Embed Size (px)
DESCRIPTION
Madhya Pradesh State Journal Indian Society Of Anaesthesiologists first issue
Citation preview

CME & WORKSHOP - 2009
1
CONTENTS
Dr. S.S.C. Chakra Rao- President (ISA-National)
Message
21
2013-2014
OFFICE BEARERS
(M.P.State Branch ISA)
PRESIDENT
Dr. Dilip Kothari
VICE PRESIDENT
Dr. Urmila Kesari
Hon. Secretary
Dr. Meenu Chadha
Treasurer
Dr. Sonal Nivsarkar
Executive Members
Dr. Alok Pratap Singh
Dr. Amit Jain
Dr. Mayank Kulshreshta
Dr. Babbar
Dr. Mukesh Nigam
Dr. Ram Avtar Singh
Editor
Dr. Meenu Chadha
Dr. M.V. Bhimeswar Hon. Secretary (ISA-National)
Dr. S. Bala Bhaskar - Editor (IJA)
Dr. Dilip Kothari - President (M.P.Chapter)
Dr. Meenu Chadha - Hon. Secretary (M.P. Chapter)
Message
Message
President's Message
Editorial
3
4
5
6
2
3
4
5
Dr. Dilip Kothari, Dr. Bhanu Choudhary
Spinal Anaesthesa: A safe option in MultipleDisease Patients
76
Dr. Sarika Katiyar, Dr. Saifullah Tipu, Dr. Rajnish kumar Jain
Anesthetic Management of a patient with Becker's Muscular Dystrophy for ASD Closure
117
Dr. Jitendra Agarwal, Dr. Dilip Kothari, Dr. Bhanu Choudhary
Postoperative Nausea and Vomiting
148
Dr. Hiren Shah, Dr. Harsha Desai Phulambrikar
Malignant PDPH- A Case Report
229
Dr. Ritesh Dixit
Anesthesia Information Management System (AIMS) Historical Overview and Future Trends
2510

2 3
Message
Dear Dr. Meenu Chadha
Namaste
I am very happy to know that ISA MP state has an idea to start their own Journal of Anaesthesiology from Indore. Indore has the experience of having a Journal for the city branch itself. Now the state branch has been privileged to start the Journal of Anaesthesiology. I learned that this Journal will help all the practising Anaesthesiologists, academicians, Corporate Institutions and the PG students for publishing their case reports and project themselves. Review articles of interest, quiz, crossword puzzles related to Anaesthesiology can be added. I suggest the ISA MP state branch to have it
thonline also so that it will be visible to the world, with increasing readership. 9 November 2014 will be a good start for this venture during the MPISACON 2014 at Gwalior. All the experience and dedication of Dr.Meenu Chadha and Dr. Dilip Kothari will definitely help the Journal to be more popular. I wish this journal of Anaesthesiology of MP state will be a grand success and many will follow.
LONG LIVE ISA
With warm regards,
Yours sincerely,
n Dr. S.S.C. Chakra Rao
Dear Dr. Meenu Chadha
I am very happy to hear that the Madhya Pardesh Society of Anaesthesiologists is starting the Madhya Pradesh Journal of Ananesthesia.
Madhya Pradesh has always been in the fore front with regards to academics, and bringing out the Madhya Pradesh Journal will be another feather in the cap of the ISA Madhya Pradesh.
The Madhya Pradesh Journal by publishing quality articles will benefit many of the PG Students, Private practitioners and Academicians.
I sincerely appreciate te efforts of the Madhya Pradesh Hon. Secretary Dr. Meenu Chadda and the Governing Council of ISA Madhya Pradesh and wish the Madhya Pradesh Journal of Anaesthesia all success.
LONG LIVE ISA
n Dr. M.V. Bhimeswar
DR. S.S.C. Chakra RaoPresident
(ISA -National)
DR. M.V. BhimeswarHony. Secretary(ISA -National)
Message
OF AL NA AN ER SU T
O H
J E
SET IOA LT OS GP Y. M

4
CME & WORKSHOP - 2009
5
Message
Dear Dr. Dilip Kothari & Dr. Meenu Chadha
It was pleasant to note that the Indian Society of Anaesthesiologists (ISA), Madhya Pradesh Branch is launching its own academic journal.
Any development contributing to growth and dissemination of research is incomplete without its actual publication. Explosive improvements in the field of anaesthesia and critical care in the last few decades have been marked simultaneously by landmark publications; and the benefits are seen worldwide, among the practicing anaesthesiologists and of course, the millions of patients.
Publications by dozens have been sprouting in the Indian scenario recently but it is imperative that for a journal to acquire popularity the editorial group maintains highest standards of publication and strive to reach greater heights. Launch of a new journal of anaesthesia by the ISA, MP State Branch is a step in the right direction, that is expected to meet the demands for publication from within the anaesthesia fraternity in M.P. The publications should reflect the sincere desire of our members to share the research evidences and not just as a cursory submission for career enhancement.
As editor of the Indian Journal of Anaesthesia, I would always be ready to submit suggestions and inputs to improve the editorial and publishing processes, standards of publication and the visibility of the journal.
I wish the journal a successful launch and also congratulate the office bearers of ISA, Madhya Pradesh, the Editor and the Editorial Board members of the journal for their decision to have an academic mouthpiece to ISA, MP state.
Long Live ISA!
n Dr. S Bala Bhaskar
It gives me immense pleasure in writing this message for the inaugural issue of a new journal entitled” M.P.State Journal of Anaesthesia” published by M.P.Chapter of Indian Society of Anaesthesiologists. I take this opportunity to congratulate Dr. Meenu Chadha Hon Secretary, M.P.Chapter of Indian Society Of Anesthesiologists for her solo efforts in presenting the first issue of the journal.
I hope that this journal will provide a platform to promote research through an intellectual exchange of ideas between the students, researchers and academicians, and would go far beyond its regional and national boundaries for dissemination of original and high quality research in the field of Anaesthesiology, Pain and Critical Care.
n Dr. Dilip Kothari
DR. S. Bala BhaskarEditor-
Indian Journal of Anaesthesia
DR. Dilip KothariPresident
(M.P. Chapter-ISA)
Message President's Message

6
CME & WORKSHOP - 2009
7
SPINAL ANAESTHESA: A SAFE OPTION IN MULTIPLE DISEASE PATIENTS
l 1 2Dr. Dilip Kothari Dr. Bhanu Choudhary
1. MD Associate professor, Dep. of Anaesthesiology G.R. Medical College, Gwalior, M.P
2. MD Associate professor, Dep. of Anaesthesiology G.R. Medical College, Gwalior, M.P
ABSTRACT
Anesthetic management of geriatric patients with multiple diseases like Hypertension, Coronary artery disease, Diabetes Mellitus, Hypothyroidism and so many other is often difficult for surgical procedures especially in emergency situations due to various anatomical, patho-physiological / biochemical changes along with polypharmacy . Spinal anesthesia is a safe option in these patients due to simplicity, reliability, cost effectiveness, minimal peri-operative biochemical changes, stress induced hemodynamic changes, rapid recovery, better cognit ive funct ion, oxygenation, superior analgesia and minimal nausea & vomiting in post operative period.
INTRODUCTION
The worldwide prevalence of Hypertension, Coronary artery disease, Diabetes mellitus are common due to various etiological factors like obesity, physical inactivity and
1-3 dietary habits. Subclinical hypothyroidism is more c o m m o n t h a n o v e r t hypothyroidism, and i ts prevalence ranges from 1 to
410%. Parkinsonism is another commonly found disease in
5elderly patients worldwide. Anesthesiologist often finds
difficulty in the anesthetic management of such geriatric patients with multiple diseases for surgical procedures especially in emergency situations due to various anatomical, patho-physiological /biochemical changes and polypharmacy .
CASE
A 75 year old, male patient (82 kgs) with obstructed right sided inguinal hernia was admitted for hernioplasty in a nursing home. The patient was suffering from multiple diseases like DM II (10 years), Hypertension, Coronary artery disease (5 years), Hypothyroidism (5 years), Parkinson disease (3 years),Chronic renal failure/Diabetic Nephropathy (3 Years), Gout (2 years) with Benign Prostatic enlargement (2 Years). For these diseases he was taking different drugs.
Table A.1: List of Medication.
Tab Amlodepin 5 mg OD (Anti hypertensive)
Tab Telmisartan 20 mg OD (Anti hypertensive)
Tab. Clopidogrel 75 mg OD (Anti platelet aggregation)
Tab Aspirin 75mg OD (Anti platelet aggregation)
Tab Carvedilol 6.25 mg OD (â1, â2 and á1 receptor antagonist)
Tab Vildagliptin 50 mgOD (Oral antidiabetic )
Tab Metformin 500 mgOD (Oral antidiabetic )
Tab Voglibose 0.3 mgOD (Oral antidiabetic )
Tab Thyroxine 100 mg OD (Thyroid hormone)
Tab Trihexyphenidyl 2 mg BD (Antiparkinson drug)
Tab Torasemide 10 OD (Diuretic)
Tab Tamsulosin 0.4 mg OD (á1 receptor antagonist)
Inj Human Actrapid 12.12,10 units SC ( Soluble Insulin)
Wish you all a very Happy 2015.
The best way to gain knowledge is to share it.
Bringing out a journal for our own state Madhya Pradesh has been a thought that has been in our minds since a long time. This Journal would give a platform our post graduates & Consultant Anesthetists to publish their work. In the long run we would try to get the Journal registered & indexed if possible. The contents of the Journal would also be posted on the M.P. State web site www.mpisa.in.
Suggestions regarding future publications are invited during the thGeneral Body Meeting at Gwalior on 9 November 2014.
“A good teacher can inspire hope, ignite the imagination & instill a love of
learning.''
n Dr. Meenu Chadha
DR. Meenu ChadhaHon. Secretary & Editor
M.P. Chapter ISA
Message

