Embed Size (px)
Citation preview

Lymphadenopathy
Prepared By Seyran KhalatUndersupervision of Dr. Akram Atroshy

Definition
Lymphadenopathy is the abnormality in the size or character of lymph nodes whether as a result of normal reactive process or pathology.


Relevant anatomy
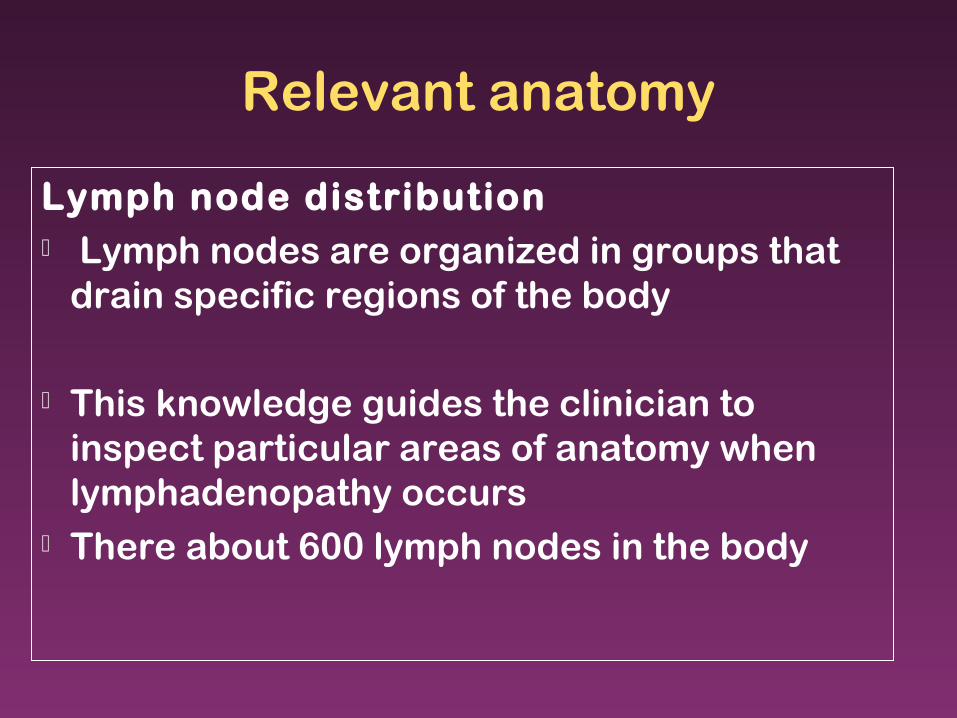
Lymph node distribution Lymph nodes are organized in groups that
drain specific regions of the body
This knowledge guides the clinician to inspect particular areas of anatomy when lymphadenopathy occurs
There about 600 lymph nodes in the body

Occipital LN, drain the back of the scalp. Retroauricular LN drain the scalp above he
auricle & from post. Wall of the ext. auditory meatus.
Parotid LN drain the scalp above the parotid and ant. Wall of ext. auditory meatus & the eyelids.
Submandibular LN drain front the scalp, the nose & adjacent cheek, the upper & lower lips (except the central parts), the frontal , maxillary, & ethmoid air sinuses, the upper & lower teeth,the ant. 2/3rd of the tongue& the floor of mouth and the gums
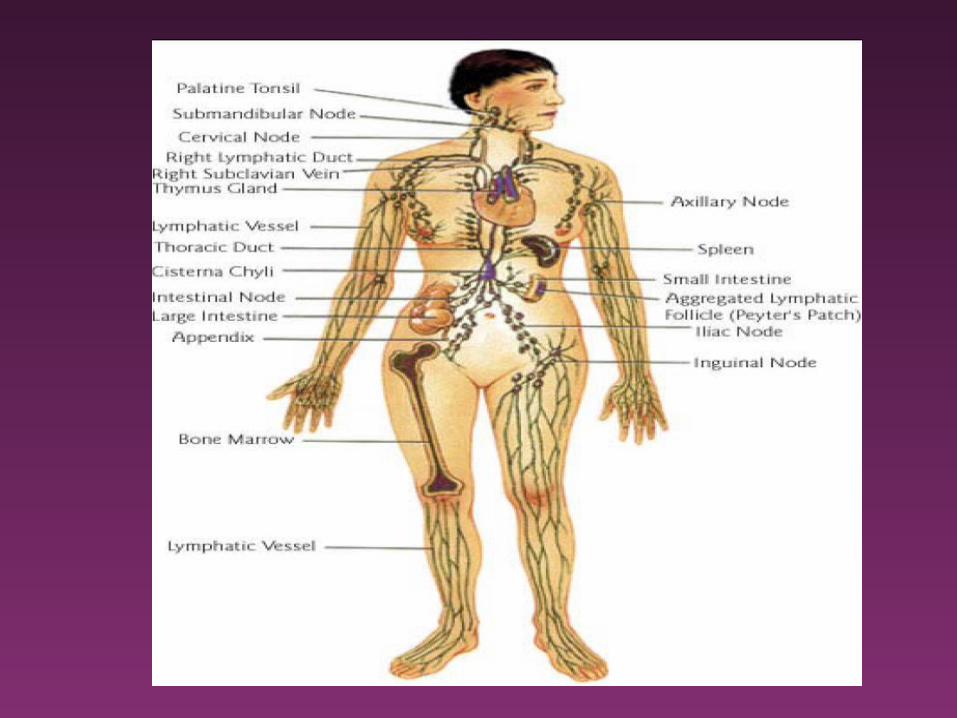
Head & Neck

