Embed Size (px)
Citation preview

Longitudinal research tracking the financing of peripheral public health care facilities in
Kenya
P4P – Evelyn Waweru Nov 2015

Outline
▪ Background: Kenyan health sector reforms
▪ Research methods (HSSF): pilot – baseline – interim – post devolution
▪ Challenges and opportunities in using the above methods
▪ Current proposal and way forward
NB: Peripheral health facilities = public health centres and dispensaries

Health Sector Services Fund
▪ An innovative GOK scheme to: - disburse funds directly to peripheral facilities - empower local communities through Health
Facility Management Committees (HFMCs)
• Overall goal: – generate sufficient resources for providing
curative, preventive and promotive services – Reduce user fees paid – account for the resources in an efficient and
transparent manner

District Focus
DEVOLUTION (2013)
KHSSP & KEPH
(1999*)
Updated financial guidelines
Gazette HFMCs (2009)
Kenya Health Policy Framework (1994*)
DHC/HFMCs
1975 1980 1985 1990
User Fees
Cost sharing (2004)
Community Strategy
FREE
Context: Global Health Debates: UHC, decentralisation and community participation
2010 Baseline survey
2012 Interim
2015 Proposal
2005 Pilot
Empirical research evaluating HSSF implementation
DFF Coast
HSSF Kenya

2005 Coast Pilot: Methods▪ Post-hoc assessment, conducted 2 to 3 years after
the scheme was introduced. ▪ It was not possible to assess the quantitative
impact on key indicators, such as utilization and fees charged, - No baseline data had been collected prior to
implementation, - Health Management Information System (HMIS) data
were neither sufficiently complete nor reliable. ▪ Focused our quantitative analysis on
intermediate/process outcomes that could be easily linked to the direct funding intervention, and using qualitative methods to explore stakeholder opinions on impact.

Community Engagement and
Accountability
Fees and Exemptions
Health Worker Motivation
Facility Level Expenditure
Increased Utilisation of services
Approval of Facility
Improved Quality of Services
Setup & Implemen-
tation
Context: Facility type and setting, experience with managing facility level funds, other MOH, NGO and FBO activities, general political and economic developments
Process Outcomes
Impact
Committee Functioning
Training and Guidelines
Facility Income
Planning and Financial
Management Systems
Support Supervision
Theory of Change: how we think HSSF should work
Coast Pilot: Key findings• Positive findings: HFMCs active and met regularly, funds
transferred and used appropriately and accounting procedures were followed – perceived impact: small increases in the funding available
for the day to day running of facilities greatly improved facility functioning and perceived quality of care
• Key challenges: inadequate training and documentation, lack of awareness of HSSF among the broader community, and continued charging of user fees above the official regulations.
• Building on this experience, HSSF was scaled up nationwide in public sector health centres and dispensaries.
Baseline survey (2010)
KWTRP commissioned by MOPHS ▪ Cross sectional survey of 248
peripheral facilities in 8 provinces
Methods ▪ Document reviews ▪ Interviews ▪ Questionnaires per facility
(n=6) In-charge HFMC (2) Patient (3)

