
unsure it provides effective spinal protection during extrication.
Additional study of short board devices is recommended to deter-
mine the clinical relevance of this practice.
12. Paramedics’ Perceptions of Mechanical Chest Compression
Devices for Use in Adult Out-of-Hospital Cardiac Arrest
>> By Darren Figgis, MSc, DIMC; Brian Carlin; Dr. Cathal O’Donnell; & Dr.
Niamh Cummins
The HSE National Ambulance Service (NAS) attends approxi-
mately 1,700 out-of-hospital cardiac arrests annually. Several
devices for performing mechanical chest compressions (m-CPR)
are being evaluated for possible future use. The opinion of para-
medics regarding which device is most suited to their use has not
yet been elicited.
Objective: This study was designed to ascertain paramedics’
perceptions of, and experience with, three m-CPR devices cur-
rently being used in Ireland.
Methods: Twenty-five members of the NAS participated in this
study. Following a standardized instruction interval (video obser-
vation) in device assembly and application, subjects were asked
to initiate mechanical chest compressions on the simulated vic-
tim (manikin) of out-of-hospital cardiac arrests (manikin). Assem-
bly time was recorded using a stopwatch. Participants were then
asked to complete a questionnaire regarding their experiences
using each of the devices.
Results: Of the 25 participants (84% male), 40.0% (10) had no
prior experience using any m-CPR device. 16.0% (4) reported pre-
vious clinical experience using the AutoPulse, 24% (6) reported
having used the Life-Stat, and 12.0% (3) reported having used a
version of the LUCAS device in clinical practice. More participants
reported feeling either “comfortable” or “very comfortable” using
the LUCAS2 (92.0%; 23), than either the AutoPulse (88.0%; 22) or
the Life-Stat (72.0%; 18). Subjects reported the LUCAS2 device as
being more portable (ease of carry), and easier to assemble and
position on the manikin.
Overall, 20.0% (5) rated their first preference for the Auto-
Pulse, 12.0% (3) preferred the Life-Stat and 68.0% (17) preferred
the LUCAS2 for use in their clinical work environment. However,
more subjects required assistance with setting-up the LUCAS2
device (36.0%; 9) than either the Life-Stat (2.04%; 6) or the Auto-
Pulse (20.0%; 5).
Conclusion: The LUCAS2 m-CPR device was chosen by NAS
personnel as being easier to use in an EMS ambulance set-
ting. However, more participants required assistance initiating
mechanical chest compressions using this device than the others.
The LUCAS2 also appears to have more consistent depth and rate
of compressions in accordance with current international guide-
lines for provision of CPR.
13. Aspirin Administration by Emergency Medical Dispatchers
Using a Protocol-Driven Aspirin Diagnostic and Instruction
Tool >> By Greg Scott, EMD-QI, MBA; Tracey Barron, BSc; Jeff Clawson,
MD; Brett Patterson, EMD-I,; Ronald Shiner, AAS; Donald Robinson, BCA;
Fenella Wrigley, FCEM; James Gummett; & Christopher Olola, PhD
Introduction: The American College of Cardiology and the
American Heart Association recommend early aspirin adminis-
tration to patients with symptoms of acute coronary syndrome
(ACS)/acute myocardial infarction (AMI). The primary objective
of this study was to determine if emergency medical dispatchers
(EMDs) can provide chest pain/heart attack patients with stan-
dardized instructions effectively, using an Aspirin Diagnostic and
Instruction Tool (ADxT) within the Medical Priority Dispatch Sys-
tem before arrival of an emergency response crew.
Methods: This retrospective study involved three dispatch cen-
ters in the United Kingdom and the United States. Six months of
data were analyzed involving chest pain/heart attack symptoms
taken using the MPDS Chest Pain and Heart Problems/Automated
Internal Cardiac Defibrillator Protocols.
Results: The EMDs successfully completed the ADxT on 69.8%
(30,810) of the 44,141 cases analyzed. The patient’s mean age
was higher when the ADxT was completed, than when it was
not (mean ±standard deviation (SD): 53.9±19.9 and 49.9±20.2;
p<0.001, respectively). The ADxT completion rate was higher for
second-party, than first-party calls (70.3% and 69.0%; p=0.024,
respectively). A higher percentage of male patients took aspirin
(91.3% and 88.9%; p=0.001). Patients who took aspirin were signif-
icantly younger than those who did not (mean±SD: 61.8±17.5 and
64.7±17.9, respectively). Unavailability of aspirin was the major
reason (44.4%; 19,598) why eligible patients did not take aspirin
when advised.
Conclusions: EMDs, using a standardized protocol, can
enable early aspirin therapy to treat potential ACS/AMI prior to
responders’ arrival. Further research is required to assess reasons
for not using the protocol and the significance of the various
associations discovered.
Call for Abstracts 2013: www.pcrf.mednet.ucla.edu
1303JEMS_56 56 2/26/13 4:03 PM

“
“
“The workshops and interaction with peers
and other first responders ensures that all my
operations keep current with local/state and
federal requirements. Vendor exhibits are also
a great way to view and operate both current
and new equipment needed for the job.”
www.iafc.org/frm
What You Hear is True.
Attendees can’t stop talking about Fire-Rescue Med. And can you blame
them? Fire-Rescue Med ofers outstanding education and networking
events and an exhibit hall with the newest and technology and products.
®2013
��������������������� ������������������������������� ���
- Stephen Larison, Chief
Fire and Emergency Service
United States Air Force
1303JEMS_57 57 2/26/13 5:06 PM

58 JEMS MARCH 2013
MISSION: LIFELINE WILL INCORPORATE EMS RECOGNITION
IN STEMI & CARDIAC RESUSCITATION SYSTEMS OF CARE
>> BY CHRIS BJERKE, MBA, BSN; GARY WINGROVE, EMT-P; FRANKLIN PRATT, MD; J. LEE GARVEY, MD; & A. GRAY ELLRODT, MD
As you may have read in the October
JEMS sponsored article, “Accelerated
Success: Mission Lifeline program
dedicated to tracking STEMI treatment,”
Mission: Lifeline is an American Heart
Association (AHA) program that focuses on
improving systems of care for ST-segment
elevation myocardial infarction (STEMI) and
out-of-hospital cardiac arrest treatment. The
program, which was initially developed in
2007 to improve care by reducing the bar-
riers that existed in STEMI treatment. The
focus on out-of-hospital cardiac arrest sys-
tems of care was added in April 2012.
The Mission: Lifeline process begins with
the initial identification of symptom onset,
which may occur with a STEMI patient expe-
riencing chest pain or, in the case of cardiac
arrest, the recognition by a family member or
a bystander that a patient is unconscious and
not breathing. Mission: Lifeline then lays out
critical elements for ideal patient care at each
stage, from prehospital EMS to referral cen-
ters to receiving centers. The program also
focuses on community involvement, with
the goal of training more than 50% of the
public in being able to initiate CPR. Thus, the
system of care begins with the community
(bystander CPR), then moves to EMS and the
hospital, and finally returns to the commu-
nity as the patient is discharged.
For more about the science behind this program, read “Accelerated Success: Mission Lifeline program dedicated to tracking STEMI treat-ment” on p. 51 of October JEMS.
IDEAL SYSTEM ELEMENTS
What are the elements that make up an
“ideal” system of care? Mission: Lifeline
focuses on the importance of data collection,
quality improvement and feedback mecha-
nisms to all parties involved in caring for the
STEMI and cardiac resuscitation patient.
The program uses the ACTION Registry-
Get with the Guidelines (GWTG) data regis-
try. The next version (2.4) of the registry will
incorporate more prehospital data elements
that can be collected and reported. Mission:
Lifeline Receiving Center reports are avail-
able for receiving centers that are percu-
taneous coronary intervention-capable and
provide aggregate-level data on time metrics
and quality outcomes for STEMI patients.
The Mission: Lifeline regional reports pro-
vide aggregate data on specified regional
hospital data, allowing hospitals to compare
their performance against other hospitals
in their region. These reports are available
quarterly to all hospitals that are contracted
with ACTION Registry-GWTG and regis-
tered with Mission: Lifeline.
In addition, Mission: Lifeline hospital rec-
ognition was launched in 2009 to recognize
hospitals that meet evidence-based recom-
mendations in the treatment of STEMI care.
The recognition program has grown since
its beginning and this past year awarded 226
hospitals for meeting achievement criteria.
RECOGNIZING EMS
The next obvious step in the evolution of the
acknowledge program is to recognize the
medical professionals who are the first point
of contact in the continuum of care—EMTs
and paramedics. Today’s prehospital profes-
sionals follow evidence-based guidelines in
the treatment of heart attacks and are now
equipped to interpret ECG results for STEMI.
This allows for early alerts to hospitals. The
public should be educated that EMS is far
from simply a transport method; but rather
can shave precious minutes off life-saving
treatment time by activating the emergency
response system.
Accordingly, the Mission: Lifeline pro-
gram is pleased to announce the develop-
ment of such a recognition program for EMS.
This initiative will focus on three important
“achievement measures.” EMS providers
must perform these measures at least 85%
of the time to qualify for recognition. No
one measure can drop below 75%, and the
three measures must equal an 85% compos-
ite score. An agency must achieve all three
measures to be eligible for achievement. This
is an annual recognition that will be made
available in 2014, using self-reported data.
The three measures are:
1. Percentage of patients who are older
than 35 years who present with non-
traumatic chest pain and for whom
EMS obtains prehospital 12-lead ECGs;
2. Percentage of STEMI patients with first
prehospital medical contact-to-bal-
loon-inflation of first device used time
within 90 minutes; and
3. Percentage of STEMI patients taken to a
referral hospital that administers fibri-
nolytic therapy with a door-to-needle
time within 30 minutes.
The recognition program committee will
begin reviewing 2013 data in February 2014.
The following are the designated recogni-
tion levels :
>> Bronze: One quarter;
>> Silver: Four quarters; and
>> Gold: Eight quarters. (The first
will be awarded in 2015.)
MORE TO COME
We hope this recognition will highlight
the essential role of the EMS community
in improving survival and life quality for
patients with the extreme manifestations
of heart disease. Additional information
will be announced on the Mission: Lifeline
website, www.heart.org/missionlifeline
and Facebook page, www.facebook.com/
AHAMissionLifeline.
Chris Bjerke, MBA, BSN, is the national director for the
American Heart Association.
Gary Wingrove, EMT-P, is with Gold Cross/Mayo
Clinic Medical Transport in Minnesota.
Franklin Pratt, MD, is medical director for the Los
Angeles County Fire Department.
J. Lee Garvey, MD, is medical director for the Chest
Pain Evaluation Center at Carolinas Medical Center, N.C.
A. Gray Ellrodt, MD, is chief of medicine of cardiol-
ogy for Berkshire Medical Center at the University of
Massachusetts Medical School.
MISSION: LIFELINE WILL INCORPORATE EMS RECOG
Expanding the Mission
PH
OT
O A
CIL
O/
IST
OC
KPH
OT
O.C
OM
1303JEMS_58 58 2/26/13 4:03 PM