Head & Neck
Submental LN receive lymph from the tip of the tongue, the floor of the mouth beneath the tip of the tongue, the incisor teeth & associated gums, the center part of the lower lip and the skin over the chin.
Anterior cervical LN receive lymph from the skin over and superficial tissues of the front of the neck.

Head & Neck
Superficial cervical LN receive lymph from the skin over the angle of jaw, and lobe of ear.
Retropharyngeal LNs receive lymph from the nasal part of the pharynx, auditory tube and the upper part of the cervical vertebral column.


Head & Neck Laryngeal LNs are situated in front of
the larynx on the cricothyroid ligament Tracheal LNs receive lymph from
neighboring structures including the thyroid gland.
Deep cervical LNs, most lie on the anterolateral aspect of the internal jugular vein.

The Thorax
Each major bronchi division has a collection of nodes called the intrapulmonary lymph nodes, which drain into a set of nodes, the left and right bronchopulmonary (hilar) lymph nodes
These nodes collect the lymphatic drainage from the segments of their respective lung

The Thorax
The posterior thoracic cavity is drained into the posterior mediastinal lymph nodes
The anterior thoracic cavity is drained through the parasternal LNs
The common drainage site for these LNs is into the jugular trunk then to the thoracic duct

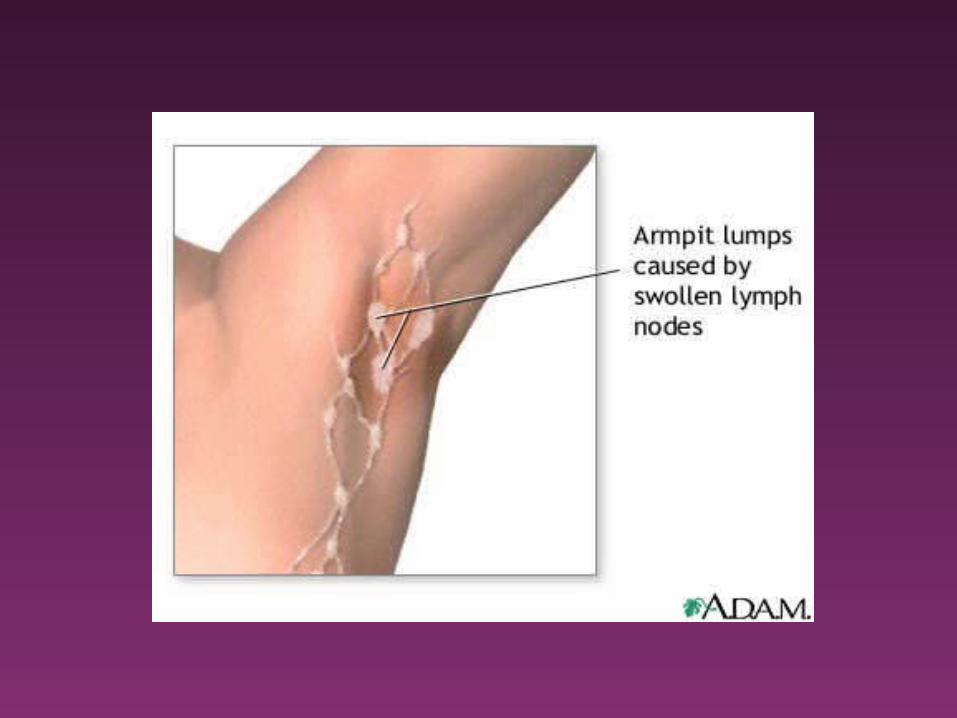
Upper limbs The upper extremity lymph node distribution
consists of the cubital fossae and axillary region
The lat. axillary group drains the upper extremity and receives lymph from the post. axillary group, which then drains the post. chest wall
The anterior axillary nodes drain lymph from the anterior chest wall.
The apical axillary nodes drain into the thoracic duct on the left or directly into the brachiocephalic vein on the right
Abdomen Lymph nodes lie in the mesentery Each artery has a cluster of nodes that
receives lymph from its corresponding arterial supply: celiac, superior, inferior mesenteric lymph nodes
The common iliac LNs drain into the Lt. and Rt. lumbar nodes, draining into the cisterna chyli.
The kidneys and adrenals drain into LNs around the renal vessels and then into the lumbar nodes.
Lower limbs The 2 groups that drain the lower limbs
are the popliteal nodes and the inguinal nodes
The inguinal nodes are grouped into external and internal subtypes.
The external group drains the anterior abdominal wall and external genitalia.
The internal inguinal nodes then drain into the external iliac nodes.

