Embed Size (px)
Citation preview

Contrast management
Dr. Luca Grancini
Centro Cardiologico Monzino, Milano
2014
NowContrast-Induced Acute Kidney Injury
CI-AKI
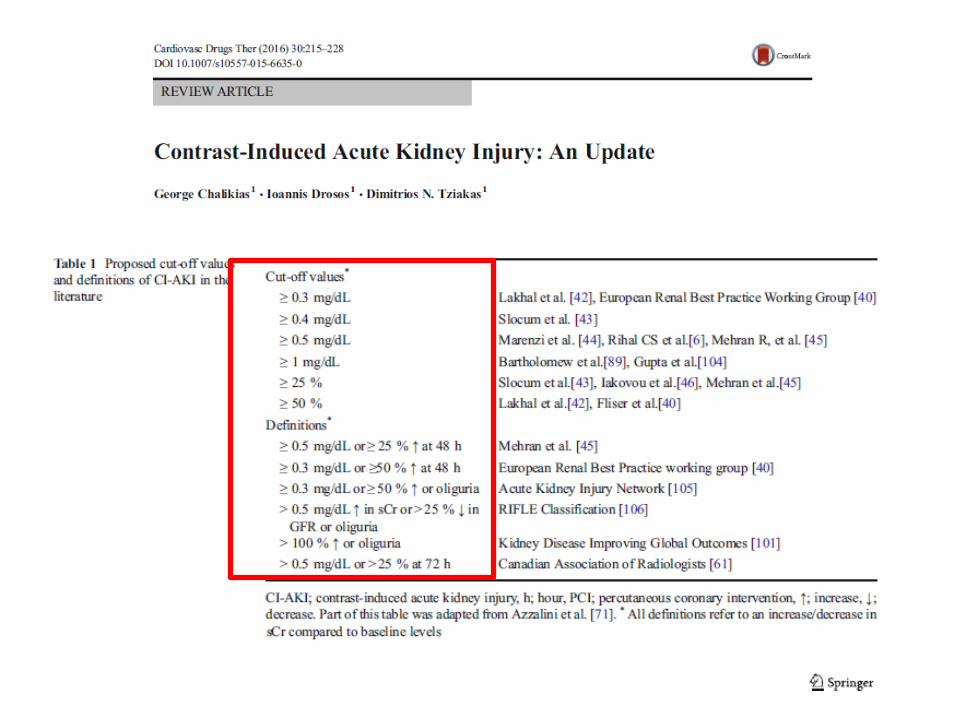
Definition
CI-AKI is defined as a 25% or 0.5 mg/dl increase in creatininefrom baselineor an increase in cystatin C >10%
within 48 to 120 hours of intravenous contrast exposure
CI-AKI
Important complication of use of radiocontrast agents, representingthe third leading cause of hospital-acquired acute kidney injury
CI-AKI typically manifests within 1-3 days of CM administration, peakswithin 3–5 days and resolves within 10– 21 days.
In rare occasions sustained or permanent kidney injury occurswarranting the use of dialysis.
To monitor for CI-AKI, it is recommended that serum creatinine follow-up should be obtained at not less than 24 h or more than 72 hfollowing contrast exposure.
It is believed to be due to renal artery vasoconstriction induced by contrast media, which leads to renal medullary hypoxia.
Other mechanisms include delayed intrarenal transit of the contrastagent as a result of vasoconstriction leading to oxidative stress damage
Direct tubular damage due to receptor-mediated tubularreabsorption of filtered contrast
CI-AKI

How much is too much?
General measures
Administration of the lowest possible dose of contrast medium, use of low or iso-osmolar contrast agents
Maintenance of hemodynamic stability throughout the procedure to ensure adequate renal perfusion.