WWW.JEMS.COM MARCH 2013 JEMS 59
Improve your patientcare skillsNAEMT courses provide high quality, cost effective,
evidence-based education to help you better care
for your patients. Sign up today to take a PHTLS,
AMLS, EPC, TCCC or EMS Safety course.
All courses are CECBEMS accredited and meet
NREMT recertifi cation requirements.
Serving our nation’s EMS practitioners
Learn more at www.naemt.org.
JEMS.com EMS Jobs can help you fill your open
positions faster and more cost-effectively than other
recruiting methods. Post your job opportunity to thousands
of qualified EMS professionals and begin finding the
qualified candidates you need … immediately!
It’s easy to fill out the online form and submit your
opening. The job will post within 24 hours of submission
and then you can begin your screening process.
Interested in making your job listing stand out?
Upgrade your Basic Job Listing to a Featured Job Listing
where it will be posted at the top of the EMS Jobs page as
well as highlighted in rotation throughout JEMS.com.
In addition, your listing will be featured in the JEMS.com
eNewsletter (sent to over 49,000* EMS professionals).
*January 2013: Publisher’s Data
EMS Recruiting
Just Got a Lot Easier.
For more information, please go to www.jems.com/ems-jobs/post-job
HR/RECRUITING TEAM:
JEMS.com is a great source
for EMS recruitment!
Choose 39 at www.jems.com/rs Choose 40 at www.jems.com/rs
1303JEMS_59 59 2/26/13 4:03 PM

60 JEMS MARCH 2013
PH
OT
OS C
OU
RT
ESY
LO
ND
ON
AM
BU
LA
NC
E S
ER
VIC
E
EMS planning started the day London won the Olympics bid.
1303JEMS_60 60 2/26/13 4:46 PM

WWW.JEMS.COM MARCH 2013 JEMS 61
HOW LONDON AMBULANCE SERVICE SUCCESSFULLY
HANDLED THEIR ‘SUMMER OF SPORT’
>> BY JASON KILLENS, MSTJ, JP
Duty Station Officer Ken Randall as venue commander.
EMS providers responded to some calls on special bicycles.
1303JEMS_61 61 2/26/13 4:46 PM

PLANNING LIKE AN OLYMPIAN>> CONTINUED FROM PAGE 61
62 JEMS MARCH 2013
Planning for the London 2012 Olym-
pic and Paralympic Games began on
the day it was announced that London
would host the Games. That day was July 6,
2005, and as Trafalgar Square and towns and
cities around the United Kingdom erupted
with joy when the words “the Games of the
30th Olympiad in 2012 are awarded to the
city of London” rang out around the world
from Singapore.
Those of us in London Ambulance Ser-
vice (LAS) operations had a different reac-
tion. We took a deep breath and said to
ourselves that we had a massive task to
deliver on. But the following day, London
was thrown into chaos as suicide bombers
targeted the underground subway system
at the height of the morning rush hour.
Fifty-two people lost their lives in what was
the first multi-sited and simultaneous use
of suicide bombers as a weapon of terror
in the UK. The London Ambulance Service
would later be subject to intense scrutiny
of its response to the bombings but would
draw lessons from that day that enhanced
our capability across the Olympic and Para-
lympic period.
OBSERVATIONAL LEARNING
A planning team of six was established in
2007. It was tasked with working full-time
across many partner organizations to scope
and understand the scale and complexity
of the Games. We worked with existing
agencies and were able to use relationships
that had been developed over many years
to aid planning. Equally there were many
new organizations that we needed to develop
relationships with. One of these was the Lon-
don Organising Committee of the Olympic
Games (LOCOG). Specifically with LOCOG,
a full-time senior operational manager from
LAS was seconded into the organization to
aid planning and share experiences.
Although London Ambulance Service
has experience in planning for sporting and
cultural events on a massive scale, its admin-
istrators had never planned for multiple ven-
ues working simultaneously across the city
over a protracted period whilst the eyes of
the world were on us. We learned from pre-
vious host cities about the nature, type and
number of patients who may be seen. We
also learned some of the more operational
issues around accreditation and the “post
Games effect.”
Members of the planning team, which
sought to learn lessons from previous host
cities, travelled to Beijing for the 2008 Olym-
pic and Paralympic Games as well as other
major sporting events. The single biggest
lesson learned from other host cities and
those that had hosted such events as the Pan
American and Commonwealth Games was
this, “Don’t leave planning until the Games
are upon you and resource the planning
team to be able to respond to the demands
placed upon it.”
RIGOROUS TESTING
Our planning team worked full-time for
five years to prepare LAS to respond to the
EMS held a pre-planned aid arrival briefing at Goldsmiths College in London.
Choose 41 at www.jems.com/rs
1303JEMS_62 62 2/26/13 4:46 PM

WWW.JEMS.COM MARCH 2013 JEMS 63
increased call volume received during the
Games. In the six to 12 months leading up
to the games they gained support from the
Games Time Command Team of senior offi-
cers on a half-time basis. These additional
officers bought the total planning team to 12
from 2011–2012.
Testing for the Games began years before
the opening ceremony and involved com-
mand post, table top and live play exercises.
The program culminated with three sets
of live sporting events in Olympic venues
across the city. We were clear from the
outset that each of these test events across
each venue would see the actual Games
Time Command Team together with
the paramedics and EMTs who would
be deployed throughout the venues. This
enabled those who would actually provide
prehospital care at the venues during the
Games to become acquainted with new
venues while establishing relationships
others, such as LOCOG venue managers.
During the final set of tests events in
May 2012, two months before the open-
ing ceremony, we deployed paramed-
ics and EMTs from around the country
into the venues. The Olympic Deploy-
ment Centre (ODC) was opened and our
Olympic Event Control Room (OECR)
managed deployments and responses to
emergency calls.
CENTRAL OPERATIONS
The ODC was an empty warehouse in East
London on a back street industrial park. It
was located immediately across the Thames
River from the Millennium Dome—now
renamed the O2 Arena. We had a vision for
the ODC. We wanted to transform it into
a flagship, albeit a temporary one, for the
Games. It would be open 24 hours a day,
and be the center for EMS response. All
ambulance service staff being deployed to
Games venues and cultural events would be
mustered, briefed, fed and deployed from the
ODC. The building was a shell and after a bit
of cleaning we installed temporary catering
facilities along with showers, toilets, lockers,
briefing rooms, a canteen, internet café plus
a vehicle preparation and equipping area.
The ODC became a working super-station
for the Olympics and was one of the key suc-
cess stories of the Games for us.
Our dedicated OECR, which was built in
2008, was open 24 hours a day during the
Games. It was where we managed deploy-
ments and responses in each of the four
Games delivery zones. The 36 position
Prehospital providers were also ambassadors.
Choose 42 at www.jems.com/rs
1303JEMS_63 63 2/26/13 4:46 PM

64 JEMS MARCH 2013
control room links via our CAD system to
our main control room, while having the
benefit of access to a network of closed-
circuit TV cameras across the city.
We considered how we would deliver
existing service requirements, such as
response time performance standards and
clinical quality, while deploying hundreds of
paramedics and EMTs to sporting venues and
cultural events. It was clear that even with
restrictions on planned workforce abstrac-
tions, which included a deferral of all train-
ing across the summer of 2012, we would
need an additional short-term boost to the
workforce. There are eleven National Health
Services ambulance services across England.
We are the biggest and busiest handling over
1.6 million emergency calls per year. Each of
the other English ambulance services agreed
to send pre-planned aid to London for the
Olympics and Paralympics, boosting our
dedicated Games specific workforce to 500
paramedics and EMTs. Outside of the Games
for business as usual we have a paramedic
and EMT workforce of 3,000.
Each ambulance service around England
works slightly differently. Because each has
different policies and procedures, it was nec-
essary to provide training to each member of
the Games cohort. Over four days, a training
team from London visited each ambulance
service in England to provide training to
staff. The training package was completed in
London when paramedics and EMTs began
to arrive in late July for the Games.
Paramedics, EMTs and Emergency Medi-
cal Dispatchers (EMDs) from around Eng-
land arrived in London over three days. Each
day, those arriving received an initial brief-
ing and their personal issue LAS baseball
cap, among other items of Games specific
personal issue equipment.
The planning team didn’t only have to
negotiate and agree how we would deliver
services across the Games and its multi-
ple venues. We also had to make sure we
complied with the bid commitments, the
requirements of the individual sport federa-
tions and LOCOG. We also had to arrange
accommodation, feeding and transport for
200 staff from outside London.
LET THE GAMES BEGIN
We began the briefings for the staff work-
ing in the Olympic Stadium with a degree
of anticipation on the day of the opening
ceremony. It was too late if we had forgotten
something. We would have to adapt, flex
and improvise. Our past five years of plan-
ning was predicated on this and had pro-
vided a framework for delivery that could be
adjusted to meet operational requirements
on the day.
Our Games Time Delivery Strategy pro-
vided a firm foundation for this flexibility.
It complimented existing event and mass
gathering doctrines in London. As the open-
ing ceremony began and Queen Elizabeth
jumped from a helicopter over the Olym-
pic Stadium in a spoof, James Bond-style
sequence, we all sat glued to the television
and watched. It was at that point I knew this
was going to be something special.
I had been involved in the planning and
delivery of many large events in London
over the past 10 years. These included
the Live8 concert, G8 and G20 summits,
New Year’s Eve celebrations, Notting Hill
Carnival, London Marathon, state visits
PLANNING LIKE AN OLYMPIAN>> CONTINUED FROM PAGE 63
A bicycle responder patrols the Southbank by Tower Bridge.
Presenting Complaint by Zone
For this table’s data and additional tables from London Ambulance Service, scan the above code or
visit jems.com/journal and click on “March.”
1303JEMS_64 64 2/26/13 4:46 PM

WWW.JEMS.COM MARCH 2013 JEMS 65
Serving our nation’s EMS practitioners
You deserve the best.
National Association of Emergency
Medical Technicians
��the best benefi ts
��the greatest opportunities
��the strongest voice
advocating on your behalf
Join NAEMT today.
www.naemt.org | 1-800-346-2368
Choose 45 at www.jems.com/rs
Choose 43 at www.jems.com/rs
Choose 46 at www.jems.com/rs
Choose 44 at www.jems.com/rs
1303JEMS_65 65 2/26/13 4:46 PM