8
CME & WORKSHOP - 2009
9
halothane and neuroleptics, post operative shivering, nausea, vomiting and poor reflexes
20can worsen the situation further.
In view of above facts and the possibility of drug interactions with anesthetic drugs due to polypharmacy we decided to manage this case under spinal anesthesia which is well known for its simplicity, reliability, cost effectiveness, minimal peri-operative biochemical, stress induced hemodynamic changes, rapid recovery, better cognitive function, oxygenation, superior analgesia and minimal nausea & vomiting in post operative
21-22 23period. Rodgers A et al in an overview found decreased risk of post operative venous thrombo-embolism, myocardial infarction, bleeding compl icat ions, pneumonia, respiratory depression, and renal failure with neuraxial blocks. Our main concern was to prevent sudden hemodynamic changes like hypotension / hypertension, bradycardia / tachycardia and fluctuation in blood glucose levels along with rapid recovery. Since we used only 2.0 ml of bupivacaine, no serious alteration in these parameters was recorded. Intra-operative blood glucose was maintained around 150-160 mg% with non glucose containing crystalloid fluids. The post operative period was uneventful. One year back his left side hernioplasty was done under spinal anesthesia almost in similar conditions and was uneventful too. Lumbar epidural anesthesia was not considered as a patient was taking aspirin and Clopidogrel for a long time and these drugs are known to increase the bleeding time due to synergistic action.[24] The risk of hemorrhage is lowest in spinal anesthesia, due to use of fine needles(25/26 SWG), and highest in epidural catheter anesthesia, which requires larger needle
25 -26gauges(16/18SWG).
CONCLUSION
Spinal anesthesia due to its simplicity, reliability, minimal systemic/ biochemical
effects and lesser chances of drug interactions due to polypharmacy is a safe option in elderly patients with multisystem diseases in contrast to general anesthesia which could lead to high morbidity and mortality especially in places lacking such facilities. Not much literature is available on the role of spinal anesthesia for safe anesthetic practice in patients with multisystem diseases, therefore multicenter randomized controlled studies could be conducted to obtain guidelines for the management of such patients.
References:1. Kearney PM, Whelton M, Reynolds K,
Munter P, Whelton PK, He J. Global burden of hypertension: an analysis of worldwide data. Lancet 2005; 365:217-23.
2. Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Bery JD, Brown TM et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation 2011;123:e18-e209.
3. Haffner MS. Relationship of Metabolic Risk F a c t o r s a n d D e v e l o p m e n t o f Cardiovascular Disease and Diabetes. Obesity 2006 ;14: 121S–127S.
4. Karmisholt J, Andersen S, Laurberg P. Variation in thyroid function tests in patients wi th stable untreated subcl in ical h y p o t h y r o i d i s m . T h y r o i d 2008;18:303–308.
5. Moghal S, Rajput AH, D'Arcy C, Rajput R. Prevalence of movement disorders in e l d e r l y c o m m u n i t y r e s i d e n t s . Neuroepidemiology 1994; 13: 175–8.
6. Malik AM, Khan A, Talpur KA, Laghari AA. Factors influencing morbidity and mortality in an elderly population undergoing inguinal hernia surgery. J Pak Med Assoc 2010;60:45–7.
7. James MFM, Dyer RA, Rayner BL. A modern look at hypertension and
(Table A.1) Patient revealed a past history of treatment for acute renal failure about 2 years back .On clinical examination patient was comfortable with mild pain in inguinal region, PR 66 / min, BP 180/104 mm of Hg, RR 22 / min, had mild anemia and edema over both legs. On admission his investigation reports revealed : Hb 10.02 gm%, TLC 11000/cu mm, DLC P 70,L25, M3 E 2, Platelet 100 000/cu mm, , RBS 197 mg%, Blood Urea 66.3 mg%, Serum Creatinine 2.34 mg%, Serum Na+ 131.5 mEq/l, Serum K+ 5.2 mEq/L, UrineSugar ++, Urine albumin ++, Serum Uric acid 9.2 mg%, Serum Protein 4.8 gm%, Serum TSH 6.107 µgm/ml ( done 6 months back)
The ECG showed ST, T changes in antero lateral leads, ECHO showed normal LV size and function.
X-ray Chest PA view showed no gross anomaly.
Since on admission pat ient was comfortable and showed no signs of strangulation of hernia, the surgery was deferred till the next day. Meanwhile Aspirin, Clopidogrel and Oral hypoglycemic drugs were stopped and the dose of insulin was increased. The patient was kept nil orally for 6 hours except for Tab Amlodepin 5 mg, Tab Telmisartan 20 mg, Tab Thyroxine 100 mcg and Tab Trihexyphenidyl 2 mg were given with 25 ml of water orally at 5AM on the day of surgery. After obtaining the detailed informed consent in operation room we again checked the FBS (190mg %), PR (90/Min), BP (170/100 mm of Hg), SpO2 (98%). After securing an intravenous line with 0.9% NaCl, under all aseptic condition the sub-arachnoid block (SAB) was performed with 0.5 % Bupivacaine 2.5 ml to obtain a sensory block up to T8. Monitoring of ECG, PR, BP, SpO2, UOP was done till the end of surgery (55 min). No e p i s o d e o f h y p o t e n s i o n , bradycardia/tachycardia (± 20% of base line) was recorded. A total of 600 ml of non glucose
containing crystalloid (NS/RL) was infused intravenously to maintain the vital signs.
DISCUSSION
Geriatric patients with multisystem disease are at increased risk due to complex patho- physiological changes along with polypharmacy especially when general anesthesia is required. A high morbidity and mortality has been reported in geriatric patients especially in emergency
6situations due to multi system disease.
Presence of hypertension increases the risk of myocardial infarction, heart failure, renal
7failure and stroke. In hypertensive patients increased hemodynamic responses during
8laryngoscopy and intubation, peri-operative hypotension and hypertension during general anesthesia have been observed by many
9investigators. These fluctuations have been associated with a 20% or more increased risk of coronary events, cerebral stroke and renal
10failure. Due to various micro vascular and macro vascular changes, diabetic patients are at increased risk of painless myocardial ischemia and infarction due to associated high
11-13 incidence of coronary artery disease, and 14 intra-operative instability. Difficult intubation,
undiagnosed reflux and delayed gastric emptying associated with diabetes can contribute to problems during general
11anesthesia.
Increased airway problems due to obstructive sleep apnea, gastrointestinal dysfunction, hypodynamic cardiovascular system, decreased neuromuscular excitability, increased response of narcotics, muscle relaxants and inhalational agents and hypothermia are the factors known to cause additional problems during general anesthesia
15-19in hypothyroid patients. Apart from various cardio-respiratory and neurological problems, potential anesthetic drug interactions are often found in patients with Parkinson disease. Drugs used in general anesthesia like fentanyl,

10
CME & WORKSHOP - 2009
11
anaesthesia. South Afr J Anaesth Analg 2011;1:168-73.
8. da Silva Neto WV, Azevedo GS, Coelho FO, Netto EM, Ladeia AM. Evaluation of hemodynamic variations duringanesthetic induction in treated hypertensive patients. Rev Bras Anestesiol 2008; 58: 330-41.
9. Balick Weber CC, Brillouet Banchereau AC, Blanchet AD, Blanchet P, Safar ME, Stephan F. General Anesthesia in Hypertensive Patients: Impact of Pulse Pressure but not Cardiac Diastolic D y s f u n c t i o n o n I n t r a o p e r a t i v e Hemodynamic Instability. J Anesthe Clinic Res 2011; 2:114.
10. Aronson S, Fonts ML. Hypertension: A new look at an old problem. Curr Opin Anesth 2006; 19:59-64.
11. Vinik AI, Maser RE, Mitchell BD, Freeman R. Diabetic autonomic neuropathy. Diabetes Care 2003; 26:1553–79.
12. Rodriguez BL, Lau N, Burchfield CM, Abbott RD, Sharp DS, Yano K, et al. Glucose intolerance and 23-year risk of coronary heart disease and total mortality. The Honolulu Heart Program. Diabetes Care. 1999; 22:1262-5.
13. Ziegler D Cardiovascular autonomic neuropathy: clinical manifestations and measurement . Diabetes Reviews 1999;7:342–57.
14. Knuttgen D, Buttner-Belz U, Gernot A, Doehn M. Unstable blood pressure during anesthesia in diabetic patients with autonomic neuropathy. Anasth Intensivther Notfallmed 1990 . 25:256–62.
15. Rajagopal RK, Abbrecht PH, Derderian SS,Pickett C, Hofeldt F, Tellis CJ,et al. Obsructive sleep apnea in hypothroisim. Ann Intern Med 1984;101:491-4.
16. Yaylali O, Kirac S, Yilmaz M, Akin F, Yuksel D, Demirkan N, et al. Does hypothyroidism a f f ec t gas t r o i n t es t i na l mo t i l i t y? Gastroenterol Res Pract. 2009;52:9802.
17. Klein I, Danzi S. Thyroid disease and the heart. Circulation 2007;116:1725-1735.
18. Kim JM, Hackman L. Anesthesia for untreated hypothyroidism: Report of three cases. Anesth Analg 1977;52:299–302.
19. Stathatos N, Wartofsky L. perioperative m a n a g e m e n t o f p a t i e n t s w i t h hypothyroidism. Endocrinol Metab Clin N Am 2003;32:503-18.
20. Nicholson G, Pereira AC, Hall GM. Parkinson's disease and anaesthesia. Br J Anaesth 2002;89:904-16
21. Handley GH, Silbert BS, Mooney PH, Schwitzer SA, Aleen NB. Combined general and epidural anaesthesia versus general anaesthesia for major abdominal surgery: post anaesthesia recovery characteristics. Reg Anesth 1997;22;:435-41.
22. McKenzie P J, Wishart HY, Dewar KMS, Gray I , Smith G. Comparison of the effects of spinal anaesthesia and general anaesthesia on postoperative oxygenation andperioperative mortality. Br J Anaesth 1980; 52: 49-53.
23. Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: Results from overview of randomised trials. BM J 2000;321:1493–7.
24. Tam NLK , Pac-Soo C, Pretorius PM. Epidural haematoma after a combined spinal–epidural anaesthetic in a patient treated with clopidogrel and dalteparin. Br J Anaesth 2006; 96: 262-5.
25. Gogarten W, Vandermeulen E, Van Aken H, Kozek S, Llau J, Samama C. Regional Anesthesia and Antithrombotic/Antiplatelet Drugs Recommendations of the European Society of Anaesthesiology. Eur J Anaesthesiol 2010;12:999–1015.
26. Vandermeulen EP, Van Aken H, Vermylen J. Anticoagulants and Spinal-Epidural Anesthesia. Anesth Analg 1994;79:1165-77.
Abstract: Becker's Muscular Dystrophy is considered to be a milder form of Duchenne's muscular dystrophy, as both are caused by mutations in the dystrophin gene and thus present with almost the same manifestations. We present the case of a patient with Becker's Muscular Dystrophy who underwent ASD (Atrial Septal Defect) closure and discuss the anaesthetic issues that are associated with such a condition.
Key Words: Becker's Muscular Dystrophy, Hyperkalemia, Rhabdomyolysis,
Case Report: A 36 kg 15 year old boy presented for surgical closure of an osteum secundum type ASD. He was being treated for hypothyroidism with 50 microgram per day of Thyroxine. At the age of 8 years he had presented with LMN weakness in the left leg and was diagnosed as a case of Becker's Muscular Dystrophy. There was no family history of congenital heart disease, early deaths or anesthesia related problems. Pulmonary Function Tests were done prior to surgery which showed moderate restrictive lung disease. He had no other co morbidity and all his preoperative investigations were n o r m a l e x c e p t C P K ( C r e a t i n i n e Phosphokinase) of 1700U/L and an ECG which showed RBBB (Right Bundle Branch Block).
The patient was premedicated with Inj. Midazolam 3 mg intravenous and anaesthesia
was induced with Inj. Morphine 10 mg intravenous and Inj. Thiopentone 200 mg intravenous. Neuromuscular blockade was achieved with 30 mg of Atracurium intravenous and trachea was intubated with an 8 mm ID endotracheal tube. Anaesthesia was maintained with Fentanyl infusion of 100 mcg/hr intravenously and Propofol infusion (15ml-35ml/hr) intravenously to keep the patient at a BIS level of less than 60. In addition, intraarterial BP (Blood Pressure), C V P ( C e n t r a l Ve n o u s P r e s s u r e ) , nasopharyngeal temperature, neuromuscular transmission and urine output monitoring was carried out during the procedure. Intra operative antibiotic was restricted to Inj. Cefuroxime 1.5 Gm IV. Amikacin was avoided. Total CPB (Cardiopulmonary Bypass) and cross clamp times were 37 min and 20 minutes respectively. During CPB care was taken to a v o i d h y p e r t h e r m i a a c i d o s i s a n d hyperkalemia. Serum potassium levels were maintained between 3.2-3.7 meq/l and hourly serum potassium levels were checked to rule out rhabdomyolysis. Urine output was adequate throughout the procedure. Patient came o f f bypass smooth ly. Drugs supplemented during and after CPB were Propofol and Morphine along with small a l i q u o t s o f A t r a c u r i u m b a s e d o n neuromuscular monitoring. In the ICU patient was extubated an hour later following spontaneous reversal of neuromuscular
ANESTHETIC MANAGEMENT OF A PATIENT WITH BECKER’S MUSCULAR
DYSTROPHY FOR ASD CLOSUREl
Dr. Sarika Katiyar, Dr. Saifullah Tipu,Dr. Rajnish Kumar Jain
1. Department of Anesthesiology and Critical care,
BMH & Research center, Bhopal