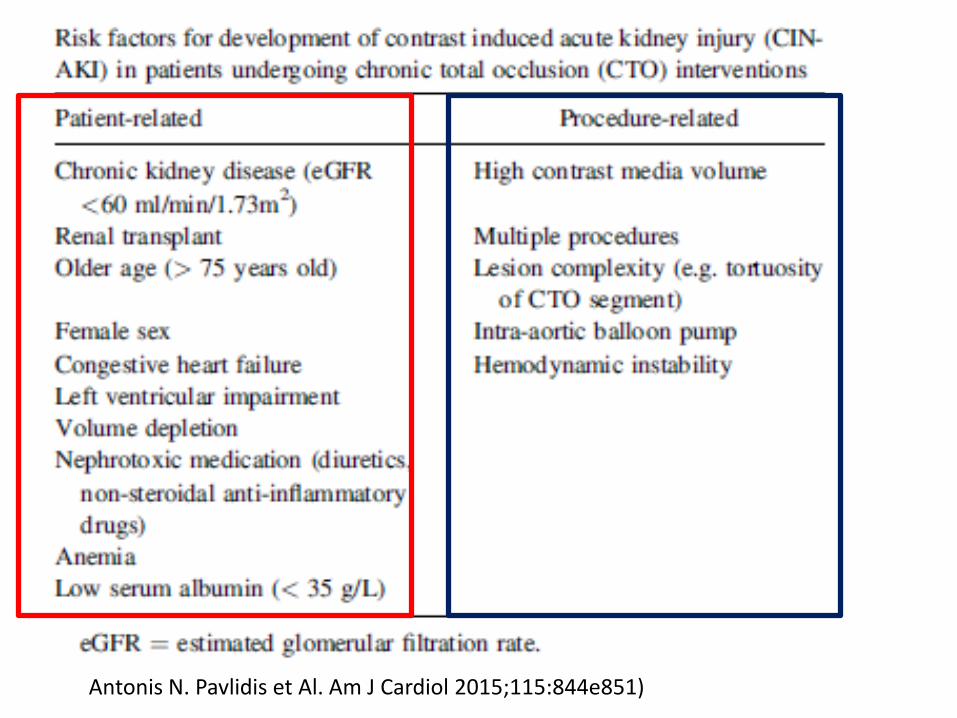
Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
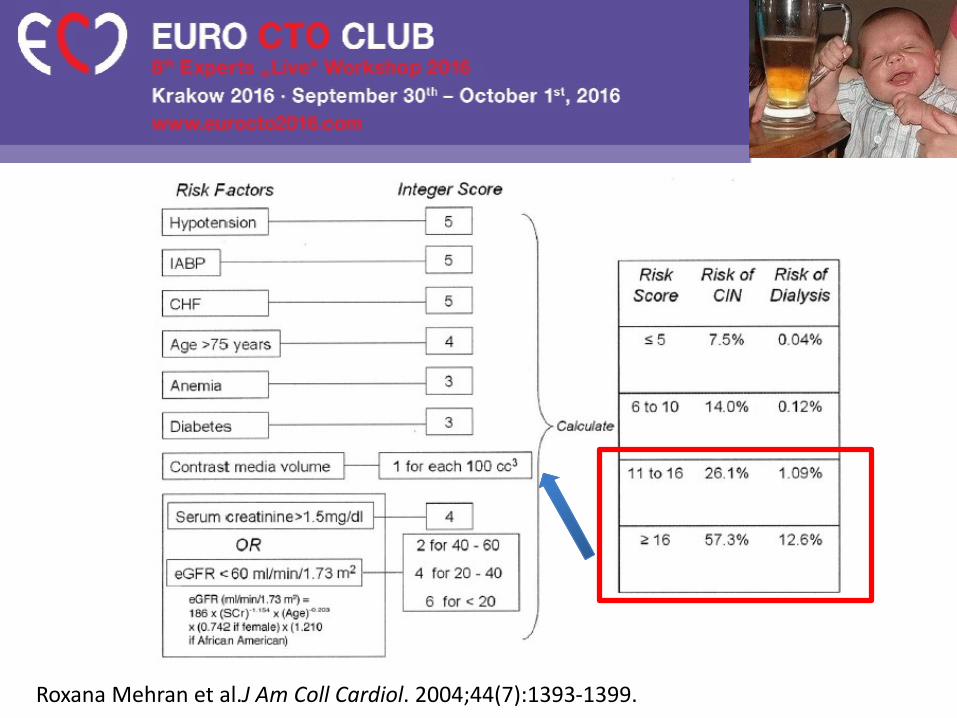
Roxana Mehran et al.J Am Coll Cardiol. 2004;44(7):1393-1399.
