Embed Size (px)
Citation preview
Perceptions, Problems, and Solutions
By Michelle Christensen
Pain Management
Objectives The post-surgical nursing staff will be able to analyze
how complementary pain management measures for post-surgical patients could be used in conjunction with pharmaceutical measures to manage pain on the unit.
The post-surgical nursing staff will be able to compare and contrast three current (with in the last five years) evidence based best practices for complementary pain management measures for post-surgical patients.
The post-surgical nursing staff will be able to compare and contrast current measures being used on unit to deter opiate abuse with current (within the past five year) evidence based best practices.
Perceptions Pain is a unique disliked experience and is perceived by
each patient in a different way.
What effects perceptions of pain?
As T. Jackson Et AL, states “ the interpersonal context of taking medication, expectations, or other verbal and nonverbal factors” can all play an important role in how the patient perceives their pain and relief of pain.
One study showed that the environment, healthcare professionals presence, and medical equipment played a role in how a patient perceived pain. This study goes on to discuss the use of pharmaceuticals in patients expectations for pain relief. In the study patients are given a strong pain reliever there after they are given a placebo to reduce their pain. In the study it was found that patients expected the medication to work as it did initially and thus it did and the placebo reduced the patients pain just as the initial dose did.
What does this mean?
Evidence suggests that during the initial pain
assessment it is important to determine what the
patients expectations for pain relief are. This
would include inquiring about;
What the patient would do to relieve pain at
home, what percent of pain relief the patient
expects to experience, and what measures the
patient expects to receive to reduce their pain.
Two proven pain relieving interventions include
pharmaceutical measures as discussed and
complementary therapies.
Complementary therapies
aka CAM therapiesBackground
Complementary therapies are “health care approaches with a history of use or origins outside of mainstream medicine.”
In the United States complementary therapies are often used in addition to conventional medical treatment, but can also be used alone.
There have been a reported 1800 CAM therapies! This makes it vital for healthcare professionals to have a basic understanding of what CAM therapies are.
Opioids or pharmaceutical measures should be used when non opioid therapy is not effective alone.
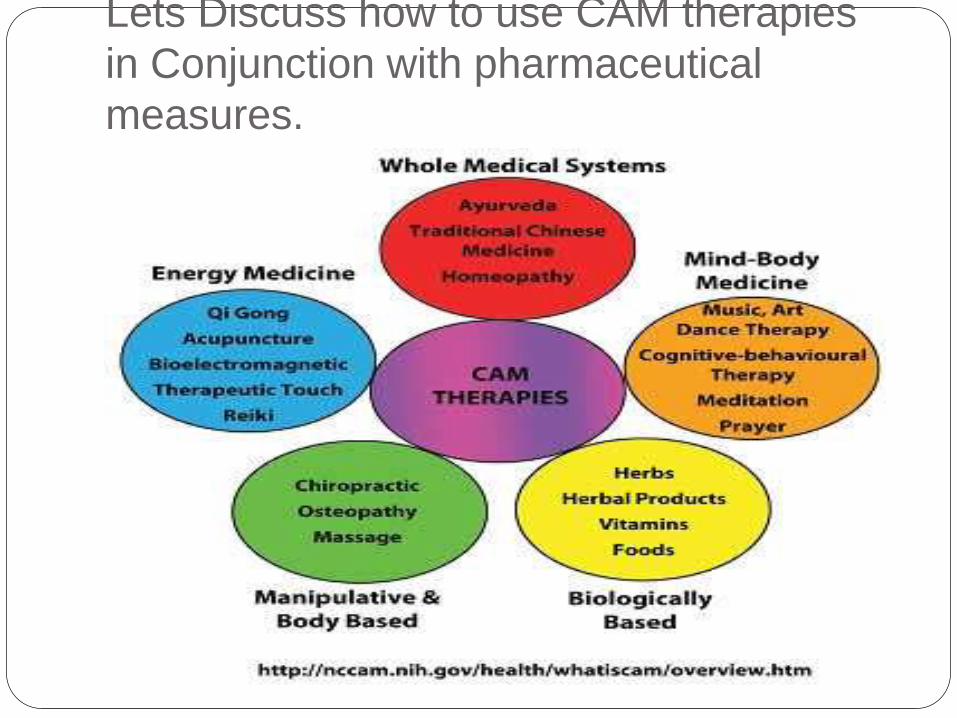
Categories of CAM therapies Whole medical systems- Some practices do not fit
into other categories and would include things such
as homeopathy and naturopathy which take a more
holistic approach to care.