66 JEMS MARCH 2013
of the Pope and other famouse people,
the royal wedding and the Queen’s Dia-
mond Jubilee. But this was different. It
was something else.
Day one of the Games followed, and our
plans were working well. Although there
were issues with some of the logistics,
they were insignificant in comparison to
the scale and complexity of the opera-
tion. Deployments of EMTs and paramed-
ics on foot, in ambulances, on motorbikes
and pedal cycles were underway. We had
people in venues, at cultural events and
standing by at transport hubs.
Our Olympic Information Unit (OIU)
was in full swing. It operated 24-hours-
a-day and provided strategic briefings on
activity, incidents and relevant issues to key
internal and external stakeholders. This
unit worked to compliment the control
room and was at the center of our EMS
response during the Games.
GAME-DAY(S) RESPONSEReserves were planned for each day of
the Games, depending on the perceived
risk. Our assessment of risk was based on
known events, the competition schedule,
the weather forecast and other intelligence.
The reserves consisted of ambulances and
special assets. The special assets allowed
us to be prepared to respond to such spe-
cific types of threats as chemical, biologi-
cal, radiological and nuclear events. They
included special equipment supply and
mobile control vehicles, plus teams of staff
able to provide urban search and rescue,
high-angle rescue and swift-water rescue.
As each day of the Olympics passed,
we saw increased demand but weren’t as
busy as we had expected. Overall activity
across London during the Games rose by
about 10%. We saw some traffic congestion
when the Games lanes went live, but the
road network and public transport network
delivered, and Londoners, visitors and spec-
tators alike were able to travel without inci-
dent. The same was true for us with limited
disruption to emergency response—per-
haps as a result of the detailed route and
access planning undertaken.
Equally as important to the provision of
EMS at Games venues was the service we
provided to the rest of London. We termed
this “maintaining service delivery” (MSD),
or core business. We had planned this to
provide the same emergency service to Lon-
doners in non-Olympic boroughs while
delivering world-class responses and care
at Olympic venues. A senior colleague over-
saw the planning and delivery of MSD. We
reconfigured many aspects of routine ser-
vice delivery to release capacity to support
Olympic or core delivery. The basis of this
planning was our existing business continu-
ity arrangements. This approach meant that
staff members were already familiar with
how we would do things when challenged,
and it meant that we were less likely to see
confusion. Existing plans formed the basis
of our MSD and Olympic planning, keeping
our delivery as close to what we normally
do as possible and not inventing something
new for the Games —both of which reduced
the potential for error.
PLANNING LIKE AN OLYMPIAN>> CONTINUED FROM PAGE 64
Paramedics celebrate success at the Olympic Stadium shown on a big screen.
�������������������
��������������
�������
����������
�����������
���������
�
��������
�����������
�������
�����������
�������
����������� ��� ��� �� ��� �� ���� �� �
�������������� ��� ��� ��� ��� ��� ���� ��� ����
��
���
����
����
����
����
����
����
����
����
�����
�����
������ ���� ������� Olympic Games Activity
Olympics providers came from all over England.
1303JEMS_66 66 2/26/13 4:46 PM

THANK YOU TO OUR SPONSORS
INTERNATIONAL CONFERENCE O
N
DISASTER & TERRORISM PREP
AREDN
ESS
MARCH 7-9, 2013
WASHINGTON, DC
MARCH 5 - 9, 2013
WASHINGTON, D.C.
With the help of these organizations, we provide a forum for quality education in EMS.
We sincerely appreciate their support.
TM
F o u n d i n g S p o n s o r S u p p o r t i n g S p o n s o r s
JEMS Games Sponsors
Additional Sponsors
Association Sponsors
TM
1303JEMS_67 67 2/26/13 4:46 PM

68 JEMS MARCH 2013
Spectators were the largest patient group
during the Olympic and Paralympic Games,
closely followed by those making up venue
workforce. Although no major or multi
casualty incidents happened over the 30 days
of sport, a number of incidents happened in
which critically ill patients presented with
cardiac arrests, ST-elevation myocardial
infarctions and convulsions in venues. Our
teams worked alongside the volunteer work-
force of LOCOG and LOCOG Medical (a
separate team within the organizing com-
mittee that provided first aiders, nurses and,
in some cases, doctors in first aid rooms) to
provide initial treatment before conveying
them to emergency departments (EDs).
SUMMARY
LOCOG Medical managed thousands of
patient contacts across all the Games venues
without our intervention. A polyclinic in
the athlete’s village had extensive diagnostic
options, including X-ray and magnetic reso-
nance imaging for athletes and the Olympic
family. These helped limit the number of
patients who needed transport to the ED.
Although the delivery was seamless,
there were “behind the scenes” moments
in the final stages of planning that made
us think. We received additional requests
for ambulance cover at training venues that
hadn’t been planned for on short notice.
In addition, the torch relay attracted bigger
crowds than initially planned for. Some of
the planning assumptions and agreements
changed on short notice for various reasons.
This meant we had to adjust our plans while
also solving human resource issues that you
would expect to see among a workforce of
around 500 across a six-week period.
As part of the National Health Service
(NHS) ambulance service Games cohort,
more than 500 staff were deployed across 18
venues and 30 days of sport in London. In
doing so, they delivered in excess of 165,000
hours of standby and care, responded to
nearly 1,500 Games-related incidents and
conveyed 800 patients to emergency depart-
ments across the capital.
After such an influx, it wasn’t easy to
return to business as usual. Officials with
previous host cities had advised us that there
would be a feeling of “what next” once the
Games concluded. When I first heard this,
I thought the opposite would be the case. I
expected feeling relieved of overwhelming
emotion as well as from the exhaustion of
the long days. I do have to say that although
this was the case, it’s also true that there is a
“post Games” come down. We had just been
part of a fantastic summer of sport with a
brilliant medal tally from Team Great Brit-
ain and Paralympics Great Britain that, of
course, helped the euphoria. But we did feel
a real sense of uncertainty about what to do
next. We had spent five years planning for
it, lived it for the past six months and been
part of it for the past 30 days. And now it
was over.
Overwhelmingly the experience was truly
great. There was an immense sense of pride
in achievement and participation on the part
of every EMT, paramedic EMD, officer and
ambulance service employee who helped
deliver prehospital care at the Games. The
Games and cultural events were a truly once-
in-a-lifetime experience. We were privileged
to be part of that experience, to provide
prehospital care during the Games and to be
able to say we were part of something that
inspired a generation.
Jason Killens, MStJ, JP, is deputy
director of operations at the Lon-
don Ambulance Service NHS Trust
and was the gold commander
for the Olympic and Paralympic
Games 2012.
PLANNING LIKE AN OLYMPIAN>> CONTINUED FROM PAGE 66
��
���
���
���
���
���
���
���
�����������
���������
���������
��������
��������
���������
���������
���������
���������
���������
���������
���������
���������
��������
�������
��������
������������������������� ��������
������
������
�����
��������
A bike medic tends to the needs of a patient at an Olympics venue.
Workload by Date and Zone-Olympics
1303JEMS_68 68 2/26/13 4:46 PM

TM
®
WHERE PEOPLE, PRODUCTS AND IDEAS
February 4 – 8, 2014WASHINGTON, DC
Serving the emergency services community, EMS Today provides professionals with a valuable combination of progressive
education, developed by industry experts and JEMS contributors, and the latest equipment from leading manufacturers.
Emergency services personnel rely on EMS Today to help develop their careers, create networking opportunities and provide an environment
where camaraderie, pride of service and dedication to saving lives is celebrated.
For information on the 2014 program, events and registration, please visit www.EMSToday.com.
Mark your calendars now for 2014!
Presented by
1303JEMS_69 69 2/26/13 4:47 PM

70 JEMS MARCH 2013
PH
OT
OS C
OU
RT
ESY
DA
VID
PA
GE
The St. Paul Fire Department EMS Academy is training its seventh class of “Freedom House” providers.
1303JEMS_70 70 2/26/13 4:12 PM

It might seem ironic to some that Minne-
sota, a state not known for diversity, is the
birthplace of one the most diverse EMS
departments in modern day U.S. history. It
might also seem ironic that its inspiration,
the diverse Pittsburgh EMS agency—called
Freedom House Ambulance Service, was dis-
solved during the height of its support by
prominent clinical leaders due to politics.
It’s certainly an ironic twist of fate that
45 years after training its first class of low-
income African Americans, Freedom House
was reborn. The new Freedom House Ambu-
lance Service, this one launched in St. Paul,
Minnesota, was created by a collaboration
of area organizations recognizing a need to
not only diversify its mostly Caucasian work-
force, but also to provide an occupational
opportunity for populations in underserved
communities.
The rebirth of the St. Paul program was
illuminated by powerful speeches from three
of the original Freedom House Ambulance
Service members at the spring 2012 St. Paul
Fire Department (SPFD) EMS Academy grad-
uation, but the groundwork and spark for
the new Freedom House Ambulance Service
began much earlier.
BIRTH OF THE ORIGINAL
FREEDOM HOUSE
It was 1966. For African-American com-
munities like the Hill District of Pittsburgh,
unemployment was epidemic. Social services
were nonexistent. Calls for emergency medi-
cal assistance were returned with silence,
delayed responses or inadequate care.
These conditions were unacceptable
to community activists Phil
Hallen and James McCoy.
Together, they proposed a pro-
gram that provided economic
opportunity and emergency
medical care to a community
that had neither.
They enlisted the expertise of
Peter Safar, MD, a prominent
anesthesiologist. Safar, a pioneer
of resuscitation techniques, was
fueled by the death of his 11-year-old daugh-
ter from an acute asthma attack and a pas-
sion for bringing advanced emergency care
to the patient in his research and practice.
The convergence of these forces birthed
an audacious, community-
based, employment and train-
ing program that was the
seed of paramedicine and the
home of one of the first (and
most diverse) ALS training
programs in the U.S.—Free-
dom House Ambulance Ser-
vice. However, the Freedom
House program has often
been neglected in EMS history.
WWW.JEMS.COM MARCH 2013 JEMS 71
HOW THE STORIED AMBULANCE COMPANY HAS BEEN REBORN
>> BY MEGAN CORRY, MA, EMT-P, CASEY KEYES, BA, NREMT-B, & DAVID PAGE, MS, NREMT-P
The new Freedom House diversifies the EMS workforce in the Twin Cities.
Darnella Wilson is one of the original Freedom House providers.
1303JEMS_71 71 2/26/13 4:12 PM