Cigarroa et al reported an empiric formula forcalculating the maximal acceptable contrast dose (MACD):
5 ml x body weight (kilograms)/serum creatinine (milligrams per deciliter)
The use of contrast beyond the MACD was later correlated to an increased risk of CI-AKI
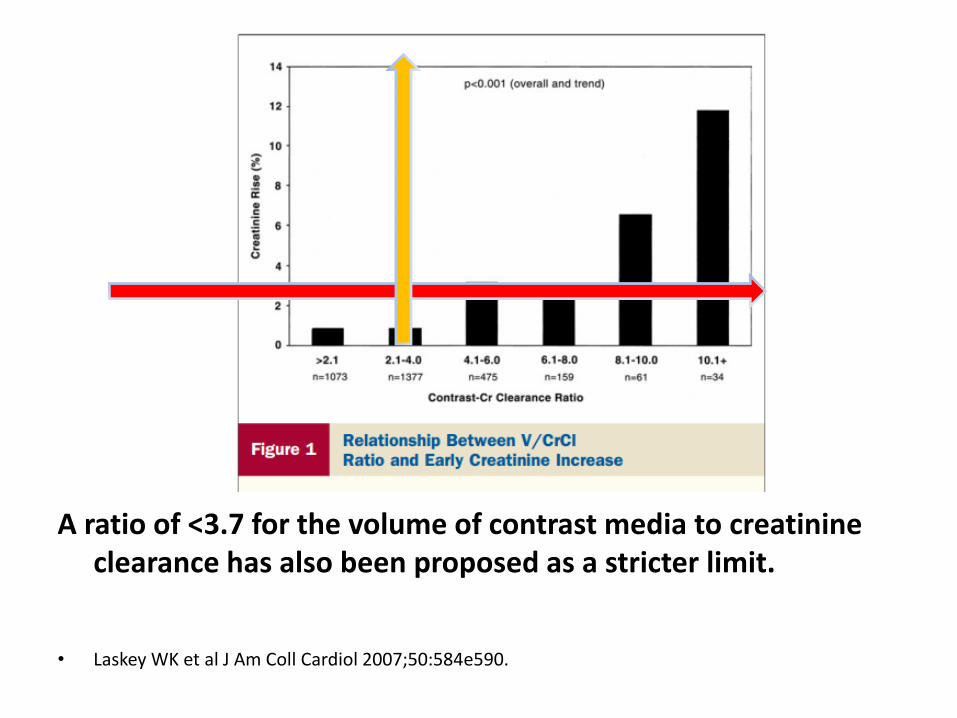
A ratio of <3.7 for the volume of contrast media to creatinineclearance has also been proposed as a stricter limit.
• Laskey WK et al J Am Coll Cardiol 2007;50:584e590.
During CTO, patients who underwent PCI receiving 400 ml of contrast have an almost 2-fold higher incidence of CI-AKI compared with those receiving <400 ml of contrast.
However, in the absence of coexistent CKD and diabetes mellitus, the incidence of CI-AKI remains low, even after high volumes of contrast media ( 5.4% ).
