Embed Size (px)
DESCRIPTION
Join Dale Sanders as he explains the concepts behind the Late-Binding (TM) Data Warehouse for healthcare. In this webinar, Dale covers 5 main concepts including 1) The history and concept of "binding" in software and data engineering, 2) Examples of data binding in healthcare, 3) the two tests for early binding (comprehensive and persistent agreement), 4) the six points of binding in data warehouse design (including a comparison of data modeling and late binding), and 5) the importance of binding in analytic progressions (including the eight levels of analytic adoption in healthcare).
Citation preview
© 2013 Health Catalyst
www.healthcatalyst.com
© 2013 Health Catalyst
www.healthcatalyst.com
Designing for Analytic Agility
Late Binding in Data Warehouses:
Dale Sanders, Oct 2013
© 2013 Health Catalyst
www.healthcatalyst.com
Overview
• The concept of “binding” in software and data
engineering
• Examples of data binding in healthcare
• The two tests for early binding
• Comprehensive & persistent agreement
• The six points of binding in data warehouse design
• Data Modeling vs. Late Binding
• The importance of binding in analytic progression
• Eight levels of analytic adoption in healthcare
© 2013 Health Catalyst
www.healthcatalyst.com
3
Late Binding in Software Engineering
1980s: Object Oriented Programming
● Alan Kay Universities of Colorado & Utah, Xerox/PARC
● Small objects of code, reflecting the real world
● Compiled individually, linked at runtime, only as needed
● Major agility and adaptability to address new use cases
Steve Jobs
● NeXT computing
● Commercial, large-scale adoption of Kay’s concepts