REVIVING FREEDOM HOUSE>> CONTINUED FROM PAGE 71
72 JEMS MARCH 2013
Freedom House Enterprises recruited 25
young African Americans from their com-
munity. This included several veterans
returning from Vietnam and others who car-
ried the burdens of poverty, drugs and alco-
hol abuse. They began training the first class
of students in 1967.
With Safar involved, the program was rig-
orous, requiring long days in the classroom
and lab. Safar noted early on that some of
the students lacked basic skills in reading
and math. However, as a testament to their
persistence and the commitment and qual-
ity of the instructors, many of the students
obtained their general educational develop-
ment (GED) degree and continued with their
medical training well after Freedom House.
Safar never swayed from his vision, and
the Freedom House recruits had the support
of the faculty, their community and each
other. Their loyalty and drive to succeed car-
ried them through the challenging program,
which consisted of more than 160 hours of
preparatory training in anatomy, physiol-
ogy, medical ethics and advanced resuscita-
tion techniques.
The year-long program also required six
weeks of hospital-based training in the oper-
ating room and emergency department, the
intensive care unit, the morgue and medi-
cal wards. The recruits also were required to
attend medical rounds and lectures with resi-
dents, something many EMS programs don’t
incorporate even today. They were trained,
mentored, monitored and evaluated on the
job, where they responded to emergencies
under the watchful eyes of, and in consulta-
tion with physicians.
Freedom House Ambulance and the
unexpected success of the once-underem-
ployed and impoverished recruits realized
Safar’s vision of bringing bring critical life-
saving care to underserved patients.
Special Premier of the Documentary
‘Freedom House’A special 90-minute documentary on Freedom
House Ambulance, sponsored by Jones & Bartlett
Learning, will be presented from 7:30 to 9
p.m. March 7 at the EMS Today Conference &
Exposition in Washington, D.C. Registered attend-
ees will be admitted free to the premier at the
Washington Convention Center. Q&A to follow.
EARLY FREEDOM HOUSE OPERATIONSFreedom House Ambulance Service started
with two donated police “wagons” and
operated on a shoe-string budget. They
responded to more than 5,800 calls in their
first year, transporting more than 4,600
patients, mostly from within the African-
American districts of Pittsburgh.
Word of this novel program spread rap-
idly through the community, particularly
after the 1968 riots following the assas-
sination of Martin Luther King, Jr. In fact,
Freedom House medics worked together
in an unprecedented collaboration with the
largely white police force to provide emer-
gency care to the sick and injured in com-
munities devastated in the wake of the riots.
The activities of the Freedom House
Paramedics are some of the first accounts of
paramedics providing ALS skills in the field,
and this timeline could arguably place Free-
dom House paramedics as the first in the
nation to provide this level of care.
By 1973, with new grant funding, Free-
dom House was able to obtain its sig-
nature orange-and-white ambulances,
which were packed with the latest medical
equipment. They continued to carry model
advancements in emergency care while
providing compassionate care to a once-
abandoned community.
As the public began hearing about this
new service, the cry “send Freedom House”
led to a further expansion of the service
into other regions of Pittsburgh, where
Freedom House paramedics often encoun-
tered racial tensions.
The expansion continued, and the ser-
vice hired an increasingly integrated work-
force. In 1974, Safar assigned a young critical
care resident, Nancy Caroline, MD, as the
new medical director of the Freedom House
ambulance service. Caroline often rode out
with the crews, advising them by phone
and catching a brief nap at their station on a
stretcher between shifts.
Caroline was mentor, teacher and friend
to many of the crew members during her
tenure at Freedom House Ambulance. She
led the service through advancements in the
areas of disaster medicine and critical care in
the streets. She even obtained a Department
The EMS Academy became the first EMT class open to the public inside the city limits.
1303JEMS_72 72 2/26/13 4:13 PM

WWW.JEMS.COM MARCH 2013 JEMS 73
of Transportation grant and developed the
first paramedic textbook Nancy Caroline’s
Emergency Care in the Streets, which became one
of the most widely used, and popular, para-
medic textbooks for years.
END OF AN ERA
Despite the involvement and support of clin-
ical leaders, like the outspoken Safar and the
young and ambitious Caroline, the political
winds were shifting in Pittsburgh. A newly
elected mayor chose to replace the Freedom
House paramedics by funding a city-run
ambulance service.
To preserve the original community-
based service, Safar insisted on a written
agreement that “grandfathered” the Free-
dom House paramedics into this new ser-
vice. But once in place, this agreement was
systematically dismantled, leaving only a
fraction of the original personnel. Many
original members, like paramedic pio-
neer John Moon, remained and advanced
through the ranks despite encountering
racial barriers along the way. Others took
their training and experience elsewhere,
becoming leaders in public health and
safety in other major cities.
FAST FORWARD
There’s no shortage of EMTs or paramed-
ics in St. Paul. In fact, the Twin Cities of
Minneapolis and St. Paul have three strong
paramedic schools, and EMS employers
report a large pool of applicants. Why
then would it be necessary to launch a
new and unique recruitment and educa-
tion program for EMS in the area?
The answer is a lack of diversity.
Although official statistics from most
Twin Cities ambulance services are not
kept, Minnesota EMS leaders acknowledge
that less than 2% of paramedics in the
Twin Cities are non-Caucasian.
Although many EMS agencies have
escaped public criticism for their lack of
diversity, the St. Paul Fire Department
(SPFD) has been scrutinized for this over
the past decade. The entrance test and
hiring practices have been the subject of
several contentious lawsuits and many
newspaper stories. In response, SPFD has
been proactive in the recruitment and hir-
ing of diverse candidates.
SPFD may actually be the most diverse
ambulance service in the state. Today, the
department boasts 80 members of diverse
ethnicity (18%) and 19 women (4%) out of its
435 members.1 Some might even ask if 18%
diversity is enough. After all, isn’t the state of
Minnesota 85% Caucasian?
The non-Caucasian populations of St. Paul
and Minneapolis are 37% and 44%, respec-
tively.2,3 This includes large Hmong, Hispanic
and Somali groups—each of whom have
unique language, cultural, and healing prac-
tices. At the time of publication, SPFD has yet
to hire its first Hmong firefighter/EMT, and
other local providers have no black or His-
panic EMTs or paramedics.
The reality is that the issue of diversity in
EMS requires a deeper contextual perspec-
tive and rests on more than just skin color.
If serving our communities with excellent
medical care requires better understanding
of these cultures, couldn’t we just educate
the current workforce?
Becoming more culturally competent
should be the goal of any healthcare pro-
vider, and wouldn’t we also want to hire at
EMS Today Booth #1656
www.firstlinetech.com | @FirstLineTech | [email protected]
How will you use it?
®®®®®
Surge Capacity.Mortuary Response.
Mass Casualty Transport.Firefghter Rehabilitation.
Functional Needs Evacuation.Bus Stretcher Conversion Kit
™.
Choose 47 at www.jems.com/rs
1303JEMS_73 73 2/26/13 4:13 PM

74 JEMS MARCH 2013
least some personnel who are already fluent
in both language and cultural practices of
these groups?
Sadly, if you ask a Hmong, Hispanic
or African-American child from a low-
income family in the inner city what career
they might dream of, “emergency medical
services” is simply not on the top of their
list. Unfortunately, even if it was, their
guidance counselors might be quick to
point out that low pay, difficult access to
expensive training, and a competitive job
market make other careers more attractive.
The educational reality in our inner-city
schools is an economic and racial catastro-
phe. Minnesota’s black and Latino students
have some of the worst reading and math
scores in the country (45 and 38 points lower
than their white counterparts).4 Inner-city
youth of diverse ethnicity have a higher like-
lihood of ending up in the penal system than
in college.
It’s not just a matter of appropriate rep-
resentation and good patient care. Having a
labor force that is representative of the com-
munities that we serve allows economic
opportunity for all of the city’s residents. It
can also save taxpayers millions if we reverse
the path of one young person who might
otherwise be disenfranchised from educa-
tion and employment as a whole.
If even one of these youth at risk
embraces a career, earns a living that sup-
ports their family, and avoids jail, there’s an
average cost savings of $20,000–30,000 per
year in court costs and governmental assis-
tance for food and shelter; the savings to the
taxpayer are significant.5
So you can now see why SPFD’s vision-
ary Chief Tim Butler, jumped at the chance
to work with the city’s already successful
St. Paul Parks and Recreation Department
Youth Job Corps (YJC) and Inver Hills Com-
munity College (IHCC) to start an innovative
new EMS program.
YJC places low-income youth in summer
jobs around the city. In 2009 a surplus of
youth and the dollars to pay them brought
the Parks and Fire departments together. The
initial idea was to have YJC workers help-
ing clean fire stations, much as they help dig
ditches for the highway department or clean
parks facilities. Instead, Butler suggested that
these funds be used to train interested appli-
cants as EMTs.
The EMS Academy provided free EMT
training and an hourly pay of $7.50 per hour
for low-income city residents under the age
of 24 who qualified for YJC. These students
wouldn’t otherwise be able to afford the
training, books, and certification exam costs.
With all of the EMT classes at the time
being offered in suburban colleges that
required difficult commutes, the EMS Acad-
emy became the first EMT class open to the
public inside the city limits.
When the program began to experi-
ence serious challenges in coordinating the
needs of low-income youth, additional part-
nerships became critical. The Community
Action Partnership of Ramsey and Wash-
ington Counties provides a social worker
who can help troubleshoot emergency food,
medical, and shelter needs. Adult basic edu-
cation specialists from the St. Paul Public
School’s Hubbs Center help inside the class-
room providing instructional support, pre-
course work and remediation.
SUCCESS—BUT WHAT KIND?The SPFD hiring list is created nearly every
four years and is highly competitive, with
3,000 initial applicants vying for a small
number of openings. After the first three
EMS Academy classes, the employment sta-
tistics and rates of graduates continuing
to college painted the program in a good
light. However, it also became apparent that
the graduates were securing jobs in many
healthcare venues, e.g., emergency depart-
ments and nursing homes, but not inside
the EMS workforce.
Area ambulance services indicated they
were passing over EMS Academy EMT grad-
uates because of their lack of experience. The
program was at an impasse.
REVIVING FREEDOM HOUSE>> CONTINUED FROM PAGE 73
EMS ACADEMY DIVERSITY BY THE NUMBERSEighty-one EMT class graduates have a
NREMT first-attempt pass rate of 85%.
>> Forty-two percent (42%) of the partici-
pants are African-American.
>> Fifteen percent (15%) are Hispanic.
>> Eleven percent (11%) are Asian.
>> Eleven percent (11%) are Caucasian.
>> Nine percent (9%) are Native American/
American Indian.
>> Ten percent (10%) are multicultural.
>> Two percent (2%) are other.
>> Fifty-four percent (54%) are female.
l
i
t
o
i
t
s
l
g
p
e
m
s
p
h
s
t
y
l
i
r
l
m
o
c
t
o
t
e
p
a
y
t
t
a
PARTICIPANT PROFILESTianna Ross: Prior to
the EMS Academy, Tiana
didn’t consider becoming
an EMT and didn’t have
a clear idea of what to
do after completing high
school. She helps care for
her brother as if she were
a single parent. Near graduation, one of her guid-
ance counselors told her about the summer EMT
class that paid an hourly wage. Ross signed up with
the program and, despite a rocky start, completed
the EMS Academy. She now works on the BLS
service. When asked about how she has changed
as a result of the Academy, Ross states, “When I
was in high school I thought that I was just going
to get a job in retail or fast food and I was going
to stay there for the rest of my life. And since
this program, I know I’m not going to be working
a dead-end job. I know my future is bright, and I
know that good things will come to me.”
Clarence Fraser:
After a brief attempt at
a college football career,
Clarence returned home
to cope with his atten-
tion deficit hyperactivity
disorder. Although his aca-
demics improved, he was
forced to withdraw because he couldn’t afford
the school’s tuition. He enrolled in the 2010 class
of the EMS Academy and is now one of the senior
members of the BLS service. Fraser is completing
his advanced EMT classes and aspires to become a
paramedic at St. Paul Fire.
Koua Xiong: The Twin
Cities are home to the
largest concentrated
Hmong population in
North America. One of the
early calls the BLS service
took was for a Hmong man
who didn’t speak English.
Luckily, Koua Xiong was on the call. Koua, a crew-
member of the BLS service, understood his cultural
and personal needs. Koua remarks, “I was happy
I took the call. I knew from the start that any of
my co-workers would have difficult conversing
and explaining what they were doing.” He learned
about the EMS Academy in a local Hmong news-
paper. When he first started the EMT course, his
reading levels were at seventh grade. After EMT
certification 10 weeks later, he tested at an 11th
grade level. He now works on the BLS service and
with Allina Health EMS, and he’s finishing up his
associate’s degree and paramedic curriculum.
Tianna Ross
Clarence Fraser
Koua Xiong
1303JEMS_74 74 2/26/13 4:13 PM