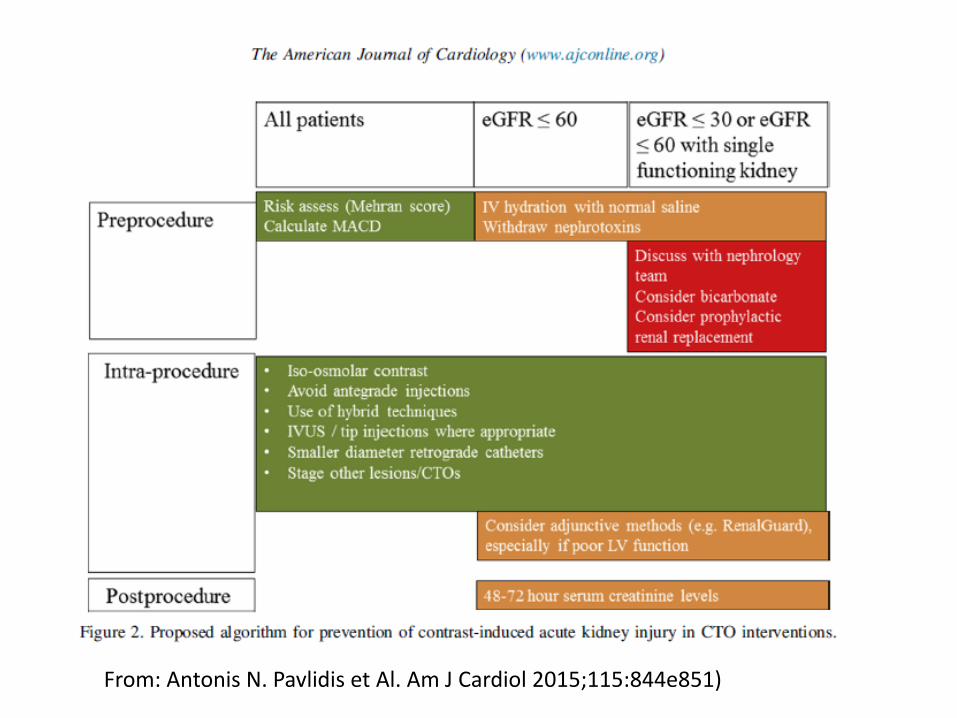
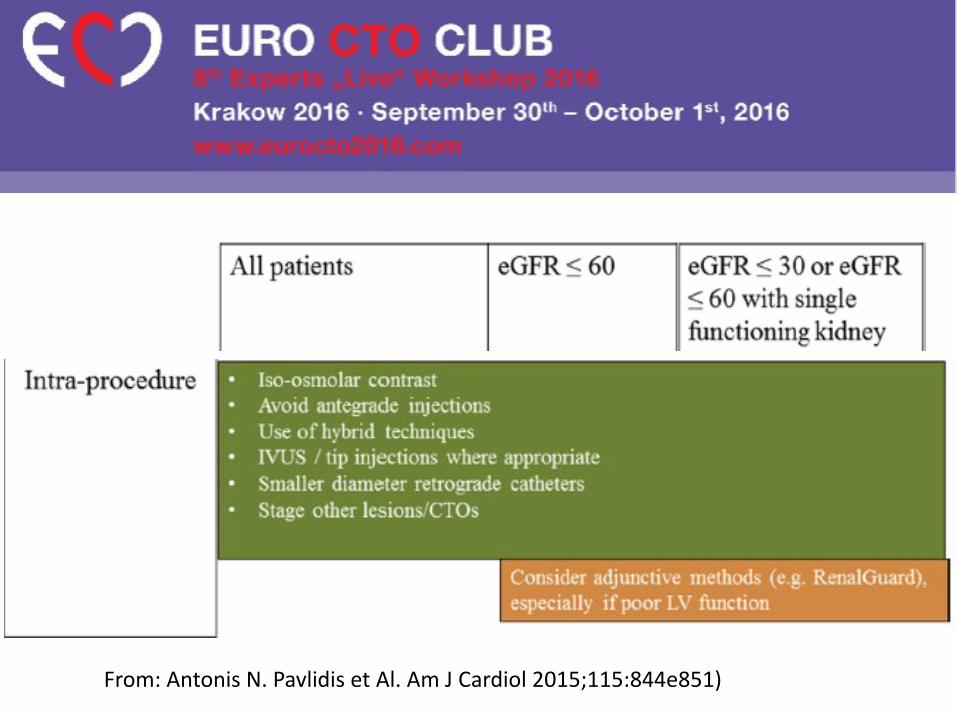
From: Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
The estimated average amount of contrast load in CTO procedures is 350 ml compared with uncomplicated PCI procedures where it has been reported in the range of 150 to 200 ml.
© 2
014 E
uro
Inte
rvention. A
ll rights
reserv
ed.
