Embed Size (px)
Citation preview
Metastatic Colorectal Cancer Treatment Platform Algorithm in 2017
Mohamed Abdulla M.D.Prof. of Clinical Oncology
Head of Gastrointestinal Malignancies UnitCairo University
KIOW 3rd EditionKhartoum – Corinthia Hotel25/11/2017
Member of Advisory Board, Consultant, and Speaker for:
• Amgen, Astellas, AstraZeneca, Hoffman la Roche, Janssen Cilag, Merck Serono, Novartis, Pfizer, Mundipharma, MSD, Ely Lilly.
• This Presentation does not relate to any pharmaceutical of commercial interest.
Speaker Disclosures:
Colon Cancer:Basic Facts & Figures:• 2nd & 3rd most common cancers in females and males.
• 9% of cancer related deaths.
• 90% occurring around the age of 40 – 50 years.
• OAS for entire patients = 65%.
• Metastatic disease: 5-year OAS = 10%.
• Organ limited metastatic disease (Metastatectomy):
5-year OAS > 40%
• Median survival of metastatic disease > 35 months.
• Improved OAS with exposure to all available drugs.
• Unified global treatment algorhytm is still controversial.
uptodate.com Accessed 01/11/2017
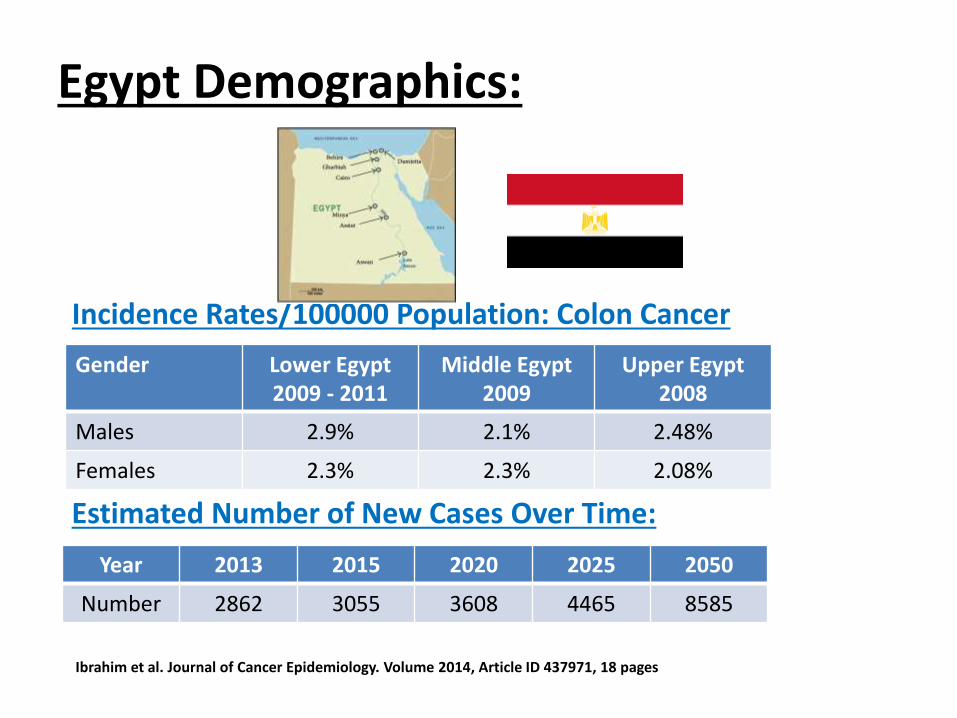
Egypt Demographics:
Gender Lower Egypt2009 - 2011
Middle Egypt2009
Upper Egypt2008
Males 2.9% 2.1% 2.48%
Females 2.3% 2.3% 2.08%
Incidence Rates/100000 Population: Colon Cancer
Year 2013 2015 2020 2025 2050
Number 2862 3055 3608 4465 8585
Estimated Number of New Cases Over Time:
Ibrahim et al. Journal of Cancer Epidemiology. Volume 2014, Article ID 437971, 18 pages
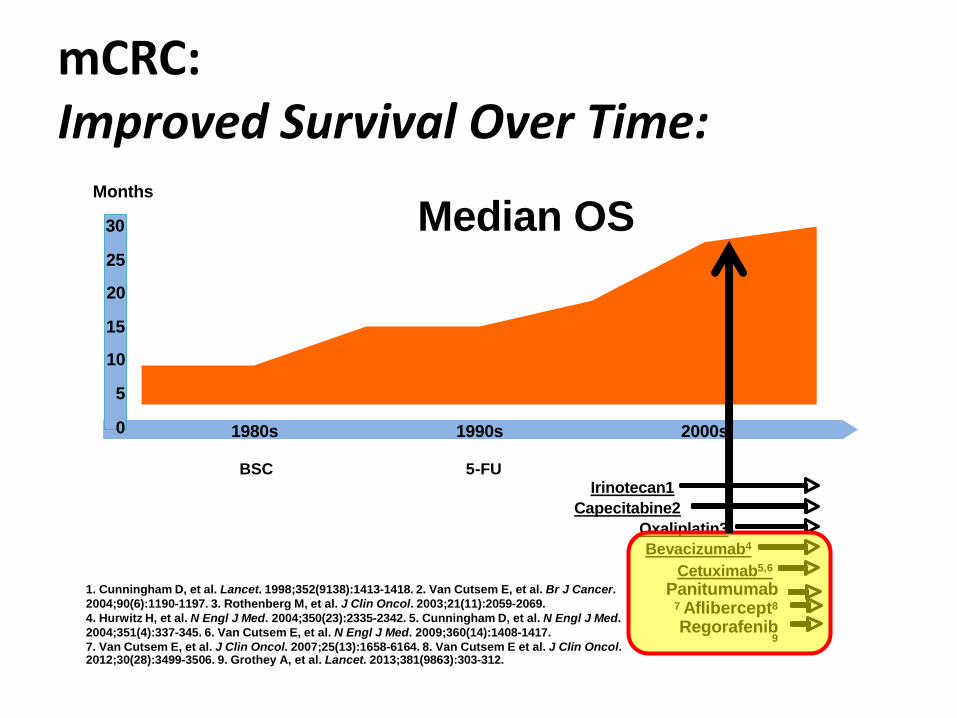
Median OSMonths
1980s 1990s 2000s
BSC 5-FUIrinotecan1
Capecitabine2
Oxaliplatin3
Bevacizumab4
Cetuximab5,6
Panitumumab7 Aflibercept8
Regorafenib9
30
25
20
15
10
5
0
1. Cunningham D, et al. Lancet. 1998;352(9138):1413-1418. 2. Van Cutsem E, et al. Br J Cancer.
2004;90(6):1190-1197. 3. Rothenberg M, et al. J Clin Oncol. 2003;21(11):2059-2069.
4. Hurwitz H, et al. N Engl J Med. 2004;350(23):2335-2342. 5. Cunningham D, et al. N Engl J Med.
2004;351(4):337-345. 6. Van Cutsem E, et al. N Engl J Med. 2009;360(14):1408-1417.
7. Van Cutsem E, et al. J Clin Oncol. 2007;25(13):1658-6164. 8. Van Cutsem E et al. J Clin Oncol.2012;30(28):3499-3506. 9. Grothey A, et al. Lancet. 2013;381(9863):303-312.
mCRC: Improved Survival Over Time:
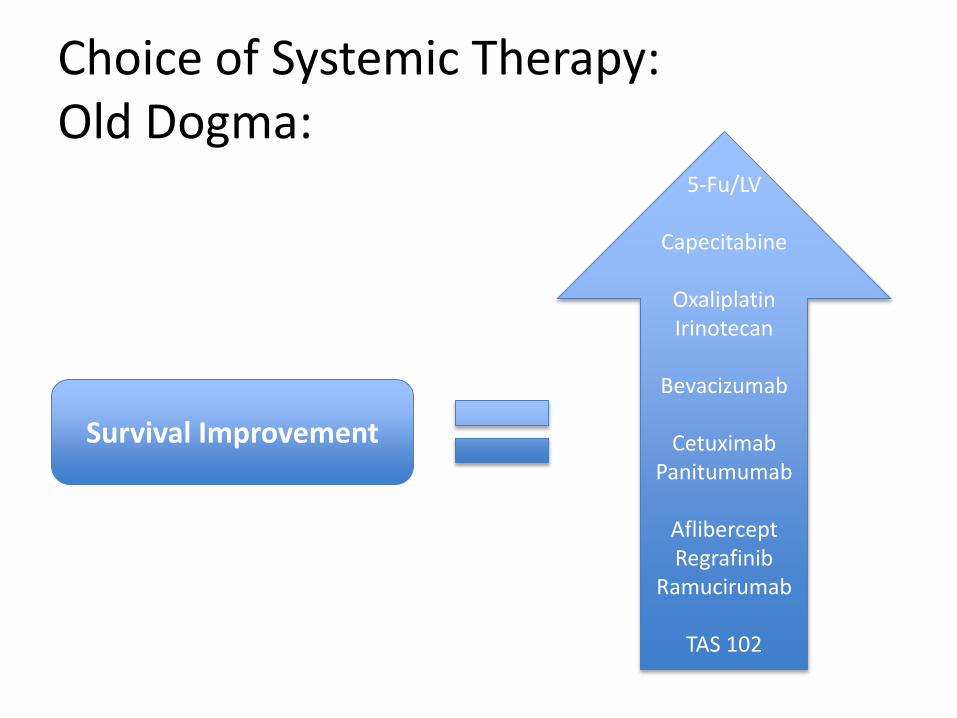
Choice of Systemic Therapy:Old Dogma:
5-Fu/LV
Capecitabine
OxaliplatinIrinotecan
Bevacizumab
CetuximabPanitumumab
AfliberceptRegrafinib
Ramucirumab
TAS 102
Survival Improvement
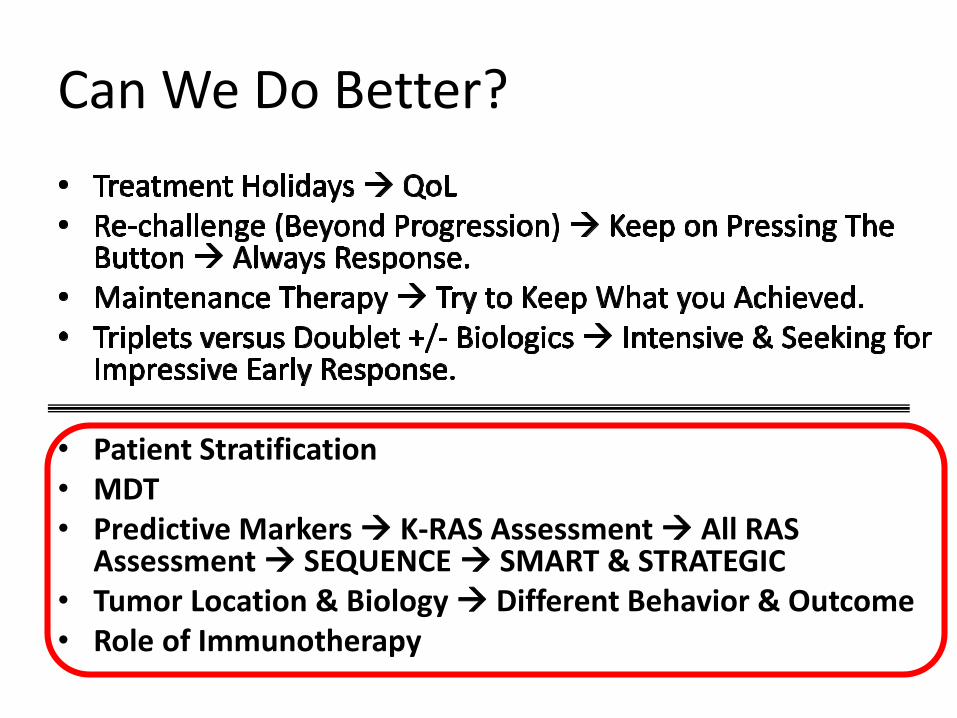
Can We Do Better?