12
CME & WORKSHOP - 2009
13
blockade and kept on noninvasive ventilation for the next 3 hours. Postoperative analgesia was maintained with Fentanyl boluses of 25-50mcg intravenously. On the second postoperative day CPK levels were 2763 U/l. Patient stood the procedure well, had a trouble free recovery and was safely discharged home on the seventh postoperative day. A letter of caution was issued to the patient detailing his condition and the precautions which should be taken in case of future anaesthetics. A copy of the letter was kept in the patients hospital records and the issue highlighted on its cover for future safety.
Discussion: Becker's Muscular Dystrophy (BMD) is an X-linked recessive inherited disorder. It affects 1 in 30000 live male births. Some people with BMD's are able to walk well into adulthood. BMD therefore may not be diagnosed until after adolescence. Clinically it presents with muscle weakness, muscle deformities, psuedohypertrophy of calf muscles and unusual walking gait. A history of motor delay in the developmental milestones of children should be thoroughly investigated as part of the preoperative evaluation. A blood test may demonstrate higher than normal levels of CPK. If CPK levels are increased, elective surgery should be delayed until specific tests are carried out. There may be involvement of respiratory muscles with deterioration of respiratory function and later patient may develop kyphoscoliosis. A preoperative respiratory evaluation including pulmonary function tests would give an indication of the severity of the problem and also provide a base line for further assessments postoperatively or for later in life. R a r e l y, h e a r t p r o b l e m s , s u c h a s cardiomyopathy will occur as the disease progresses and some BMD children may develop intellectual problems or learning difficulties. DNA studies , muscle biopsy are requi red to conf i rm the d iagnosis . Many case reports with alarming cardiac
arrests in children undergoing anesthesia in 1980's were found to be related to the use of Succinylcholine or volatile anaesthetic agents
1in patients with undiagnosed myopathies. More recently, Sevofluorane has also been shown to be associated with rhabdomyolysis in
2patients with Duchenne's Muscular Dystrophy. This is due to acute rhabdomyolysis and hyperkalemia that can occur after the use of volatile anesthetics and depolarizing muscle relaxants in muscular dystrophy. On this basis some authors advocate the routine avoidance of these drugs.
The defect in dystrophies such as Becker's muscular dystrophy is in the membrane stabilizing protein Dystrophin. This protein is present in the post synaptic nicotinic receptors of muscles but its function has not been clearly delineated. Although unproven, these case reports lead to the speculation that defective Dystrophin destabilizes the cell membrane and the additive effect of another destabilizing agent, a volatile anesthetic agent or a depolarizing muscle relaxant, could predispose these pa t ien ts to mi ld to severe rhabdomyolysis leading to hyperkalemia and on rare occasions, death. Rhabdomyolysis may lead to post operative acute kidney injury which has its own morbidity and mortality. Aminoglycoside antibiotics are known to prolong the action of Non depolarizing muscle relaxants and thus we avoided their use. Short acting drugs like Fentanyl and spontaneously lysing drugs like Remifentanil, Atracurium or Mivacurium would avoid the problems of accumulation and prolonged effect in such an eventual i ty. Spontaneous reversal of neuromuscular blockade may also avoid the possibility of hyperkalemia which may be
3triggered off by reversal with neostigmine. The fact that these events occur in awake recovering children also suggests that the dose of volatile agents required may be minimal and at levels less than MAC awake for volatile agents. Alternatively, destabilization may have occurred
earlier during the anaesthetic when drug concentrations were higher. The precipitating event could be movement during recovery which may simply be the trigger. There are no known reports of any such problem with the use of intravenous anaesthetics or even local
4anaesthetic agents. Muscular dystrophies thus make a good indication for the use of TIVA(Total Intravenous Anesthesia), local, regional or neuraxial techniques.
We therefore resorted to total intravenous anesthesia (TIVA) with Propofol and Fentanyl. Ordinary syringe pumps were used for this purpose. BIS monitoring was used during the anesthetic to guide the rate of administration of Propofol.
Cardiopulmonary Bypass can also trigger 5rhabdomyolysis. In our case though, total
bypass time was short and patient was minimally cooled. To be cautious we monitored potassium levels hourly and checked the urine myoglobin and CPK levels postoperatively.
Our patient had moderate restrictive lung disease as demonstrated by preoperative pulmonary function tests. We therefore extubated onto non invasive ventilation and used it to gradually wean him off from ventilatory support. Incentive Spirometry was advised thereafter. It is generally this phase where many patients who have had a safe anaesthetic land into trouble and develop respiratory failure.
These patients are generally on chronic steroid therapy which may lead to obesity, glucose intolerance, osteoporosis and may require stress doses during surgery. Our patient though, had no history of steroid therapy.
In summary, careful history can alert an astute anesthesiologist towards the possibility of a muscular dystrophy. Serum CPK levels have a high negative predictive value for these conditions. Preoperative workup should
include pulmonary function testing. Total intravenous anesthesia (TIVA) with propofol is a safe option as it avoids the use of volatile anesthetic agents. Atracurium not just avoids the use of Succinylcholine but is preferred over other nondepolarisers because its spontaneous reversal obviates the use of neostigmine and does not carry the risk of accumulation if a patient were to go into renal failure from rhabdomyolysis. Prompt recognition and management of hyperkalemia is paramount for a successful outcome. Written information to the patient and recording of the problem prominently in the case notes may avoid future anesthetic mishaps.
References:
1. Poole TC, Lim TYJ , Buck J et al. Perioperative cardiac arrest in a patient with previously undiagnosed Becker's Muscular Dystrophy after isofluorane anesthesia for elective surgery. British Journal of Anesthesia; 2010;104(4):487-9.
2. Obata R, Yasumi Y, Suzuki A, et al. Rhabdomyolysis in associat ion with Duchenne's muscular dystrophy. Canadian Journal of Anesthesia 1999; 46:564-6.
3. Buzello W, Krieg N, Schlickwei A. Hazards of neostigmine inpatients with neuromuscular disease: report of two cases. British Journal of Anesthesia; 1982:54:529-532.
4. Birnkrant DJ, Panitch HB, Benditt JO, Boitano LJ, Carter ER, Cwik VA et al. American College of Chest physicians Consensus statement on respiratory and related management of patients with Duchenne Muscular Dystrophy undergoing anesthesia or sedation. Chest 2007:132:1977-1986
5. Maccario M, Fumagalli C, Dottori V et al. The association between rhabdomyolysis and acute renal failure in patients undergoing cardiopulmonary bypass. Journal of Cardiovascular Surgery.1996:37:153-159.