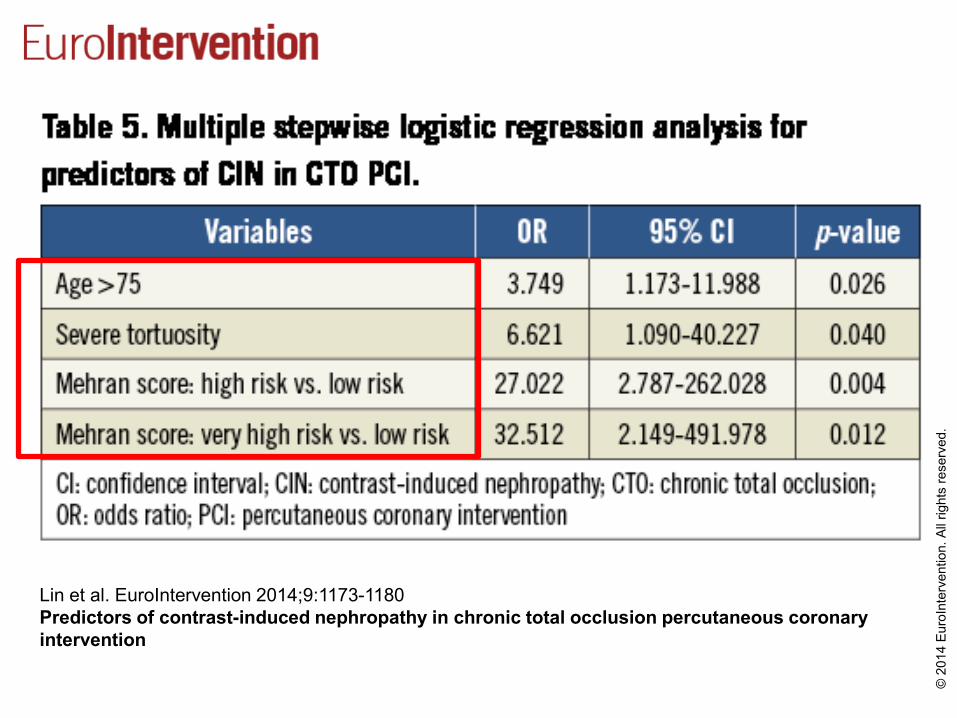
Lin et al. EuroIntervention 2014;9:1173-1180
Predictors of contrast-induced nephropathy in chronic total occlusion percutaneous coronary
intervention
The majority of CIN patients (53.6%; 15/28) recovered their baseline renal function within three months, even those who were in the high-risk categories (50%; 7/14).
The risk of developing CIN in CTO PCI is relatively low and the Mehran scoring system is a good predictor for CIN in CTO PCI
Lin et al. Eurointervention 9:1173-1180 2014
CI-AKIPREVENTION
From: Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
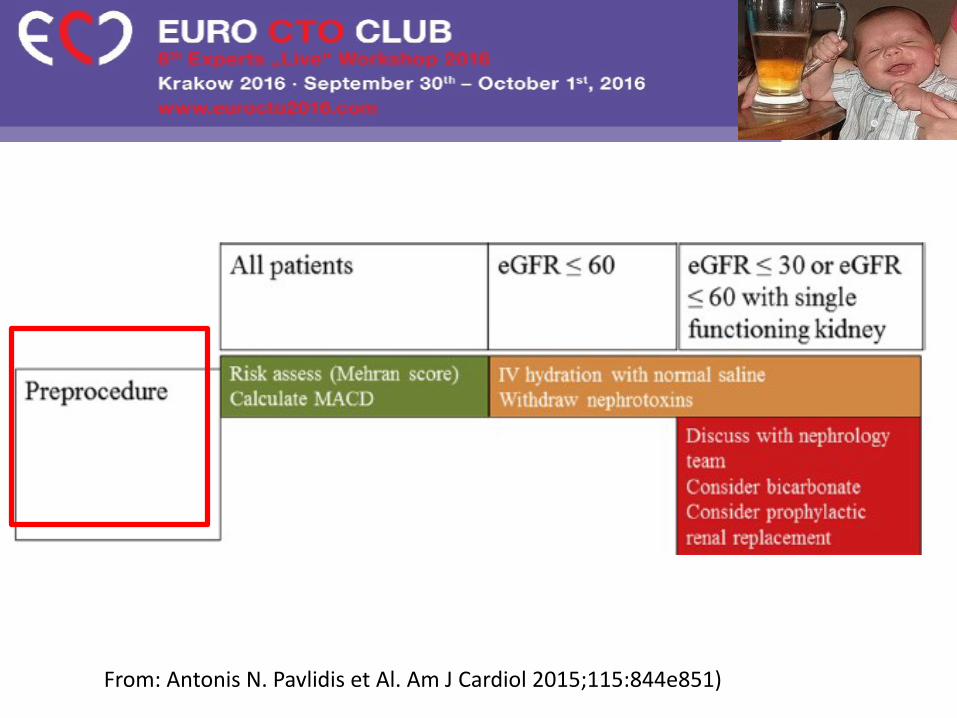
From: Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
Intravenous 0.9% sodium chloride has been shown to be more effective than 0.45%sodium chloride or oral hydration in prevention of CI-AKI
The most widely used approach is the administration of
intravenous 0.9% sodium chloride at a rate of 1 ml/kg/hour for 24 hours
beginning 12 hours before administration of the contrast medium
to achieve a urine output of >150 ml/hour.