Mind-body medicine- These are the most widely used
CAM therapies today. They use the mind to effects
the bodies function.
Biologically based practices-substances generally
found in nature such as herbs.
Manipulative and body-based practices- Apply
Pressure to manipulate or move one or more body
parts.
Energy medicine-These therapies use
electromagnetic fields or biofield energies thought to
originate from the body.
Risks
Kramlich confirms these therapies do not come with out risk.
“Concerns with some of the energy therapies include inaccurate
diagnoses of conditions by practitioners and safety issues
associated with the manipulative therapies
Biologics-Such products may be disruptive to normal
physiological processes, such as coagulation and glucose
regulation, and interactions with conventional medications may
produce devastating effects.
Some concerns about manipulative therapies include delay or
avoidance in seeking conventional care and aggravation of
existing conditions
What are They?Within these categories there are different therapies that
can be utilized such as;
Aromatherapy
Acupuncture
Herbal medicine
Massage therapy
Visualization (guided Imagery)
Yoga
Music therapy
Reflexology
Spinal manipulation
Some misconceptions
Many people believe that complementary
therapies are a joke and that people don’t want to
use them.>>>>This is not true in fact according to
the National institutes of health 40% of adults and
12% of adolescents reported using CAM
therapies. For a reported spending of 34 billion
dollars!
All CAM therapies are all safe and anyone can
use them because they aren’t medical
treatments. False there are several CAM
therapies that require a licensed professional to
perform them, for example chiropractic services.
Benefits of Using Cam Therapy
Although there are risks involved with CAM
therapy careful considerations and accurate
patient history can eliminate many of these risks.
One benefit of CAM therapies for your unit is the
evidence that CAM therapies can reduce pain
perceptions and or eliminate pain.
Lets Discuss how to use CAM therapies
in Conjunction with pharmaceutical
measures.
Potential Problems with Pain
management
It’s no secret that opiate abuse is a serious and
potential risk when treating patients for acute and
chronic pain.
Opiate abuse is on the rise and according to the
Centers for disease control they have“ identified
prescription drug abuse and overdose as one of the
top five health threats for 2014”.
Opiate addictions are becoming one of the top leading
reasons that many people are seeking drug
rehabilitation.
The institute for clinical systems improvement
performed a retrospective cohort study showing that
patients who received a prescription for opioids within
seven days of surgery were 44% more likely to result
in long term opioid use within one year.
Minnesota DHS I would now like to discuss a video I watched
produced by the Minnesota Department of Health
about opiate addiction called Heroin at home.
What does the Heroin Epidemic have to do with
the Opiate epidemic?
https://www.youtube.com/watch?v=nXAu_pWg0s
s
According to the Minnesota Department of Health
the united states has 5% of worlds population but
consumes 80% of the worlds opiates.
Signs of an addiction Larger than expected amounts of opiates to control
pain.
Patient may report allergies or unwanted side effects
to many other opiates in order to gain access to the
desired drug of choice. For example a patient may
report GI upset with oral oxycodone, but reports that
they do not have the same issue with IV dilaudid.
Patient requests specific pain medications possibly
stating that others do not work for them.
Symptoms of withdrawal when opiates are not given
may arise. Such as; Low energy, irritability, yawning,
teary eyes, muscle aches/pains, hot and cold sweats,
abdominal pains, and or N/V.
DSM-V substance use disorder
Criteria
The drug is taken in larger amounts and over longer periods of time than intended
There is a persistent desire or unsuccessful attempts to cut down or control use
A great deal of time is spent in activities to obtain, use or recover from the effects.
Craving or a strong desire for the substance
Tolerance: a need for increased amounts to achieve the desired effects
Withdrawal: A syndrome developing after cessation characteristic to the specific substance.
Solutions
what can we do?
Assessing a patients opiate exposure can aide in determining a patients risk for opiate abuse. As it has been shown that those exposed to opiates more so then those not have a higher risk for developing abuse. Also if a patient has history of street drug use they are more likely of opiate addiction. Overall an in depth risk assessment prior to opioid administration is beneficial in the reduction of opioid abuse.
Use clinical judgment and effective communication with your healthcare team to determine whether a patient truly needs opioid therapy and if so how much is needed. Implementation of an algorithm to aide in opiate administration could also be beneficial.
Solution cont… Let your postoperative patients know in advance there
is and endpoint to their surgical pain.