Baseline: Key findings▪ Most facilities were ready to
receive HSSF: - Bank account - Functioning HFMC - Some training – more emphasis
on financial management
▪ Associations between health facility characteristics and the poverty level of the facility location - No major inequalities in inputs
received with slight pro-rich indicators in elec., lab, drug availability and staff
- There was need for an overall increase in inputs:
▪ User fees did not increase but there was still no adherence to cost sharing policy (10/20)
Health Policy and Planning
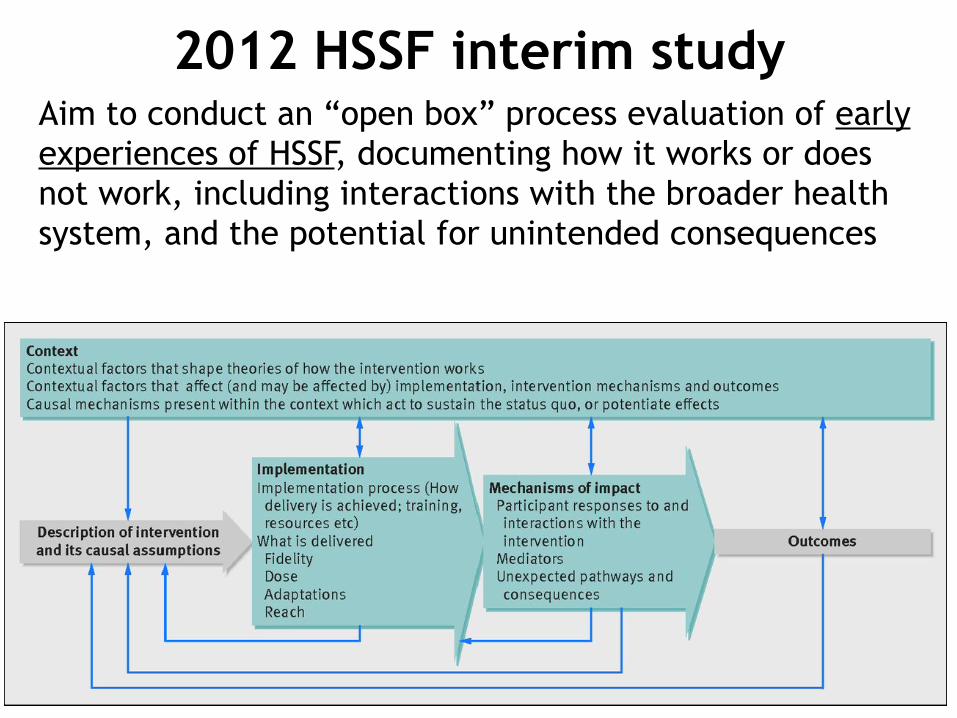
2012 HSSF interim studyAim to conduct an “open box” process evaluation of early experiences of HSSF, documenting how it works or does not work, including interactions with the broader health system, and the potential for unintended consequences

Methods (HSSF interim study)• Review of policy documents, administrative reports,
and financial data related to HSSF
• Key informant interviews with key stakeholders at national level (9)
• Sampling ➢ Selection: range of SES levels, and geographic locations,
discussions with DHMT (performance)
• Data collection in 10 health centres in 5 districts: ➢ 22 semi-structured interviews with managers, accountants and
facility in-charges ➢ 10 FGDs with committee members ➢ 99 exit survey with users (curative) ➢ facility record reviews on income and expenditure

Experiences with HSSF implementation

0.9% of total ‘on-budget’ health sector budget

▪ Disbursements started in November 2010 and by 2013 the money was being sent to almost all DHMTs, public health centres and dispensaries
KSH 112,000 (1,339 USD) per health centres KSH 27,500 (327 USD) per dispensariesKSH 131,500 (1,565 USD) per DHMTs
Per Quarter

▪ Funds were reaching facilities ▪ Visible improvements in facilities ▪ More reported outreach activities ▪ Improved perceived quality of care, staff
motivation and patient satisfaction ▪ Active involvement of HFMCs; greater
transparency and improved oversight of user fee revenues
Perceived positive impacts

HSSF Implementation ChallengesFinancing ▪ Delays in receiving funds: AIEs
were also fixed ▪ Inadequate level of funds ▪ Low allowances “peanuts” ▪ Different donor opinions
“the lack of the involvement of the district treasury is the Achilles heel of HSSF” (National KI)
Low adherence to user fee policy ▪ Only one facility reported
reducing user fees ▪ User fee revenue accounted for
half of facility annual income: – User fees – USD 910 – 25,455 – HSSF funds – USD 3,870 – 6,543
Supportive supervision
▪ Lack of training on financial management
▪ Lack of facilitation and systematic M&E
▪ Overworked CBAs
▪ Reluctant in-charges “Kwamad with terror” (National KI)
▪ Lack of clarity in roles and responsibilities across all levels
▪ Low community awareness of HSSF