In most instances, lymph nodes up to 1 cm can still be considered normal.
The two exceptions to this rule include the epitrochlear node in which up to 0.5 cm is allowed and the inguinal nodes in which up to 1.5 cm is allowed

Pathophysiology
Most lymphadenopathy in children is due to benign self-limited disease because self-limited viral or bacterial infections are the most common causes.

PathophysiologyLymphadenopathy can be caused
by:
1. an increase in normal lymphocytes and macrophages during a response to an antigen (e.g. viral illness)
2. nodal infiltration by inflammatory cells in response to an infection in the nodes themselves (lymphadenitis)
3. proliferation of neoplastic lymphocytes or macrophages (lymphoma)
4. infiltration of nodes by metabolite-laden macrophages in storage diseases (Gaucher disease)

Outline-etiologies of lymphadenopathy
Generalized lymphadenopathy is defined as enlargement of more than 2 noncontiguous lymph node groups
Infections :1. Viral 2. Common upper respiratory infections 3. Infectious mononucleosis 4. CMV 5. Acquired immunodeficiency syndrome 6. Rubella 7. Varicella 8. Measles

Etiology
Bacterial 1. Septicemia
2. Typhoid fever
3. Tuberculosis
4. Syphilis
5. Plague
Protozoal – Toxoplasmosis>
Fungal - Coccidioidomycosis

Autoimmune disorders and hypersensitivity states
1. Juvenile rheumatoid arthritis
2. Systemic lupus erythematosus
3. Drug reactions (e.g., phenytoin, allopurinol)
4. Serum sickness
Storage Diseases 1. Gaucher disease
2. Niemann-Pick disease
Etiology
Neoplastic and proliferative disorders
1. Acute leukemias
2. Lymphomas (Hodgkin, non-Hodgkin)
3. Neuroblastoma
4. Histiocytoses II.
Regional lymphadenopathy involves enlargement of a single node or multiple contiguous nodal regions.
Cervical 1. Viral upper respiratory infection 2. Infectious mononucleosis 3. Rubella 4. Catscratch disease Streptococcal pharyngitis 5. Acute bacterial lymphadenitis 6. Toxoplasmosis 7. Tuberculosis/atypical mycobacterial infection8. Acute leukemia 9. Lymphoma 10.Neuroblastoma 11.Rhabdomyosarcoma 12.Kawasaki disease

Submaxillary and submental
1. Oral and dental infections
2. Acute lymphadenitis
Occipital
1. Pediculosis capitis
2. Tinea capitis
3. Secondary to local skin infection
4. Rubella
5. Roseola
Preauricular
1. Local skin infection
2. Chronic ophthalmic infection
3. Catscratch disease

Mediastinal 1. Acute lymphoblastic leukemia 2. Lymphoma 3. Sarcoidosis 4. Cystic fibrosis 5. Tuberculosis 6. Histoplasmosis 7. Coccidioidomycosis 8. Supraclavicular 9. Lymphoma 10.Tuberculosis 11.Histoplasmosis 12.Coccidioidomycosis