14
CME & WORKSHOP - 2009
15
POSTOPERATIVE NAUSEA AND VOMITING
l 1Dr. Jitendra Agrawal, Dr. Bhanu Choudhary, Dr. Dilip Kothari
1. Department of Anaesthesia
GRMC Gwalior
espite having the better understanding knowledge about the pathophysiology of D
nausea and vomiting and use of more stable and effective anti-emetics like ondansetron, granisetron, the postoperative nausea / vomiting (PONV) continues to be the most disturbing complication following surgery and anaesthesia.1 The negative impact of PONV on patient's physical, metabolic and psychological condition not only delays discharge from or cause re-admission to hospital but also decreases the confidence level in future surgery and anaesthesia.1 PONV is considered by some patients to be even worse than postop pain. While the incidence of postoperative nausea and vomiting (PONV) varies considerablyin both the inpatient and outpatient setting, 2-5 studies indicatethat the incidence of nausea ranges from 22% to 38%6and the incidence of vomiting ranges from 12% to 26%.6
Definitions
Nausea: It is an unpleasant sensation referred to a desire to vomit, not associated with expulsive muscular movement.
Retching: When no stomach contents are expelled even with expulsive muscular efforts.
Vomiting:It is the forceful expulsion of even a small amount of upper gastrointestinal contentsthrough mouth.
Physiology of nausea and Vomiting
There are three major components of vomit
reflexemetic detectors, integrative mechanism and motor output .
The main sensors of somatic stimuli are located in the gut and chemo-receptor trigger zone (CTZ). The emetic stimuli in gut are detected by two types of vagal afferent fibers.
(a) Mechanoreceptors:They are located in the muscular wall of the gut and are activated by contraction and distension of the gut, on physical damage and manipulation during surgery. Distension of the proximal gut may induce vomiting such as in overeating.
(b) Chemoreceptors: They are located in the mucosa of the upper gut and sensitive to noxious chemical stimuli. CTZ (chemoreceptor trigger zone) lies withinthe portion of brain stem. The area postrema is able todetect the circulating toxins in the CSF and activates thevomiting centre in the medulla. Afferent impulses fromother areas can also influence the vomiting centre (Vestibularlabyrinthine e.g. morning sickness, input from higher centresuch as limbic system and visual cortex). Vestibular cardiacafferent may induce nausea and vomiting as in MI.
The vomiting centre in medulla oblongata is inthe close proximity to other visceral centres like the respiratory and vasomotor centres. Four types of receptorsare involved cholinergic, dopaminergic, histaminic andserotonergic.
Integrative mechanism: It is a motor
1. MD Associate professor, Dep. of Anaestheilogy G.R. Medical College, Gwalior, M.P
2. MD Associate professor, Dep. of Anaestheilogy G.R. Medical College, Gwalior, M.P
CME & WORKSHOP - 2009programmeinvolving coordination between many physiological systemsand autonomic and somatic components of the nervous system. These occur in brain stem.
The motor component of vomiting reflex is mediatedby both autonomic and somatic senses, and is coordinatedby the vomiting system in the brainstem. The vagal motor neurons supplying the gut and the heart originate in dorsalmotor vagal nucleus and nucleus ambiguous. The dorsal and ventral respiratory groups regulating phrenic nerveoutput from the cervical spine, located in the brainstem,are parasympathetic neurons (which also maintain sympathetic tone to heart and blood vessels). The output of these nuclei is coordinated to produce the physiological pattern associated with vomiting.
The vomiting reflex is divided into two phases.
1. Pre-e ject ion phase: Th is i s characterized by a sensation of nausea associated with cold, sweating, pupil dilatation, salivation and tachycardia mediated bysympathetic and parasympathetic nerves.
2. Ejection phase: This comprises of retching and vomiting with expulsion of gastric contents.
Causes of vomiting
1. Pharyngeal stimulation.
2. Gastrointestinal distension.
3. Abdominal surgery.
4. Anaesthetic agents.
5. Pain.
6. Opioid medication.
7. Hypoxia.
8. Hypertension.
9. Vestibular
RISK FACTORS
PONV is supposed to be multifactorial in
origin, involving anaesthetic, surgical, and individual risk factors. Apfel and colleagues7 identified four risk factors that form the basis for the Apfel scoring system: female gender, history of PONV/motion sickness, non-smoking status, and use of postoperative opioids. Each risk factor increases the likelihood of PONV by ~18–22%7. Although Apfel defined the risk criteria with the largest impact on PONV, multiple other risk factors have been identified. These can be broadly divided into three categories: patient risk factors, anaesthetic technique, and surgical procedure.Only some of these factors can be influenced by the anaesthetist (Table I).
Factors not under the control of the anaesthetist
There are so many factors which affect the incidence of PONV include age, sex, history of previous PONV or motion sickness, smoking, surgical procedure, duration of surgery and anaesthesia, and patient and parental anxiety.
Sinclair et al reported that the incidence of PONV decreased after age of 50 years. Age decreased the likelihood of PONV by 13% for each 10-year increase8. In patients between 18-49 years, the incidence of PONV was 24%, and the incidence decreased to 6% among patients from 49-79 years.9
Women have three times the risk for PONVcompared to men9. This gender difference has beenattributed to variations in serum gonadotropin or other hormone levels10.
History of previous PONV or motion sickness is a strong predictor and increases the risk for PONV by two to three times.
Smoking is associated with a decreased risk forPONV. The relative risk for PONV in smokers is0.6. Sinclair et al reported that smoking decreased the likelihood of PONV by 34%. Preoperative factors like food, anxiety and premedication also has a role in PONV.

16 17
2) Sex
3) History of previous PONV or motion sickness
4) Smoking
5) Surgical procedure
6) Duration of surgery and anaesthesia
7) Patient and parental anxiety
Factors under the control of the anaesthetist
1) Premedication
2) Type of anaesthesia
3) Intraoperative anaesthetic drugs
(a) Nitrous oxide
(b) Intravenous agents
(c) Inhalation agents
(d) Antagonists of non-depolarising neuromuscular blocking drugs
4) Postoperative management
(a) Pain management
(i) Local anaesthetics
(ii) NSAIDs
(iii) Opioids
(b) Movement
(c) Oral intake
( d ) N o n - p h a r m a c o l o g i c a l – acupressure/acupuncture
5) Antiemetic drugs
6) Other factors – hypovolemia, gastric distension
ANTIEMETIC DRUGS
There are at least four major receptor systems involvedin the aetiology of PONV. Currently, available antiemeticsmay act at the cholinergic (muscarinic), dopaminergic(D2), histaminergic (H1), or serotonergic (5HT3) receptors.Neurokinin-1(NK-1) receptor
antagonists are also beinginvestigated. Cholinergic receptors are found in the vomitingcenter and vestibular nuclei. The area postrema is rich indopamine (D2), opioid, and serotonin (5HT3) receptors. Thenucleus tractus solitaries is rich in enkephalins and in histaminic(H1), muscarinic cholinergic, and NK-1 receptors. The latter are also found in the dorsal motor nucleus of thevagus nerve.
Butyrophenones
Droperidol is the only commonly used butyrophenonefor its antiemetic action. It is a heterocyclic neurolepticwhich inhibits d o p a m i n e r g i c r e c e p t o r s i n t h e chemorecep to r t r i gge r zone o f t he medulla.Droperidol in small doses (e.g. 0.625 mg) is highly effective in adults and has minimal side-effects.Droperidol, in doses as low as 0.625 or 1.25 mg has been shown to be as effective as ondansetron 4 mg without increasing sedation, agitation, anxiety or delaying discharge.
Benzamides
Metoclopramide is the most effective antiemetic ofthis class and has been used for almost 40 years. Its antiemetic effect results fromantagonism of dopamine's effects in the chemoreceptortrigger zone. At high doses, it also antagonises 5-HT3receptors. Additional antiemetic effects are dueto its dopaminergic and cholinergic actions on thegastrointestinal t r a c t w i t h i n c r e a s e s i n l o w e r esophagealsphincter tone and facilitation of gastric emptyinginto the small intestine. These latter effects reverse thegastric immobility and cephaled peristalsis thataccompany the vomiting reflex. Opioid-induced PONVcan be treated with metoclopramide because it reversesthe gastric stasis induced by morphine. There wasno evidence of dose-responsiveness, with the bestdocumented regimen in adults being intravenous(i.v.) 10 mg and in children i.v. 0.25 mg/kg. Side effectsinclude abdominal cramping, sedation,
Some surgeries eg. plast ic (breast augmentation), ophthalmologic (strabismus repa i r ) , ENT-denta l , gynaeco log ic , laparascopic(sterilisation), genitourinary, orthopaedic surgery(shoulder procedures), mastectomies and lumpectomies are associated with higher incidence of PONVthan others.With increasing duration of surgery and anaesthesia,the risk of PONV increases possibly because of greateraccumulation of emetogenic anaesthetic agents.The incidence of PONV increases from 2.8% in patientswith a surgical duration of less than 30 minutesto 27.7% in patients with a surgical duration of between151 to 180 minutes. The duration of anaesthesiaincreases the risk for PONV by 59% for each 30 minute increase8.
Factors under the control of the anaesthetist
Factors such as premedication, type of anaesthesia, intraoperative anaesthetic drugs, postoperative management and antiemetic drugs can affect the incidence of PONV.
Premedication
Atropine delays gastric emptying and lowers the esophageal tone, opioids like morphine andpethidine increase gastric secretion, decrease GImotility delay gastric emptying increases the risk of PONV.The a2 agonist clonidine can reduce PONV in children after strabismus repair.
Type of anaesthesia
When possible, regional anaesthetic should be given as patients receiving general anaesthesia are more likely to experience11 foldincreased risk of PONV monitored
8anaesthetic care .When general anaesthetic is required, the use ofpropofol as the induction agent is effectivein reducing early PONV
12incidence when comparedwith thiopentone 13and other induction agents .Nitrous oxide
14omission reduces incidence of vomitting ,
keeping in mind that omission may increase the risk of intraoperative awareness.Ether and cyclopropanecause a higher incidence of PONV due tocatecholamines. Sevoflurane, enflurane, Desflurane and halothane are associated with lesser degree ofPONV.It is commonly thought thatneostigmine,reversal of non-depolarizing is associated with increased PONV due to the muscarinic actions on thegastrointestinal tract. It is interesting then that someauthors reported no significant difference in PONVbetween those who received a reversal agent and those who did not.
Postoperative factors
Pain can increase the incidence of PONV15by prolonginggastric emptying time resulting in nausea andvomiting.Opioids are often used to treat postoperativepain. However, the use of postoperative opioids canincrease PONV.Balanced analgesiausing combinations of systemic opioids, regionalnerve blocks, local anaesthetic, and other forms ofanalgesia like n o n - s t e r o i d a l a n t i - i n f l a m m a t o r y drugs(NSAIDS) can be used to manage pain and reducethe incidence of opioid-related PONV16.Regional anaesthesia can be used as the soleanaesthetic or as a supplement to general anaesthesia to reduce PONV.
Postoperative hypovolemia can result in orthostatichypotension, dehydration and dizziness, all of whichcan increase PONV. Appropriate intraoperative fluid administration h a s b e e n r e p o r t e d t o r e d u c e postoperativenausea and vomiting following ambulatory surgery.
Gastric distension, early ambulation and postoperative oral intake affect PONV as well.
Table I. Factors affecting the incidence of postoperative nausea and Vomiting11.
Factors not under the control of the anaesthetist
1) Age