Patients with moderate-to-severe left ventricular dysfunction:
cautious hydration with isotonic 0.45% saline
and close monitoring of urine output aiming to maintain a euvolemic state.
From: Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
Intra CTO technical tips
From: Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
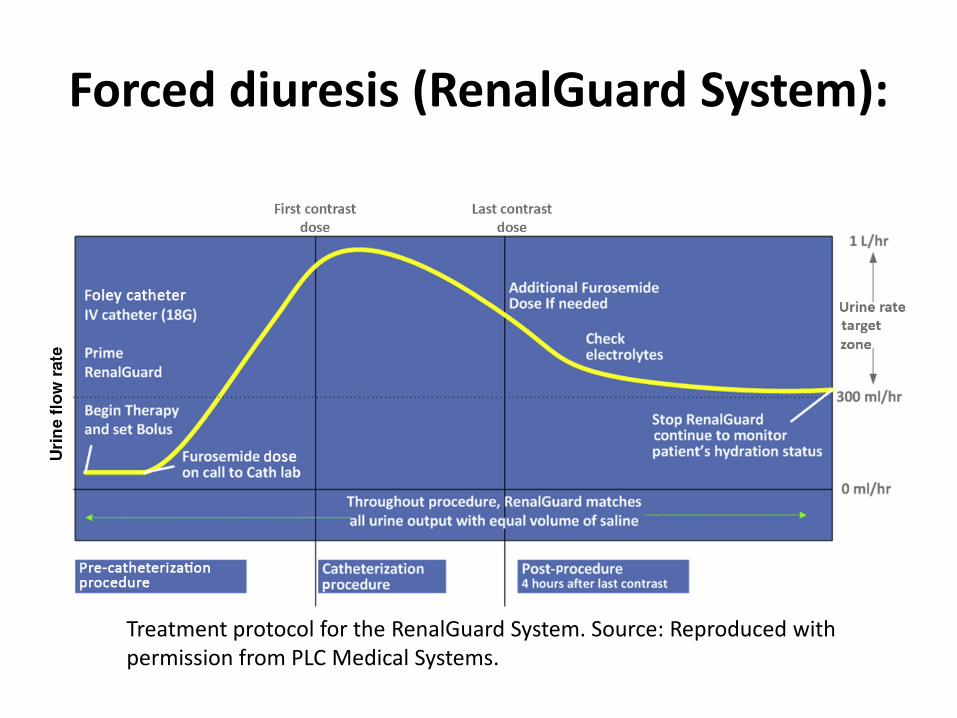
Forced diuresis (RenalGuard System):
Treatment protocol for the RenalGuard System. Source: Reproduced with permission from PLC Medical Systems.
The physiological benefits include a more rapid transit of contrast through the kidneys and reduced oxygen consumption in the medulla of the kidney.
The study showed a 3-fold reduction in CI-AKI,which was also associated with a lower incidence of postprocedural major adverseclinical events
Marenzi G et al.: the MYTHOS trial. JACC Cardiovasc Interv 2012;5:90e97.
