Embed Size (px)
Citation preview
Introduction & epidemiology Tropical disease
.
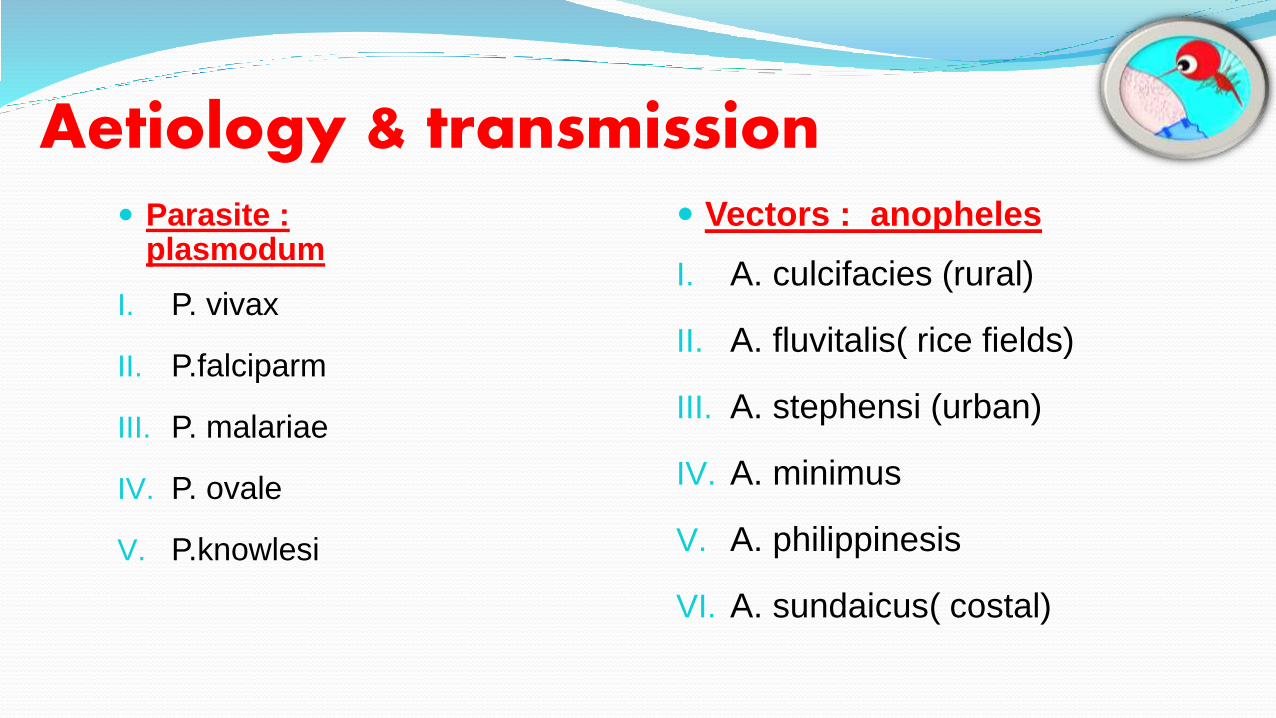
Aetiology & transmission Parasite :
plasmodum
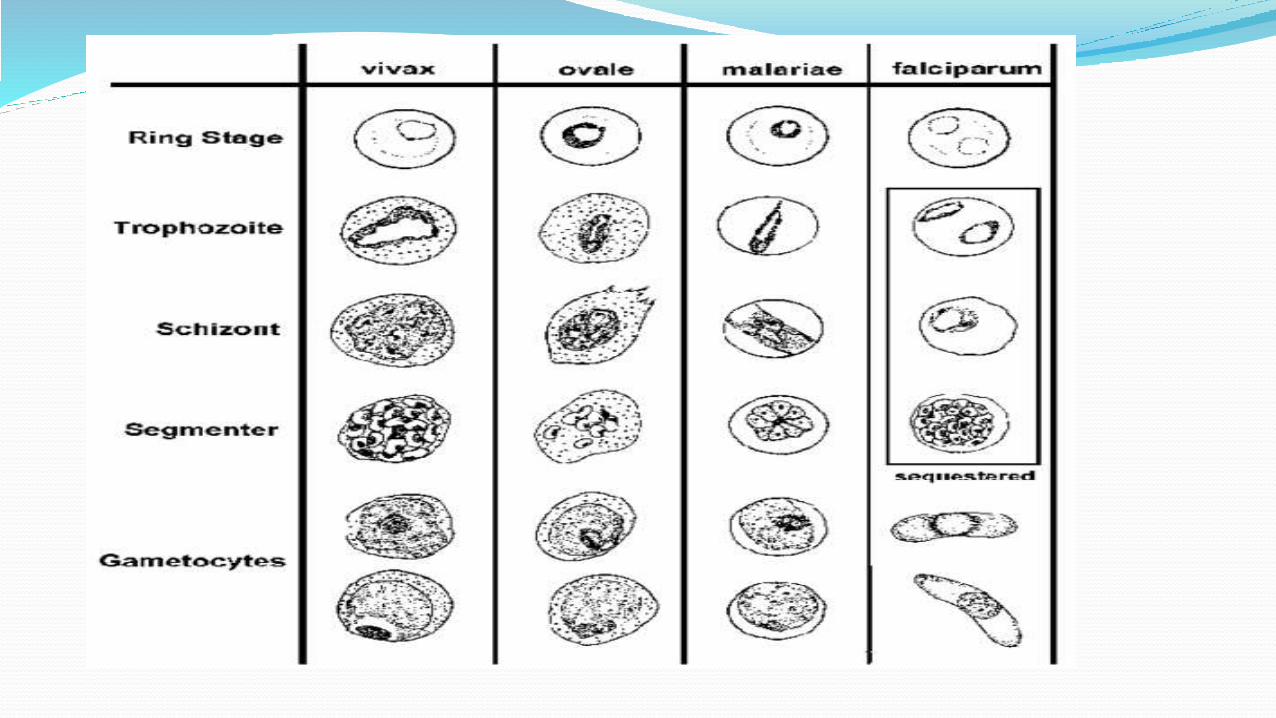
I. P. vivax
II. P.falciparm
III. P. malariae
IV. P. ovale
V. P.knowlesi
Vectors : anopheles
I. A. culcifacies (rural)
