Embed Size (px)
Citation preview

LOWER RESPIRATORY TRACT DISORDERS
Presented By:Pandya Tejas.J.
2nd Year M.Sc Nursing StudentChild Health Nursing
Sumandeep Nursing College

1/6/2015 2
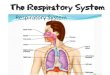
Anatomy of the Lower Respiratory Tract

1/6/2015 Free template from www.brainybetty.com 3

1/6/2015 Free template from www.brainybetty.com 4

1/6/2015 Free template from www.brainybetty.com 5

1/6/2015 Free template from www.brainybetty.com 6

1/6/2015 Free template from www.brainybetty.com 7

1/6/2015 Free template from www.brainybetty.com 8

1/6/2015 Free template from www.brainybetty.com 9

1/6/2015 Free template from www.brainybetty.com 10

Role of Nurse
1/6/2015 Free template from www.brainybetty.com 11

1/6/2015 Free template from www.brainybetty.com 12

Bronchopneumonia
1/6/2015 Free template from www.brainybetty.com 13

Introduction:Pneumonia is an inflammation of thePneumonia is an
inflammation of the parenchyma of the lungs.parenchyma
of the lungs.
Pneumonia can be classified anatomically
asPneumonia can be classified anatomically as lobar or
lobularlobar or lobular,,
bronchopnemoniabronchopnemonia andand interstitial
pneumoniainterstitial pneumonia.
Pathologically there is consolidation of
alveoliPathologically there is consolidation of alveoli or
infiltration of the interstitial tissue withor infiltration of the
interstitial tissue with inflammatory cell or bothinflammatory
cell or both
1/6/2015 Free template from www.brainybetty.com 14

Definition:
Acute inflammation of the walls of the smaller bronchial
tubes, with irregular areas of consolidation due to spread of
the inflammation into the peribronchiolar alveoli and the
alveolar ducts of the lungs.
INCUBATION PERIOD IS 1 TO 3 DAYS
1/6/2015 Free template from www.brainybetty.com 15

Etiology:-• Viral Pneumonia by RSV Influenza
• Bacterial:-
• Klebsiella
• E. coli
• H. influenza
• Gram (+)& (-) Bacteria
• Staphylococcus
• Chlamydia & Mycoplasma organism
• Pneumocystis carinii
• Fungi
• Histoplasmosis
• Coccidiomycosis
• Metazoa
• Aspiration of food, oily nose drops and liquid paraffin
• Kerosene poisoning
• Hypersensitivity pneumonia 16

Some terms
Recurrent pneumonia is defined is defined as 2 or as 2
or more episodes in a single yr episodes in a single yr or
3 or more or 3 or more episodes ever, with radiographic
clearing episodes ever, with radiographic clearing
between occurrences. between occurrences.
Slowly resolving pneumonia refers to the refers to the
persistence of symptoms or radiographic persistence of
symptoms or radiographic abnormalities beyond the
expected time abnormalities beyond the expected time
course.
1/6/2015 Free template from www.brainybetty.com 17

PATHOPHYSIOLOGY:
1/6/2015 Free template from www.brainybetty.com 18

Clinical Manifestation• Onset of pneumonia may be insidious starting Onset of
pneumonia may be insidious starting with URTI or may be
acute with high fever,
• Dypsnea
• grunting respiration.
• Respiratory rate always is increased.
• In drawing of chest
1/6/2015 Free template from www.brainybetty.com 19

Conti…• Nasal Flare Nasal flaring: with inspiration, the side of the
nostrils flares outwards
• Wheezing
• Coughing
• High fever
• Crackles
• techypnea
• Chest pain
• Respiratory distress
1/6/2015 Free template from www.brainybetty.com 20

Diagnosis
1/6/2015 Free template from www.brainybetty.com 21

Conti…
• The peripheral white blood cell (WBC) count can be The
peripheral white blood cell (WBC) count can be useful in
differentiating viral from bacterial useful in differentiating
viral from bacterial pneumonia.
• In viral pneumonia, the WBC count can be normal or
elevated but is usually not higher than
20,000/mm3,elevated, with a lymphocyte predominance.
Bacterial with a lymphocyte predominance. Bacterial
pneumonia (occasionally, adenovirus pneumonia)
ispneumonia (occasionally, adenovirus pneumonia) is
often associated with an elevated WBC count in the often
associated with an elevated WBC count in the range of
15,000-40,000/mm3 and granulocytes.
1/6/2015 Free template from www.brainybetty.com 22

Conti….Chest X-ray
CT-Scan
ASO-titer
Tuberculin Skin Test
1/6/2015 Free template from www.brainybetty.com 23

Treatment
1/6/2015 Free template from www.brainybetty.com 24

1/6/2015 Free template from www.brainybetty.com 25

Prevention
1/6/2015 Free template from www.brainybetty.com 26

1/6/2015 Free template from www.brainybetty.com 27

• Treatment of suspected bacterial pneumonia is based on
the presumptive cause and the clinical appearance on
the presumptive cause and of the child.
• For mildly ill children who do not require hospitalization,
amoxicillin is recommended. In communities with a high
percentage of penicillin-resistant pneumococci, high (80–
90 mg/kg/24 hr) should be prescribed.90 mg/kg/24 hr)
should be prescribed.
• Therapeutic alternatives include cefuroxime axetil or
amoxicillin/clavulanate amoxicillin/clavulanate
1/6/2015 Free template from www.brainybetty.com 28

• For school-aged children and in those in whom infection with M.
pneumonia or C. pneumoniae (atypical pneumonias) is
suggested, a macrolide antibiotic such as azithromycin is an
appropriate choice.
• In adolescents, a respiratory fluoroquinolone , a respiratory
fluoroquinolone (levofloxacin, gatifloxacin, moxifloxacin, may
be considered for atypicalgemifloxacin).
• The empirical treatment of suspected bacterial pneumonia in a
hospitalized child requires an pneumonia in a clinical
manifestations at the time of presentation.
• Parenteral cefuroxime (150 mg/kg/24 hr), cefotaxime, or
ceftriaxone is the mainstay of therapy cefotaxime, when bacterial
pneumonia is suggested.
• If clinical features suggest staphylococcal pneumonia
(pneumatoceles, empyema), initial antimicrobial therapy should
also include vancomycin or therapy should also include
vancomycin or clindamycin.clindamycin. 29

Complication
1/6/2015 Free template from www.brainybetty.com 30

If present of the plural effusion perform the
Inter costal Drainage
1/6/2015 Free template from www.brainybetty.com 31