• Patient Stratification• MDT• Predictive Markers K-RAS Assessment All RAS
Assessment SEQUENCE SMART & STRATEGIC• Tumor Location & Biology Different Behavior & Outcome • Role of Immunotherapy
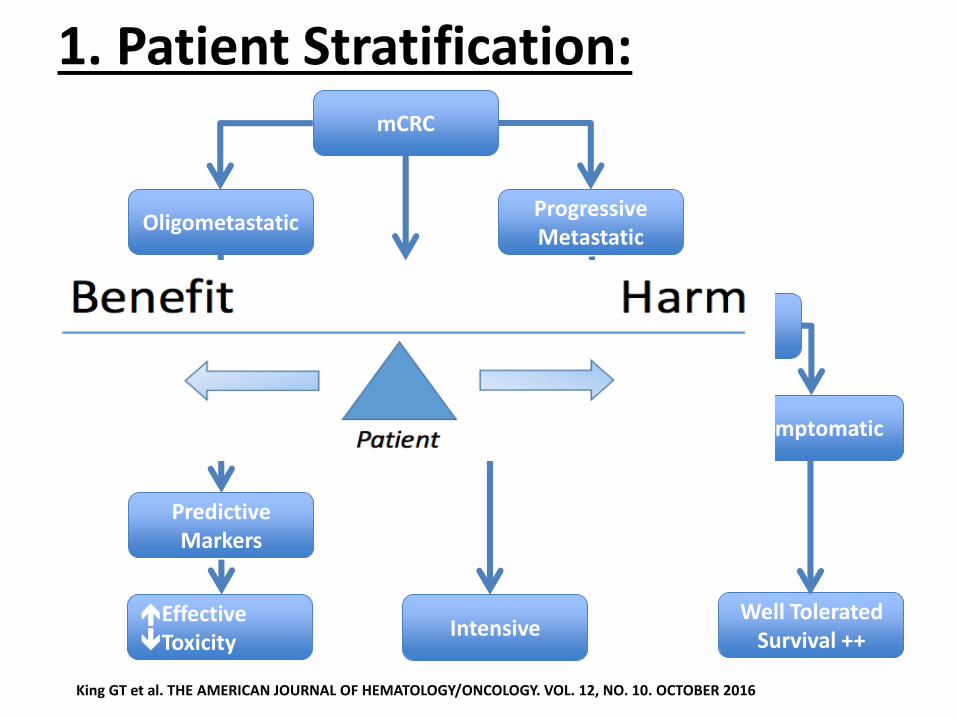
1. Patient Stratification:mCRC
Oligometastatic
Symptomatic Asymptomatic
Progressive Metastatic
Cure 1. Symptom Relief2. Extension of QoL
1. R.R.2. Shrinkage
Predictive Markers
IntensiveEffectiveToxicity
Well ToleratedSurvival ++
King GT et al. THE AMERICAN JOURNAL OF HEMATOLOGY/ONCOLOGY. VOL. 12, NO. 10. OCTOBER 2016
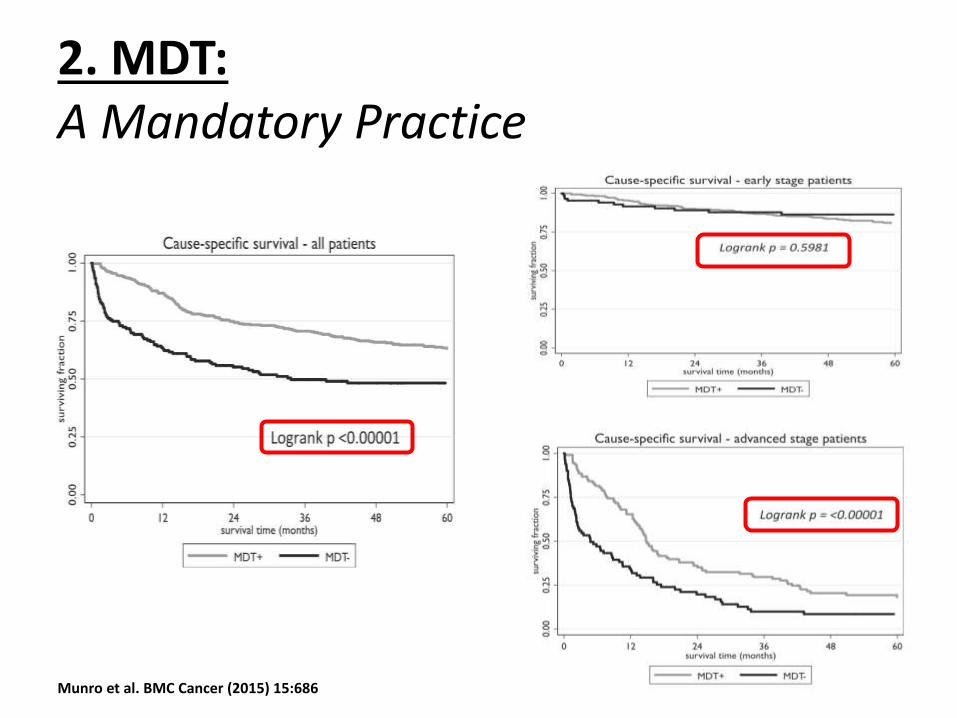
2. MDT: A Mandatory Practice
Munro et al. BMC Cancer (2015) 15:686
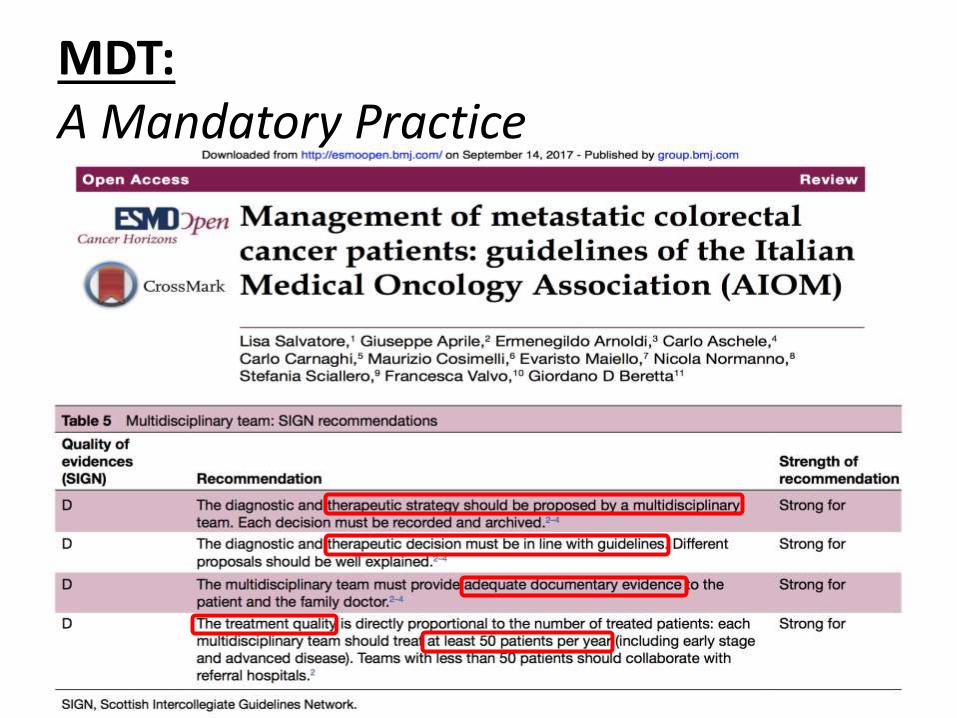
MDT: A Mandatory Practice
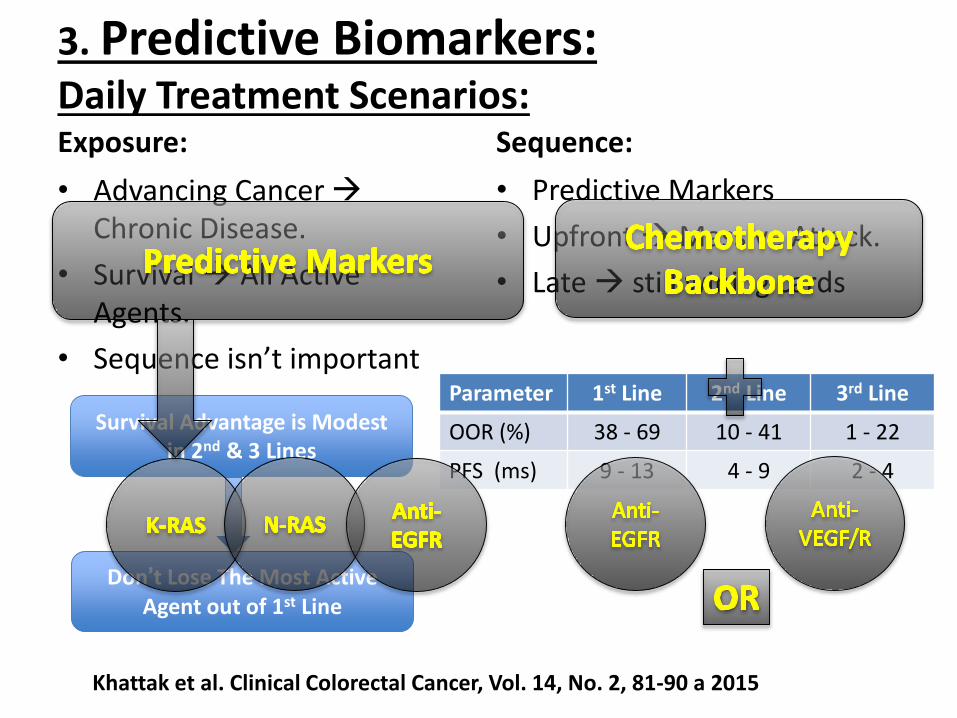
3. Predictive Biomarkers:Daily Treatment Scenarios: Exposure:
• Advancing Cancer Chronic Disease.
• Survival All Active Agents.
• Sequence isn’t important
Sequence:
• Predictive Markers
• Upfront Massive Attack.
• Late still wining cards
Khattak et al. Clinical Colorectal Cancer, Vol. 14, No. 2, 81-90 a 2015
Survival Advantage is Modest in 2nd & 3 Lines
Don’t Lose The Most Active Agent out of 1st Line
Parameter 1st Line 2nd Line 3rd Line
OOR (%) 38 - 69 10 - 41 1 - 22
PFS (ms) 9 - 13 4 - 9 2 - 4
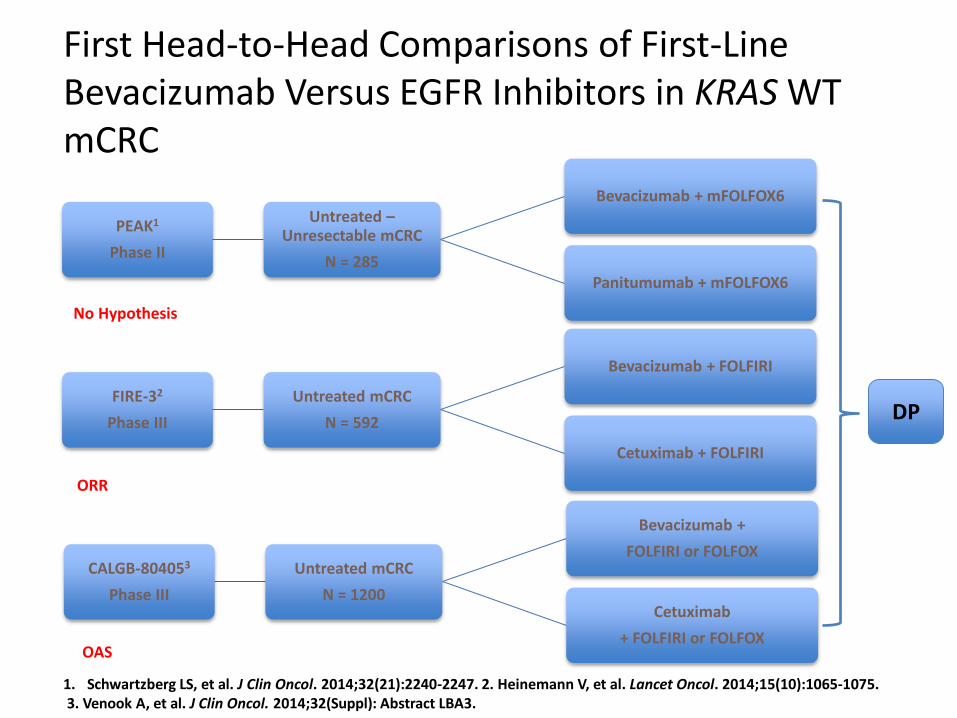
First Head-to-Head Comparisons of First-Line Bevacizumab Versus EGFR Inhibitors in KRAS WTmCRC
1. Schwartzberg LS, et al. J Clin Oncol. 2014;32(21):2240-2247. 2. Heinemann V, et al. Lancet Oncol. 2014;15(10):1065-1075.3. Venook A, et al. J Clin Oncol. 2014;32(Suppl): Abstract LBA3.