II. A. fluvitalis( rice fields)
III. A. stephensi (urban)
IV. A. minimus
V. A. philippinesis
VI. A. sundaicus( costal)
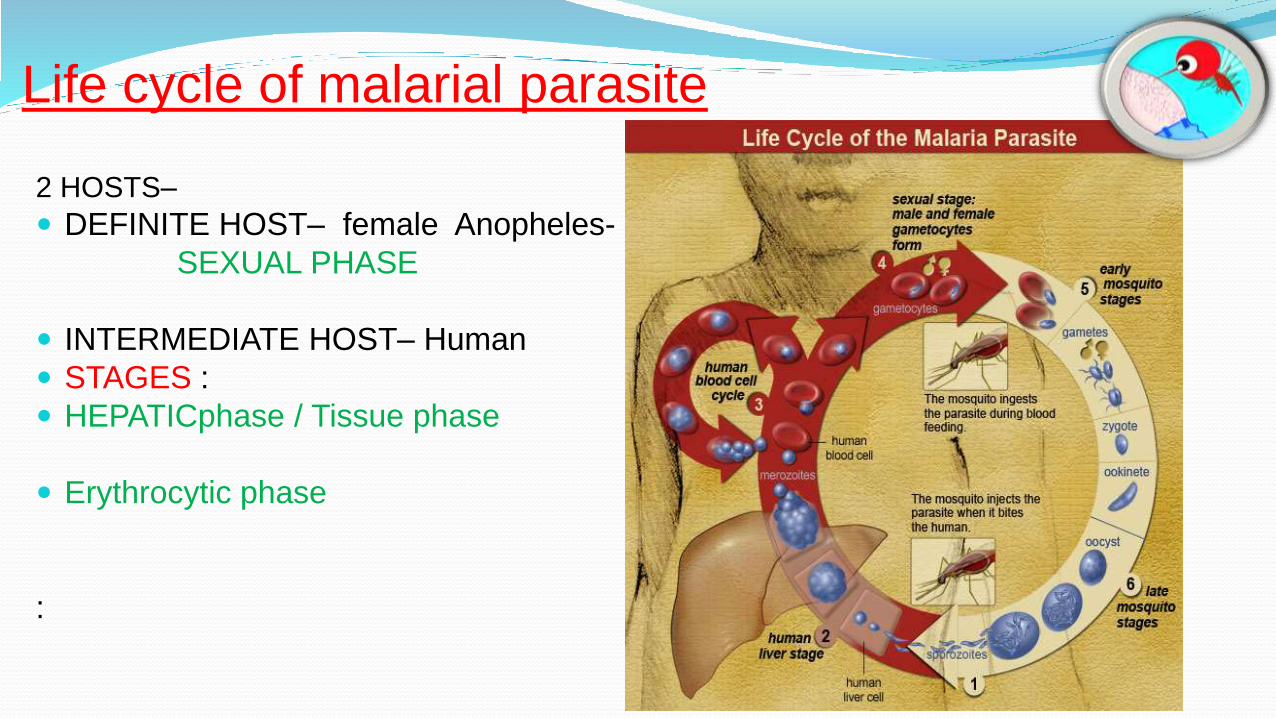
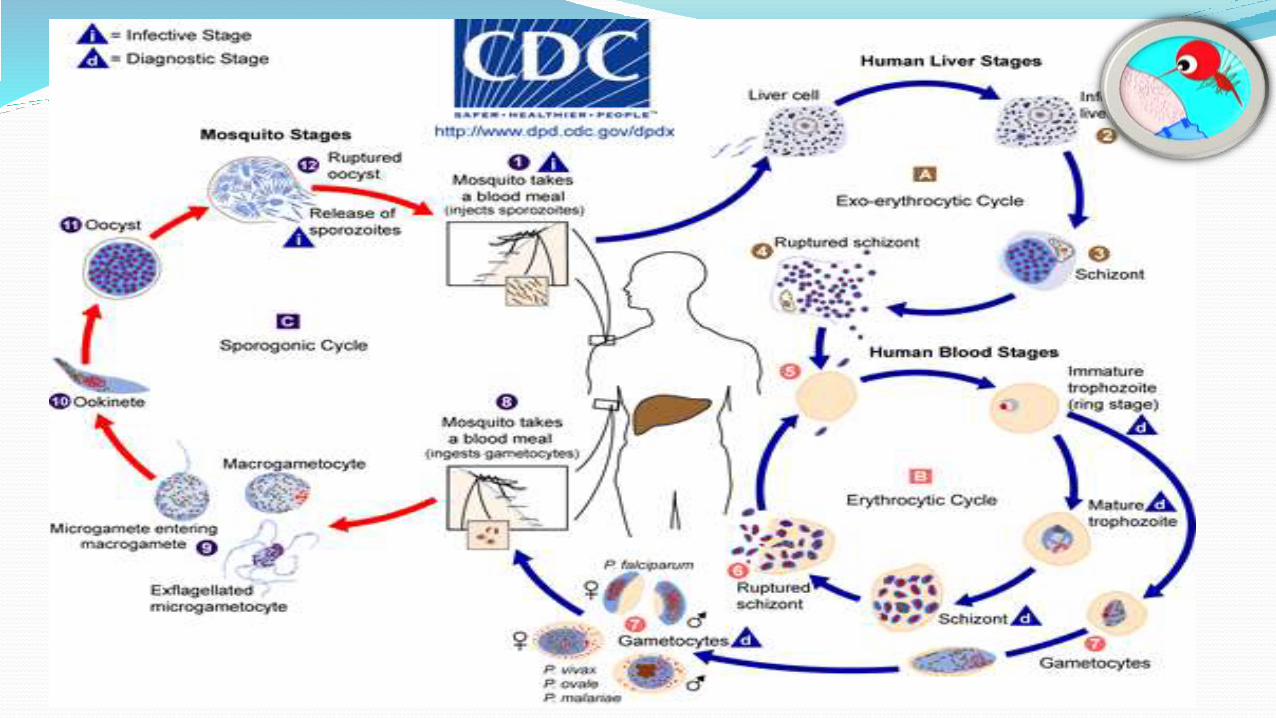
Life cycle of malarial parasite
2 HOSTS–
DEFINITE HOST– female Anopheles-
SEXUAL PHASE
INTERMEDIATE HOST– Human
STAGES :
HEPATICphase / Tissue phase
Erythrocytic phase
:
RESISTANCE MECHANISMS INNATE RESISTANCE
Natural capacity of host to resist infection from malaria. ( which is due to
differences in surface receptors , intra erythrocytic factors or yet unknown
causes. )
In Endemic zones – repeated infection – development of resistance.