● Late binding– or as late as practical– becomes the norm
● Maybe Jobs’ largest contribution to computer science
© 2013 Health Catalyst
www.healthcatalyst.com
4 4
Atomic data must be “bound” to business rules about that data and
to vocabularies related to that data in order to create information
Vocabulary binding in healthcare is pretty obvious ● Unique patient and provider identifiers
● Standard facility, department, and revenue center codes
● Standard definitions for gender, race, ethnicity
● ICD, CPT, SNOMED, LOINC, RxNorm, RADLEX, etc.
Examples of binding data to business rules ● Length of stay
● Patient relationship attribution to a provider
● Revenue (or expense) allocation and projections to a department
● Revenue (or expense) allocation and projections to a physician
● Data definitions of general disease states and patient registries
● Patient exclusion criteria from disease/population management
● Patient admission/discharge/transfer rules
Late Binding in Data Engineering
© 2013 Health Catalyst
www.healthcatalyst.com
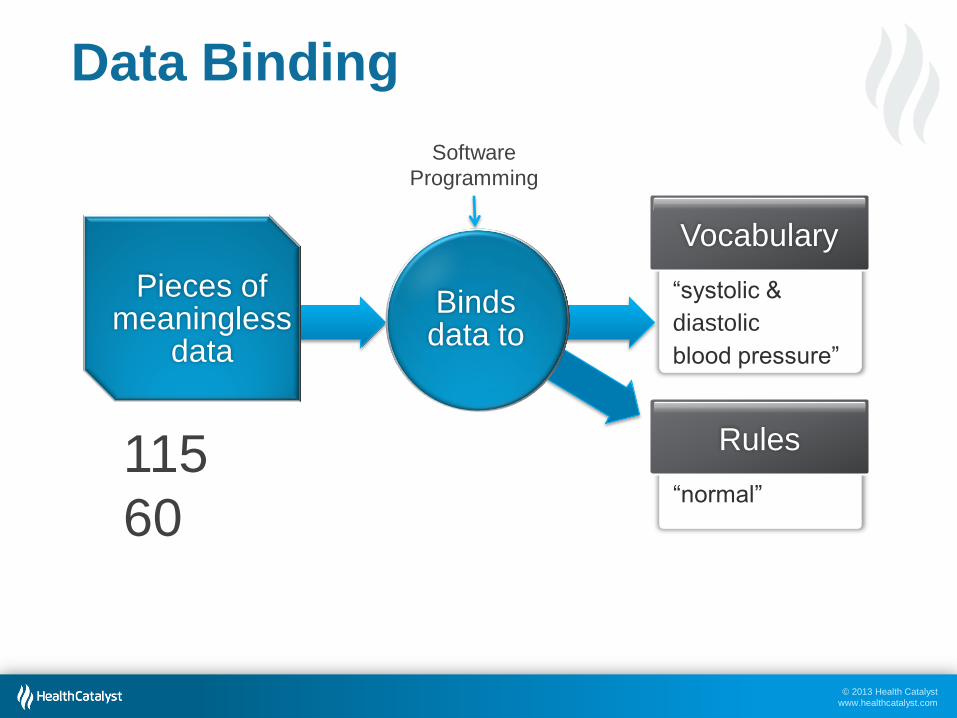
Data Binding
Vocabulary
“systolic &
diastolic
blood pressure”
Rules
“normal”
Pieces of meaningless
data
115
60
Binds data to
Software
Programming
© 2013 Health Catalyst
www.healthcatalyst.com
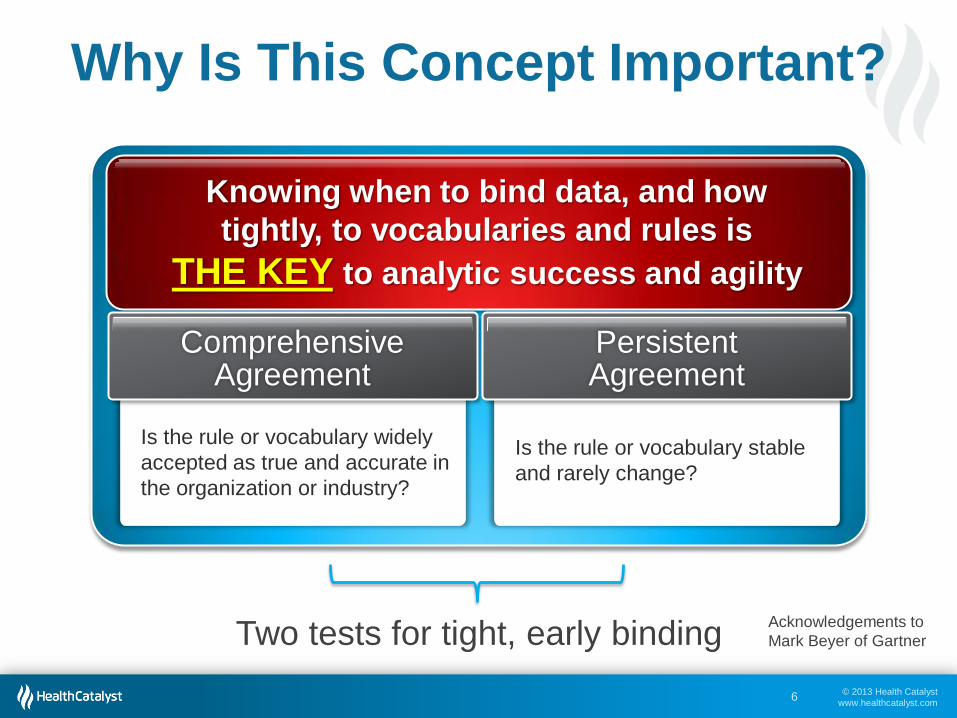
Why Is This Concept Important?
Two tests for tight, early binding
6
Knowing when to bind data, and how
tightly, to vocabularies and rules is
THE KEY to analytic success and agility
Is the rule or vocabulary widely
accepted as true and accurate in
the organization or industry?
Comprehensive Agreement
Is the rule or vocabulary stable
and rarely change?