PEAK1
Phase II
Untreated –Unresectable mCRC
N = 285
Bevacizumab + mFOLFOX6
Panitumumab + mFOLFOX6
FIRE-32
Phase III
Untreated mCRC
N = 592
Bevacizumab + FOLFIRI
Cetuximab + FOLFIRI
CALGB-804053
Phase III
Untreated mCRC
N = 1200
Bevacizumab +
FOLFIRI or FOLFOX
Cetuximab
+ FOLFIRI or FOLFOX
No Hypothesis
OAS
ORR
DP
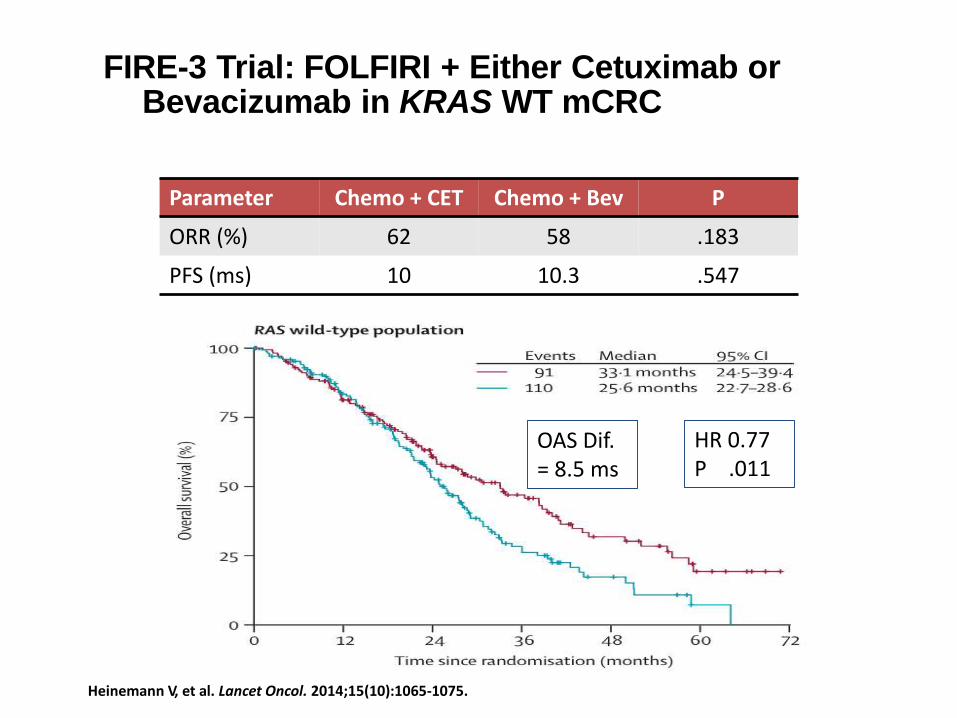
FIRE-3 Trial: FOLFIRI + Either Cetuximab orBevacizumab in KRAS WT mCRC
Heinemann V, et al. Lancet Oncol. 2014;15(10):1065-1075.
HR 0.77P .011
Parameter Chemo + CET Chemo + Bev P
ORR (%) 62 58 .183
PFS (ms) 10 10.3 .547
OAS Dif. = 8.5 ms
Anti-EGFR or Anti-VEGF/R in RAS-Wild mCRC: Evidence from Literature:
Modest et al. J Clin Oncol 33. © 2015 by American Society of Clinical Oncology
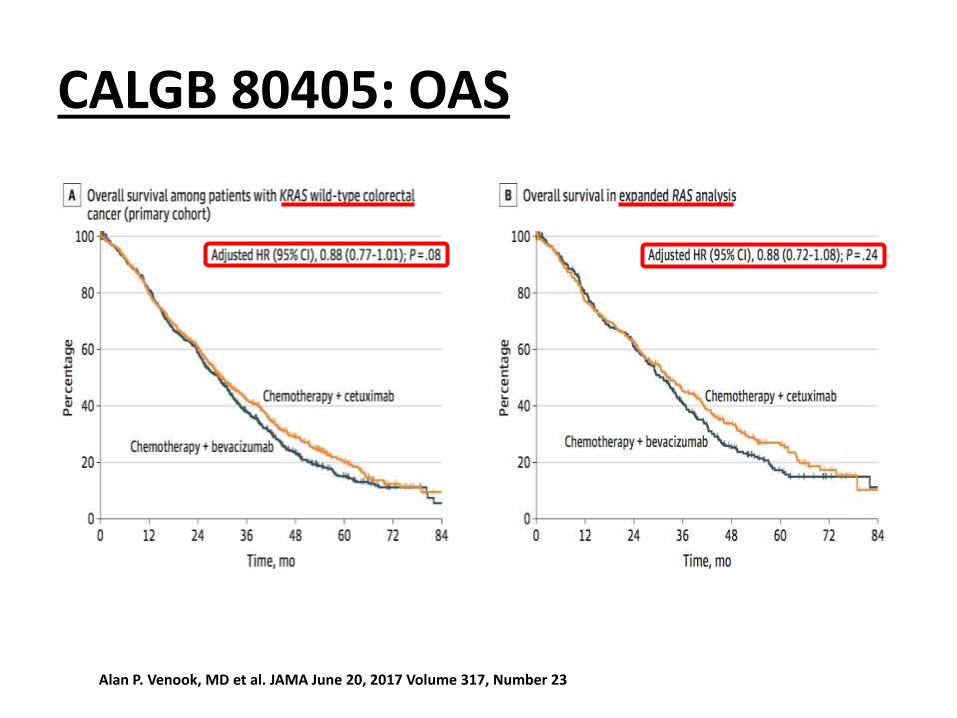
CALGB 80405: OAS
Alan P. Venook, MD et al. JAMA June 20, 2017 Volume 317, Number 23
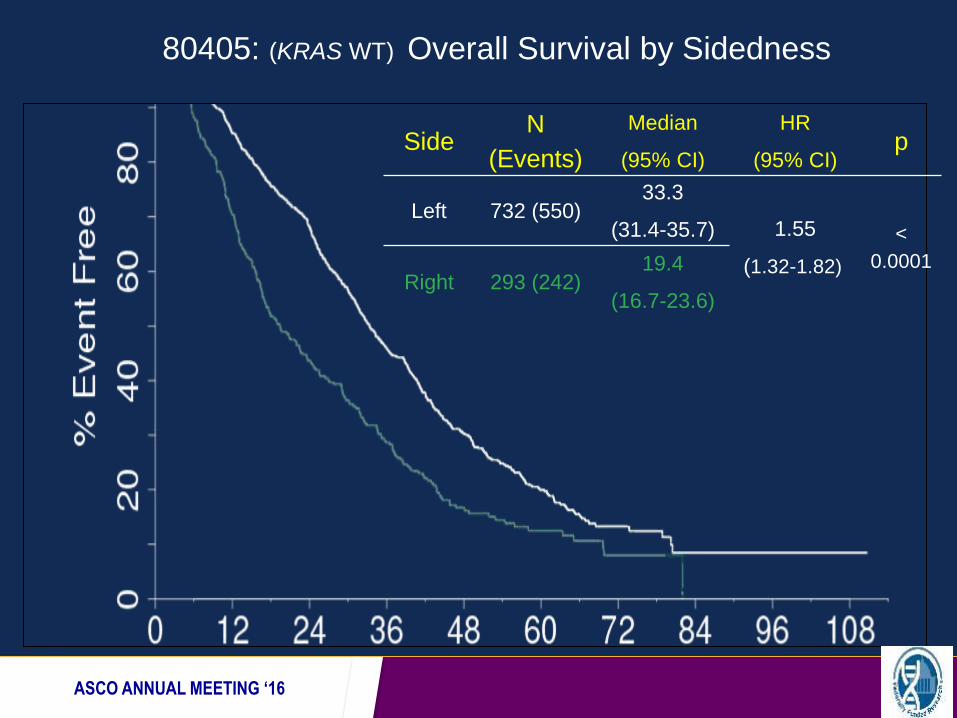
80405: (KRAS WT) Overall Survival by Sidedness
Presented by:ASCO ANNUAL MEETING ‘16
SideN
(Events)
Median
(95% CI)
HR
(95% CI)p
Left 732 (550)33.3
(31.4-35.7) 1.55
(1.32-1.82)
<
0.0001Right 293 (242)
19.4
(16.7-23.6)
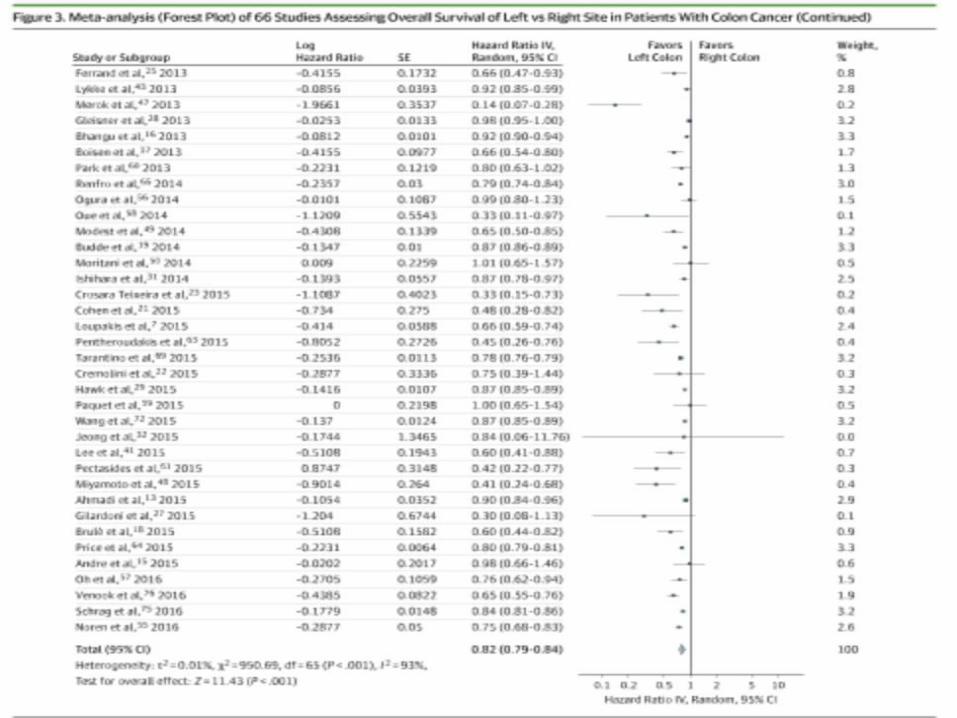
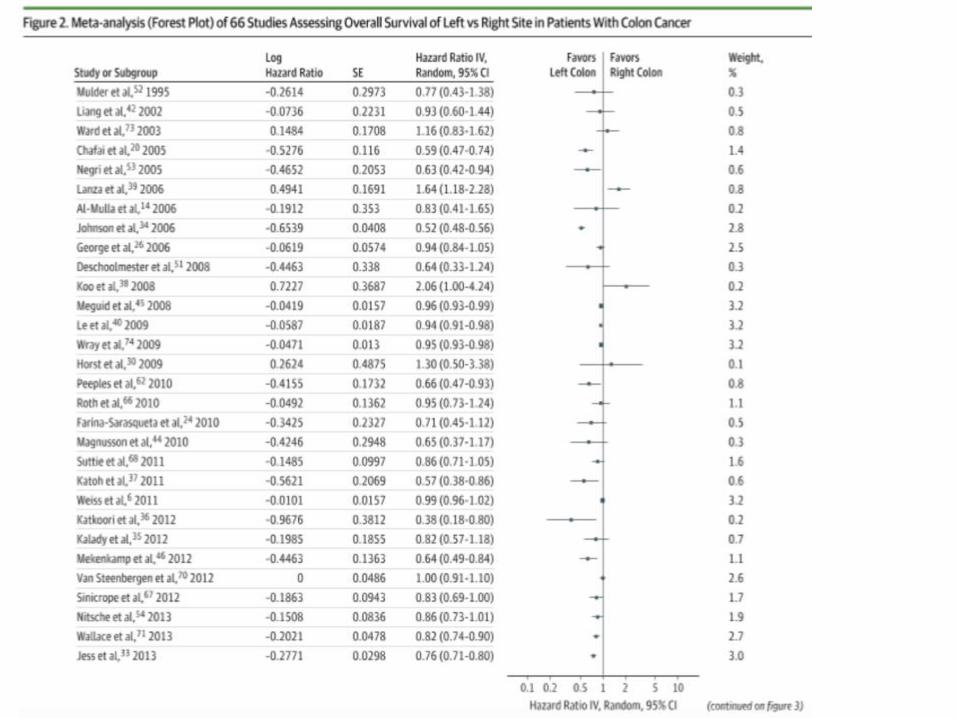
Petrelli et al. Jama Oncology. 2017 Vol 3 Number 2
66 RCT = 1437846 Colon Cancer Patients