WWW.JEMS.COM MARCH 2013 JEMS 75
In 2012, an amazing thing
occurred. Three of the origi-
nal members of the Pittsburgh
Freedom House Ambulance
Service delivered inspiring
graduation speeches for the
St. Paul Fire Department EMS
Academy spring class.
Seeing the similarities in
the Pittsburgh and St. Paul projects, But-
ler approved a request to rededicate Station
51, which had been converted into a train-
ing academy, as Freedom House Station 51 in
honor of the original members of Freedom
House ambulance.
During the original members’ St. Paul
visit, a recently released documentary by
Gene Starzenski was screened in a closed
door summit of EMS leaders. The meeting
provided insights as to the systemic barri-
ers that inner-city youth face when seeking
employment in Twin Cities EMS agencies.
Access Gene Starzenski’s documen-tary on the Freedom House website. www.freedomhousedoc.com.
Seeing that competent EMT graduates
weren’t being hired was difficult for admin-
istrators. Although employers often cite the
lack of diverse qualified candidates, the new,
more rigorous requirement of qualified and
experienced candidates was an even bigger
challenge. Graduates’ lack of training, cou-
pled with shrinking grants from founda-
tions, prompted novel action on the part
of the EMS Academy. Regions hospital, a
local Level 1 trauma center which provides
medical direction for SPFD and IHCC, had a
pressing need to transport stretcher bound
discharged patients home. The combination
of these needs propelled a landmark event
in Minnesota EMS: The creation of the SPFD
non-emergency BLS ambulance scheduled
transport service.
A NEW FREEDOM HOUSE
TRANSPORT SERVICE
In July 2012 SPFD, in line with Mayor
Coleman’s youth initiatives, the St. Paul
Department of Human Rights, the Parks
Department, Regions Hospital and IHCC
received City Council approval to launch the
EMS Academy YJC-BLS unit.
Inver Hills instructors volunteered to
coordinate additional training, scheduling
and field supervision. Two college ambu-
lances were leased to the city for $1 to min-
imize start-up costs. Regions Hospital and
Allina Health EMS funded uniforms, pagers
and other operational needs.
The local EMS community embraced the
idea and viewed it as a beneficial partnership
and “feeder system” for diverse employees.
Allina and HealthEast Medical Transporta-
tion, two local private ambulance services
went as far as supporting it with additional
donations and run referrals.
Ten graduates of the EMS Academy were
hired back at $7.50 per hour (without ben-
efits) in a temporary YJC job class with St.
Paul Parks, and placed under the supervision
of SPFD for training. On July 9, 2012, the BLS
service was officially launched. The new ser-
vice has completed more than 500 runs in its
first six months of operation.
The funds generated by the ambulance
service are able to wholly sustain the opera-
tion of the BLS ambulance service, and excess
funds are used to support future Academy
projects. In addition to providing a mul-
tilingual and culturally diverse ambulance
service to St. Paul and receiving accolades
from patients, the crew has found remark-
able success securing jobs. Of the original 10-
member crew, seven now have jobs as EMTs
with local ambulance services.
All SPFD BLS unit workers are required to
attend classes to further their EMS education,
with the goal of attaining paramedic certi-
fication. Beyond those working for the BLS
service, roughly 50% are pursuing further
their education and 70% have found jobs in a
medically related field.
SUMMARY
Freedom House is our national EMS leg-
acy. It was a revolutionary idea born out of
the convergence of political forces. It’s our
EMS history, but it isn’t found in our text-
books. Today we labor over the need to build
workforce diversity, create community para-
medicine and increase physician interaction
during paramedic training. Freedom House
had all of those things, yet we have collec-
tively forgotten.
Freedom House isn’t about being the first.
It’s about believing in the power of each indi-
vidual to achieve success. It’s about building
a system of clinical excellence and responsi-
bility to the public.
The original Freedom House paramed-
ics became known for their advanced medi-
cal care, but to those they treated, they were
known for their compassion and commit-
ment to public service.
Megan Corry, MA, EMT-P, is the Paramedic Program
Director and Primary Instructor at the City College of San
Francisco Paramedic Program and doctoral student at San
Francisco State University. She is also on the Board of
Advisors for the UCLA Prehospital Care Research Forum.
She can be reached at [email protected].
Casey Keyes, BA, NREMT-B, is the Saint Paul EMS
Academy Program Coordinator through AmeriCorps
VISTA. Keyes graduated from St. Olaf College where he
worked as a volunteer EMT. He can be reached at casey.
David Page, MS, NREMT-P, is an EMS instructor at
Inver Hills Community College and supervises the EMS
academy, and the St. Paul Fire YJC-BLS unit. He is a field
paramedic with Allina EMS in the Minneapolis/St. Paul
area. He can be reached at [email protected].
REFERENCES
1. Hallman C. (Jan. 30, 2010). St. Paul wants more black
firefighters. In Twin Cities Daily Planet. Retrieved
from www.tcdailyplanet.net/news/2010/01/30/
st-paul-wants-more-black-firefighters.
2. Reilly K, Santiago T. (Summer 2012). St. Paul Trends
Report. In St. Paul Department of Planning and
Economic Development. Retrieved from www.stpaul.
gov/DocumentCenter/View/60943.
3. U.S. Department of Commerce. (Jan. 10. 2013).
Minneapolis (city), Minn. In U.S. Census. Retrieved
from http://quickfacts.census.gov/qfd/
states/27/2743000.html.
4. Minnesota School Boards Association. (n.d.).
Achievement Gap in Minnesota. In Minnesota School
Boards Association. Retrieved from www.mnmsba.
org/Public/MSBA_Docs/achievementgap.pdf.
5. U.S. Department of Justice. Federal prison system
operation cost per inmate. In U.S. Department of
Justice. Retrieved from www.justice.gov/archive/
jmd/1975_2002/2002/html/page117-119.htm.
RESOURCES
>> Bell RC. The Ambulance: A history. McFarland: Jef-
ferson, N.C. 2008.
“The vital part of what I learned from Freedom House was to help my fellow man.”
—George McCleary,
Freedom House paramedic
1303JEMS_75 75 2/26/13 4:13 PM

76 JEMS MARCH 2013
PH
OT
OS B
OB
VA
CC
AR
O
76 JEMS MARCH 2013
THE BAY SHORE/
BRIGHTWATERS RESCUE
AMBULANCE’S NEW
VEHICLE WILL RESPOND
TO MULTIPLE INCIDENT
TYPES AND PROVIDE
MUTUAL AID
1303JEMS_76 76 2/26/13 4:20 PM

WWW.JEMS.COM MARCH 2013 JEMS 77
>> BY BOB VACCARO
In certain areas around the country, we sometimes see a duplication
of fire services and EMS, not to mention competition—sometimes
downright animosity—between the two. But among the negative
relationships, there are positive examples of fire and EMS working
together in innovative, productive ways.
The Bay Shore/Brightwaters Rescue Ambulance (BSBRA) organiza-
tion, located on Long Island, N.Y., has found a way to provide and expand
service to their community while continually working side by side with
the Bay Shore Fire Department. A great example of this positive relation-
ship is apparent in the latest addition to the BSBRA’s fleet.
MULTIPLE USES
According to BSBRA Chief of Department
Bill Froehlich, the organization first had
the idea to design a special operations
vehicle some 10 years ago. “We already
provide BLS and ALS services to our com-
munity but wanted to expand what we
do,” Froehlich says. “The basic concept was
to have a vehicle with which we could
respond to MCI and rehab incidents. We
didn’t want a heavy-rescue vehicle, because
that would infringe upon what the local fire
department was responsible for.” The idea
took a backburner until BSBRA Assistant
Chief Gerald Guszack started working on
the concept with earnest.
“We had operated with an older ambulance and a van for a long time”
Guszack says. “We really needed more space for our equipment. We also
wanted the vehicle to have 4 x 4 capabilities because we had some areas in
our district that were not accessible with our available vehicles.” Guszack
also specced the vehicle with a front-mounted winch, a light tower, a heat
and air-conditioning unit large enough to power a 15' x 30' tent, a micro-
wave, a refrigerator, life preservers, and BLS and ALS medical equipment.
“Initially we looked around locally and nationally at what other EMS
organizations were using,” Guszack says. “Using the Internet also helped
in our search for a manufacturer to build the vehicle of our choice.” And
this was no simple build. The BSBRA wanted the vehicle to be able to
respond to mass-casualty incidents (MCIs), large fires, rehab, triage, wild-
The Bay Shore/Brightwaters Rescue Ambulance recently took delivery of this special operations vehicle built on a Chevy Kodiak C5500 chassis with body by Custom Fab.
Above: The vehicle is stocked with rehab supplies as well as needed first aid and medical supplies.
A roof-mounted light mast supplies needed lighting to a scene.
A roof-mounted light mast
More about BSBRAThe Bay Shore/Brightwaters Rescue Ambulance operates with five ambulances:
>> 2005 PL Custom
>> Two 2003 PL Custom
>> 1998 PL Custom
>> 2009 Braun
All five vehicles are built on Ford F-350 chassis. The organization also operates
several fly cars and a paramedic ALS vehicle that carries narcotics, telemetry and
defibrillators .
The organization is staffed by 150 volunteer members and four paid members
who work 6 a.m.–6 p.m., with duty crews covering the remainder. The response
district covers eight square miles, with light industrial, restaurants, strip shopping
centers, apartment complexes and a large waterfront area.
During Hurricane Sandy, the company responded to an average of 25 runs per
day for a total of 238 calls from Sunday through Wednesday of that week; 25
members were on duty during the week.
1303JEMS_77 77 2/26/13 4:20 PM