Explain the risks of opiate use and encourage the patient to be involved with their care.
Encourage prescribing providers to check the prescription monitoring website prior to administration to determine current narcotic prescriptions with in the last year.
Remind your patients to discard any unused pain medication and to not save for future pains as this is considered drug abuse.
The FDA is also currently working on an opioid abuse deterrent pain medication that if made could help control pain while reducing the risk for opioid addiction!
Case Study Your patient rates there a pain at a 2 on a 0-10 scale where 0
is no pain and 10 is the worst pain. The patient has had a
total knee replacement and is post op day 3. This rating is
given after having an hour of physical therapy. The patient
describes the pain as dull and aching and states it gets
worse with exercise and activity. Which would be the most
appropriate action.
A. Do nothing the pain rating is not high enough
B. Give the patient 10mg of Oxycodone P.O as ordered
C. Give the patient Tylenol 650mg P.O as ordered and assist the
patient with guided imagery.
D. Give the patient 5mg of Oxycodone P.O as ordered and assist
the patient with guided imagery.
Case StudyYou are the primary RN for a patient who has been admitted with
severe abdominal pain. X rays, ultrasounds, and other diagnostic studies are finding no cause for the pain. You have been given orders for 5 to 10mg of oxycodone q4hours P.O as needed. The patient has taken 10mg of oxycodone and is still rating their pain at a 10 on a 0-10 scale with 10 being the worst possible. You request an order for IV dilaudid .5mg to 1mg q 1-2 hours as needed. After receiving the order you give the patient .5mg of dilaudid. The patient continues to rate pain at a 10 despite IV medication. You administer the other .5mg of Dilaudid IV and the patient rates pain has decreased and is now rating pain at a 9. You have also tried several other complementary therapies such as guided imagery, music therapy, and aromatherapy with no results. Despite best efforts the patient continues to call every 10 to 15 minutes about pain. You notify the provider that you are concerned about your patient as nothing is helping. The provider decides to do exploratory studies and again finds nothing. You begin to wonder if the patient has a history of opioid abuse and share this with the provider they are suspecting the same thing. What would be the best way to gather further information to determine the patients history with narcotic pain medications?
Case Study cont…. A. Next time the patient calls for pain medication notify them that
you are concerned that they have been taking way to many pain
meds and this is a classic sign of opioid abuse, also letting them
know that they need to tell you the truth.
After administering the patients pain medication you begin
talking with them about them about the current epidemic with
pain medications telling them how much you are disgusted with it
and then ask them if they have ever had any issues with opioid
abuse.
You enter the patients room letting them know that you are
concerned about there increasing needs for increased dosing of
narcotic pain medications. In a matter of fact approach you let
them know that you are concerned there might be an issue with
opioid abuse.
Case study This same patient tells you that they do have a problem with
opioid abuse and have had an addiction to narcotics for 5
years now. They state they heard about tolerance with the
drugs after using for a period of time, but that their pain is
real. They state that they generally take 50mg of oxycodone
a day recreationally. What is your response to this situation
A. Let the patient know that tolerance is very likely and that you
believe their pain is real. While letting them know you will have to
notify the provider in order to determine a more effective
approach to their treatment.
B. Let the patient know that because they have an addiction to
pain medication you can not give them narcotics any longer
despite their complaints of pain.
Leave the patients room immediately and notify the provider.
Questions???
References
Acute Pain Assessment and Opioid Prescribing Protocol. (2014). Quality Improvement Support, 1-44.
Cobaugh, D., Gainor, C., Gaston, C., Kwong, T., Magnani, B., Painter, J., & Krenzelok, E. (2014). The opioid abuse and misuse epidemic: Implications for pharmacists in hospitals and health systems. Am J Health-Syst Pharm, 71, 1539-1551.
General Internal Medicine in Minnesota. (2015, January 1). Retrieved April 12, 2015, from http://www.mayoclinic.org/departments-centers/general-internal-medicine/minnesota/overview/specialty-groups/complementary-integrative-medicine
Jackson, T., Iezzi, T., Nagasaka, T., Fritch, A., & Gunderson, J. (2002). Does the mere presence of over-the-counter pain medication affect pain perception? Some preliminary findings. Psychology, Health & Medicine, 215-222.
Kramlich, D. (2014). Introduction to Complementary, Alternative, and Traditional Therapies. Critical Care Nurse, 34(6), 50-56.
https://www.youtube.com/watch?v=nXAu_pWg0ss