18
CME & WORKSHOP - 2009
19
dizziness, andrarely dystonic extrapyramidal reactions (oculogyriccrises, opisthotonus, trismus, torticollis), and cardiacdysrhythmias. Metoclopramide has been shown notto be as effective as ondansetron and droperidol inpreventing postoperative vomiting in a meta-analysis17.
Histamine Receptor Antagonists
The most commonly used drug is dimenhydrinate.Intravenousdimenhydrinate 2 0 m g d e c r e a s e s v o m i t i n g a f t e r outpatientsurgery in adults. In children, i.v. dimenhydrinate0.5 mg/kg significantly
decreases the incidence ofvomiting after strabismus surgery and is not associatedwith prolonged sedation.
Muscarinic Receptor Antagonists
Scopolamine blocks transmission of impulses to the medulla arising from overstimulation of the vestibular apparatus. Application of a scopolamine patchbefore the induction of anesthesia protects against PONV after middle ear surgerythat is likely to alter the function of the vestibular apparatus.
5-HT3 Receptor Antagonists
Ondansetron, granisetron, dolasetron,
tropisetron, palonosetron andother serotonin an tagon i s t s have been shown t o provideeffective treatment and prophylaxis of PONV and are associatedwith a low incidence of side effects. These agents arenot dopamine,muscarinic, or histamine receptor antagonistsand, as such, are not associated with the side effects commonto those classes. Side effects common to the serotonin a n t a g o n i s t s i n c l u d e h e a d a c h e , l i g h t h e a d e d n e s s , d i z z i n e s s , a n d constipation.They are highly effective in the preventionand treatment of postoperative nausea and vomiting.They are not effective in the treatment of motion induced nausea and vomiting.
Ondansetron
Ondansetronwas the firstdrug of this class to become available for clinical use in1991.It is a carbazalone derivative that isstructurally related to serotonin and possesses specific5-HT3 subtype receptor antagonist properties, withoutaltering dopamine, histamine, adrenergic, or cholinergic receptor activity.The usual clinical doses of ondansetron is 4 to 8 mg.for the treatment of established PONV, Tramèret al concluded that there were no differences in the effectiveness of 4, or 8 mg ondansetron when usedfor rescue from PONV in the PACU.
Granisetron
Granisetron is a more selective 5-HT3 receptorantagonist than ondansetron. An i.v. dose as low as0.04 mg/kg is effective in the prevention of PONV.The elimination half-life of granisetron (nine hours) is2.5 times longer than that of ondansetron and thusmay require less frequent dosing. The high cost ofgranisetron may limit its clinical application.
Dolasetron
Dolasetron is a highly potent and selective 5-HT3receptor antagonist. The optimal dose for prophylaxisis 50 mg if given at induction of
anaesthesia.Established PONV is effectively ameliorated by IVdolasetron 12.5 mg. After its admin is t ra t ion,dolaset ron is rap id ly metabolised to hydrodolasetron,which is r e s p o n s i b l e f o r t h e a n t i e m e t i c effect.Hydrodolasetron has an elimination half-life ofapproximately eight hours and is 100 times more potentas a serotonin antagonist than the parent compound.
Tropisetron
Tropisetron is an indoleacetic acid ester of tropine thatpossesses 5-HT3 receptor antagonist activity. Intravenoustropisetron 2 mg in adults or 0.1 mg/kg in children may be effective against PONV. It has a longer half-lifethan ondansetron but whether this translates to a clinicaladvantage remains unclear.
Palonosetron
Palonosetron is a second generation 5-HT3 receptor antagonist with longer half-life and higher receptor binding affinity than Ondansetron.Palonosetron was initially approved for prophylaxis of nauseaand vomiting in cancer patients, as it improves theprevention of chemotherapy induced nausea andvomiting and proved superior to ondansetron in thesepatients.Because of its unique chemical structure, greater binding affinity with additional allosteric site binding property and a substantially longer half-life of almost 40 hours made palonosetron suitable for its use in prevention of PONV1.It is given as a single dose of 0.25 mg IV dose be administered over 30 seconds. Maximum dose 0.75 mg
NK1 receptor antagonists
Aprepitant , a novel NK-1 receptor antagonist ,the first of this class, has been approved by the FDA for the prevention of both acute and delayed chemotherapy-induced nausea and vomiting (CINV).The dose of aprepitant for PONV prophylaxis is 40
Table 2. Prophylactic doses and timing for the administration ofantemetics
Drug Dose Timing Adverse effects
30 31 Ondansetron 4-8 mg IV At end of Surgery Headache, lightheadedness, elevated liver enzymes
32 32 Dolasetron 12.5 mg IV At end of Surgery Headache, lightheadedness, elevated liver enzymes
33-35 33,35 Granisertron 0.35-1 Mg IV At end of Surgery Headache, lightheadedness, elevated liver enzymes
36-37 36-37 Tropisetron 5 mg IV At end of Surgery Headache, lightheadedness, elevated liver enzymes
38-40 41 Dexamethasone 5-10 mg IV Before induction Vaginal itching or anal irritation with IV bolus
36-37 42 Droperidol 0.625-1.25 mg IV At end of Surgery Sedation, dizziness, anxiety, hypotension, EPS
43 Dimenhydrinate 1-2mg/kg IV Sedation, dry mouth, blurred vision, dizziness, urinary retention
44 44 Prochlorperazine 5-10mg IV At end of surgery Sedation, hypotension, EPS
44 44 Promethazine 12.5-25 mg IV At end of surgery Sedation, hypotension, EPS
4546 Scopolamine Transdermal patch Prior evening or 4 hours Sedation dry mouth, visual disturbances; CNS effects in elderlybefore end of surgery patients, renal or hepatic impairment sedation, hypotension,
EPS
Metoclopramide 25 or 50 mg IV for Sedation, hypotension, EPS47Prophylaxis
Diclectin 10 mg doxylamine Before inductionSuccinate and 10 mg Prior evening 2 tabletsPyridoxine Before induction,hydrochloride moming of
surgery, 1 tablet
After surgery, 1 tablet
Aprepitant 40 mg PO 1-3 hours prior to Headache, fatigue, dizziness elevated liver enzymesinduction of anaesthesia

20
CME & WORKSHOP - 2009
21
mgadministered 3 hours or less prior to surgery. Aprepitanteffectively diminishes post-operative nausea and vomitingwhile increasing analgesic tolerance in laparoscopic gynecological procedures.18It appears c o n c e i v a b l e t h a t a t l e a s t i n certa incircumstances NK-1 receptor antagonists and 5-HT3 antagonists may be somewhat synergistic.
Other Drugs
Dexamethasone has antiemetic effects that are reportedly comparable with conventional antiemetic agents. Antiemetic efficacy is better when it is used in combination with another antiemetic drug than when it is used as the sole agent.
Combination Drug Therapy
Despite the many drugs available for PONV, there is no single drug that can claim to be the def in i t ive t reatment of th is problem.Combination drugtherapy could do as due to different mechanisms of action, combination of drug should be more effective than single drugs alone ininhibiting the complex emetic reflex.
The combination ofdexamethasone with a serotonin receptor antagonistdroperidol with ondansetron has been reported to bemore effective than either drug alone in preventingPONV.Other combinations like ondansetron and cyclizine, ondansetron and p r o m e t h a z i n e , d r o p e r i d o l a n d metoc lopramide,d imenhydr inate and metoc lopramide, d imenhydr inateand droperidol, have been tried with varying efficacyin preventing PONV.
NON-PHARMACOLOGIC METHODS
T h e s e i n c l u d e a c u p u n c t u r e , electroacupuncture, transcutaneouselectrical nerve stimulation, acupoint stimulation, andacupressure. Lee and Done, in their meta-analysis,showed that nonpharmacologic techniques wereequivalent to commonly used
antiemetic drugs inpreventing PONV in adults but not in children.19Supplemental oxygen has also been shown to have aprotective effect against PONV.20 The cost of newerantiemetic drugs and their possible side effects maywarrant renewed interest and research in this area.
SUMMARY
PONV is one of the commonest complaints following anaesthesia, and can result in morbidity like wound dehiscence, bleeding, pulmonary aspiration of gastric contents, fluid and electrolyte disturbances, delayed hospital discharge, unexpected hospital admission, and decreased patient satisfaction. Despite the vast amount of research done in this field and the variety of antiemetic drugs available, PONV still has a high incidence. Knowledge of the risk factors of PONV can assist the anaesthetist in the judicious use of pharmacotherapy to ameliorate this problem, especially in the high-risk patient. The management of PONV requires a multi-modal approach which can include the use of less emetogenic anaesthetic techniques, balanced analgesia, appropriate intravenous hydration, the use of pharmacotherapy and possibly nonpharmacologic methods.
References
1. Shadangi BK, Agrawal J, Pandey R, Kumar A, Jain S. Mittal R and Chorasia. A prospective, randomized, double-blind, comparative study of the efficacy of intravenous ondansetron and palonosetron for prevention of postoperative nausea and vomiting. Anaesth Pain & Intensive Care 2013;17:55-58
2. Apfel CC, Kranke P, Katz MH, et al. Volatile anaesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized controlled trial of factorial design. Br J Anaesth 2002; 88: 659–68
3. Chen HL, Wong CS, Ho ST, Chang FL, Hsu CH, Wu CT. A lethal pulmonary embolism during percutaneous vertebroplasty. AnesthAnalg 2002; 95: 1060–2, table of contents
4. Wu CL, Berenholtz SM, Pronovost PJ,
Fleisher LA. Systematic review and analysis
of postdischarge symptoms after outpatient
surgery. Anesthesiology 2002; 96:
994–1003
5. Visser K, Hassink EA, Bonsel GJ, Moen J,
Kalkman CJ. Randomized controlled trial of
total intravenous anesthesia with propofol
versus inhalat ion anesthesia with
isoflurane-nitrous oxide: postoperative
nausea with vomiting and economic
analysis. Anesthesiology 2001; 95: 616–26
6. Cohen MM, Duncan PG, DeBoer DP, Tweed
WA. The postoperative interview: assessing
risk factors for nausea and vomiting.
AnesthAnalg 1994; 78: 7–16
7. Apfel CC, Laara E, Koivuranta M, Greim CA,
Roewer N. A simplified risk score for
predicting postoperative nausea and
vomit ing: conclusions from cross-
val idat ions between two centers.
Anesthesiology 1999; 91: 693–700
8. Sinclair DR, Chung F, Mezei G. Can
postoperative nausea and vomiting be
predicted? Anesthesiology 1999; 91:109-
18.
9. SadqaAftab, Abdul Bari Khan,GhulamRaza.
The Assessment of Risk Factors for
P o s t o p e r a t i v e N a u s e a a n d
Vomiting.Journal of the College of
Physicians and Surgeons Pakistan 2008,
Vol. 18 (3): 137-141
10. Lerman J. Surgical and patient factors
involved in postoperativenausea and
vomiting. Br J Anaesth 1992; 69:24S-32S
11. C M Ku, B C Ong.Postoperative Nausea and
Vomiting: a Review of Current Literature.
Singapore Med J 2003; 44:366-374.
12. Myles PS, Hendrata M, Bennett AM, Langley
M, Buckland MR. Postoperative nausea and
vomiting. Propofol or thiopentone: does
choice of induction agent affect outcome?
Anaesth Intensive Care 1996; 24:355-9
13. Visser K, Hassink EA, Bonsel GJ, Moen J, Kalkman CJ. Randomized controlled trial of total intravenous anesthesia with propofol versus inhalation anesthesia with isoflurane-nitrous oxide: postoperative nausea with vomi t ing and economic ana lys is . Anesthesiology 2001; 95:616–26.
14. Tram r M, Moore A, McQuay H. Meta-analytic comparison of prophylactic antiemetic efficacy for postoperative nausea and vomiting: propofol anaesthesia vs omitting nitrous oxide vs total i.v. anaesthesia with propofol. Br J Anaesth 1997; 78:256-9.
15. Kotiniemi LH, Ryhnen PT, Valanne J, Jokela R, MustonenA,Poukkula E. Postoperative symptoms at home following day-case surgery in children: a multicentre survey of 551 children. Anaesthesia 1997; 52:963-9.
16. White PF. Management of postoperative pain and emesis. Can JAnaesth 1995 Nov; 42(11):1053-5.
17. Domino KB, Anderson EA, Polissar NL, Posner KL. Comparative efficacy and safety o f ondanse t ron , d rope r i do l , and m e t o c l o p r a m i d e f o r p r e v e n t i n g postoperative nausea and vomiting: a meta-analysis. AnesthAnalg 1999; 88:1370-9.
18. Kakuta N, Tsutsumi YM, Horikawa YT, et al. Neurokinin-1 receptor antagonism, aprepitant,effectively diminishes post-operative nausea and vomiting while increasing analgesic to lerance in laparoscopic gynecological procedures. J Med Invest 2011; 58:246-51.
19. L e e A , D o n e M L . T h e u s e o f nonpharmacologic techniques to prevent postoperative nausea and vomiting: A meta-analysis. AnesthAnalg 1999; 88:1362-9.
20. Greif R, Laciny S, Rapf B, Hickle RS, Sessler DI. Supplemental oxygen reduces the incidence of postoperative nausea and vomiting. Anesthesiology 1999; 91:1246-52.