Persistent Agreement
Acknowledgements to
Mark Beyer of Gartner
© 2013 Health Catalyst
www.healthcatalyst.com
ACADEMIC
STATE
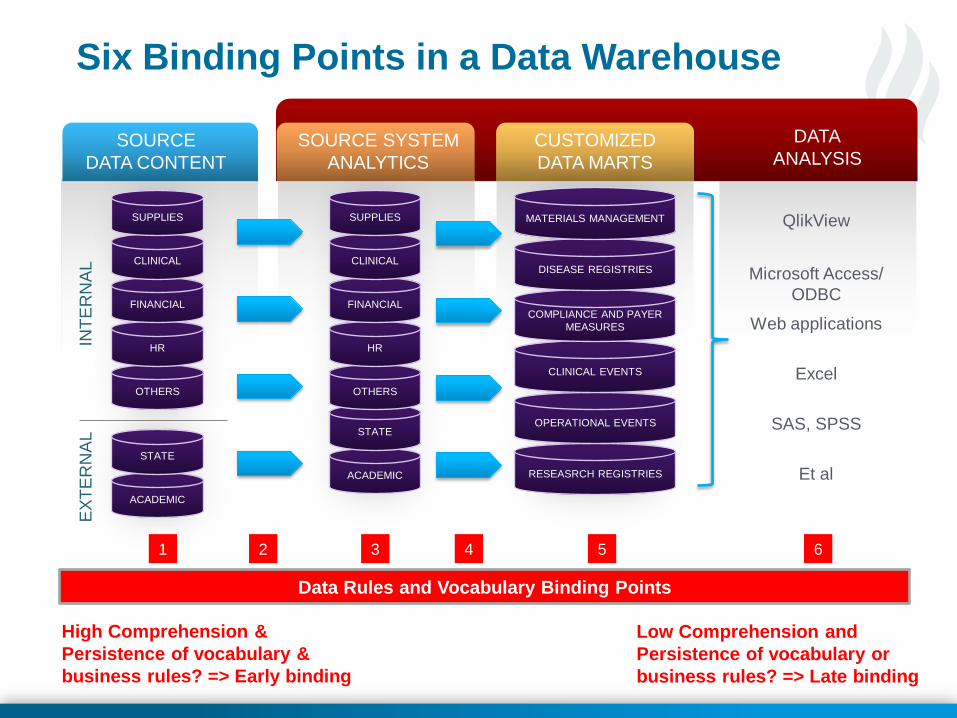
SOURCE
DATA CONTENT
SOURCE SYSTEM
ANALYTICS
CUSTOMIZED
DATA MARTS
DATA
ANALYSIS
OTHERS
HR
FINANCIAL
CLINICAL
SUPPLIES
INT
ER
NA
L
EX
TE
RN
AL
ACADEMIC
STATE
OTHERS
HR
FINANCIAL
CLINICAL
SUPPLIES
RESEASRCH REGISTRIES
QlikView
Microsoft Access/
ODBC
Web applications
Excel
SAS, SPSS
Et al
OPERATIONAL EVENTS
CLINICAL EVENTS
COMPLIANCE AND PAYER
MEASURES
DISEASE REGISTRIES
MATERIALS MANAGEMENT
3
Data Rules and Vocabulary Binding Points
High Comprehension &
Persistence of vocabulary &
business rules? => Early binding
Low Comprehension and
Persistence of vocabulary or
business rules? => Late binding
Six Binding Points in a Data Warehouse
4 2 1 5 6
© 2013 Health Catalyst
www.healthcatalyst.com
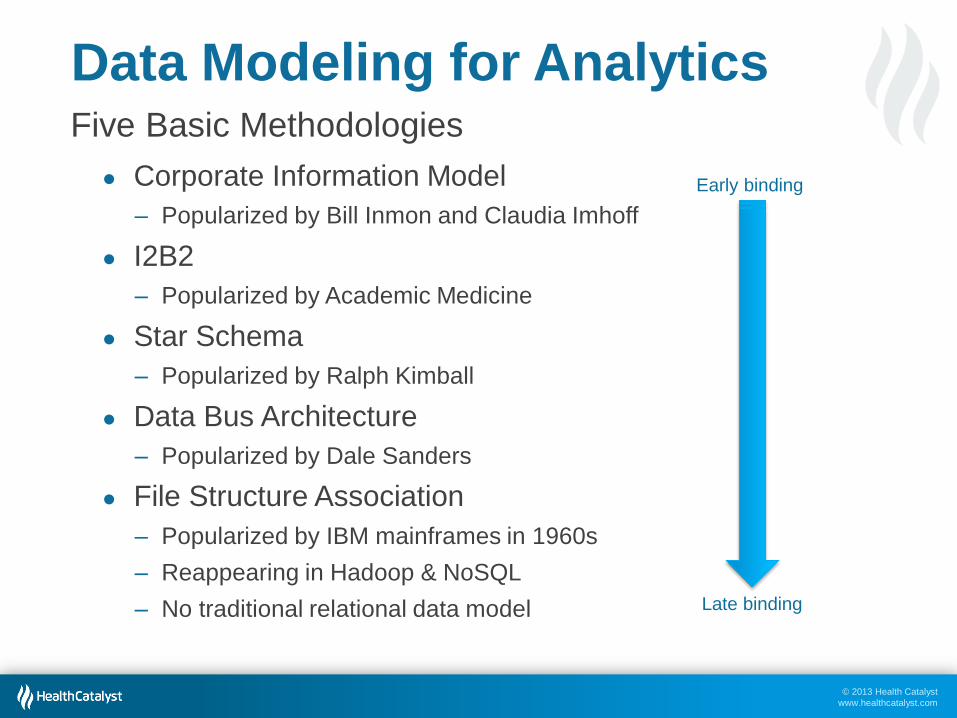
