Embed Size (px)
Citation preview

Dr. Mohit GoelDept. of Radiology21/06/2013

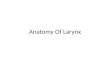
• The larynx is a 5-7 cm long structure. • Its upper boundary starts at
the tip of the epiglottis, opposite the 3rd to 4th, cervical vertebra.
• Its lower end is at the lower border of the cricoid cartilage.• This lies opposite the 6th
cervical vertebra.




• Largest laryngeal cartilage, "shields" larynx• 2 anterior laminae meet anteriorly at acute angle• Superior thyroid notch at anterior superior aspect• Posteriorly laminae form superior & inferior
cornua• Superior cornua are elongated & narrow, attach
to thyrohyoid ligament• Inferior cornua are short & thick, articulating
medially with sides of cricoid cartilage

Front view Side view

• Only complete ring in endolarynx, provides structural integrity
• Two portions, posterior lamina & anterior arch
• Lower border of cricoid cartilage is junction between larynx above & trachea below.

Posterior view Side view

• Paired pyramidal cartilages that sit at top of cricoid
cartilage lamina posteriorly.
• Span supraglottis & glottis, most in supraglottis
• Vertical height of arytenoid spans ventricle
• Vocal & muscular processes are at level of TVC.
• Vocal processes: Anterior projections of arytenoid
cartilages to which posterior margins of TVC attach.
• Superior process is at level of FVC
Arytenoid cartilage

• Corniculate cartilage: Rests on top of superior process
of arytenoid cartilage, within AE folds.
• Cuneiform cartilage: Lateral & superior to corniculate
within free edge of AE folds

The supraglottic division:From the superior-most tip of the epiglottis -to a
transverse plane through the laryngeal ventricle. The glottis:From this transverse plane to 1 cm inferiorly and
includes the true vocal cords. The subglottic regionFrom the inferior-most plane of the true cords -to
the inferior portion of the cricoid cartilage.


• Extends from tip of epiglottis above to laryngeal ventricle below.
• Contains vestibule, epiglottis, pre-epiglottic fat, AE folds, FVC, paraglottic space, arytenoid cartilages

• Pre-epiglottic space: Fat-filled space between hyoid bone anteriorly & epiglottis posteriorly
• AE folds: Projects from cephalad tip of arytenoid cartilages to inferolateral margin of epiglottis• Represents superolateral margin of supraglottis, dividing it from pyriform sinus (hypopharynx)

• False vocal cords: Mucosal surfaces of laryngeal vestibule of supraglottis.• Beneath FVC are paired paraglottic spaces
• Paraglottic spaces: Paired fatty regions beneath false & true vocal cords• Superiorly they merge into pre-epiglottic space• Terminates inferiorly at under surface of TVC




• TVC & anterior & posterior commissures
• Comprised of thyroarytenoid muscle (medial fibers are "vocalis muscle")• Anterior commissure: Midline, anterior meeting point of TVC



• Subglottis extends from under surface of TVC to inferior surface of cricoid cartilage
• Mucosal surface of subglottic area is closely applied to cricoid cartilage
• Conus elasticus: Fibroelastic membrane extends from medial margin of TVC above to cricoid below



















• Post-contrast:a) No enhancement of mucosal surface of larynxb) Hypopharyngeal mucosa enhances
Collapsed piriform sinus may mimic tumor on CT – confirmation is with a modified valsalva maneuver which distends the region

• False vocal cords, aryepiglottic folds, pre and para-epiglottic spaces are fat contatining – hence appear hypoattenuating
• Membranes such as thyrohyoid and cricothyroid are not well visualized
• Ossified cartilages appear hyperdense in outer and inner cortex with a hypodense central area (medullary fat)

• Cortical bone, fatty marrow and non-ossified hyaline cartilage do not show post-contrast enhancement.

• Compared with CT, MR imaging has an increased ability to separate various soft tissues such as tumor and muscle.
• Coronal and Axial T1 and Sagittal T2 sequences are used
• Fast spin-echo (FSE) imaging gives excellent images with valuable T2 information. Fat suppression may be used, as the fat signal can be high on FSE images. This allows better appreciation of the higher signal intensity coming from abnormal soft tissues that may be bordered by fat.

Neck surface coil is needed.
Slice thickness : 3–5 mm.
axial plane : parallel to the true vocal cords,
coronal plane :perpendicular to the definedaxial plane.
T1, T2, Fat saturation (FS) MRI, and Contrast-enhanced FS T1-WI are required.
Imaging techniquesMRI

• Sagittal images show the epiglottis, valleculae, and base of the tongue well.
• The postcricoid area is seen well, and the arytenoid cartilage often can be visualized on the cricoid cartilage.
• The preepiglottic fat is clearly seen on T1-weighted images.


The coronal view represents the ideal orientation for evaluation of the upper margin of the true cord.
On T1-weighted images true cord can be seen contrasted against the high signal intensity fat of the false cord immediately above.

• The axial images represent slices perpendicular to the inner surface of the thyroid and cricoid cartilage, allowing assessment of cartilaginous erosion.
• Ossified cartilage with fat in the medullary space has a high signal intensity on T1-weighted sequences. By comparison, the non-ossified cartilage tends to be dark on both T1-weighted and T2-weighted sequences.



• Hypopharyngeal and laryngeal mucosa show low to
intermediate SI on T1WI, higher SI on T2WI and significant post-contrast enhancement
• Muscular tissue eg pharyngeal constrictors and vocal cords show intermediate SI on T1 and T2WI, with no
post-contrast enhancement
• Therefore, with a T2WI and a post-contrast T1WI, we can easily differentiate mucosa (which enhances) from
muscle (which doesn’t enhance).


Enhancing mucosa with underlying non-enhancing muscle

• Previously described fat containing structures as expected show high SI on T1 and intermediate SI on T2 SE.
• On T1 and T2 FSE – fatty tissue shows high SI.• Despite MRI’s excellent tissue depiction, thin connective
tissue and membranes cannot be visualized.