vulnerable to infection with one species – due to difference in genetic
constitution of species.
INNATE RESISTANCE
INTRA ERYTHROCYTIC FACTORS :
Resist penetration of cell by merozoites- Absence of duffy Ag.-vivax
Impede their development- HbS.
Assist their removal by RES.
Differences in cell membrane – decides attachment/penetration of
merozoites to receptors/cells.
Hb F & Ovalocytes- resist p. falciparum
ACQUIRED RESISTANCE
Sporozoites --- Liver cells --- No immunological response
Merozoites --- erythrocytes ---- Immunological response
First response – phagocytosis in spleen / hyperplastic RE cells.
Cell mediated immunity – -> through activated macrophages
Host defence - defervescence of fever.
ACQUIRED RESISTANCE
Protective antibodies against merozoites – IgM
Complement system not involved
Schizont infested cells – phagocytosed rapidly – after OPSONISATION
Antibodies against toxins
Antibodies and antigens may be transmitted to fetus trans placentally
Antibodies protect while antigens / antigen-antibody complexes help toacquire immunity.
Immune Evasion By Parasite :
Reasons for survival of parasite :
Antibodies against parasite may promote their survival instead ofdestruction
Infection may impair antibody synthesis
Handling & processing of antigens by macrophages is impaired
Sporozoites , schizonts & gametocytes are not destroyed by immunesystem.
immunopathologyAnaemia
Disproportionate to the damage to RBCs by parasite.
Formation of autoantibodies to RBCs & immune binding or adherence of
circulating Ag-Ab complexes to uninfected RBCs.
Hemolysis – blackwater fever – drug hypersensitivity.
Bone marrow suppression
Renal damage
Acute transient lesion as nephritis
May progress to ARF
ARF secondary to ATN
Development of proteinuria over a period of 1 to
2 weeks
ARF is reversible
Chronic progressive nephritic syndrome
Secondary to P. malariae infections
Soluble immune complexes deposits in
BM of Glomerular capillaries – glomerular
lesions
SPLENOMEGALY
Splenomegaly – elevated levels of IgM & Lymphocytosis in peripheral blood ,
bone marrow & liver sinusoids.
Sequestration of RBC.
Splenectomy – Relapse of latent infection.