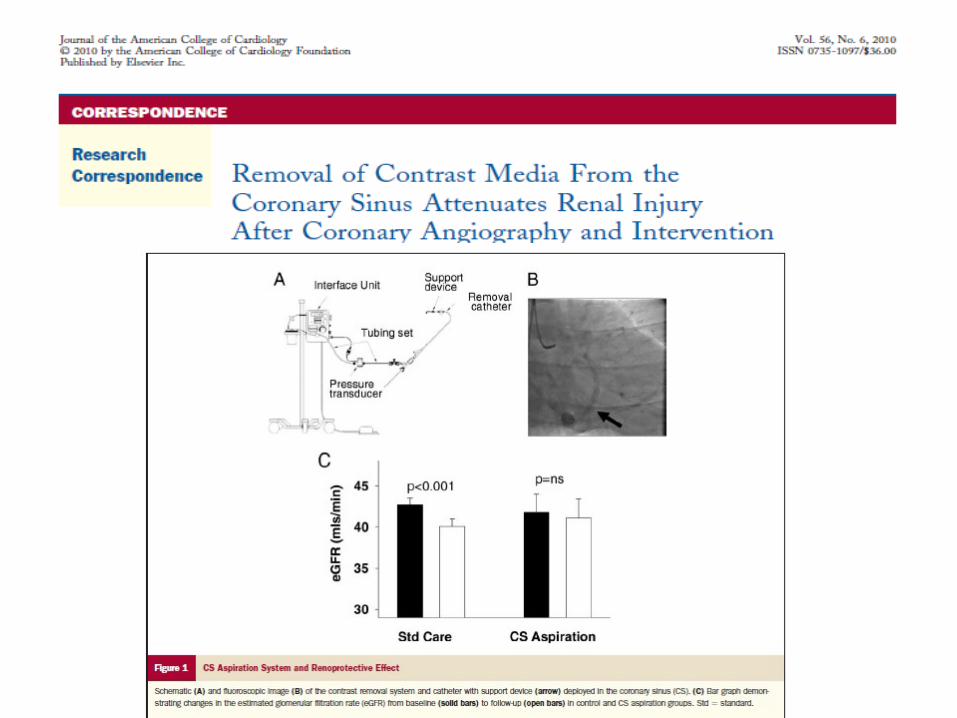
The CI-AKICOR System
Comprises an 11Fr coronary sinus aspiration catheter that is inserted through the jugular vein. On activation,it exerts a vacuum effect and removes contrast from the coronarysinus.
Stephen J. Duffy, MD, PhD
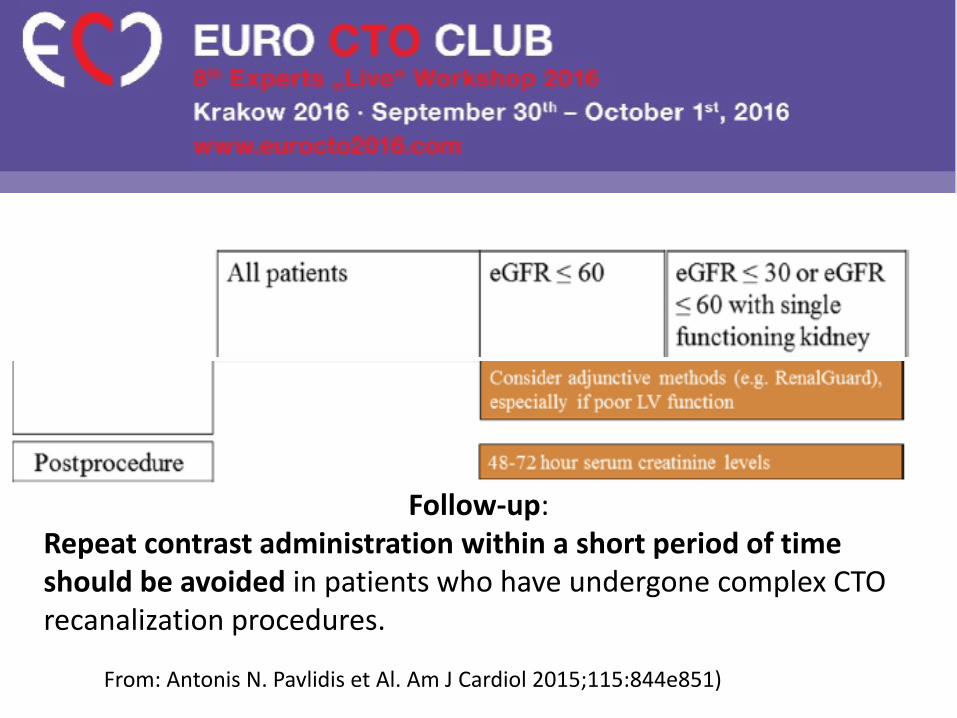
Follow-up: Repeat contrast administration within a short period of time should be avoided in patients who have undergone complex CTO recanalization procedures.