Location as an Independent Prognostic Factor:
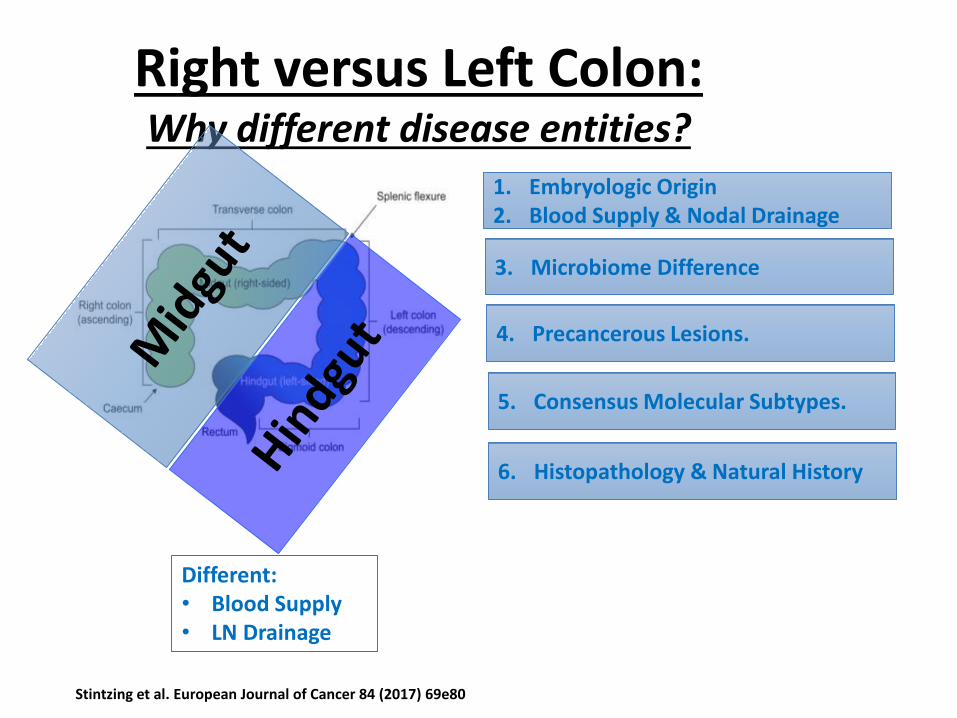
Right versus Left Colon:Why different disease entities?
Different:• Blood Supply• LN Drainage
1. Embryologic Origin2. Blood Supply & Nodal Drainage
3. Microbiome Difference
4. Precancerous Lesions.
6. Histopathology & Natural History
5. Consensus Molecular Subtypes.
Stintzing et al. European Journal of Cancer 84 (2017) 69e80
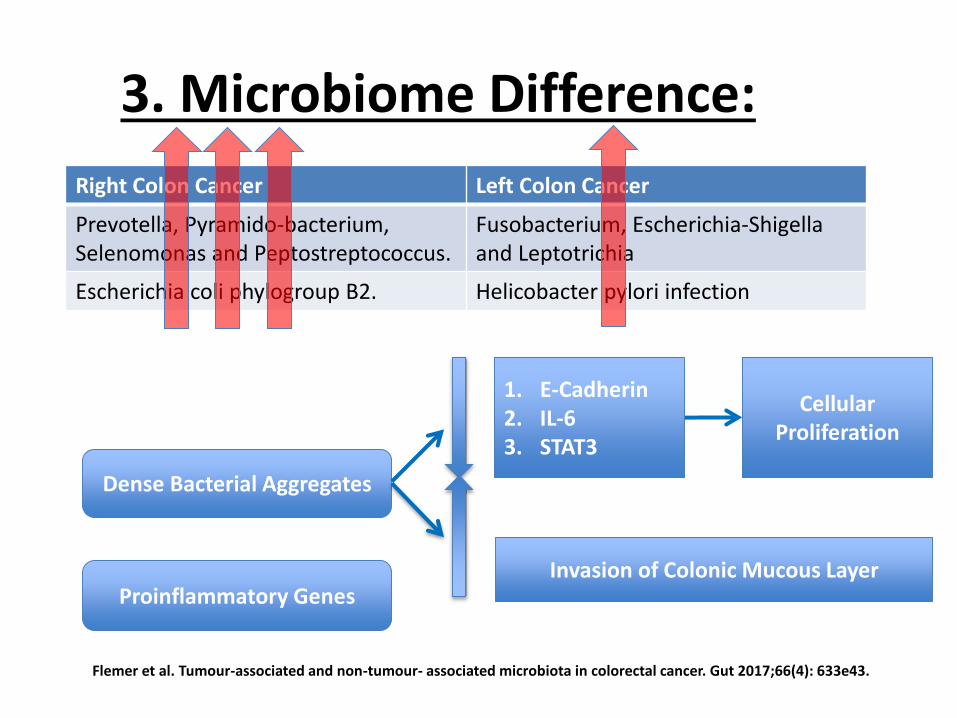
3. Microbiome Difference:
Right Colon Cancer Left Colon Cancer
Prevotella, Pyramido-bacterium, Selenomonas and Peptostreptococcus.
Fusobacterium, Escherichia-Shigellaand Leptotrichia
Escherichia coli phylogroup B2. Helicobacter pylori infection
Dense Bacterial Aggregates
1. E-Cadherin2. IL-63. STAT3
Cellular Proliferation
Invasion of Colonic Mucous LayerProinflammatory Genes
Flemer et al. Tumour-associated and non-tumour- associated microbiota in colorectal cancer. Gut 2017;66(4): 633e43.
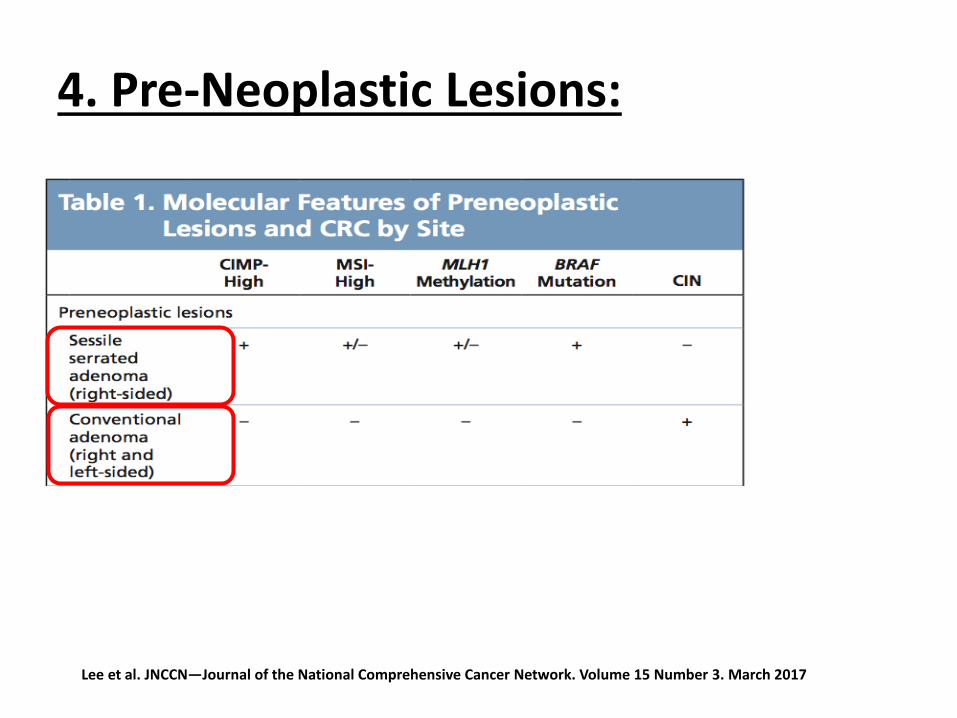
4. Pre-Neoplastic Lesions:
Lee et al. JNCCN—Journal of the National Comprehensive Cancer Network. Volume 15 Number 3. March 2017
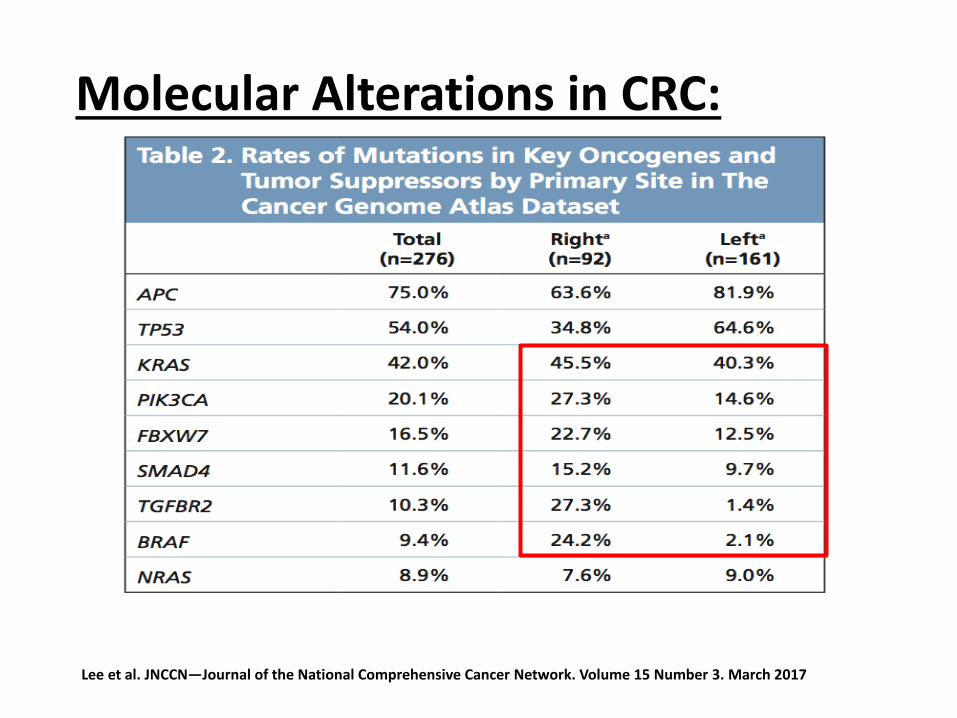
Lee et al. JNCCN—Journal of the National Comprehensive Cancer Network. Volume 15 Number 3. March 2017
Molecular Alterations in CRC:
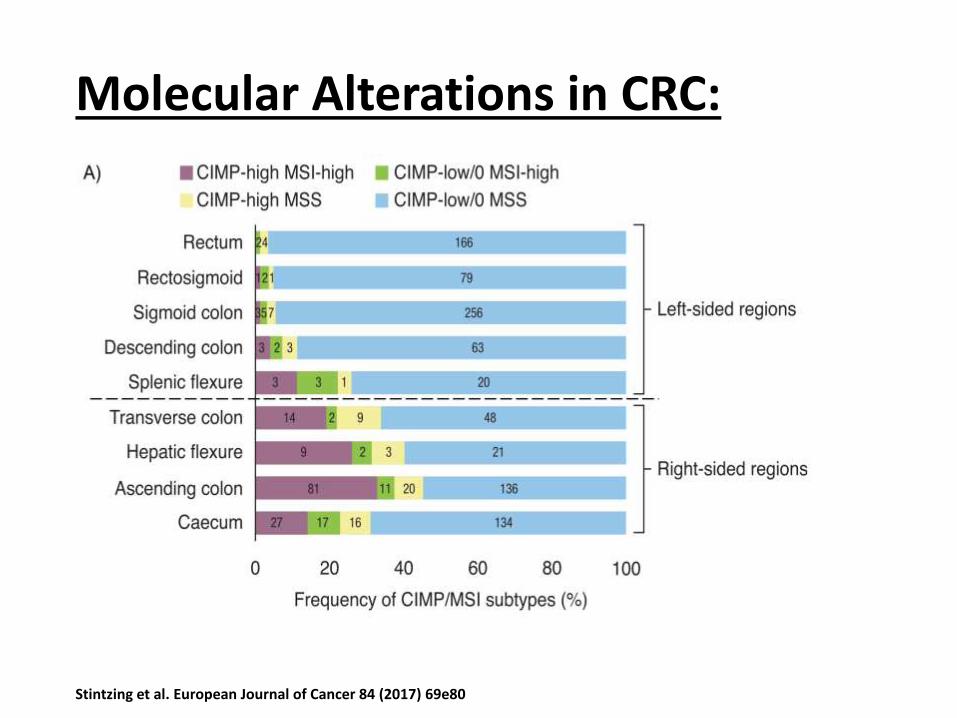
Molecular Alterations in CRC:
Stintzing et al. European Journal of Cancer 84 (2017) 69e80
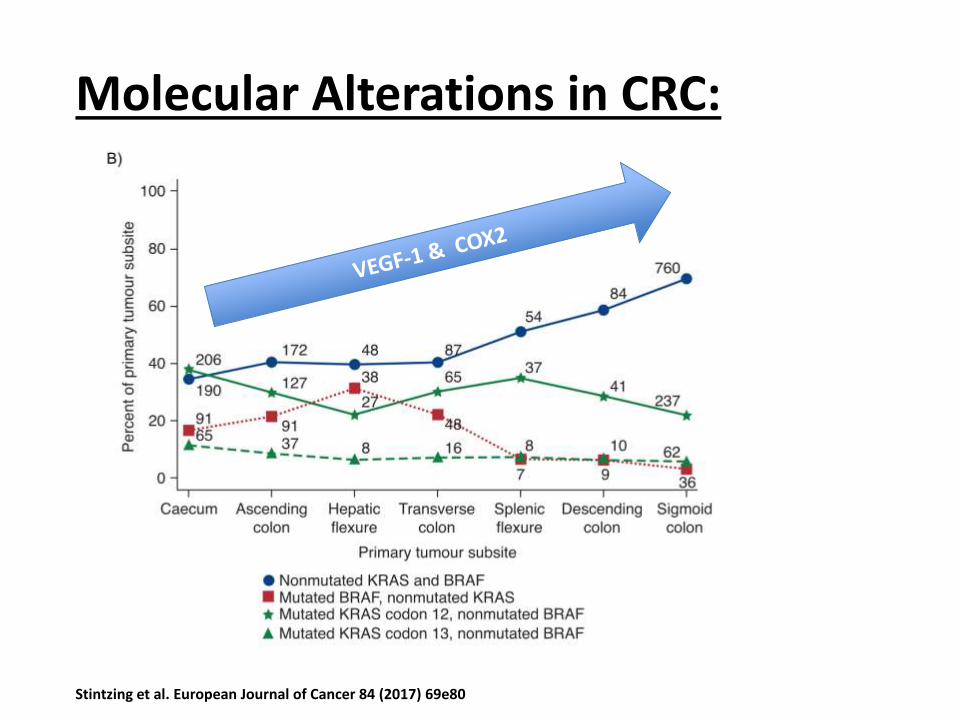
Molecular Alterations in CRC:
Stintzing et al. European Journal of Cancer 84 (2017) 69e80
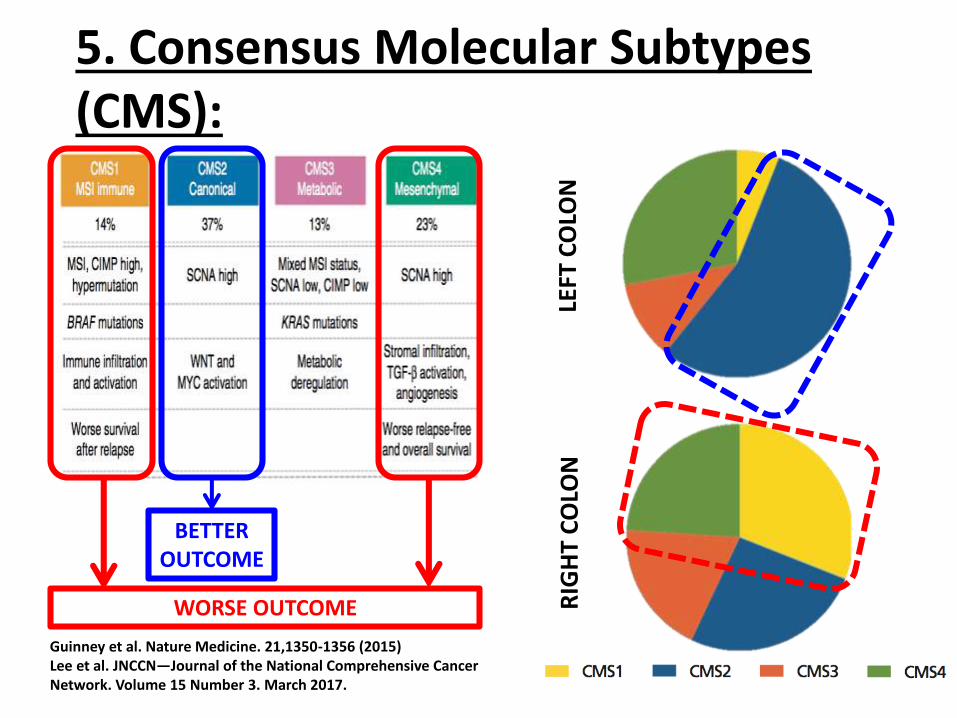
5. Consensus Molecular Subtypes (CMS):
RIG
HT
CO
LON
LEFT
CO
LON
BETTER OUTCOME
WORSE OUTCOME
Guinney et al. Nature Medicine. 21,1350-1356 (2015)Lee et al. JNCCN—Journal of the National Comprehensive Cancer Network. Volume 15 Number 3. March 2017.
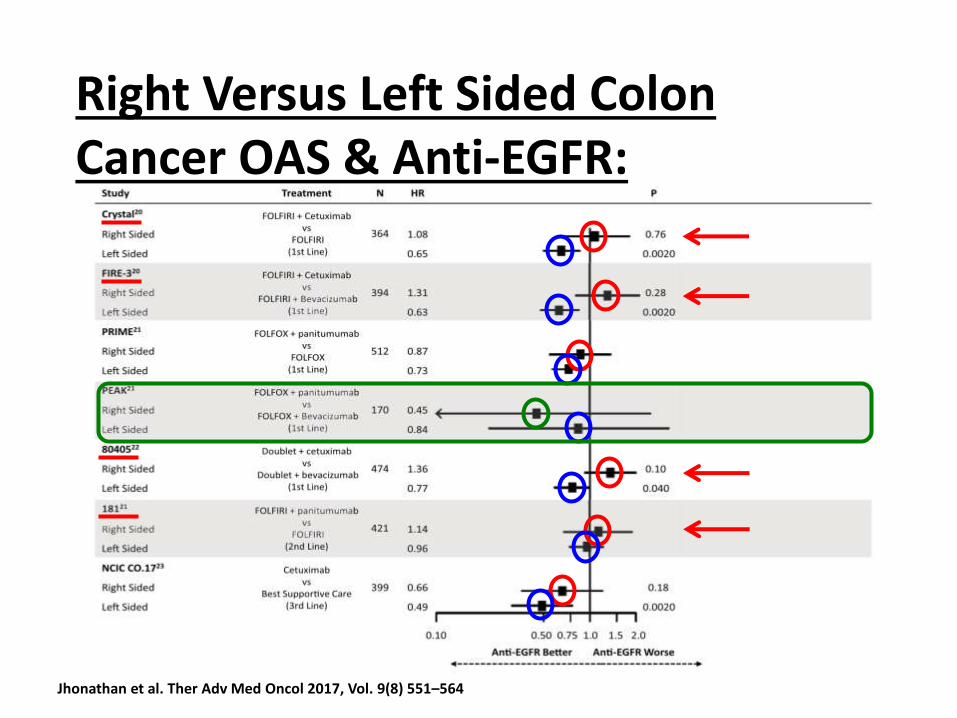
Right Versus Left Sided Colon Cancer OAS & Anti-EGFR:
Jhonathan et al. Ther Adv Med Oncol 2017, Vol. 9(8) 551–564
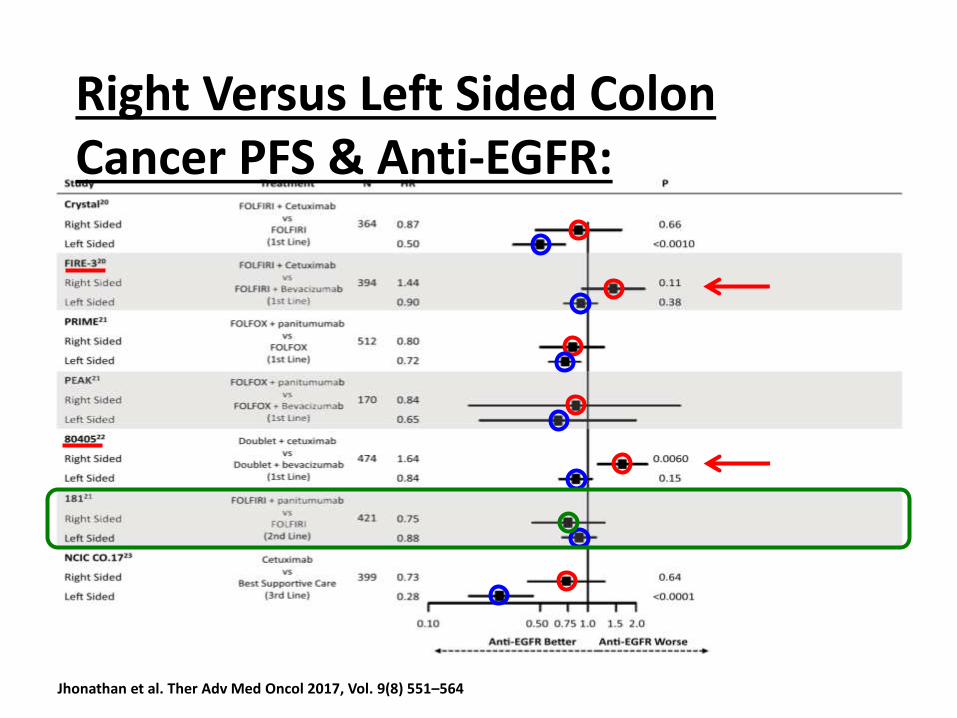
Jhonathan et al. Ther Adv Med Oncol 2017, Vol. 9(8) 551–564
Right Versus Left Sided Colon Cancer PFS & Anti-EGFR:
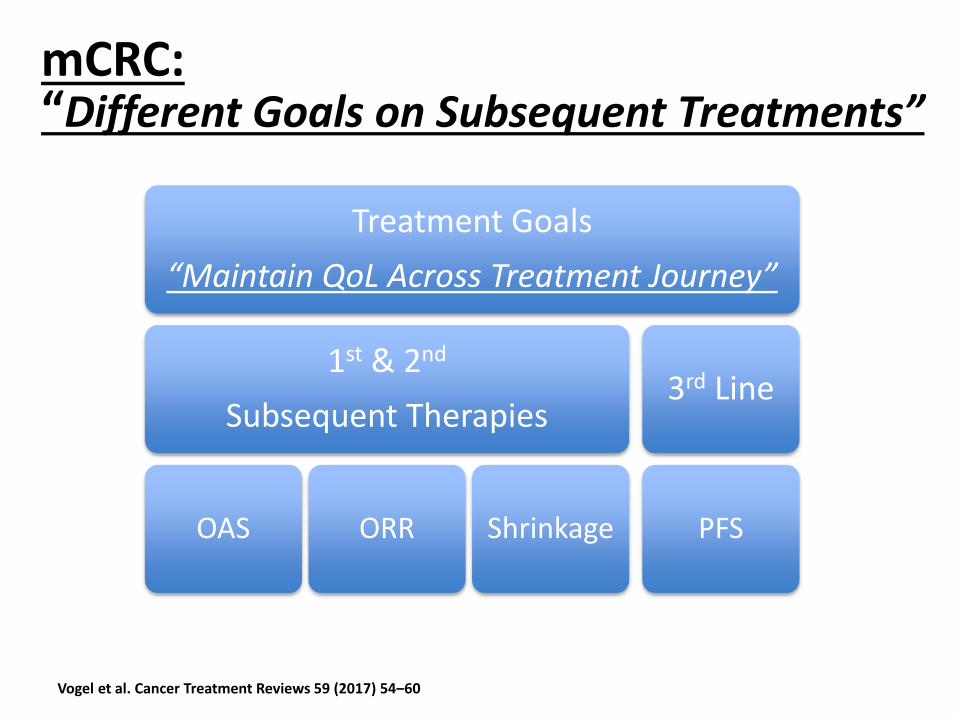
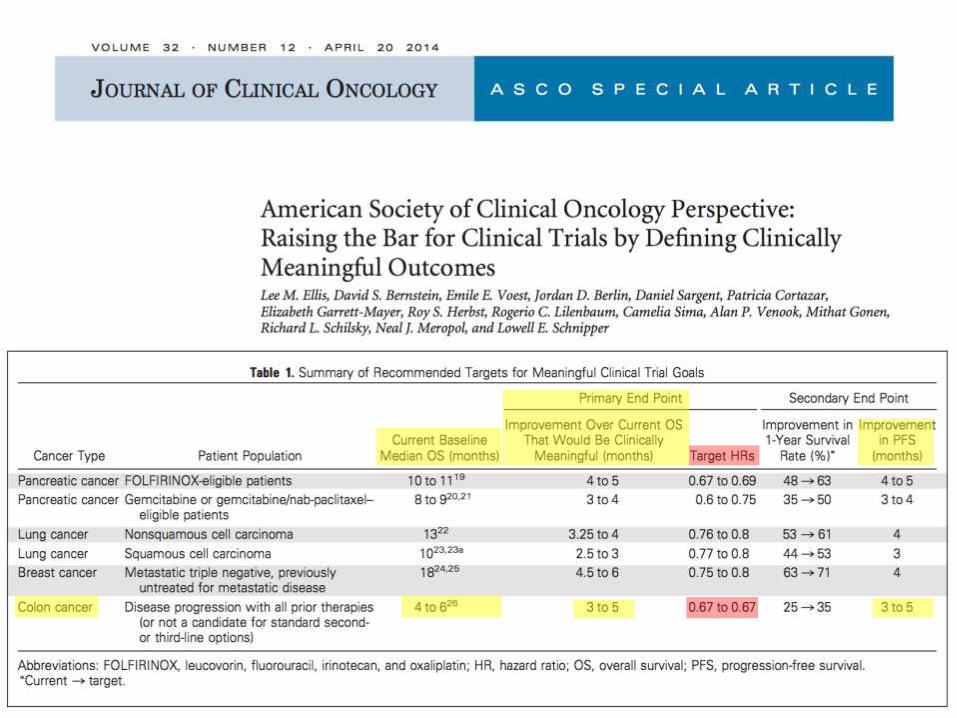
mCRC: “Different Goals on Subsequent Treatments”
Vogel et al. Cancer Treatment Reviews 59 (2017) 54–60
Treatment Goals
“Maintain QoL Across Treatment Journey”
1st & 2nd
Subsequent Therapies
OAS ORR Shrinkage
3rd Line
PFS
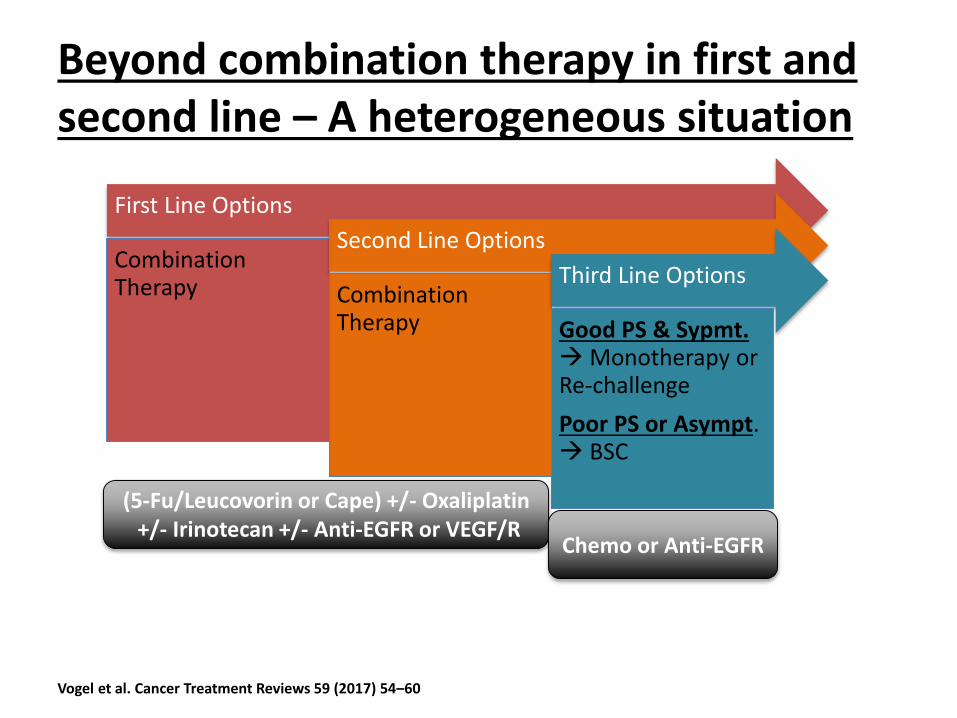
First Line Options
Combination Therapy
Second Line Options
Combination Therapy
Third Line Options