CEREBRAL MALARIA
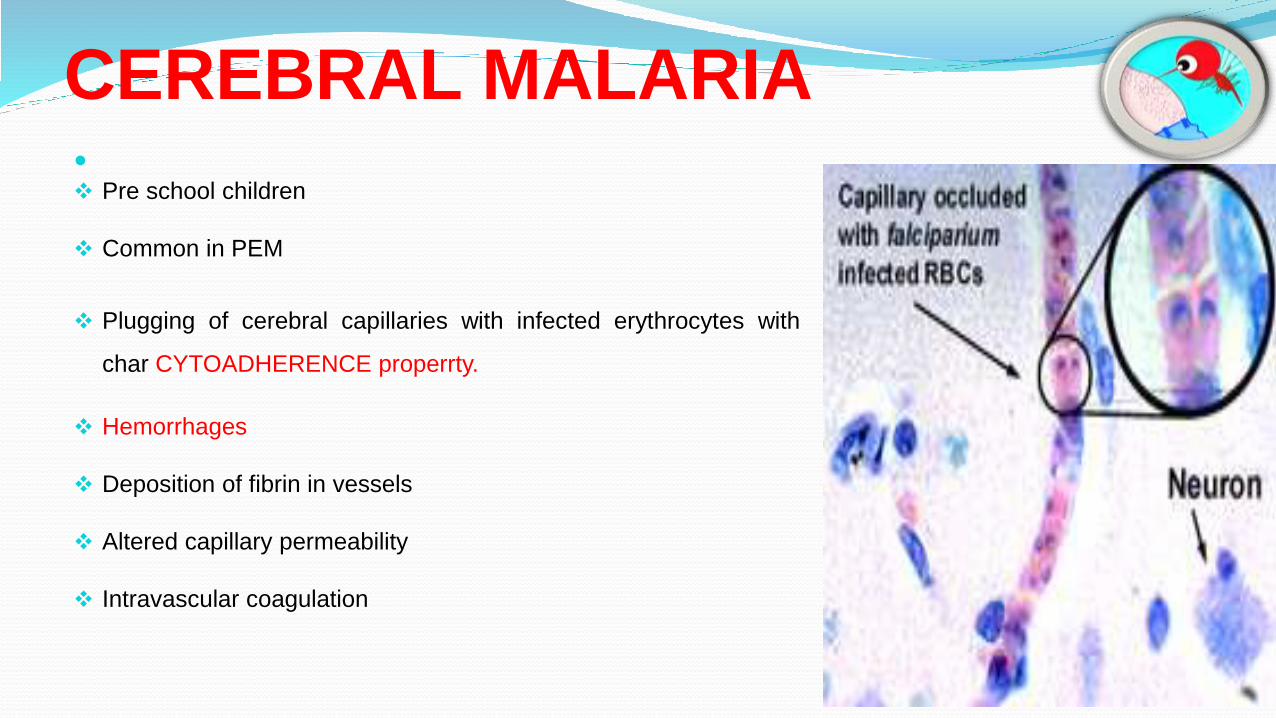
Pre school children
Common in PEM
Plugging of cerebral capillaries with infected erythrocytes with
char CYTOADHERENCE properrty.
Hemorrhages
Deposition of fibrin in vessels
Altered capillary permeability
Intravascular coagulation
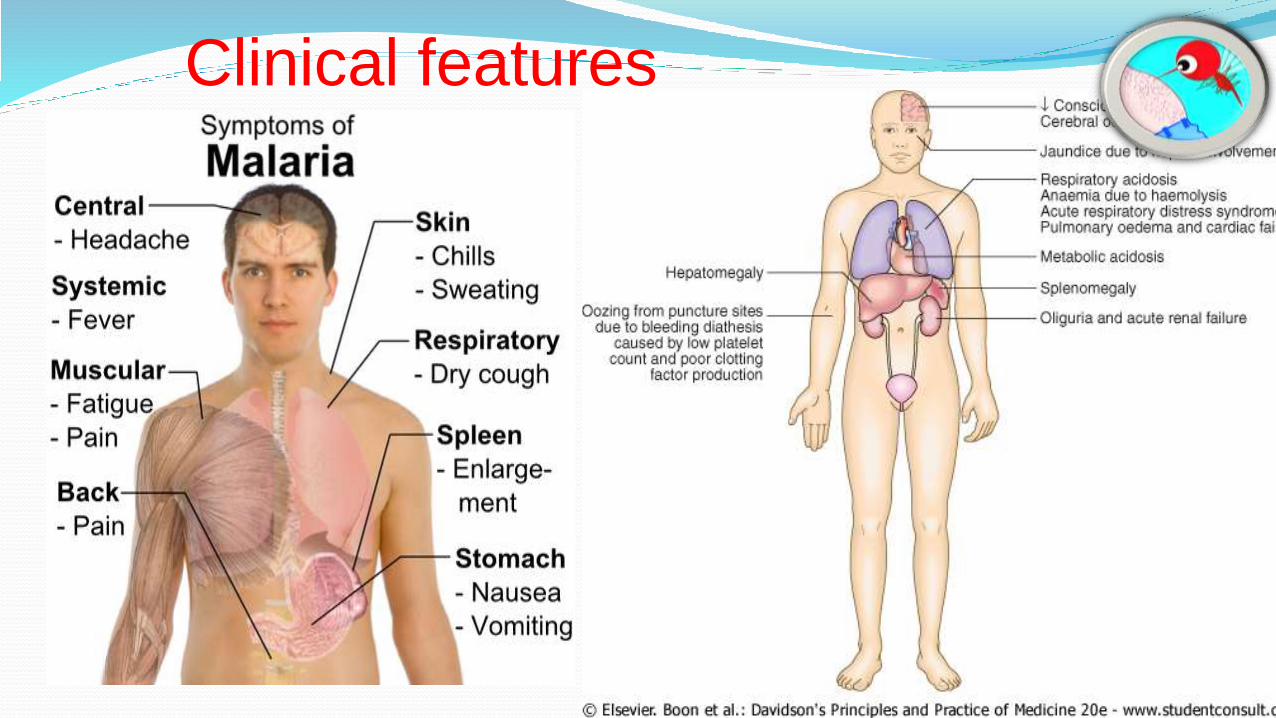
Clinical features
High risk patients –depressed level of consciousness with
deep coma.
seizures
Irregular resp.
Hypoxia
Orthostatic Hypotension
Tachycardia
JAUNDICE, PUL. OEDEMA, RENAL FAILURE- RARE.
Dehydration
Hypoglycemia
Metabolic acidosis
Hyperkalemia
Children > 2 months (non immune ) – symptoms vary widely
Low grade fever to temp of 104 F with headache, drowsiness
Anorexia, nausea, vomiting, diarrhoea
Pallor, cyanosis
Splenomegaly
Hepatomegaly
Anaemia , Thrombocytopenia
Incubation period & stages of malaria
P. falciparum: 9 – 14 days
P. vivax: 12-17 days
P. ovale: 16 – 18 days
P. malariae: 18 – 40 days
Onset – sudden with fever , headache ,
loss of appetite , lassitude , pain in
limbs.
Initially – continuous or remittent fever
Later stages – classically remittent
fever
Clinical pattern in endemic zones
Atypical
Tolerance leading to less parastitemia
Mild symptoms
After sometime – inherited immunity ->( due to continuous heavy exposure
leading to poor immunological defence) –> severe form of disease->Cerebral
malaria Death/ Re-development of tolerance
Chronic malaria with marked HEPATOSPLENOMEGALY in highly endemic
zones.
Relapse & recrudescenceRecrudescence/ re occurrence/ late rx failure – reappearance of asexual
parasites with in 28 days of treatment
Optimising the drug therapy/ change to alt . Regimens wil be the cure.
Recurrence/true relapse - persistence of hypnozoite forms in liver in which
erythrocytic schizogony commences again.
Falciparum malaria – rare relapse
(since erythrocytic schizogony does not lead to exoerythrocytic phase.)