22
CME & WORKSHOP - 2009
23
27 year old female, Primigravida, 37 weeks pregnancy with gestational A
diabetes mellitus, presented with history of leaking since 1day, for emergency LSCS and Mcdonald Stitch removal.
Her Pre op sugar was 55mg%, for which she was given dextrose 25%, 50ml. She was on regular Insulin 6u and 4 u BD.
A male child of weight 2.99 kg delivered uneventfully.Baby CIAB with normal Apgar scores, shifted to nursery.
Post op, Patient was shifted to ward with pulse 52 pm, BP108/60, RBS118 and sp02 100%.
Patient previous history included H/o migrainous attacks with photophobia since childhood days.She had no other positive medical history. Her sugar levels were normalised after delivery.
On Day 1 - Post operatively her vitals were normal and liquids were started.
On Day 2 - She complained of headache, for which treatment on line of PDPH was started, which included , I/M Dexona, Plenty of fluids and Deriphyline retard tablet, NSAIDS and Antax 0.5mg symptoms gradually improved.
On day 4 - Her discharge was planned but she complained of severe cervical pain and nausea. Pain relieved by fentanyl injection.
On day 5 - Headache persisted and she had an episode of vomiting. Her BP was
MALIGNANT PDPH - A CASE REPORT
l 1 2 3 4Dr. Hiren Shah, Dr. Harsha Desai Phulambrikar, Dr. Renuka Gupta, Dr. Seema Khandelwal,
Indeed, lumbar puncture to diagnose SAH is indicated in the scenario of a negative CT scan when the clinical suspicion is high, or in centres which lack facilities for radiological detection of SAH.
Intracerebral haemorrhage and SAH following subarachnoid block have been reported in the literature, but this appears to be a rare event and the pathophysiology is unclear.
To avoid the occurrence of an inadvertent dural puncture, an epidural technique was not selected because of the longer time of onset, relatively lower density of sensory blockade and increased risk of significant CSF leak or Post-Dural Puncture Headache (PDPH).
A possible problem of a spinal block is the potential for sudden hypotension, which can not only compromise uterine perfusion, but also precipitate nausea and vomiting, which can aggravate raised ICT, this was prevented by maintaining a narrow blood pressure margin with the use of small boluses of phenylephrine.
Patients with peripartum SAH generally present with headache.This can potentially confound diagnoses more commonly associated with pregnancy such as Severe Pre-Eclampsia and PDPH. The latter is of particular concern for anaesthetists when assessing obstetric patients with atypical headaches after central neuraxial blockade.
Conversely, worsening headache due to PDPH may confound the evaluation of a re-bleed.
Conclusion;
Loss of Cerebrospinal fluid (CSF) from the puncture site with a subsequent decrease in CSF pressure and an increase in transmural wall tension of the vessels might be predisposing factors for the rupture of a pre-existing cerebral aneurysm.
180/100mm Hg. for which Depin-R was given and CBC and Urine for albumin sent. Physician opinion sought and CT scan was advised.
Pt. convulsed on same day (GTCS 1 episode), Neurologist opinion sought and he m a d e d i a g n o s i s o f H y p e r t e n s i v e Encephalopathy / CVST. She was given Epsolin, Mannitol and supportive treatment.
CT Venogram revealed Good opacification of superficial and deep cerebral venous sinuses with no evidence of thrombosis. no obvious brain parenchymal hemorrhage or major territory inshemic infarct. Evidence of minimal sub arachnoid hemorrhage in Left sylvian fissure and along Left MCA .Mild cerebral edema.
Patient was discharged on day 8 in stable condition, with no headache,no convulsion or vomiting.
Discussion
The leakage of Cerebrospinal fluid following lumbar puncture (LP) is usually of a minor degree and seldom gives rise to any symptoms. The incidence of Spontaneous SAH is increased five-fold in a pregnant woman compared to a non-pregnant woman.
Spontaneous SAH is a rare event, ruptured intracranial aneurysms being the main cause (51-80%) followed by hypertensive diseases
Severe headache fol lowing Spinal Anesthesia (SA) in the lower segment
caesarean section (ISCS) may be due to
varieties of causes viz. postdural puncture headache (PDPH), pre-eclampsia migraine, drug induced headache and intra cranial pathology which includes hemorrhage, venous sinus thrombosis and post-partum cerebral angiopathy and PDPH in 6 hrs. After Spinal Anaesthesia and the incidence of which may vary with the size of the needle used.Peripartum SAH provides a unique clinical challenge, because there is a requirement to consider both Obstetric and Neuroanaesthetic issues during management.
A Recent Cochrane database systematic review has not shown that either Regional Anaesthesia (RA) or General Anaesthesia (GA) for LSCS is superior with respect to major maternal or neonatal outcome measures.
General anaesthetic management of caesarean section in a patient with intracranial haemorrhage has been described. The administration of a single shot of spinal block was based on the following maternal-foetal considerations: Avoidance of airway manipulation and aspiration risk, minimization of foeta l drug exposure, excel lent postoperative analgesia, earlier return to oral intake and facilitation of maternal bonding with the new-born. Additionally, there were neurosurgical concerns regarding the possibility of an unsecured ruptured vascular lesion.
A regional technique would enhance safety by preventing hypertensive responses to intubation and surgical stimuli as well as allow better perioperative monitoring for headache, focal neurological symptoms and GCS.
The major concern with central neuraxial blockade is the potential for cerebral herniation or worsening of Intracranial haemorrhage in the setting of raised ICP, secondary to a rapid decrease in CSF pressure. However, despite the evidence of raised elevated ICP being absent, the technique is reasonably safe.
1. Consultant Anaesthesiologist, GK Hospital, Indore
2. Consultant Anaesthesiologist and Head of Department of Anaesthesia GK Hospital, Indore
3. Consultant Obstetrics and Gynecology Greater Kailash Hospital Indore
4. Consultant Obstetrics and Gynecology Greater Kailash Hospital Indore