Good PS & Sypmt. Monotherapy or Re-challenge
Poor PS or Asympt. BSC
Beyond combination therapy in first and second line – A heterogeneous situation
(5-Fu/Leucovorin or Cape) +/- Oxaliplatin+/- Irinotecan +/- Anti-EGFR or VEGF/R
Chemo or Anti-EGFR
Vogel et al. Cancer Treatment Reviews 59 (2017) 54–60
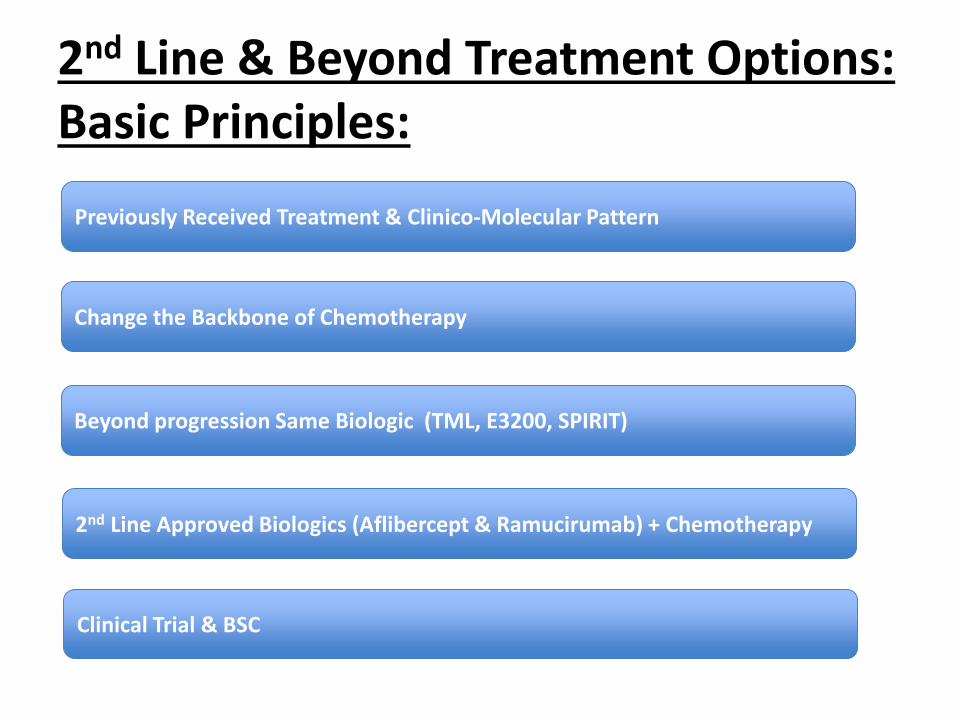
2nd Line & Beyond Treatment Options:Basic Principles:
Previously Received Treatment & Clinico-Molecular Pattern
Change the Backbone of Chemotherapy
Beyond progression Same Biologic (TML, E3200, SPIRIT)
2nd Line Approved Biologics (Aflibercept & Ramucirumab) + Chemotherapy
Clinical Trial & BSC
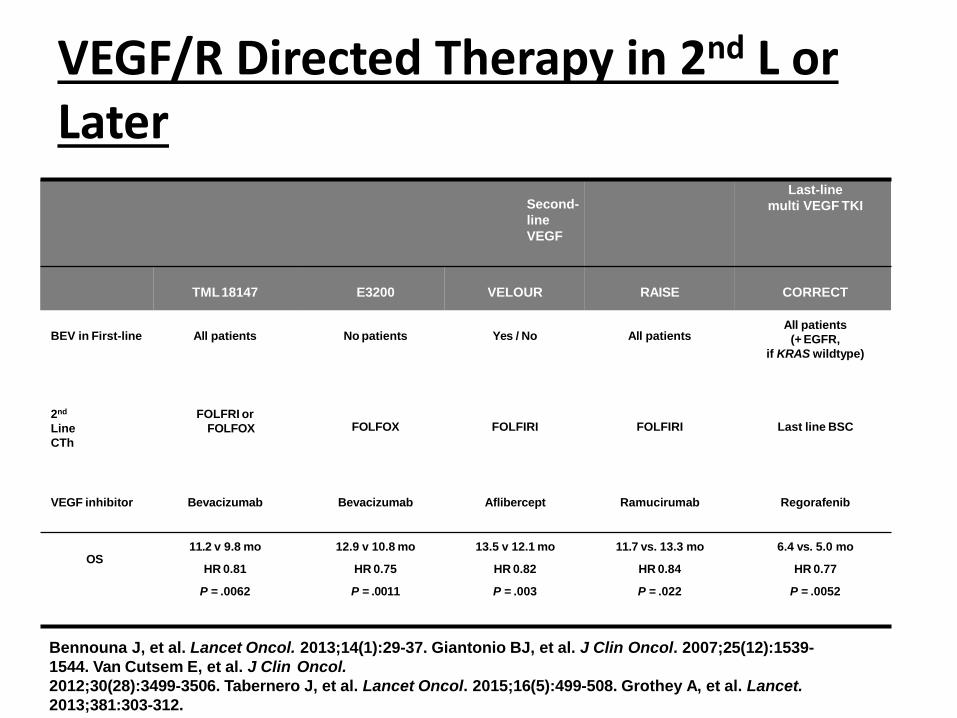
VEGF/R Directed Therapy in 2nd L or Later
Second-
line
VEGF
Last-line
multi VEGF TKI
TML18147 E3200 VELOUR RAISE CORRECT
BEV in First-line All patients No patients Yes / No All patientsAll patients
(+ EGFR,
if KRAS wildtype)
2nd
Line
CTh
FOLFRI or
FOLFOX FOLFOX FOLFIRI FOLFIRI Last line BSC
VEGF inhibitor Bevacizumab Bevacizumab Aflibercept Ramucirumab Regorafenib
OS11.2 v 9.8 mo
HR 0.81
P = .0062
12.9 v 10.8 mo
HR 0.75
P = .0011
13.5 v 12.1 mo
HR 0.82
P = .003
11.7 vs. 13.3 mo
HR 0.84
P = .022
6.4 vs. 5.0 mo
HR 0.77
P = .0052
Bennouna J, et al. Lancet Oncol. 2013;14(1):29-37. Giantonio BJ, et al. J Clin Oncol. 2007;25(12):1539-