Vivax malaria – frequent relapse
(since erythrocytic schizogony can be started in these plasmodia)
complicationsCerebral malaria
Anemia
Gastrointestinal illness
Algid malaria
Blackwater fever
Renal lesions
Splenic rupture
Hypoglycemia
Hyperpyrexia
Convulsions
Spontaneous bleeding &
coagulopathy
Aspiration pneumonia
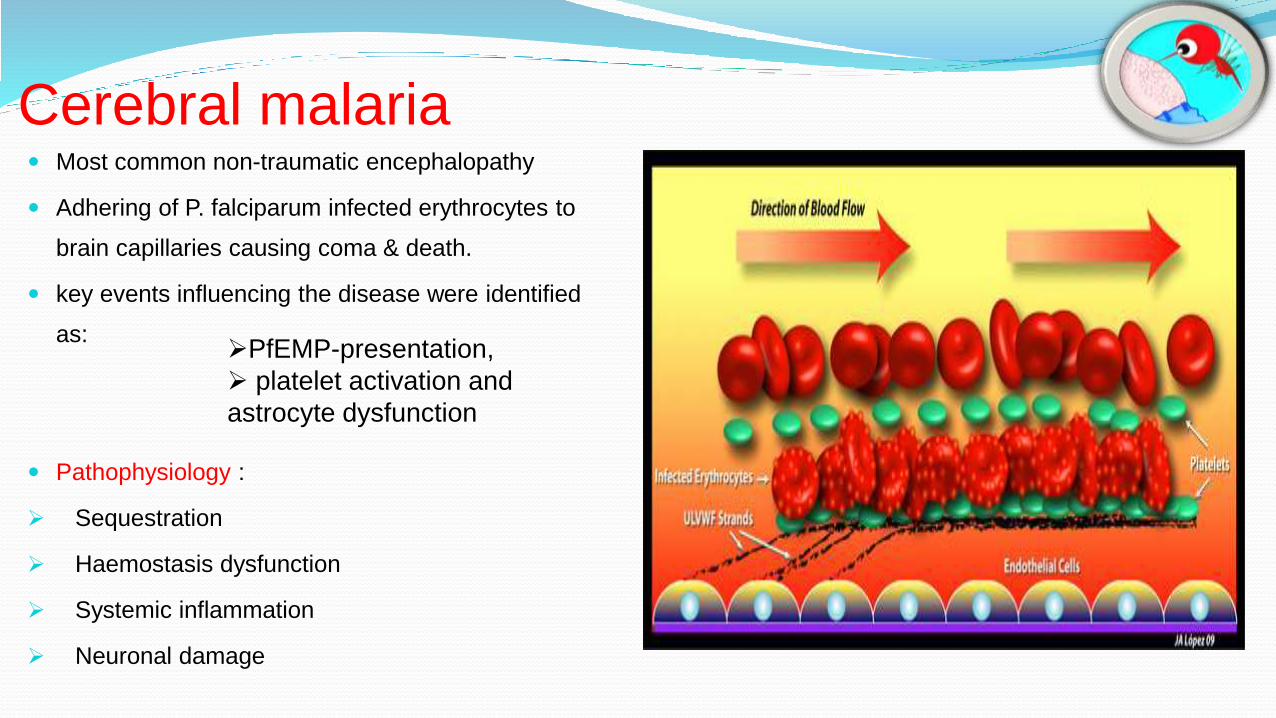
Cerebral malaria Most common non-traumatic encephalopathy
Adhering of P. falciparum infected erythrocytes to
brain capillaries causing coma & death.
key events influencing the disease were identified
as:
Pathophysiology :
Sequestration
Haemostasis dysfunction
Systemic inflammation
Neuronal damage
PfEMP-presentation,
platelet activation and
astrocyte dysfunction
It is manifested by coma or confusion.
Cerebral malarial fever d/d:
menigititis , encephalitis , head injury or tetanus
on investigation on examination
CSF is normal. splenomegaly
anaemiaIt is common in severe malaria.
Causes:
Haemolysis of infected & uninfected
erythrocytes.
Dyserythropoiesis./ BM DEPRESSION
Splenomegaly causing erythrocyte
sequestration & hemodilution.
Depletion of folate stores.
Gastrointestinal illness
Marked vomiting in infants
Diarrhoea
Dehydration
Dyselectrolytemia
Dark green or brownish stools tinged with blood
Symptoms relieved on antmalarial therapy
Algid malaria
It is charectorised by pheripheral circulatory failure and shock.
