Embed Size (px)
DESCRIPTION
for the presentation of first years of srilankan university students
Citation preview

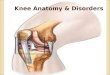
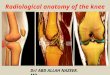
Knee joint

Content
Type of jointArticular surfacesLigamentsSynovial membraneMobility of the joint

- The Knee Joint is the largest & most complicated joint in the body .
- It consists of 3 Joints within a single synovial cavity :
1) Medial Condylar Joint : Between the medial condyle “of the femur” & the medial condyle “of the tibia” .
2) Lateral Condylar Joint : Between the lateral condyle “of the femur” & the lateral condyle “of the tibia” .
3) Patellofemoral Joint : Between the patella & the patellar surface of the femur .
- The fibula is NOT directly involved in the joint .

Types : - 1 & 2 : Hinge joint. - 3 : Planar gliding .

1) Fibrous capsule2) Ligamentum patellae3) Tibial collateral or medial ligament4) Fibular collateral or lateral ligament5) Oblique popliteal ligament6) Arcuate popliteal ligament7) Anterior cruciate ligament8) Posterior cruciate ligament9) Medial meniscus10) Lateral meniscus11) Transverse ligament


CapsuleFemoral attachment Anteriorly it is deficientPosteriorly it is attached to intercondylar ridge Laterally encloses the origin of poplitieus
Tibial attachment Anteriorly it descend to the tibial tuberosity along margins of the condylesPosteriorly it is attached to intercondylar ridge Posterolaterally passage of popliteus tendon

The weak capsular ligament is strengthened by
Anteriorly by medial and lateral retinacula (extensions of v. medialis & v. lateralis )Laterally by iliotibial tractPosteriorly by oblique polpliteal ligament Medially by tendons of sartorius and semimembranosus

Ligamentum patellaeAttachmentAbove – margins and rough posterior margins of patellar retinacular Below- smooth upper part of tibial tuberosity
Related to deep and superficial infrapatella bursa , infrapatella pad of fat

Tibial collateral or medial ligamentThis is a long band of great strength
AttachmentsSuperioly –medial epicondyle of femur Inferioly -anterior part & posterior part Anterior part- below to medial border of medial surface of shaft of tibia (covers inferior medial genicular vessels and nerve ,anterior part of semimembranosus tendon)
Posterior part – medial condyl of tibia above groove for semetendinosus (blends with medail meniscus and capsule)

Fibular collateral or lateral ligament Strong and code like ligament Attachments Superiorly –lateral epicondyle of femur
below to popliteal groove Inferiorly head of fibula in front of its apex (it is separated from lateral meniscus from
capsule and tendon of popliteus)

Oblique popliteal ligament
This is an expansion of semimembranosus tendon which runs upwards and laterally
Attached to intracondylar line and lateral condyle of femur
Have a close relation with popliteal artery

Arcuate popliteal ligamentPosterior expansion of short lateral ligament It expands backwards from head of the fibula , arches over tendon of poplitieus and attached to the posterior border of intracondylar region of tibia
Anterior & Posterior cruciate ligaments Both are very strong and thick fibrous bands they act directly to maintain anteroposterior stability of knee joint




Anterior Cruciate Ligament (ACL) :Attached to the anterior intercondylar area of the tibia , passes upward , backward & laterally to get attached to the lateral femoral condyle .Prevents posterior displacement of the femur ( With the knee joint flexed , the ACL prevents the tibia from being pulled
anteriorly)

~ Posterior Cruciate Ligament (PCL)
Attached to the posterior intercondylar area of the tibia , passes upward , forward , & medially to get attached to the medial femoral condyle.
Prevents anterior displacement of the femur ( With the knee joint flexed , the PCL prevents the tibia from being pulled posteriorly ).

- The medial and lateral menisci are 2 C-shaped sheets of fibrocartilage between the tibial & femoral condyles
- Their peripheral border is thick & attached to the capsule and vascular
their inner border is thin & forms a free edge and avascular
- Each meniscus is attached to the upper surface of the tibia by anterior & posteriorly
- They are connected to each other by the transverse ligament and to the margins of the head of the tibia by coronary ligaments.

Medial menisci Lateral menisci
Nearly semicircular Nearly circular
Posterior fibers of anterior end continues with the transverse ligament
Posterior end of meniscus is attached to the femur through two meniscofemoral ligaments
Peripheral part attach with deep part of tibial collateral ligament
Medial part of tendon of politius attach to lateral meniscus
Functions •Make articular surfaces more congruent•Act as shock absorbers •Lubricate joint cavity•Give rise to proprioceptive impulses due to their nerve supply

Synovial membrane lines the capsule except posteriorly where it is forwards by cruciate ligaments
In front it is absent from patella Below it covers the deep surface of
infrapatellar fatty pad Medially the infrapatellar synovial fold
extend backwards from fatty pad to intercondylar fossa of femur

There are 13 bursae around knee joint 4 anteriorly 4 laterally 5 medially

Flexion and extension are take place in upper compartment of the joint
Flexion : these muscles produce flexion : Biceps femoris , Semitendinosus ,
Semimembranosus , Gracilis, Sartorius , Popliteus .
Flexion is limited by the contact of the back of the leg with the thigh .
Extension : by the Quadriceps femoris , tensor fasciae latae
Extension is limited by the tension of all the ligaments of the joint .

Flexion
Extension

Raotatry movements at the knee take place in lower compartment around a vertical axis
- Medial Rotation : by the Semtendinosus , Semimembranosus, Popliteus Sartorius , Gracilis
- Lateral Rotation : by the Biceps femoris .


Popliteal artery Femoral artery Tibial artery

Osteoarthritis (OA) : a chronic inflammatory joint disorder in which there’s progressive softening & destruction of the articular cartilage , accompanied by new growth of cartilage and bone at the joint margins (osteophytes) and capsular fibrosis... leading to bone exposure & severe pain .
OA is the most common joint disease.
The knee is the most common site.


Risk factors: age . obesity. Family
Predisposing factors : Articular surface injury . Torn meniscus . Ligament instability . Preexisting deformity .


It is an angle formed by two intersecting lines
anterior superior illiac spine mid patella tibial tubercle mid patella
10° - 15° in male 10° - 19° in female Increase of the angle causes the Genu Valgum
( knock knee ) Decrease of the angle causes the Genu Varus


Injuries to menisci Injuries to crucial ligaments Injuries to collateral ligaments