Axillary 1. Local infection
2. Catscratch disease
3. Brucellosis
4. Reactions to immunizations
5. Lymphoma
6. Juvenile rheumatoid arthritis
Abdominal
1. Acute mesenteric adenitis
2. Lymphoma

Inguinal 1. Local infection
2. Diaper dermatitis
3. Insect bites
4. Syphilis
5. Lymphogranuloma venereum

Generalized lymphadenopathy

Generalized lymphadenopathy-infection
Generalized LAP is most often associated with systemic viral infections
IMN results in widespread adenopathy Roseola infantum (caused by human herpes
virus 6), CMV, varicella, and adenovirus all cause generalized lymphadenopathy
Although usually associated with localized node enlargement, some bacterial infections cause generalized adenopathy e.g. typhoid fever caused by Salmonella typhi, syphilis, and tuberculosis

Generalized lymphadenopathy-Malignant etiologies
Malignancy often is associated with constitutional signs, such as fever, anorexia, nonspecific aches and pains, weight loss, and night sweats like in acute leukemias and lymphomas.
Generalized LAP is present at diagnosis in 70% of children with (ALL) and in 31% of children with (AML)
The lymphomas more often present with regional lymphadenopathy, but generalized lymphadenopathy occurs

Generalized lymphadenopathy-Malignant etiologies
1/3rd of children with Hodgkin disease and 10% with non-Hodgkin lymphoma display them
Malignancies usually present with nodes that tend to be firmer and less mobile or matted; however, this finding can be misleading
Benign reactive lymph nodes may be associated with fibrotic reactions that make them firm

Generalized lymphadenopathy-Storage disease
In Niemann-Pick disease, sphingomyelin and other lipids accumulate in the spleen, liver, lymph nodes, and central nervous system
In Gaucher disease, the accumulation of the glucosylceramide leads to the engorgement of the spleen, lymph nodes, and the bone marrow.

Generalized lymphadenopathy-Drug reaction
Within a couple of weeks of initiating phenytoin, some patients experience regional or generalized LN enlargement, followed by a severe maculopapular rash, fever, hepatosplenomegaly, jaundice, and anemia
Several other drugs cause similar symptoms, including, pyrimethamine, phenylbutazone, allopurinol, and isoniazid

Generalized lymphadenopathy-Other non-neoplastic etiologies
Rare non-neoplastic causes of generalized LAP include Langerhans cell histiocytosis.
Autoimmune causes include juvenile rheumatoid arthritis, which often presents with adenopathy, especially during the acute phases of the disease
Sarcoidosis and graft verses host disease also can cause LAP

Localized Lymphadenopathy

Cervical Lymphadenopathy
Adenopathy is most common in cervical nodes in children and usually is related to infectious etiologies
LAP posterior to the SCM typically is a more ominous finding, with a higher risk of serious underlying disease

Infectious causes
IMN often manifests with posterior and anterior cervical adenopathy
Firm tender nodes that are not warm or erythematous characterize this lymph node enlargement.
Other viral causes of cervical LAP include adenovirus, herpes virus, Coxsackie virus, and CMV
In herpes gingivostomatitis, impressive submandibular and submental adenopathy reflects the amount of oral involvement

Infectious causes
Bacterial infections cause cervical adenopathy by causing the draining nodes to respond to local infection or by the infection localizing within the node itself as a lymphadenitis
Localized cervical lymphadenitis typically begins as enlarged, tender, and then fluctuant nodes.

Infectious causes
In patients with cervical adenopathy, determine whether the patient has had recent or ongoing sore throat or ear pain
Examine the oropharynx, paying special attention to the posterior pharynx and the dentition
Atypical mycobacteria cause subacute cervical lymphadenitis with nodes that are large and indurated but not tender

Infectious causes TB presents with a suppurative LN identical to
that of atypical mycobacterium. Catscratch disease, caused by Bartonella
henselae, presents with subacute LAP often in the cervical region
The disease develops after the infected pet (most likely a kitten) inoculates the host, usually through a scratch
Approximately 30 days later, fever, headache, and malaise develop, along with adenopathy that often is tender
Non-infectious causes Malignant childhood tumors develop in the head
and neck region in 27% of cases. In the first 6 years of life, neuroblastoma,
leukemia, non-Hodgkin lymphoma, and rhabdomyosarcoma (in order of decreasing frequency) are most common in the head and neck region
In children older than 6 years, Hodgkin disease and non-Hodgkin lymphoma both predominate
Children with Hodgkin disease present with cervical adenopathy in 80-90% of cases as opposed to 40% of those with non-Hodgkin lymphoma

Infectious causes
Kawasaki disease is an important cause of cervical adenopathy. These children have fever for at least 5 days, and cervical lymphadenopathy is one of the 5 diagnostic criteria (of which 4 are necessary to establish the diagnosis).