1544. Van Cutsem E, et al. J Clin Oncol.
2012;30(28):3499-3506. Tabernero J, et al. Lancet Oncol. 2015;16(5):499-508. Grothey A, et al. Lancet.
2013;381:303-312.
1st Line 2nd Line 3rd Line
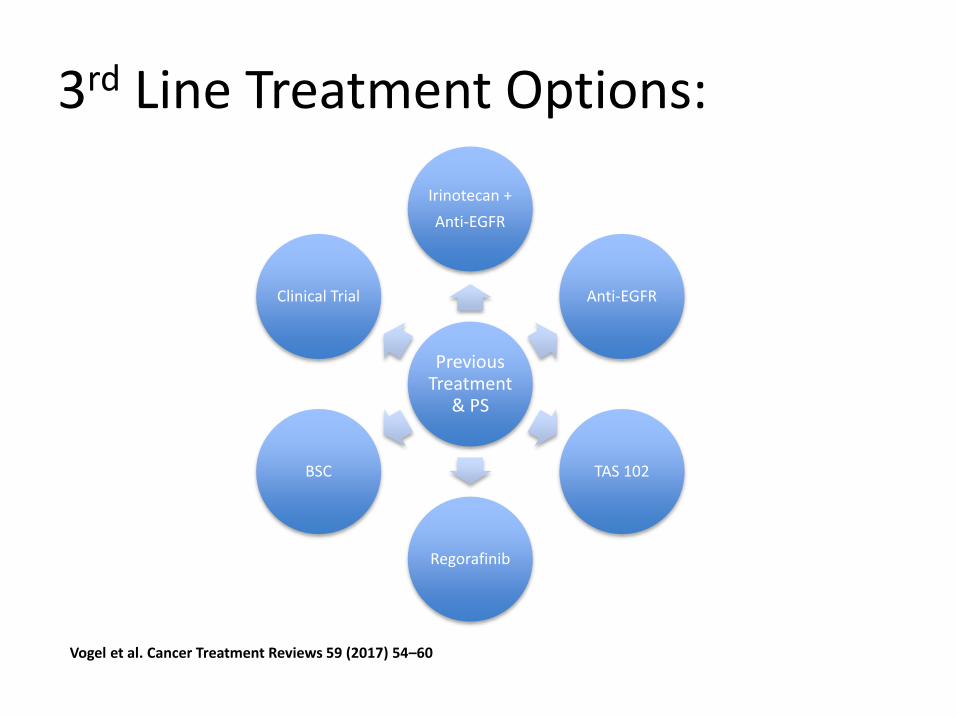
3rd Line Treatment Options:
Previous Treatment
& PS
Irinotecan +
Anti-EGFR
Anti-EGFR
TAS 102
Regorafinib
BSC
Clinical Trial
Vogel et al. Cancer Treatment Reviews 59 (2017) 54–60
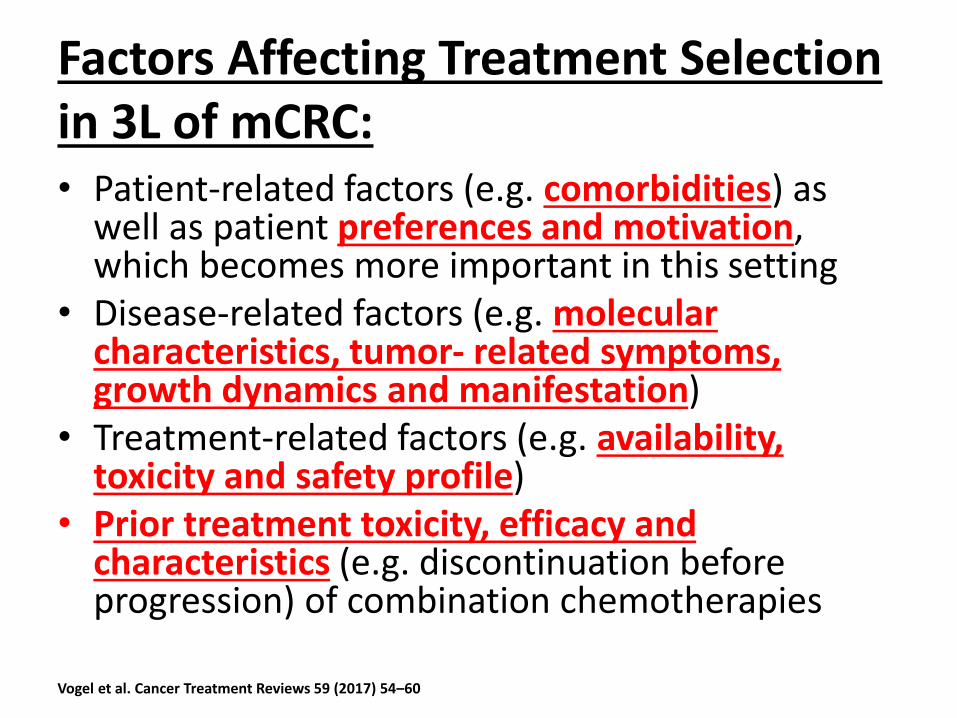
Factors Affecting Treatment Selection in 3L of mCRC:• Patient-related factors (e.g. comorbidities) as
well as patient preferences and motivation, which becomes more important in this setting
• Disease-related factors (e.g. molecular characteristics, tumor- related symptoms, growth dynamics and manifestation)
• Treatment-related factors (e.g. availability, toxicity and safety profile)
• Prior treatment toxicity, efficacy and characteristics (e.g. discontinuation before progression) of combination chemotherapies
Vogel et al. Cancer Treatment Reviews 59 (2017) 54–60
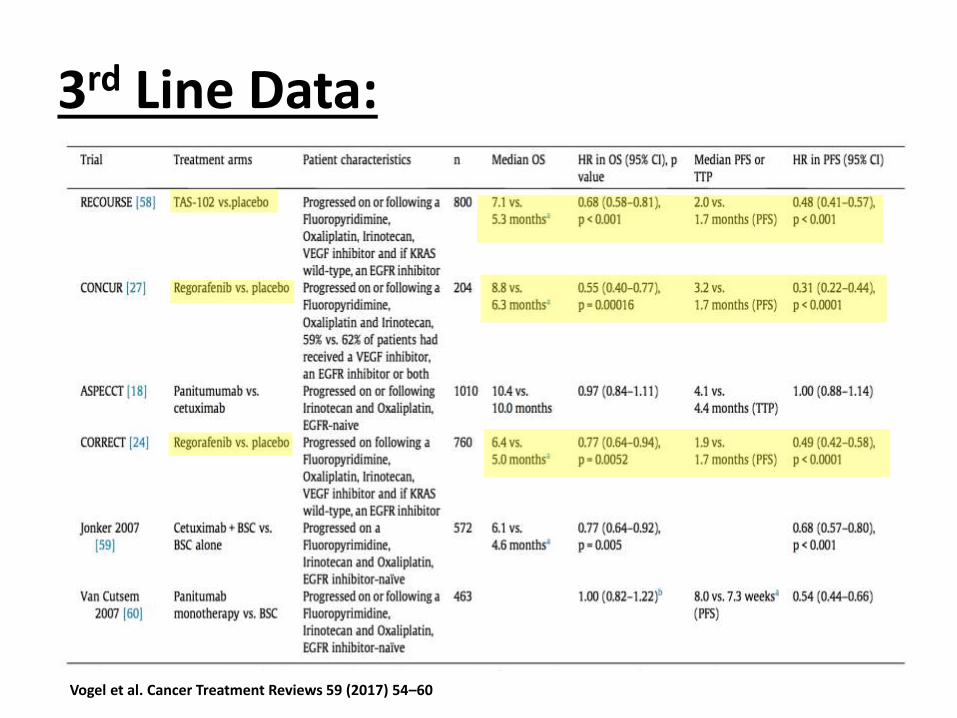
3rd Line Data:
Vogel et al. Cancer Treatment Reviews 59 (2017) 54–60
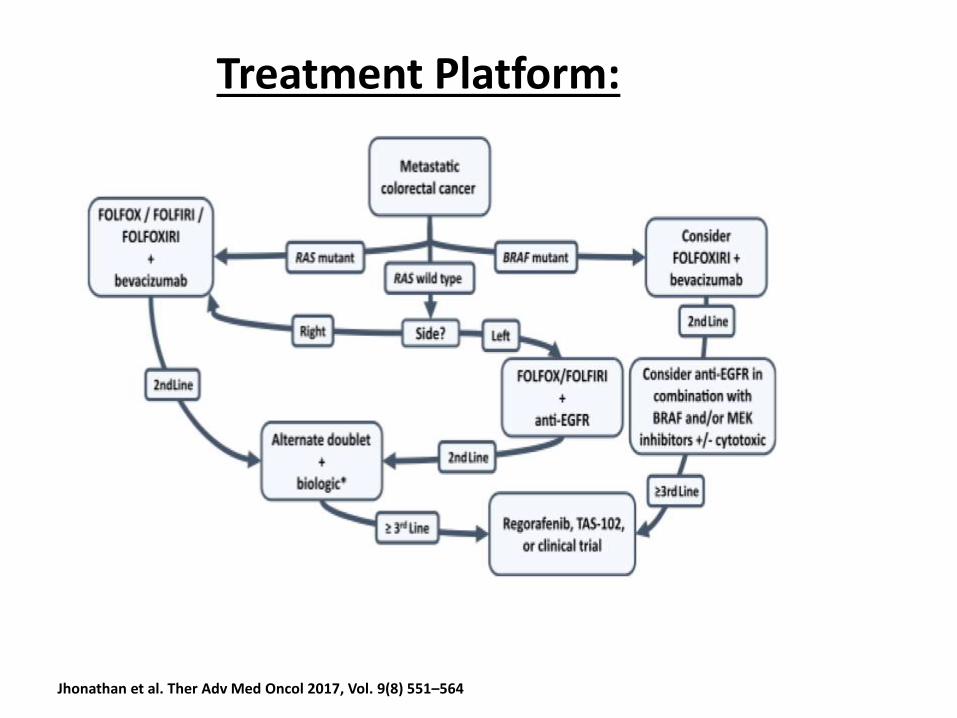
Treatment Platform:
Jhonathan et al. Ther Adv Med Oncol 2017, Vol. 9(8) 551–564
Basic Unites of Tumorigenesis:
• Microsatellites: Repetitive genetic units Maintained by MMR system (5 Genes).