Data Modeling for Analytics Five Basic Methodologies
● Corporate Information Model
‒ Popularized by Bill Inmon and Claudia Imhoff
● I2B2
‒ Popularized by Academic Medicine
● Star Schema
‒ Popularized by Ralph Kimball
● Data Bus Architecture
‒ Popularized by Dale Sanders
● File Structure Association
‒ Popularized by IBM mainframes in 1960s
‒ Reappearing in Hadoop & NoSQL
‒ No traditional relational data model
Early binding
Late binding
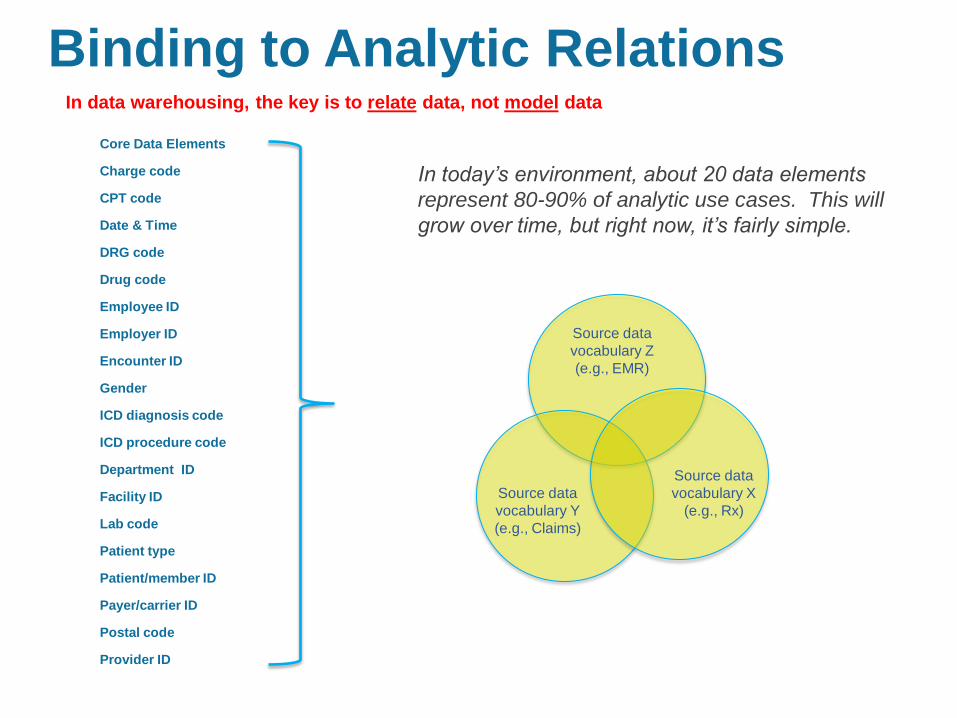
Binding to Analytic Relations
Core Data Elements
Charge code
CPT code
Date & Time
DRG code
Drug code
Employee ID
Employer ID
Encounter ID
Gender
ICD diagnosis code
ICD procedure code
Department ID
Facility ID
Lab code
Patient type
Patient/member ID
Payer/carrier ID
Postal code
Provider ID
In today’s environment, about 20 data elements
represent 80-90% of analytic use cases. This will
grow over time, but right now, it’s fairly simple.