BUILT TO SHARE >> CONTINUED FROM PAGE 77
78 JEMS MARCH 2013
fires, hurricanes and any other major disas-
ter locally and even in a mutual-aid capacity
throughout Islip, Suffolk and Nassau coun-
ties, and the five boroughs of New York City.
WORKING TOGETHER
Before the BSBRA purchased the vehicle,
it met with the chiefs of the Bay Shore Fire
Department. “We discussed what we want-
ed to accomplish with the response of the
vehicle,” Froehlich says. “Normally we have
two ambulances respond to every fire scene,
so this would be an additional option should
the vehicle be needed. We explained that we
weren’t trying to step on anyone’s toes and
that we would like to work with them at all
emergency scenes. They welcomed the idea
100%, which alleviated a great deal of stress.”
Like most organizations, the BSBRA went
out for competitive bidding. “We received
quotes from three manufacturers,” Froehlich
says. “Great Lakes Specialty Vehicles repre-
sented Custom Fab & Body of Marion, Wis.
We felt that Custom Fab was good for us,
simply based on the fact that their company
had built similar vehicles for other agencies
nationwide.”
Custom Fab also gave the BSBRA a great
price. “Since we didn’t have grant money,
this helped us out a great deal,” Froehlich
says. “Our budget comes from a special
ambulance district tax, so price was impor-
tant for us going forward with the purchase.”
Representatives from the BSBRA traveled
to Custom Fab on at least four occasions to
meet with engineers and oversee the build
process. “They offered suggestions on what
would or wouldn’t work, as well as being
receptive to our ideas and implementing
most of them,” Froehlich says. “The vehicle
was delivered in record time and has worked
out well for us. It came just in time for
Hurricane Sandy.” The BSBRA fondly calls it
Hercules. (For a related article on Hurricane
Sandy response, see p. 38.)
GET CREATIVE
The BSBRA was proactive in their thinking.
They planned for this purchase more than
10 years ago and designed the vehicle to
not only help them expand their service to
the community, but also to help the local
fire department and other organizations
through mutual aid.
Preplanning in advance for your
response district’s needs should be your
first priority in any vehicle purchase. Also
take into consideration budget constraints,
and how the vehicle will respond and be
used. In today’s poor economy, sharing
equipment among agencies and work-
ing together is a great concept—one that
should be expanded upon all over the
country.
Bob Vaccaro has more than 30 years of fire service
experience. He is a former chief of the Deer Park (N.Y.)
Fire Department. Vaccaro has also worked for the
Insurance Services Office, the New York Fire Patrol
and several major commercial insurance companies as
a senior loss-control consultant. He is a life member
of the IAFC.
The rear A/C and heating unit is powerful enough to heat or cool a large tent.
The BSBRA also operates this ALS paramedic vehicle.
One of five ambulances operated by Bay Shore/Brightwaters Rescue Ambulance.
The rear A/C and heating unit is powerful
TThe BSBRA also operates this ALS paramedic vehicle
One of five ambulances operated by Bay Shore/Brightwaters Rescue Ambulance
A Closer LookThe Bay Shore/Brightwaters Rescue Ambulance’s
new rescue vehicle is built on a 2009 Chevrolet
C5500 Kodiak crew cab chassis with Duramax
diesel engine and Allison automatic transmission.
The OEM front bumper was removed and replaced
with a Buckstop bumper that houses a recessed-
mounted Warn 16,000-lb. winch. The truck is
equipped with an Onan 20-kW Protec PTO gen-
erator that powers a Will-Burt NS4.5-9000(OPT)
9,000-watt light mast and two Hannay electric
rewind cable reels with 200 feet of 8/3 cable. The
body is a 13' all-aluminum walk-around rescue-style
body equipped with ROM aluminum roll-up doors.
The body top features two coffin compartments,
one on each side of the body with a center walk-
way. These compartments are equipped with mul-
tiple adjustable shelves and slide-out trays, includ-
ing a dual direction tray. Other features include a
Whelen M Series Super LED warning-light package
and Whelen Pioneer LED scene lights.
1303JEMS_78 78 2/26/13 4:20 PM

JEMS makes a great appreciation
gift, retention tool or incentive.
Take advantage of discounts
on multiple subscriptions.
A one-year subscription to JEMS consists of twelve issues including
the Buyer’s Guide and Hot Products
issues.
Call: (888) 456-5367 or visit www. JEMS.com
Reward your personnel with a subscription to JEMS.
1303JEMS_79 79 2/26/13 4:21 PM

80 JEMS MARCH 2013
Dominic Silvestro, EMT-P, EMS-I, is
a firefighter/paramedic for the
Richmond Heights (Ohio) Fire
Department. He is also an EMS
coordinator and EMS educator for the Univer-
sity Hospitals EMS Training and Disaster Prepared-
ness Institute and an adjunct faculty member at
Cuyahoga Community College. He can be reached
HANDS ONPRODUCT REVIEWS FROM STREET CREWS
>> IN THE NEXT ISSUE: Whelen 360 Degree Remote Control Spotlight >> Rayovac On-The-Go Battery Charger >> Panasonic Toughpad Tablets
VITALS
Color: White
Sizes: Medium (8", with green cuffs),
large (9", with yellow cuffs) & XL (10", with brown cuffs)
Price: $1.69 per pair
www.keybomedical.com
877/855-3199
O2 for Mass Casualty Incidents
Here is a quick math problem. How many additional ambulances
do you need to provide emergency oxygen to eight patients?
Now how many ambulances do you need to provide emer-
gency oxygen to 16 patients? If you have the Multi-Manager
O2 Administrator from Spiracle Technology/Ferno, the answer
to this math problem is one ambulance. The Multi-Manager O2
Administrator has eight flow-control valves that are manifolded
together. The manifold is mounted to a collapsible aluminum
alloy tripod. Two Multi-Managers can be connected in a series
allowing you to provide oxygen to 16 patients. Independent
flow settings are: OFF, ¼, ½, 1, 2, 3, 4, 6, 8, 10, 15 and 25 LPM. A
dust case is included.
ACLS? PALS? There Are Apps for ThatThere’s nothing worse than test anxiety. Over years of teaching ACLS and PALS
courses, I have seen everything from students’ hands shaking to breaking out
in hives on test day. The ACLS and PALS Review Apps from Limmer Creative
give you high-quality, realistic practice examinations to help you prepare for
your ACLS and PALS tests. These apps are easy to use and are based on the
2010 American Heart Association guidelines. There are four, 25 question exams
that include scenario-based questions just like the questions you will see on
your ACLS or PALS test. After submitting your answer to each question, you
are immediately told whether your answer is correct, and a detailed rationale is
given for that answer to help you to improve and gain confidence in your ACLS
and PALS knowledge. There are also integrated ECG strips to help you with your
interpretation skills. The apps run on Apple iOS and Android based products.
Keep Your Hand WarmIf you have worked an emergency run in
extremely cold temperatures you quickly real-
ize that your medical gloves provide you with no
protection from the elements. The gloves even
seem to attract the cold to your hand and make
it difficult to perform your job. Medical Glove
Warmers from KEYBO Medical are ultra-thin lin-
ers that are thin enough to wear under your
medical gloves. Made from 100% nylon, the glove
warmers seamless knit allows for the stretch
necessary for a close comfortable fit under your
medical gloves. The middle and index fingers are
open at the tip. This allows for the sensitivity you
need when taking a pulse on your patient.
VITALS
Operating system:
Apple iOS, Android
Web version:
www.LC-Ready.com
Price: $3.99 each
www.limmercreative.com
VITALS
Dimensions when setup: 10.5" H x 18" L x 7" W
Dimensions when stored: 2.75" H x 18" L x 6" W
Weight: 6 lbs.
Price: $1,145
www.spiracle.com
714/418-1091
1303JEMS_80 80 2/26/13 4:14 PM

VITALS
Color: Blue
Dimensions: 72" L x 18" W x 2.75" H
Weight: 22 lbs.
Price: $1,249
www.ezliftrescue.com
435/214-7141
WWW.JEMS.COM MARCH 2013 JEMS 81
>> Chinook Medical Gear Medical Operator TMK-MO >> North Coast Outfitters SR601J-49UW Stretcher >> Hartwell Medical BioHoop Collection Bag
For more product reviews: www.jems.com/tags/Hands-On
Not Your Typical Multi-ToolsThe Raptor Medical Shears are the latest in
a long line of multi-tools from Leatherman.
Developed over an 18-month period, the
Leatherman team worked closely with spe-
cial operations medics as well a fire/EMT
professional. The Raptor Medical Shears
are the result of these collaborations. The
420HC stainless-steel medic shear also
includes an oxygen wrench, strap cutter, a
carbide tip glass breaker and a ring cutter.
All of the extra features on the shears can
be used with the tool open or closed. The
handles are made from glass-filled nylon
that provides a secure grip and comfort in
hot or cold weather conditions. The sheath
allows you to store the shears in the open
or closed position and rotates for your
comfort. A removable pocket clip and lan-
yard attachment provides additional non-
sheathed carry options.
VITALS
Color: Black handle
with stainless shears
Weight: 5.8 oz.
Size: Shear length 1.9",
closed length 5"
Price: $70
www.leatherman.com
800/847-8665
Reduce Back InjuriesLifting with proper technique is an important
factor in reducing and/or preventing back inju-
ries. Unfortunately, lifting a patient who is on a
backboard from the ground to your stretcher
causes excessive torque on lower back muscles
and knees. The EZ LIFT Rescue System from EZ
LIFT Rescue Systems reinvents the traditional
backboard. Designed with extendable handles,
the EZ LIFT Rescue System allows crew members
to lift from a safe position at or above the knees.
The handles can be used for two, three or four
person carries. The system comes ready to use
right out of the box and is rated for up to 1,000
lbs. The EZ LIFT Head Bed lives on the board and
is a comfortable and effective way to immobi-
lize a patients head during transport. Head Bed
replacements are sold separately or with the dis-
posable adhesive head straps.
1303JEMS_81 81 2/26/13 4:14 PM