Unintended consequences
▪ Difficult documentation with the reporting process still centralised
▪ Difficulties in accessing crucial user fee funds: same access rules
▪ Bypassing the district treasury
▪ Relationship problems between key stakeholders - Diff views on how HSSF
should work after devolution
Recommendations
▪ Expand decision space - local levels
▪ Facilitate supportive supervision - Improvise to manage
paperwork
▪ Clarify roles and responsibilities: refresher training
▪ Increase pool, buy- in / alternatives
▪ Increase inputs

Now? Re-organisation of the Kenyan health system
• Devolution: 47 new semi-autonomous counties (control decisions)
• User fee “removal” + free maternal (P. Directive)
• Debate on future HSSF design o funds be controlled at county of
national level? o integrated into standard
government financial systems? Role of insurance?
o performance related?

Financing of peripheral public health care facilities in Kenya:
similarities and differences across counties in strategies, and their implementation and perceived
impact
1. To describe the range of financing approaches for peripheral facilities across Kenyan counties
– allocation of HSSF funds, alternative finance mechanisms, accountability and supervision processes, and staff involved
2. To document peripheral facility income sources, levels and expenditure patterns in the period before and during devolution
3. To explore how differences in supportive supervision and accountability procedures affect facility processes

Conceptual framework : How HSSF is to function in a devolved health system context
• 1. • Use of Funds • 2. • Access rules • 3. • Human resource • 4. • Governance / • accountability • 5. • Resource Allocation
Context: Peripheral facility funding regulatory/legislative frameworks, policies and priorities of national government, international organisations, and county government
Consequences for peripheral health facilities
Facility income & expenditure
Adherence to user fee
regulationsInternal & community
accountability
Health worker motivation
Perceived Quality of
care
Utilisation
5 key decision making domains: theory and practice

Study site selection
Kilifi County
National Level KIs
Vihiga County
Sub County1
Kajiado County
Sub County3
Sub County 2
Sub County4
Sub County6
Sub County5
Sub County7
Sub County9
Sub County8
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
1 HC 1 Disp
TOTALS National interviews: 12 or more Counties: 3 Sub-counties: 9 Health centres: 9 Dispensaries: 9
Selection of counties and sub-counties
• Geographical location • SES • Interim study sites • For sub-county rural/Urban

Data collection methods National • MOH, National treasury, the HSSF Secretariat, CRA,
Donors (World Bank, DANIDA and WHO)
County • CHMT, • CBAs, county treasury • County assembly
Sub- county • Sub-county health management team members (at
least 4)
Facility • Facility in-charge (health workers) • HFMC (Quorum of 3) • Patients (after curative care)
In-depth interviews Observation Meeting minutes FGDs Document review Questionnaires
In-depth interviews Document review
In-depth interviews Document review
In-depth interviews Document review

Limitations • Primarily qualitative: need for balanced mixed
methods - baseline costing requirements to guide resource allocation?
• Achievements of one financing intervention in the context of other mechanisms and other mechanisms
• Comparative sampling • Timeliness of data analysis and write up • Influence of contextual challenges,
– Unreliable drug supply, – Poor access to emergency transportation – Shortages of qualified staff – Limits in downwards accountability to users and
communities. – Continuity: personnel and funding- for reflexivity

Opportunities and future considerations
• Use of mixed methods, process evaluation, economic evaluation?
• Theory driven design • How to evaluate the interactions between
and influences of different mechanisms studied
• Learning from challenges and opportunities • Data sharing opportunities • Your suggestions?

Acknowledgements• Supervisors: Drs Sassy
Molyneux, Catherine Goodman
• Co-investigators: Benjamin Tsofa, Mary Nyikuri, Jacinta Nzinga, Edwine Barasa, Jane Chuma, Anisa Omar, Timothy Malingi