Source data
vocabulary Z
(e.g., EMR)
Source data
vocabulary Y
(e.g., Claims)
Source data
vocabulary X
(e.g., Rx)
In data warehousing, the key is to relate data, not model data
© 2013 Health Catalyst
www.healthcatalyst.com
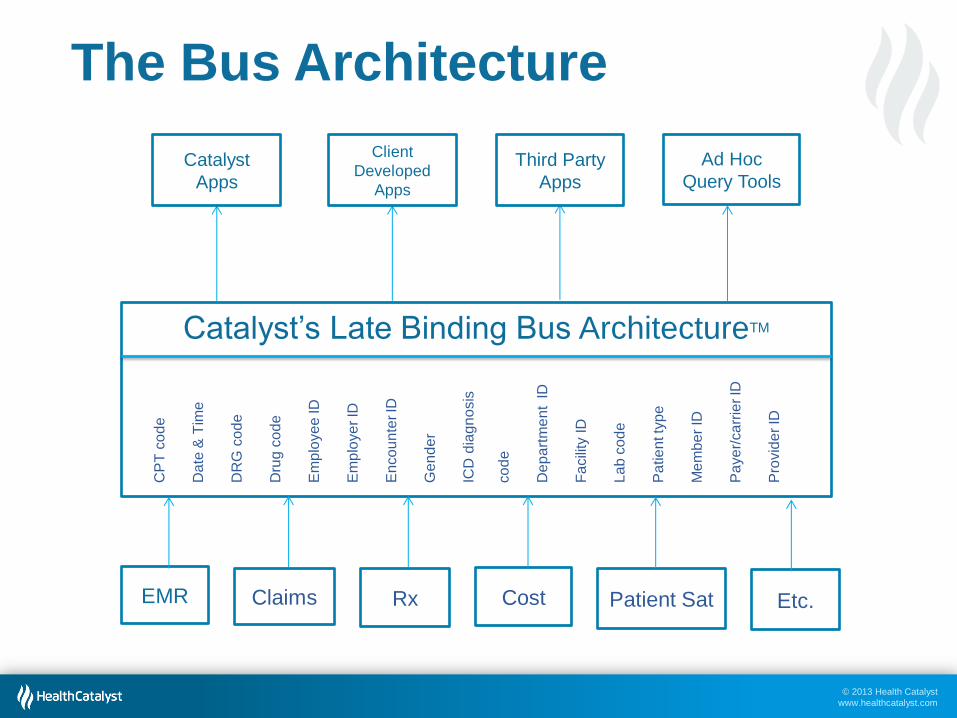
Catalyst
Apps
Client
Developed
Apps
Third Party
Apps
Ad Hoc
Query Tools
EMR Cost Rx Claims Etc. Patient Sat
Catalyst’s Late Binding Bus ArchitectureTM
CP
T c
od
e
Da
te &
Tim
e
DR
G c
od
e
Dru
g c
od
e
Em
plo
ye
e ID
Em
plo
ye
r ID
En
co
un
ter ID
Ge
nd
er
ICD
dia
gn
osis
co
de
De
pa
rtm
en
t ID
Fa
cili
ty ID
La
b c
od
e
Pa
tie
nt ty
pe
Me
mb
er
ID
Pa
ye
r/ca
rrie
r ID
Pro
vid
er
ID
The Bus Architecture
© 2013 Health Catalyst
www.healthcatalyst.com
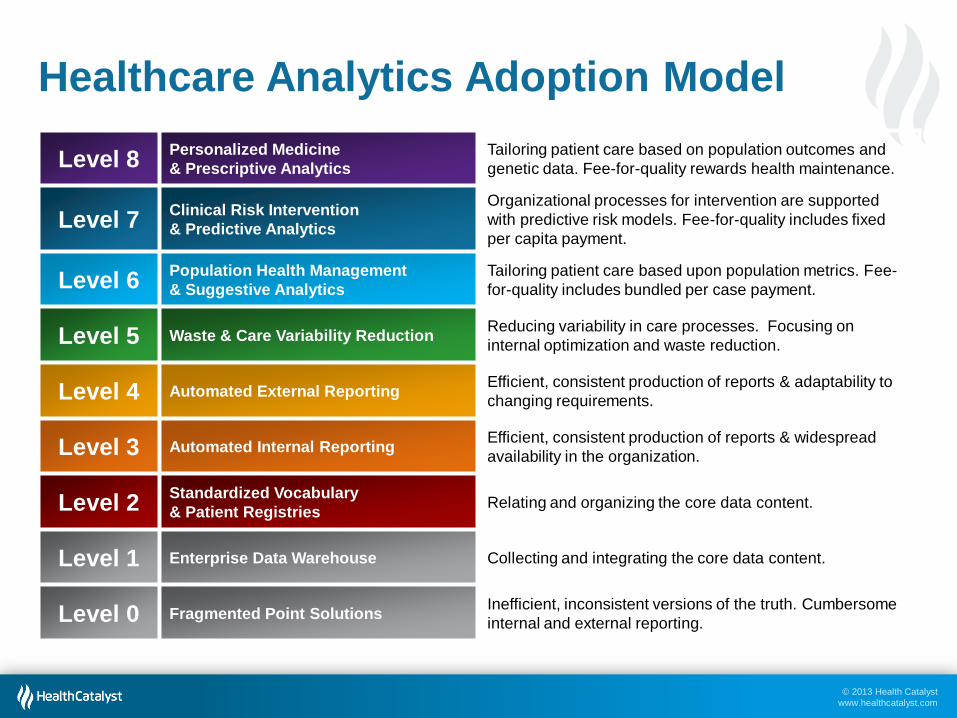
Healthcare Analytics Adoption Model
Level 8 Personalized Medicine
& Prescriptive Analytics
Tailoring patient care based on population outcomes and
genetic data. Fee-for-quality rewards health maintenance.
Level 7 Clinical Risk Intervention
& Predictive Analytics
Organizational processes for intervention are supported
with predictive risk models. Fee-for-quality includes fixed
per capita payment.
Level 6 Population Health Management
& Suggestive Analytics
Tailoring patient care based upon population metrics. Fee-
for-quality includes bundled per case payment.
Level 5 Waste & Care Variability Reduction Reducing variability in care processes. Focusing on
internal optimization and waste reduction.
Level 4 Automated External Reporting Efficient, consistent production of reports & adaptability to
changing requirements.
Level 3 Automated Internal Reporting Efficient, consistent production of reports & widespread
availability in the organization.
Level 2 Standardized Vocabulary
& Patient Registries Relating and organizing the core data content.
Level 1 Enterprise Data Warehouse Collecting and integrating the core data content.
Level 0 Fragmented Point Solutions Inefficient, inconsistent versions of the truth. Cumbersome
internal and external reporting.
© 2013 Health Catalyst
www.healthcatalyst.com
Progression in the Model The patterns at each level
• Data content expands
• Adding new sources of data to expand our understanding of care
delivery and the patient
• Data timeliness increases
• To support faster decision cycles and lower “Mean Time To
Improvement”
• Data governance and literacy expands
• Advocating greater data access, utilization, and quality
• The complexity of data binding and algorithms increases
• From descriptive to prescriptive analytics
• From “What happened?” to “What should we do?”