“Nothing is at last sacred but the integrity of your own mind.”
—Ralph Waldo Emerson
T he jovial cackle reverberated loudly
off the captive walls—an unlikely
resonance from such a sad and cus-
tomarily dispirited place. I hate this neces-
sitated habitat as much as I hate the disease
that stole them from me. Yet, I could not
help but generate a small grin knowing
the incessant laughter I was now tracking
would eventually lead me to them— begin-
ning with my mother, whose laughter is
so clearly identifiable, so boisterous and
delightfully contagious that even those out-
side the circle hypnotically gather to its
source. Find my mother and I will find my
father. She’s the only person he now recog-
nizes, and they’re inseparable.
Just as before, I found them sitting in the
lounge of their Alzheimer’s residence home,
holding hands. Today, however, it was my
mother’s birthday and she was rewarding
her self-imposed wit with nonstop laughter
after complaining about the cook’s blender,
which was no doubt being used to puree a
patient’s food, not being subjugated to make
her a margarita.
“Happy birthday, Ma!” I whispered loudly
so I didn’t frighten my father. Her eyes grew
large as she reached to hug me. My father
simply looked at me with curious uncer-
tainty. “Birthday? What birthday?” she
blurted. “We’re celebrating your father finally
paying off his college student loan.” Not
waiting for a reaction, my mother once again
laughed at her cleverness.
“How old are ya, Ma?” I asked as I smiled.
“Old enough not to give a $%#!,” she
roars in between chortles. “All I know is I’m
so old that all my friends in heaven think I
didn’t make it… or is it hell? %$#! Where’s
my margarita?”
Today was a good day for my parents.
My father was alert and my mother wasn’t
repeatedly asking the same questions over
and over again. They appeared happy and,
despite the series of small strokes (vascu-
lar dementia) that had raped my father’s
brain, he was smiling each time my mother
laughed. This is a sign of humor’s capacity to
survive and sooth, I suppose.
My mother’s dementia was diagnosed five
years earlier—fifteen years after my father’s
symptoms first began to appear. My mother
is old-school; despite how his disease pro-
foundly changed her, she insisted on tak-
ing care of my father alone up until her own
cruel collection of cerebral symptoms began
to manifest themselves, thereby making it
impossible for either of them to be without
the consistent care of assisted living.
I had felt blessed that my father’s retire-
ment would provide them with a safe, clean,
and stimulating environment for the rest of
their lives, so it breaks my heart every time
I enter this regrettable facility—a facility so
familiar to those of us in EMS.
“Where’s the music? We need music in this
%$#! Place!” my mother cursed sarcastically.
“How about the Village People’s, Y-M-C-
A… except that we’ll sing it A-A-R-P,” I pro-
posed straight-faced. My mother furrowed
her brow for a second, thinking about what
I had just said and then imparted a high-
pitched giggle that grew into a pulverizing
snort. Delightfully surprised by the unex-
pected sound, she roared laughter until her
eyes were filled with tears.
“Now look at what you’ve done,” she whis-
pered back at me loudly. Not waiting for an
answer, she turned to one of the aides stand-
ing nearby yelling, “Hey Marge. These dia-
pers aren’t going to change by themselves!”
Again, my mother cackled as I tried to find a
tissue to dry her eyes.
As more residents began to gather around
our small family get-together, it became
increasingly clear that even in their late stages
of dementia, these confused strangers hun-
gered for more than just my mother’s birth-
day cake. They were invigorated by the smiles
and laughter and wanted to be a part of
it—except for one elderly woman who kept
THE LIGHTER SIDEWHAT THEY DIDN’T TELL YOU IN MEDIC SCHOOL
>> BY STEVE BERRY
82 JEMS MARCH 2013
THE SLOW FAREWELLIf you can’t do anything else, laugh
1303JEMS_82 82 2/26/13 4:15 PM

WWW.JEMS.COM MARCH 2013 JEMS 83
yelling out each time my mother laughed,
“What’s so %$#! funny?!” (This, by the way,
only provoked my mother’s laughter to an
even more brazen level.)
It’s important to empower oneself with
humor during those silly moments that
Alzheimer’s can produce. Why shouldn’t
laughter bargain its way in whenever pos-
sible? My mother’s mantra has always been,
“What are ya gonna do? So laugh #@$!”
“Hey ma! Knock! Knock! “Who’s there?” I
asked. My mother grinned.
“HIPAA,” I said.
“HIPAA who?” she eagerly asked back.
“Sorry, can’t tell ya,” I said.
She laughed on cue, just like I knew she
would. “Get it?” I asked her.
“No,” she chuckled. “But it made you laugh,”
she added as she playfully slapped my cheek.
Mothers are good for that.
As I prepared to leave, I could see the smile
slowly fade from my mother’s face, despite
her best effort to show otherwise. Despite all
the laughter, I knew she was ready to leave
this world of confusion and separation.
I couldn’t hide my despair. Her scrapbook
was fading before my eyes. As I averted my
eyes, she grabbed my arm and said, “And
don’t worry about your father. He’s always
by my side. Where else am I going to apply
my Post-it notes?”
Occasionally I see my parents’ eyes in those
geriatric patients my ambulance responds
to—especially those who use humor to
maintain what’s left of their dignity while in
transit. I now regret not being more com-
passionate during my novice years as a para-
medic toward those who cannot recall what
happened 20 minutes ago, much less 20 years
ago. They deserved better from me.
As for my parents, I’m not sure how long
their remembrances and laughter will last,
but I treasure the gift of comical relief that
my mother has instilled in me since the time
the diapers were reversed, and I pray that
it continues to allow my parents to thrive
despite their undeserved clinical prognosis.
Thanks, Ma. You are, and always will be, my
favorite fan.
Until next time, remember: What are ya
gonna do? So laugh $#@!
Steve Berry is an active paramedic with Southwest
Teller County EMS in Colorado. He’s the author of the
cartoon book series I’m Not An Ambulance Driver. Visit
his Web site at www.iamnotanambulancedriver.com
to purchase his books or CDs.
Choose 48 at www.jems.com/rs
Choose 49 at www.jems.com/rs
1303JEMS_83 83 2/26/13 4:15 PM

84 JEMS MARCH 2013
Employment
The NREMT EMS Fellowship is
a rare opportunity to pursue a
doctoral degree while benefiting
from mentoring, hands-on
research skill development, and
a unique education at both the
NREMT and The Ohio State University (OSU).
You must be highly motivated and committed
to positively impact EMS on a national level.
Research Fellows receive fully-funded tuition
while pursuing graduate studies at OSU. Work
responsibilities at the NREMT will include
research activities, conference presentations,
committee memberships, running projects, and
publications.
The ideal candidate is a Nationally Certified,
field-experienced EMS professional possessing
a Bachelor’s degree. Successful candidates
must be able to gain admission to OSU graduate
school for an approved Master’s and Doctoral
studies program.
To be considered for the position, please send
a cover letter and your resume or vitae to
Melissa Bentley, NREMT, P.O. Box 29233,
Columbus, OH 43229 or [email protected]
by April 12th, 2013.
The NREMT is an equal opportunity employer.
NREMT EMS RESEARCH
FELLOWSHIP POSITION
AVAILABLE
Eastern Kentucky University, located in Richmond, KY, is accepting applications for a tenure-
track Assistant or Associate Professor in the Emergency Medical Care (EMC) Program to start
August 2013. The EMC program is accredited by the Committee on Accreditation of Educational
Programs for the Emergency Medical Services Professions (CoAEMSP) and offers Associate and
Baccalaureate degrees. The primary responsibilities may include EMT and Paramedic instruc-
tion, classroom and on-line instruction, student advising, and engaging in scholarly and profes-
sional service activities. Position Responsibilities: Ensures academic preparation of EMTs and
Paramedic students; Teaches CPR, ACLS, PALS, and emergency medical responder courses;
Coordinates and oversees clinical/field experiences of EMT or paramedic students; Advising for
an assigned group of students; May act as a faculty advisor for student organizations; May teach
Continuing Education programs on and off site; Ensures equipment is operational, up-to-date
and in good working order; Works closely with administration; meets with students on a regular
basis; assures all American Heart Association procedures are followed; Assists in completion of
all evaluations and assessments; Engages in scholarly activities (including regional and national
publication, presentations, etc.); Organizes, schedules, and oversees education and training at
all levels; And performs other duties consistent with the University Faculty Handbook. A Master's
degree required from a regionally accredited or internationally recognized institution by the time
of appointment. Applicants must also hold Current Paramedic or Registered Nurse licensure with
current NREMT by time of appointment and have 3-5 years of related experience--some of which
must be in out-of-hospital emergency care. All interested applicants must apply at
jobs.eku.edu for consideration (search requisition #0612858).
All offers of employment are contingent on completion of a satisfactory background check. Eastern Kentucky University is an EEO/AA institution that values diversity in its faculty, staff, and student body. In keeping with
this commitment, the University welcomes applications from diverse candidates and candidates who support diversity.
EASTERN KENTUCKY UNIVERSITY
Assistant or Associate Professor inthe Emergency Medical Care
1303JEMS_84 84 2/26/13 4:16 PM

WWW.JEMS.COM MARCH 2013 JEMS 85
Equipment
Employment Employment
ParamedicsFull-Time, Days & Nights and Per Diem
Certified as a Paramedic by the State of New Jersey, current BLSHCP, ACLS, PALS or PEPP certifications required.
Specialty Care Transport RNFull-Time, Days & Nights and Pool
Must have one year of full-time nursing care performing advanced clinical skills in the Critical Care Unit or Emergency Department. Possess Emergency Medical Technician - Basic, Health Care Provider CPR and ACLS. Possess PALS, PEPP or has successfully completed the Emergency Nurse Pediatric Course. Possess either PHTLS or BTLS. NJ Paramedic or National Registry Paramedic Certification is preferred. Also, CCRN or CEN is preferred.
EMT-BPer Diem/Pool
Current National Registry and/or New Jersey Emergency Medical Technician - Basic Certification required. Current BLSHCP (professional rescuer or healthcare provider level) required.
Emergency Medical CommunicatorsFull-Time and Per Diem
Knowledge of local EMS systems/radio communications required. Certifications include BLSHCP, Emergency Medical Dispatch certification, National Registry or New Jersey Emergency Medical Technician - Basic Certification. Proof of completing ICS Courses ICS 100 and IS 700 required. 2 years’ experience is preferred.
AtlantiCare is a great place to work with excellent benefits and real opportunities for career growth. In fact, 94% of AtlantiCare employees say they would recommend working at AtlantiCare to friends or family. We are also the recipient of the 2009 Malcolm Baldrige National Award for Quality. Join us and help make a difference, one person at a time. We have the following opportunities at our Egg Harbor Township location.
Apply online at www.atlanticare.org. EOE, m/f/d/v
HAVE OPEN POSITIONS?
Get them f lled with a JEMS recruitment classif ed.
Reach our audience with your message!
Eastern Region: Judi Leidiger, [email protected],
619-795-9040
Western Region: Cindi Richardson, [email protected],
661-297-4027
1303JEMS_85 85 2/26/13 5:08 PM