From: Antonis N. Pavlidis et Al. Am J Cardiol 2015;115:844e851)
CONCLUSIONNearly one-third of the in-hospital mortality risk post PCI is attributable to AKI; avoiding nine cases of AKI post PCI could potentially save one life.
Although the use of a high contrast dose at time ofPCI significantly increases the risk of AKI, contrast dosing is only a minor contributor to the overall burden of AKI.
Judith Kooiman et al. Circ Cardiovasc Interv. 2015;8:e002212
CONCLUSION
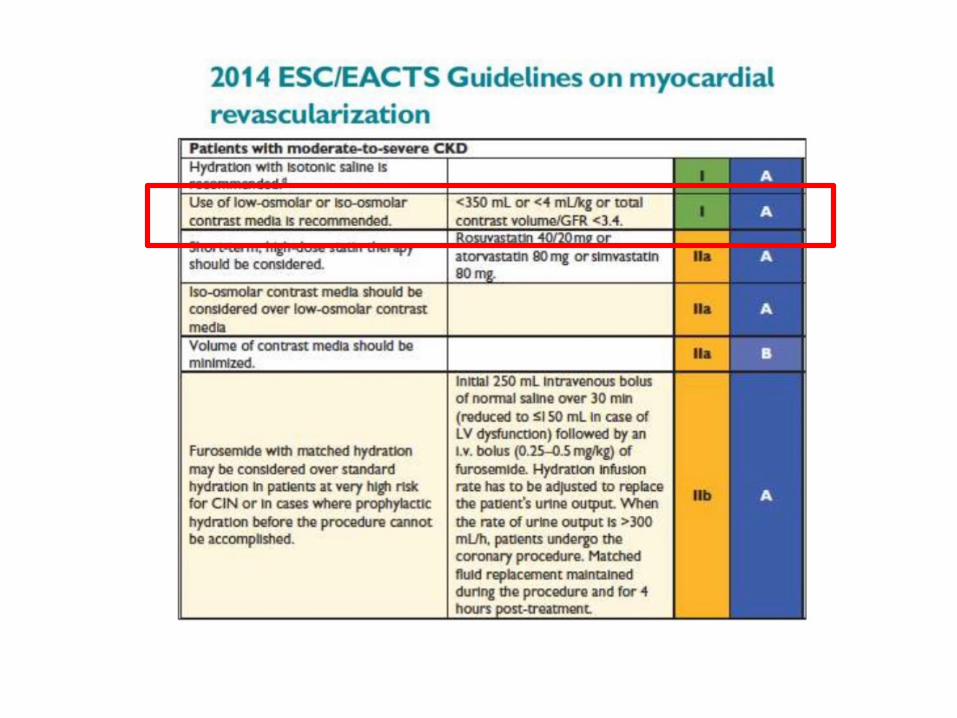
In patients with moderate-to-severe CKD the 2014 ESC EACTS guidelinesrecommend: <350 mL or <4 mL/kg or total contrast volume/GFR <3.4.
Short-term, high-dose statin therapy should be considered:
Rosuvastatin 40/20 mg or atorvastatin 80 mg or simvastatin 80 mg.
Consensus document from the EuroCTO Club: Eurointervention May 2012
CONCLUSION
In patients with normal e GFR keep dye load to less than 400 ml; however, up to 500-600 ml can be tolerated
Consensus document from the EuroCTO Club: Eurointervention May 2012
In CTO procedures use of retrogradely positioned wires as markers (rather than using contrast injections) and IVUS may all help to reduce dye load.





