24
CME & WORKSHOP - 2009
25
Intracranial subarachnoid haemorrhage should be listed among the rare complications of spinal anaesthesia.
A dural leak following lumbar puncture might persist for months or even years without causing symptoms.
In case of a planned second puncture, persisting leakage should be ruled out by taking a thorough history.
Spinal and epidural anaesthesia are
contraindicated in patients with persisting low pressure in the CSF system or known intracranial vascular malformations.
Reference
1. British Journal of Anesthesia
86(3):442-4(2001)
2. www.oapublishinglondon.com/article/508.
3. www.ncbi.nlm.nih.gov/pubmed/1570889
magine if clinicians of earlier ages didn't Ishare their experiments and practices, successes and failures! Experiences of clinicians in form of case record and data have become foundation of e v i d e n c e b a s e d medicine. Experience of others teaches us a n d c o l l e c t e d evidence is used in making guidelines and standards. A dynamic b r a n c h a s a n e s t h e s i o l o g y i s n o e x c e p t i o n . Comprehensively recorded data will not only help to understand the clinical practices and pharmacologic properties of drugs used, but will also be helpful in medico legal instances. It will help the administration to keep check on drugs used and thus billing properly.
1Historical view
Though every event related to evolution of anesthesiology was well published and discussed, recording details of each and every case was practiced sparingly. In 1894, at Massachusetts General Hospital, Boston, surgeons Ernst A Codman (1869–1940) and Harvey Cushing (1869–1939) established the practice of keeping a careful written record (on graph paper) of the patient's pulse and
respiration rate during operations—known as the 'ether chart', Thus initiating the era of what
2we today know as "case record" . Apparently this was prompted by a d e a t h u n d e r
3anesthesia in 1893.
R a l p h Wa t e r s c h a m p i o n e d a n d e m p h a s i z e d t h e importance of written anesthetic records and later Noseworthy
(1945) produced special cards on which to 4record anesthetic details.
Manual record keeping had various advantages as ease of availibilty, ease of input and required less technical skill. Lack of better technology also favored use of manual case records. They became very popular with every institute developing its own version suited better to their functioning. But it had serious limitations of difficulty in reproduction, comparability, compilation, interpretation and analysis.
Machines moved the world and also science. The first mechanical device capable of printing an anesthetic record was the Nargraf machine of 1930 developed by EI McKessons (Westhorpe 1989) which
Anesthesia Information Management System (AIMS) : Historical Overview and Future Trends
Dr. Ritesh Dixit
Associate Professor, Dept. of Anesthesiology,
RD Gardi Medical College, Ujjain (MP) Contact- 9424881623; [email protected]
ANESTHESIA INFORMATION MANAGEMENT SYSTEM (AIMS):
HISTORICAL OVERVIEW AND FUTURE TRENDS
l 1Dr. Ritesh Dixit
1. Associate Professor, Department of Anesthesiology
RD Gardi Medical Colege, Ujjain
“Processed data is information.Processed information is knowledgeProcessed knowledge is Wisdom.”
¯ Ankala V Subbarao
RSACPCON 2014
(November 14th-16th, 2014)
24th National Conference of Research Society of Anaesthesiology Clinical Pharmacology at Dehradun
Contact Person : Dr. JP Sharma
Telephone : +91 9411718466
Email Id : [email protected]
Website : http://www.rsacpcon2014.com
6th Annual Conference of ICA (21st-23rd November, 2014)
6th Annual Conference of the Indian College of Anaesthesiologists in collaboration with University of Minnesota, USA at Bangalore
Contact Person :Dr. Murlidhar K
Telephone : +91 8027836966
Email Id : [email protected]
CAAP 2014 (22-23 November 2014)
Calicut Anaesthesia Academic Programme at Kozhikode
Contact Person : Fijul Komu
Telephone : 9865660004
Email Id : [email protected]
Website : http://www.caap2014.com
ISACON 2014 (25th-29th December, 2014)
62nd Annual National Conference of Indian Society of Anaesthesiologists at Madurai
Contact Person :Dr. SC Ganesh Prabu
Telephone : +91 9443496835
Email Id : [email protected]
Website :http://isacon2014.com
ISNACC 2015 (30th January-1st February 2015)
16th Annual National Conference of Indian Society of Neuroanesthesiology and Critical Care at Lucknow
Contact Person : Dr. Shashi Srivastava, Dr. Devendra Gupta
Telephone : 8004904594
Email Id : [email protected]
Website : http://www.isnacc.org/isnacc-2015/index.html
ISSPCON 2015
DR. Karthic Natarajan
Back and pain Centre
The Apollo clinic
62, GN Chetty Road,
T. Nagar Chennia
Email: [email protected]
IAPCON 2014 (13-15 February, 2015)
22nd International Conference of Indian Association of Palliative Care at Hyderabad
Contact Person :Dr. Gayatri Palat
Telephone : 09848021801
Email Id : [email protected]
Website :http://iapcon2015hyd.com
IACTA 2015 (20-22 February, 2015)
18th Conference of Indian Association of Cardio-Vascular Thoracic Anaesthesiologists at Jaipur
Contact Person : Dr. Navneet Mehta
Telephone : 9571549931
Email Id : [email protected]
Website : http://iacta2015.com/index.html
CRITICARE 2015 (4-8 March, 2015)
21st Annual Conference of Indian Society of Critical Care Medicine at Bangalore
Contact Person :Dr. Pradeep Rangappa
Telephone : +91 9611700888
Email Id : [email protected]
Website :http://www.criticare2015.com
CONFERENCE CALENDER

26
CME & WORKSHOP - 2009
27
generated a semi-automated record of inspired oxygen, tidal volume and inspiratory
5gas pressure.
With advent of computers, data collection and analysis peaked new heights. The monitors fed the vital data in computers which could store and reproduce data in various forms and ready to be analyzed as needed by the clinician. A feature known as RS-232 port was incorporated into all early medical monitoring devices. Equally significant, IBM decided to incorporate the same RS-232 port into the IBM Personal Computer
6 since1981. Thus facilitating use of a PC to access various measured parameters by patient monitoring devices with a view to develop useful trend displays of measured data, real-time calculation of derived parameters and hard-copy data printouts.
The RS-232 interface is to be replaced in future by the Medical Interface Bus. This is a high-tech high-speed medical plug-and-play version of the familiar domestic USB interface and will greatly facilitate medical device inter-connectivity, largely by allowing the relevant interface software to be more easily standardized.
Anesthetic Data: an important but tedious task!
Various institutions and associations have clearly lined out the list of parameters that should be monitored, documented and ready to be analyzed as part of standard anesthetic care. One comprehensive list can be viewed in Table 1 provided by American Association of Nurse Anesthetists (AANA) Practice Committee standard.
Just glancing over the exhaustive list given in Table 1, it is quite obvious that it's practically impossible to cover all these parameters manualy. Also bothering anesthesiologist with the task can interfere with the care and safety of the patient. Thus we entered the world of automation.
Automated anesthesia information management systems (AIMS)
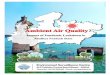
AIMS is a specialized form of electronic health record (EHR) system that allows the automatic and reliable collection, storage and presentation of patient data during the Perioperative period. This data is also used for
7management, quality assurance and research. in simple terms; it is a highly sophisticated hardware and software system which keeps track of all the events that happens during conduct of anesthesia. It also records all the drugs or instrument used. All the clinical parameters are continuously recorded and can be viewed or analyzed by any statistical tool.
In 2002, Anesthesia Patient Safety Foundation (APSF) formally endorsed the use of automated anesthesia information management systems (AIMS). The advantages and emphasis on AIMS can easily be decoded by excerpts quoted from Anesthesia Information Management Systems and Sharing Your Patient Data: A Resource for Potential Users (P repa red by Amer i can Soc ie t y o f Anesthesiologists Committee on Information Management)
"Concerns over required behavior changes, costs and legal implications have been the primary deterrents in migrating to electronic
11records. Advances in computational power, ease of use and hardware pricing have diminished many of these concerns. All the while, clinicians have intuitively recognized the potential for electronic records to provide value and improve patient safety. The directors of the Anesthesia Patient Safety Foundation (APSF), a patient safety–focused group sponsored primarily by the American Society of Anesthesiologists (ASA), have gone on record to state “The APSF endorses and advocates the use of automated record keeping in the perioperative period and the subsequent retrieval and analysis of the data to improve patient safety.”
Described by some as the “black box” or flight recorder for anesthesiology, AIMSs have been recognized and advocated as a method by which to provide better tools to analyze adverse events and near misses and to provide a global repository of outcomes data that may help to shape future safety efforts. Properly configured and implemented, an AIMS should facilitate the collection of accurate and comprehensive clinical data, thereby representing the anesthetic management of a given patient. From these data, it should be easier for institutions to demonstrate compliance with regulatory requirements, better charge capture of professional fees, and clinical competency
8through performance measurement."
Specific benefits of AIMS as in Peer 7reviewed literature are as follows
1. Cost and Billing improvements
2. Controlling and Reducing anesthesia drug costs
3. Clinical Decision Support
4. Training and provides education
5. Patient Safety and Quality Assurance
6. Enhancement of c l in ica l qual i ty improvement programs
7. Monitoring of controlled substances
8. Data quality and clinical research
9. Improved intraoperative record quality
Limitations of AIMS
1. Clinicians's hesitation – it can be either due to lack of exposure to new technologies, uncomfortable to work under continuous surveil lance of
Figure 1. Basic structure of AIMS (from Philips health care)