Submaxillary and submental lymphadenopathy
These nodes drain the teeth, tongue, gums, and buccal mucosa. Their enlargement usually is the result of localized infection, such as pharyngitis, herpetic gingivostomatitis, and dental abscess.

Occipital lymphadenopathy
Occipital nodes drain the posterior scalp. These nodes are palpable in 5% of healthy children. Common etiologies of occipital lymphadenopathy include tinea capitis, seborrheic dermatitis, insect bites, orbital cellulitis, and pediculosis.
Viral etiologies include rubella and roseola infantum.
Periauricular adenopathy
Preauricular nodes drain the conjunctivae, skin of the cheek, eyelids, and temporal region of the scalp and rarely are palpable in healthy children.
Mediastinal lymphadenopathy
Because these nodes are not directly demonstrable on physical examination, their enlargement must be assessed indirectly
Mediastinal nodes may cause cough, wheezing, dysphagia, airway erosion with hemoptysis, atelectasis, and the obstruction of the great vessels, which constitutes superior vena cava syndrome with mediastinal adenopathy,airway compromise may be life threatening

Mediastinal lymphadenopathy
Mediastinal LAP is usually a sign of serious underlying disease
More than 95% of mediastinal masses are caused by tumors or cysts
Lymphomas and ALL are the most common etiologies and usually involve the anterior mediastinum
Unlike most other adenopathies, mediastinal lymphadenopathy less frequently is a result of infection
Mediastinal lymphadenopathy
Nonlymphoid mediastinal tumors may be confused with adenopathy. These include neurogenic tumors (usually found in the posterior mediastinum), germ cell tumors, and teratomas
Nonneoplastic conditions also may be confused with mediastinal adenopathy. These include the typically large thymus of a child, substernal thyroid glands, bronchogenic cysts, and abnormalities of the great vessels

Supraclavicular lymphadenopathy Left supraclavicular nodes reflect intra-
abdominal drainage and enlarge in response to malignancies in that region
This is particularly true when adenopathy in this region occurs in the absence of other cervical adenopathy.
Right supraclavicular nodes drain the lung and mediastinum and are typically enlarged with intrathoracic lesions
Early lymph node biopsy should be considered in children with supraclavicular adenopathy

Axillary lymphadenopathy
A common cause of axillary lymphadenopathy is catscratch disease
Local axillary skin infection and irritation commonly are associated with local adenopathy
Other etiologies include recent immunizations in the arm (particularly with BCG vaccine), brucellosis, juvenile rheumatoid arthritis, and non-Hodgkin lymphoma.
Abdominal lymphadenopathy Although abdominal adenopathy is not usually
demonstrable on physical examination, abdominal pain, backache, increased urinary frequency, constipation, and intestinal obstruction secondary to intussusception are possible presentations.
Mesenteric adenitis is thought to be viral in etiology and is characterized by right lower quadrant abdominal pain caused by nodal enlargement near the ileocecal valve.
Abdominal lymphadenopathy
Mesenteric adenopathy may be caused by non-Hodgkin lymphoma or Hodgkin disease.
Typhoid fever and ulcerative colitis are other etiologies of mesenteric adenopathy
Il iac & inguinal lymphadenopathy
They are typically palpable in healthy children, although usually no larger than 1-1.5 cm in diameter
Regional lymphadenopathy typically is caused by infection; however, insect bites and diaper dermatitis also are frequent
Nonlymphoid masses that may be confused with adenopathy include hernias, ectopic testes, and lipomas

Management Starting with the History
1. Age of the child: Neonates: need investigations because LN are
not palpable during neonatal period, but with time during childhood period there is antigenic exposure so some LN may palpable in the body like cervical up to 2 cm , axillary 1 cm, inguinal 1.5 cm but if more than these measures LNs are considered enlarged
The peak prevalence of leukemia is in children younger than 10 years, whereas Hodgkin disease is observed more often in adolescents.