Exclusively for EMS Management
POWERFUL SOLUTIONS
FROM SMART THINKERS
EMS Insider provides you with the “inside information” on EMS. It’s a monthly publication
from PennWell and affiliated with JEMS (Journal of Emergency Medical Services) so it has
the best network of sources in EMS. That means you get only the highest quality reporting .
. . insightful, timely, authoritative. . . not available elsewhere. EMS Insider pays for itself. Every
issue contains articles to help you, by bringing you money-saving and revenue-generating
ideas. Don’t miss out, order your subscription today!
Subscribe to EMS Insider
www.JEMS.com
avoid pending lawsuits
�����
����
�������
EMS TrendAnalysis
EMS Research & Technology
revenuegenerating
ideasAVOID
COSTLY FINES
1303JEMS_86 86 2/26/13 4:16 PM

ad directYour source for immediate information on advertisers’ products and services
Advertiser RS# Page Advertiser RS# Page
FREE advertiser and product informationwww.jems.com/rs
IT’S FAST, IT’S EASY AND JUST A CLICK AWAY!WWW.JEMS.COM MARCH 2013 JEMS 87
ADVANCED CIRCULATORY SYSTEMS INC. 13 2
AMERICAN HEART ASSOC. 28 33
AMERICAN MILITARY UNIV. 41 62
B BRAUN MEDICAL INC. 18 13
BOUND TREE MEDICAL 11 C2
CENTRAL WASHINGTON UNIV. 37 47
CINDY ELBERT INSURANCE SERVICES 45 65
COLUMBIA SOUTHERN UNIV. 46 65
COMPX SECURITY PRODUCTS 25 31
DEMERS AMBULANCES 21 21
ECOLAB 26 31
EMERGENCY MEDICAL PRODUCTS, INC. 34 45
FIRST LINE TECHNOLOGY LLC. 47 73
FITCH & ASSOCIATES 24 27
HAIX NORTH AMERICA INC. 29 34
HARTWELL MEDICAL 20 19
INTL ASSOCIATION OF FIRE CHIEFS 57
JUNKIN SAFETY APPLIANCE CO. 39 59
KNOX COMPANY 49 83
LAERDAL MEDICAL CORP. 51 C4
LMA NORTH AMERICA 19 15
M2 INC. 36 47
MASIMO 16 7
MERCEDES BENZ 17 9
MERCURY MEDICAL 22 23
MOORE MEDICAL CORP. 30 35
NAEMT 40, 43 59, 65
ONSPOT OF NORTH AMERICA 44 65
OXYGEN GENERATING SYSTEMS INTL. 48 83
PENNWELL CORP. 17, 59, 67, 69, 79, 86
PHYSIO-CONTROL INC. 14 4
PINNACLE 2013 38 49
PULMODYNE 15 6
SANSIO 32 37
SPRINT 23 25
STRYKER EMS 50 C3
TEXAS A&M ENGINEERING EXTENSION SERVICE 33 43
VIDACARE CORP. 35 45
WHELEN ENGINEERING CO., INC. 42 63
WITMER PUBLIC SAFETY GROUP 31 37
ZIAMATIC CORP. 27 32
ZOLL MEDICAL 12 1
Advertiser RS# Page
1303JEMS_87 87 2/26/13 4:16 PM

minutes of the initial call, she says. By the time
EMS providers arrived on scene, the patient
didn’t need any more shocks.
“The officers are moving. They’re already
on their way when the call comes in,” Olejnik
says. Oceanside police officers aren’t required
to check out AEDs, but an AED is standard
equipment for San Diego Harbor, which has
the highest save rate out of the law enforce-
ment agencies in the county. Olejnik says San
Diego Project Hearbeat uses this information
to go after grants that will help them provide
more AEDs for officer vehicles, which she
says officers can use on patients or even on
each other if necessary.
“It’s just another tool,” Olejnik says, adding
that the program just received an initial grant
to put at least one AED on a San Diego Police
Department vehicle in each division.
We congratulate law enforcement agen-
cies like Oceanside Police Department and
San Diego Harbor Police for pairing up with
EMS agencies to ensure their officers are
equipped to save lives of sudden cardiac
arrest patients.
LAST WORDTHE UPS & DOWNS OF EMS
88 JEMS MARCH 2013
PATIENT DATA PLEDGE
In January, ZOLL Medical Corpo-
ration made a pledge that will facilitate the
360-degree patient data sharing that will help
EMS agencies improve their quality assur-
ance programs—ultimately improving over-
all patient care.
The company made the pledge to allow
data-sharing between ZOLL defibrillators
and non-ZOLL data systems at the Masimo
Foundation Patient Safety, Science & Tech-
nology Summit. An example, they stated in
a prepared statement, is when EMS services
transit 12-lead ECG data to a receiving hospi-
tal and each system uses data systems made
by different manufacturers.
ZOLL Chief Executive Officer Richard A.
Packer said in the statement, “It’s all about
connecting our devices to everyone’s devices
to help improve patient care. From a patient
perspective, providing data from ZOLL
devices and integrating the information to
other devices is doing the best we can for the
patient.” We applaud ZOLL Medical Cor-
poration for taking the first step in breaking
down the walls of data ownership and mak-
ing medical devices interoperable for the
sharing for patient data, and we encourage
other medical device manufacturers to take
the leap as well. EMS providers and patients
everywhere will benefit.
POLICE OFFICER AEDS
On Super Bowl Sunday, San Diego
Project Heartbeat received great news. An
Oceanside Police Department officer saved a
civilian in cardiac arrest outside a Starbucks.
Oceanside (Calif.) Police Department is
one of the agencies in the San Diego County
area that provides its officers, who are so
often the first responders on scene, with the
opportunity to check out an AED for their
shift. “They’re on scene first. They’re there
before EMS is there,” San Diego Project Heart-
beat Community Relations Specialist Loralee
Olejnik says. “We’ve really been pushing to
get AEDs out in law enforcement vehicles just
because we have had so much success.”
The officer credited with the Super Bowl
Sunday save got to the Starbucks within five
JEMS (Journal of Emergency Medical Services), ISSN 0197-2510, USPS 858-060, is published 12 times a year (monthly) by PennWell Corporation, 1421 S. Sheridan Road, Tulsa, OK 74112; phone 918/835-3161. Copyright © 2013 PennWell Corporation. SUBSCRIPTIONS: Send $44 for one year (12 issues) or $74 for two years (24 issues) to JEMS, P.O. Box 3425, Northbrook, IL 60065-9912, or call 888/456-5367. Canada: Please add $25 per year for postage. All other foreign subscriptions: Please add $35 per year for surface and $75 per year for airmail postage. Send $20 for one year (12 issues) or $35 for two years (24 issues) of digital edition. Single copy: $10.00. POSTMASTER: Send address changes to JEMS (Journal of Emergency Medical Services), P.O. Box 3425, Northbrook, IL 60065-9912. Claims of non-receipt or damaged issues must be filed within three months of cover date. Periodicals postage paid at Tulsa, Oklahoma and at additional mailing offices. Advertising information: Rates are available at www.jems.com/about/advertise or by request from JEMS Advertising Department at 4180 La Jolla Village Drive, Ste. 260, La Jolla, CA 92037-9142; 800/266-5367. Editorial Information: Direct manuscripts and queries to JEMS Editor, 4180 La Jolla Village Drive, Ste. 260, La Jolla, CA 92037-9142. No material may be reproduced or uploaded on computer network services without the expressed permission of the publisher. JEMS is printed in the United States. GST No. 1268113153.
INNOVATIVE RESCUE
TRAINING
In June 2012, a one-of-a-kind vehicle rolled into the
Kansas Fire & Rescue Training Institute. Their new
grain engulfment rescue training vehicle is a custom
35' trailer that includes a grain bin, grain hopper and
a metal cutting station that allows them to replicate
(to the extent possible) the “real world” environ-
ment in which grain rescues occur.
The grain engulfment rescue course is deliv-
ered in local communities throughout Kansas and
is unique for a state fire and rescue service training
organization. Participants from the local fire depart-
ment and the local grain facility are encouraged to
train together. “The philosophy used recognizes
that during grain emergencies, employees of the
grain handling facility are an integral part of the res-
cue,” explains institute director Glenn Pribbenow.
“By training together, firefighters and grain facility
employees will be able to form a true team working
to accomplish the rescue.”
Institute staff has used the vehicle to teach
more than 750 students in 47 grain engulfment
rescue classes. An additional 42 classes are sched-
uled through the remainder of 2013 and into
2014, notes Pribbenow, with more requests being
received daily.
Both thumbs are up to the Kansas Fire & Rescue
Training Institute at the University of Kansas Con-
tinuing Education for their collaborative and inclu-
sive training approach as well as for the design of
their unique simulation vehicle.
The Kansas Fire & Rescue Training Institute’s grain engulfment rescue training vehicle unit was made possible by a $90,000 donation from the Kansas Feed & Grain Association, the Kansas Cooperative Council and the Kansas Farmers Service Association.
PH
OT
OS C
OU
RT
ESY
KA
NSA
S F
IRE &
RESC
UE T
RA
ININ
G I
NST
ITU
TE
1303JEMS_88 88 2/26/13 4:18 PM

INTRODUCING
THE ALL IN ONE SOLUTION FOR A VARIETY OF PATIENTS AND ENVIRONMENTS.
XPS provides a stable, expandable patient surface area that can be easily retrofitted to work
with compatible cots.1 XPS is adjustable with 7 locking positions and a wider mattress, designed
with patient comfort in mind. For more info, call 800.874.4336 or visit www.getxps.com
1Power-PRO XT, Power-PRO TL and Performance-PRO
XPS expandable patient surface
Choose 50 at www.jems.com/rs
1303JEMS_C3 C3 2/26/13 2:43 PM

Team Training in Realistic Environments
©2013 Laerdal Medical. All rights reserved. Printed in USA. #13-13250
laerdal.com/essential
�������� ���� ��������� ������� �� �������� �� ������� ���� �������
������ ���� ���� ������ �� �������� �������� ��� ���� � ������
������� ���� ��������� �� �������� ������������ �� ���� ������ ���
����������������������� ������� ������������������������������������
���� ��� ������� �� �������� ��� �� ������ � ����� �� �� ����
���������������������������������® Essential bring greater realism
�� ����������� ��������� ���� �������� ����� �� �������������� ����
����������������������������� ������
SimMan® Essential
See SimMan Essential
test team competency during
the 2013 JEMS Games
Competition!
Scan code to watch a team training cardiac arrest scenario
featuring SimMan Essential
Choose 51 at www.jems.com/rs
1303JEMS_C4 C4 2/26/13 2:43 PM




















![Controlledenviro20130708 Dl[1]](https://img.pdfslide.net/doc/110x75/577cdb171a28ab9e78a74a35/controlledenviro20130708-dl1.jpg)

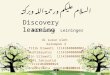




![Yun Li Presentation Dl[1][1]1[1]](https://img.pdfslide.net/doc/110x75/545b3ecab1af9fba5d8b586d/yun-li-presentation-dl1111.jpg)