© 2013 Health Catalyst
www.healthcatalyst.com
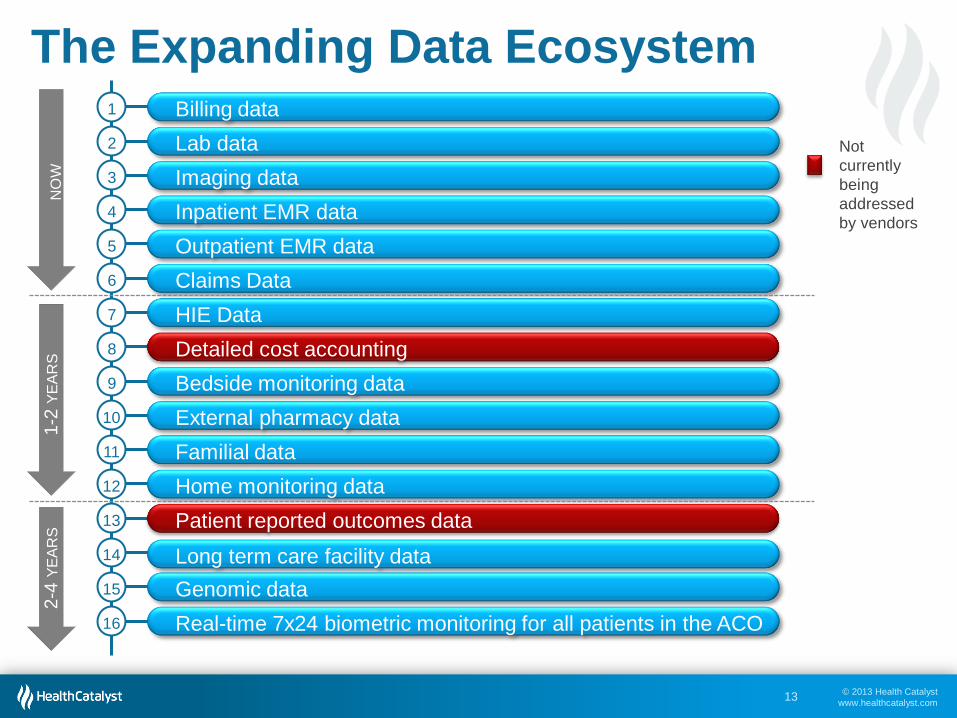
The Expanding Data Ecosystem
13
Billing data 1
Lab data 2
Imaging data 3
Inpatient EMR data 4
Outpatient EMR data 5
Claims Data 6
HIE Data 7
Detailed cost accounting 8
Bedside monitoring data 9
External pharmacy data 10
Familial data 11
Home monitoring data 12
Patient reported outcomes data 13
Long term care facility data 14
Genomic data 15
Real-time 7x24 biometric monitoring for all patients in the ACO 16
NO
W
1-2
YE
AR
S
2-4
YE
AR
S
Not
currently
being
addressed
by vendors
© 2013 Health Catalyst
www.healthcatalyst.com
Principles to Remember
1. Delay binding as long as possible… until a clear analytic
use case requires it
2. Earlier binding is appropriate for business rules or
vocabularies that change infrequently or that the
organization wants to “lock down” for consistent analytics
3. Late binding, in the visualization layer, is appropriate for
“what if” scenario analysis
4. Retain a record of the changes to vocabulary and rules
bindings in the data models of the data warehouse
● Bake the history of vocabulary and business rules bindings into
the data models so you can retrace your analytic steps if need be
14
© 2013 Health Catalyst
www.healthcatalyst.com
Closing Words of Caution
15
Healthcare suffers from a low degree of Comprehensive and Persistent agreement on many topics that impact analytics
The vast majority of vendors and home grown data warehouses bind to rules and vocabulary too early and too tightly, in comprehensive enterprise data models
Analytic agility and adaptability suffers greatly
• “We’ve been building our EDW for two years.”
• “I asked for that report last month.”