2.Duration: If it is of short duration (less than 2 weeks)
infection is suspected. If it is of long duration ( more than 2 weeks but
less than 1 year) there is possibility of malignant etiology.
If more than one year other pathologies should be thought of like connective tissue disease

3.Associated symptoms Also may be helpful to reach the underlying
pathology like: Pain & sore throat Wt loss more than 10% over 6 months Night sweating Pruritus Myalgia, arthralgia Skin rash, bruising, Malaise Constipation or diarrhea Headache, abdominal pain Conjunctivits

4. Animal contact
5. Traveling history
6. History of recent immunization
7. Family history
8. Drug history.

Physical examinationNode themselves
1.Location: Generalized or localized
2.Characters of LNs: Hard, firm, painless, fixed, circumscribed,
suspect malignancy Mobile, non tender, clearly demarcated
suspect viral infection Matted suspect TB
3. Other signs: signs of anemia like tachycardia, pale
conjunctiva, may be associated with malignancy or autoimmune disease
Jaundice Dermatological changes. Petechiae, bruising,
bleeding may be associated with malignancy Wt and growth- poor growth may be
associated with malignancy Presence of hepatospleenomegaly

WorkupLab Studies: The following studies typically
are included:
1. CBC, ESR is nonspecific but may be helpful.
2. LFT & RFT and a urine analysis are useful to identify underlying systemic disorders that may be associated with lymphadenopathy
3. Skin testing for tuberculosis is usually indicated.
4. In specific regional adenopathy, lymph node aspirate for culture may be important if lymphadenitis is suspected clinically
5. Serology for HIV, CMV, EBV

Workup
Imaging Studies: Chest radiography is usually the primary
screening imaging study Chest X ray is often helpful in elucidating
mediastinal adenopathy and underlying diseases affecting the lungs
Supraclavicular adenopathy may be an indication for other studies, including CT of the chest and/or abdomen
Ultrasonography for extent of LAP

Biopsy: avoid sampling of inguinal LNs because are
frequently destroyed by chronic Inflammatory Processes.
if after biopsy the Dx is not reached then another biopsy is indicated if symptoms persist or worse.
histological studies of LNs can exclude malignancy, granulomatous disease, storage disease, even can Dx some infections.
Indications of biopsy
1. Failure to reach diagnosis by non invasive investigation
2. if there is persistent or unexplained fever, weight loss, night sweats, hard nodes, or fixation of the nodes to surrounding tissues.
3. If there is supraclavicular L .N
4. If there is continuous enlargement over 2 weeks
5. no decrease in size in 4–6 wk
6. no regression to "normal" in 8–12 wk
7. development of new signs and symptoms.
8. no respond to antibiotics

TreatmentMedical Care: Treatment is determined by the specific
underlying etiology of lymphadenopathy Most clinicians treat children with cervical
lymphadenopathy conservatively Antibiotics should be given only if a
bacterial infection is suspected If the clinical picture exist suggest
malignancy, such as persistent fevers, weight loss, or more impressive adenopathy with weight loss, biopsy should be pursued sooner

Treatment
Surgical Care Surgical care usually involves a biopsy. If
lymphadenitis is present, aspirate may be needed for culture, and removal of the affected node may be indicated.
Drainage is required if an abscess formed
Complications
Mediastinal adenopathy can cause superior vena cava syndrome with obstruction of blood flow; bronchial or tracheal obstruction with cough, wheezing, and ultimately respiratory tract obstruction (which can be life threatening); and dysphagia from esophageal compression. Occasionally, erosion of a node into a bronchus or trachea can result in hemoptysis
Complications
When the diagnosis of an underlying malignancy is missed, serious metabolic complications can occur. These include uric acid nephropathy, hyperkalemia, hypercalcemia, hypocalcemia, hyperphosphatemia, and acid renal failure.
Abdominal adenopathy can cause abdominal or back pain, constipation, and urinary frequency. Intestinal obstruction caused by intussusception can be life threatening

Prognosis
The prognosis of lymphadenopathy is almost entirely dependent on the underlying etiology. Patients with specific complications, such as superior vena cava syndrome, are at risk unless this specific complication is managed. Their prognosis is dependent on the management of the neoplastic process resulting in superior vena cava syndrome.

Thank you