28
CME & WORKSHOP - 2009
29
Standard perioperative record as given by AANA
(American association of Nurse Anesthetists)
Information to be contained in the Anesthesia Record
A. Patient Information - 1. Name, 2 .Age, 3. Identification number, 4. Sex, 5. Weight, 6. Height, 7. Allergies, 8. Physical status
B. Provider Information - 1. Primary anesthetist, 2. Secondary anesthetist, if any, 3. Relief provider, times of relief, credentials
C. Anesthesia Equipment - Safety Check - 1. Equipment functioning, 2. Check performed just prior to case, 3.If indicated, list equipment numbers
D. Monitors to be Used - Minimal Standard - 1. Electrocardiogram, 2. Blood pressure, 3. Precordial stethoscope, 4. Pulse oximetery, 5. Oxygen analyzer, 6. End tidal carbon dioxide
E. Monitoring Information - Minimal Standard - On Graphic Display - 1. Electrocardiogram, 2. Blood pressure, 3. Heart rate, 4. Ventilation status, 5. Oxygen saturation,
F. Additional Monitors if Indicated - 1. Esophageal stethoscope, 2. Thermometer, 3. Nerve stimulators, 4. Respirometers, 5. Arterial catheters, 6. Central lines/pulmonary artery catheters, 7. Mass spectrometry, 8. Electroencephalography
G. Monitoring Information Indicated by Type of Procedure - Graphic Recording or Other Continuous Trending- 1. Temperature, 2. Inspired oxygen, 3. End tidal CO2 level, 4. Ventilator information - a. Tidal/minute volume, b. Peak inspiratory pressure, c. Rate, 5. Central line pressure readings - a. Pulmonary artery, b. Central venous pressure, 6. Electroencephalographic changes, 7. Other readings as indicated, i.e., degree of muscle paralysis
H. Airway Management Techniques - Indicated on Anesthesia Record - 1. Mask, 2. Intubation - a. Oral, nasal, double lumen, b. Endotracheal tube size and type, c. Cuff - absent, present, d. Laryngoscope - blade type and size, e. Performed awake or asleep, f. Technique: direct vision, blind, fiber optic, 3. Difficulties with intubation, 4. Assessment of tube placement- a. Breath sounds checked, b. Presence of EtCO2 readings, c. How secured and depth (cm) at lips/teeth, 5. Cuff inflation-air, saline, amount/pressure, 6. Times of intubation/extubation, 7. Ventilation parameters - a. Respiratory rate, b. Tidal/minute volumes, c. Peak inspiratory pressures, d. Positive end expiratory pressure, 8. Artificial airway- a. Oral, nasal.
I. Medications Administered (anesthetics, adjuncts, antibiotics, etc.) - 1. Names, 2. Routes, 3. Amounts/concentrations, 4. Times - use of graphic or continuous flow charting most desirable for anesthetic drugs, 5. Totals, when indicated, 6. Unusual patient responses (i.e., rash)
J. Techniques Used - 1. Type of anesthesia - a. General, mask or Endotracheal, b. Regional, c. Monitored care, d. Other, 2. Induction - a. Inhalation, b. Intravenous, c. Rectal, d. Intramuscular, 3. Maintenance, general anesthetics - a. Circle system, b. Non-rebreathing, 4. Intravenous routes established - a. Location of IV(s), size and patency, 5. Monitoring lines placed - a. Technique, equipment, problems, 6. Regional - a. Specific technique, equipment, problems, levels achieved, results
K. Intake - 1. Crystalloid, 2. Blood/blood products, 3. Colloids, 4. Volume expanders
L. Output - When Indicated, Should be on Record- 1. Urine, 2. Blood loss, 3. Nasogastric (may be on operative record), 4. Other, i.e., ascites could be on the anesthesia record / operating room nurse’s record
M. Procedural Data- 1. Actual operative procedure performed, 2. Date, 3. Times of starting and stopping anesthesia using 24-hour clock, 4. Times of starting and stopping procedure
N. Patient Protection - 1. Position, position changes, 2. Eye protection, 3. Securing of monitoring lines
Information to be Immediately Available in the Patient’s Operative Chart
A. Preanesthesia Assessment - 1. Review of systems, 2. Current diagnosis, 3. Pertinent lab data, 4. Pertinent physical examination findings, 5. Allergies/sensitivities, 6. Airway assessment- a. Anatomy, b. Dentures/teeth, c. Previous problems under anesthesia, 7. Surgical/anesthesia history, 8. Medication history, 9. Social history - a. Smoking, b. ETOH use, c. Drug use, 10. Family problems with anesthesia, 11. Other - a. Transfusion history, b. Disabilities, c. Communication problems, d. Prosthetics
B. Physicalal Status Assigned
C. Patient Interview Accomplished - 1. Risks/benefits discussed 2. Anesthesia plan discussed 3. Patient consent obtained
D. Patient and Procedure Identification - 1. Surgery consent form signed and dated, 2. Anesthesia consent form signed and dated, 3. Patient identified 4. Proposed procedure, 5. Surgical site affirmed
E. Patient Protection (may be on operating room nurse’s record) 1. Padding of pressure points created by surgical position requirements, 2. Special anatomical considerations, 3. Safety strap, 4. Tourniquets, placement and times, 5. Grounding plate, site
F. Transfer of Care Information - 1. To what unit (ICU, PACU, etc.) 2. Report given on - a. Patient identification, name, age, b. Allergies,c. Anesthetic type, drugs used, d. Blood/fluid status,e. Complications, if any, f. Procedure performed, g. Vital signs, h. Pre-existing conditions/medications, i. Condition, j. Airway status/oxygen requirements
Anesthesia Related Information to Appear in the Patient’s Hospital Chart
A. Post anesthesia Note - 1. Time and date of visit, 2. Complications, if any, 3. General status- a. Systems reviewed should reflect care given, 4. Signature
B. Additional Comments (May be in anesthesia record if space allows, or in progress notes. Should be indexed to events on record, if indicated.)
1. Unanticipated patient responses,
2. Emergency measures
TABLE-1

30
CME & WORKSHOP - 2009
31
automated record, less inclined for training and update, fear of increase in medico legal cases
2. Financial considerations – right way from inception to full functioning of AIMS require full monetary flow. Though beneficial in later stages, the early burdon may be too much, especially in developing countries
3. Infrastructure and Logistics – every part of AIMS will require round the clock support system along with proper training and updating of IT (Information Technology) wing of a hospital.
4. Ensuring that the data collected and analyzed is not merely used for billing and monetary gains but should reach the desired researchers and policy makers.
5. No standardization of AIMS regarding features among venders.
Broadly, there are three types of AIMS available. Examples of these types with various manufacturers are listed below. Salient features of all the options are collected from product brochures available online listed in Table 2 and listed to give a better understanding of AIMS, comparison with peers and emphasize their unique features to make a wise choice. Though efforts are made to include important features of each system, readers are requested to access to various websites given in Table 2 for a detailed understanding.
1. AIMS integrated with anesthesia monitors – examples
(A) GE- Aestiva's 7900 – Its open architecture allows you to use your current monitors and data management systems or purchase a fully integrated anesthesia system with GE CARESCAPE Monitors
(B). Philips – Besides the beautiful illustration of working of an AIIMS in figure 1
(courtesy Phillips aims product brochure) its preoperative module provides missing or abnormal test results or special conditions, can display cost alerts and alternatives as soon as a drug is selected. Charges captured from clinical data (such as administration of a drug) can be exported to pharmacy or billing. Intraoperative “Event keys” are tailored to specific procedures, Intuitive touch screen interface, Case templates, and Automatic integration of data from anesthesia machines, ventilators and patient monitors are other features.
(C). Drager-It provides Web-based pre-anesthesia assessment, comprehensive Intra-operative patient record, accurate and complete billing information data capture, supports anesthesia clinical workflow, configurable case environments to support various types of cases. Back office- Web-based access to patient records. Data can be used for research purposes and to support patient safety initiatives. Data capture of regulatory and compliance elements required for anesthesia billing.
2. AIMS integrated with operating room management systems
(A) GE (B) PICIS / OPTUM - Preop Clinical Decision Support, O R Scheduling and Workflow Management to combine superior multi-facility features with Flexible local and remote scheduling tools for better utilization of resources, Intelligent Patient Tracking, O R Dashboard and Analytics, Intelligent Supply Chain Automation and Interoperability.
(C) McKESSON – Customizes anesthesia EMR (Electronic Medical Record) in form of patient history documentation, Medication alerts to promote timely drug delivery, Formulary reference for allergies and medication increasing patient safety, Cross-checking for adverse events reduces medication errors by notifying clinicians of potential contraindications, Templates for common procedures help speed the clinical
documentation process, Automated capture of physiological data adds accuracy to the anesthesia EMR.
(D) SIS (Siemens) – Anesthesia is integrated with Other Surgery Solutions, Soarian's advanced workflow management technology, “Notify Me” workflow for reminder of patients test results, Urinary catheter workflow, Venous thrombosis embolism (VTE) workflow.
(E) CERNER - Through web based features such as automatic methods to capture information and simple reporting tools device integration, intuitive real-time documentation resources and immediate access to patient records helps to provide effective anesthesia care.
(F) EPIC - Integrated with Operating Room Management and EpicCare EMR to streamline documentation workflows across roles. Epic Anesthesia provides dedicated
support for documentation of all events from pre to post operative stage. Have multiple other modules for intensive care, nursing care, emergency, radiology, home care, pathology, biochemistry, etc.
3. Exclusively sell anesthesia information management systems (AIMS)
(A) MERGE - Besides routine features it has SAM (Smart Anesthesia Manager) which is a decision support system working in conjunction with Merge AIMS to find issues related to quality of care, billing and compliance and will be notified via pop-up screens or text pages
(B) iMD Soft – Uniquely flexible, with various advantages as Clinical decision support, Adaptability to all workflows, Reporting and analysis, Data continuity across the entire continuum of care, Full integration with healthcare IT infrastructure
( C ) A C U I T E C - V P I M S ( V i g i l a n t Perioperative Information Management
TABLE - 2

32
CME & WORKSHOP - 2009Solution), a comprehensive solution for perioperative setting that scales to facilities of all sizes, includes scheduling, preference cards, nurse documentat ion, case management, reports, anesthesia charting, mobile capabilities, etc.
(D) PLEXUS- Anesthesia Touch™ is an easy to use, full-featured AIMS for both iPad and Windows, with cloud based support and storage. Pharmacy Touch™, a modular add-on to Anesthesia Touch further helps with drugs administered in various clinical, administrative and billing aspects.
This collection of information about newer frontiers of data and information management can only provide only an overview of exhaustive newer trends in a n e s t h e s i a d a t a a n d i n f o r m a t i o n management. Though in a developing cost conscious country like India, it may appear distant dream. But with advent of medical tourism, advanced cutting edge technologies and health care setups, the IAMS are just round the corner. I hope this piece of information will stimulate your intellect and helps you to be ready for future. Remember,
anesthesiologists are usually the last warriors between patient and distress and AIMS definitely proves to be a valuable ally besides being a multi level performer.
References
1. Richard W. D. Nickalls, Simon Dales,Adrian K. Nice; Chapter 2-Data processing in anesthesia, An Open Source Anaesthesia Workstation (Linux)
2. Beecher HK (1940). The f i rst anesthesia records (Codman, Cushing). Surg.Gynecol. Obstet., 71, 689–693.
3. Rushman, Davies and Atkinson 1996, p.128
4. Noseworthy M (1945), Anesthesia and Analgesia; 24, 221. [from Rushman,Davies and Atkinson (1996)]
5. Westhorpe R (1989). McKesson 'Nargraf' anaesthesic record. Anaesthesia and Intensive Care; 17, 250.
6. Nickalls, RWD and Ramasubramanian R (1995). Interfacing the IBM-PC to medical equipment: the art of serial communication. ISBN 0-521-46280-0; pp 402 (Cambridge University Press)
o oo