• Deficient MMR MSI Genomic Instability Tumor formation.
• MSI:
– H: instability in > 30% of microsatellite loci.
– L: instability in < 30% of microsatellite loci.
E. Vilar, J. Tabernero, Molecular dissection of microsatellite instable colorectal cancer, Cancer Discov. 3 (5) (2013) 502e511.
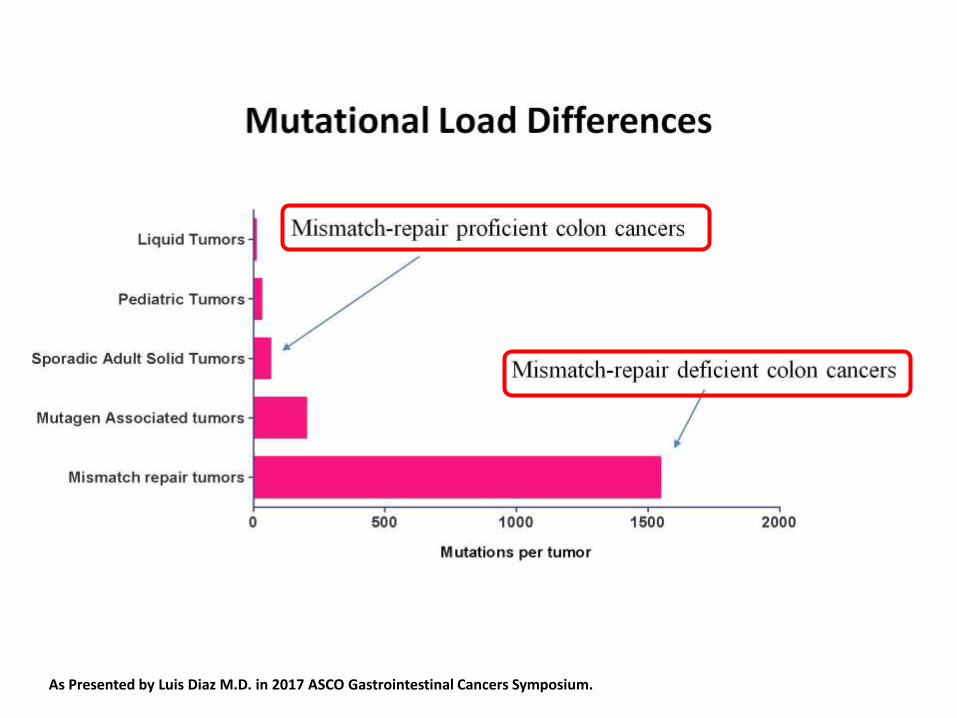
Slide 4
Presented By Luis Diaz at 2017 Gastrointestinal Cancers SymposiumAs Presented by Luis Diaz M.D. in 2017 ASCO Gastrointestinal Cancers Symposium.
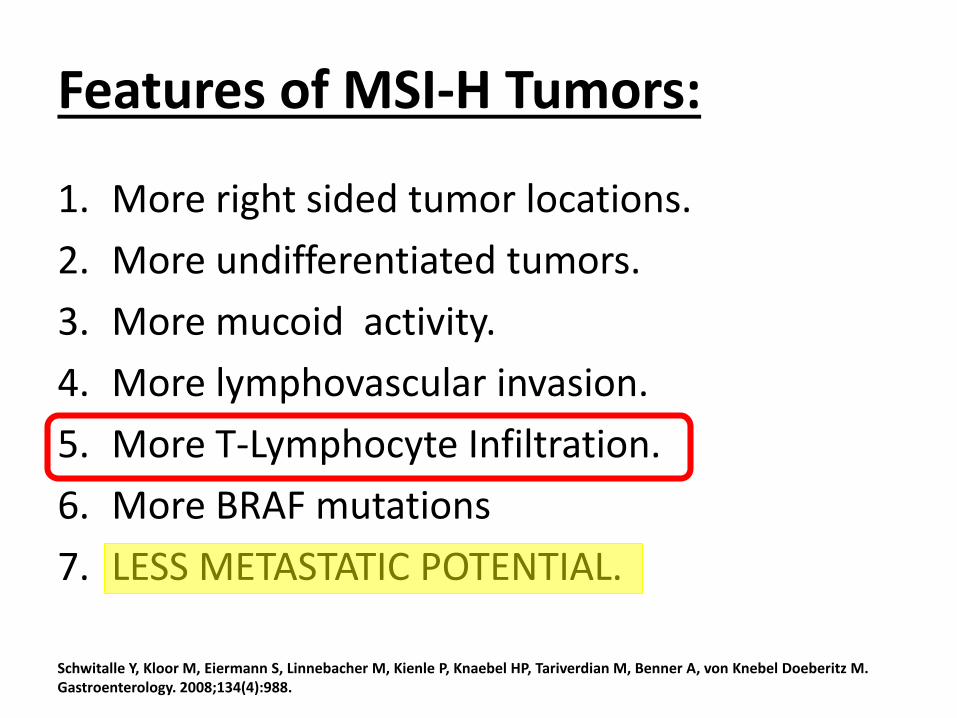
Features of MSI-H Tumors:
1. More right sided tumor locations.
2. More undifferentiated tumors.
3. More mucoid activity.
4. More lymphovascular invasion.
5. More T-Lymphocyte Infiltration.
6. More BRAF mutations
7. LESS METASTATIC POTENTIAL.
Schwitalle Y, Kloor M, Eiermann S, Linnebacher M, Kienle P, Knaebel HP, Tariverdian M, Benner A, von Knebel Doeberitz M. Gastroenterology. 2008;134(4):988.
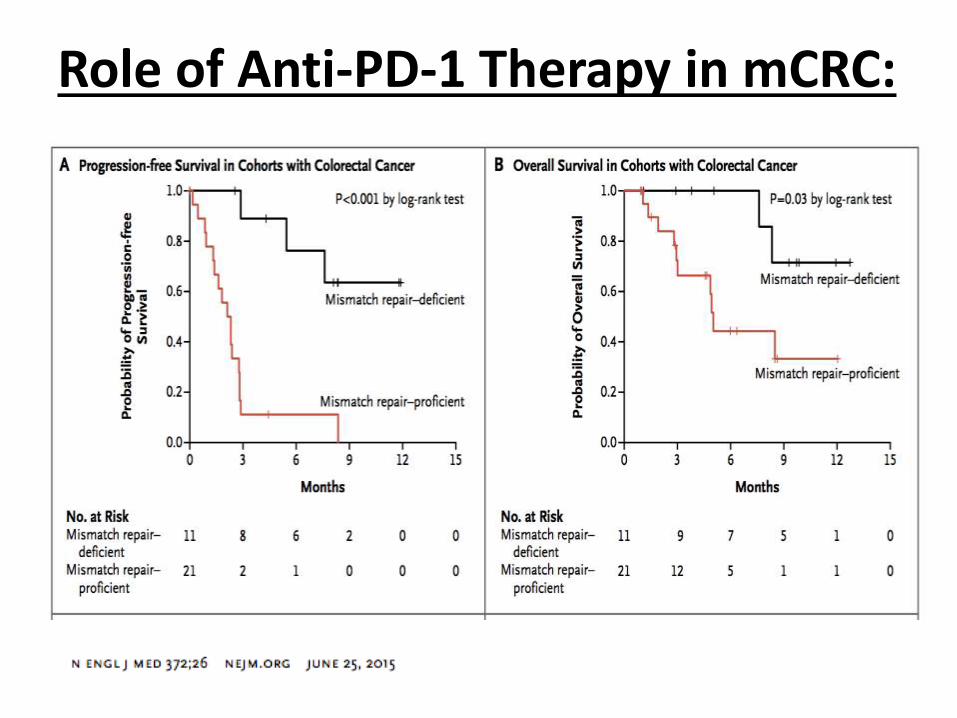
Role of Anti-PD-1 Therapy in mCRC:
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
Presented By Luis Diaz at 2017 Gastrointestinal Cancers Symposium
Slide 18
Presented By Luis Diaz at 2017 Gastrointestinal Cancers Symposium
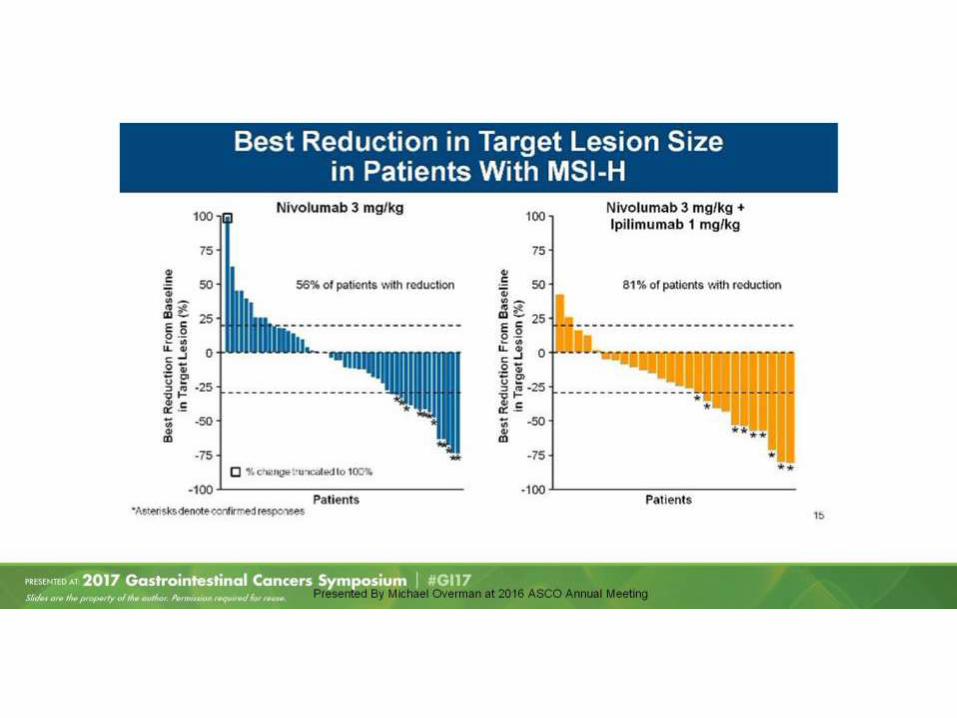
Best Reduction in Target Lesion Size <br />in Patients With MSI-H
Presented By Luis Diaz at 2017 Gastrointestinal Cancers Symposium
The Art of Today:
• The landscape of treating mCRC is expanding.
• Proper stratification & MDT implementation are pre-requisites of effective therapeutic approach.
• Molecular subtyping and location are the most crucial factors in deciding treatment algorithm.
• More options are readily available for treatment beyond first line.
• Immunotherapy knowledge curve is steeply rising 1st line treatment option.



![Surgery for metastatic tumors of the pancreas...However, metastatic pancreatic tumor can be de-veloped from renal cell cancer, lung, breast, colon, or skin tumors [1–7]. Metastasis](https://img.pdfslide.net/doc/110x75/610075a214c702770f00fe5a/surgery-for-metastatic-tumors-of-the-pancreas-however-metastatic-pancreatic.jpg)