Usually occurs with falciparum inf in non immune children
Circulatory collapse – low BP , hypodermia , rapid thready pulse
Abdominal pain , vomitting , diarrhoea may be seen
Adrenal damage – congested , necrotic , haemorrhagic on post mortem
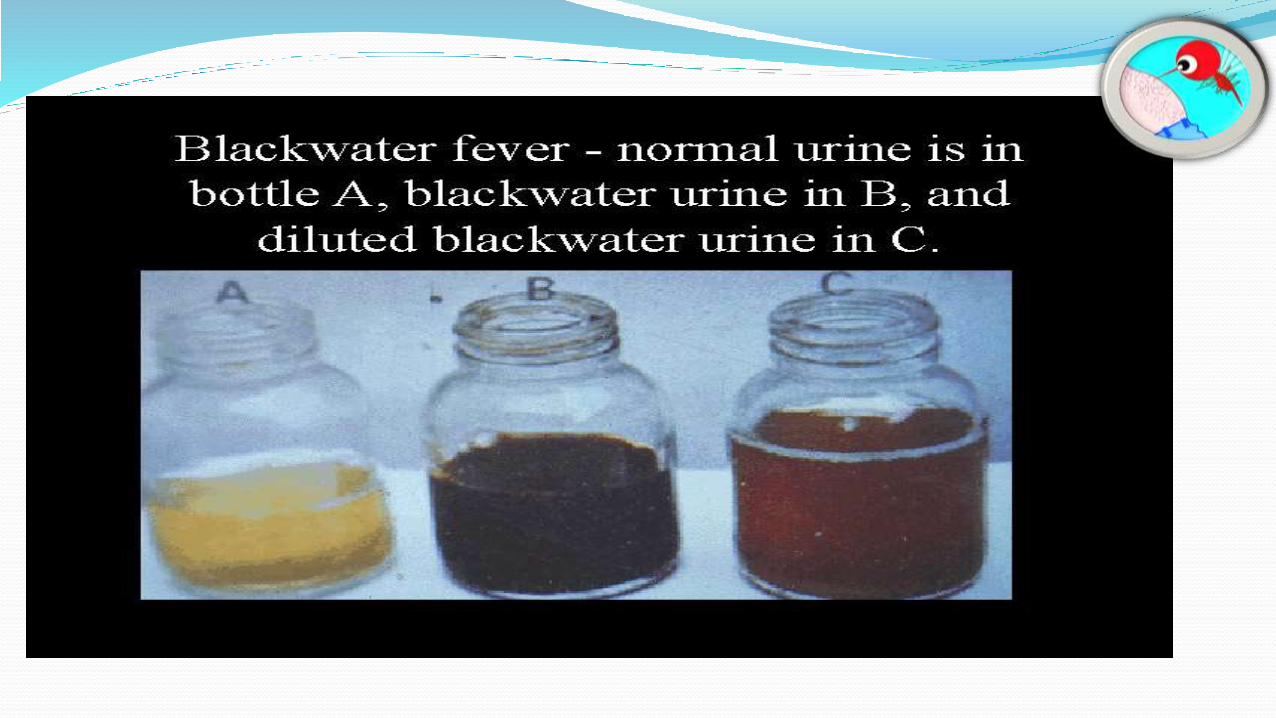
Blackwater fever Sudden severe hemolysis
Hemoglobinuria
Renal failure
Caused by hypersensitivity to antimalarial
drugs.
Nowadays – rare due to development of
synthetic drugs.
Repeated falciparum infection
Hypersensitivity
Anti erythrocyte antibodies&
Intravascular haemolysis
RBCs destroyed rapidly
Haemoglobinaemia & haemoglobinuria
Hypoglycaemia
It is a frequent complication of falciparum malaria.
It can occur due to various mechanisms:
Failure of hepatic gluconeogenesis.
Increased consumption of glucose by host & parasite.
Treatment with quinine results in stimulation of pancreas to
secrete insulin. The resulting hyperinsulinaemia causes
hypoglycaemia.
jaundice
It occurs due to severe hemolysis
& hepatic involvement.
Rare in children
Clinical manifestation include:
haematemesis or malaena
bleeding gums
epistaxis
petechiae
subconjuctival h’ages
Spontaneous bleeding
&
Disseminated intravascular coagulation
INVESTIGATIONS
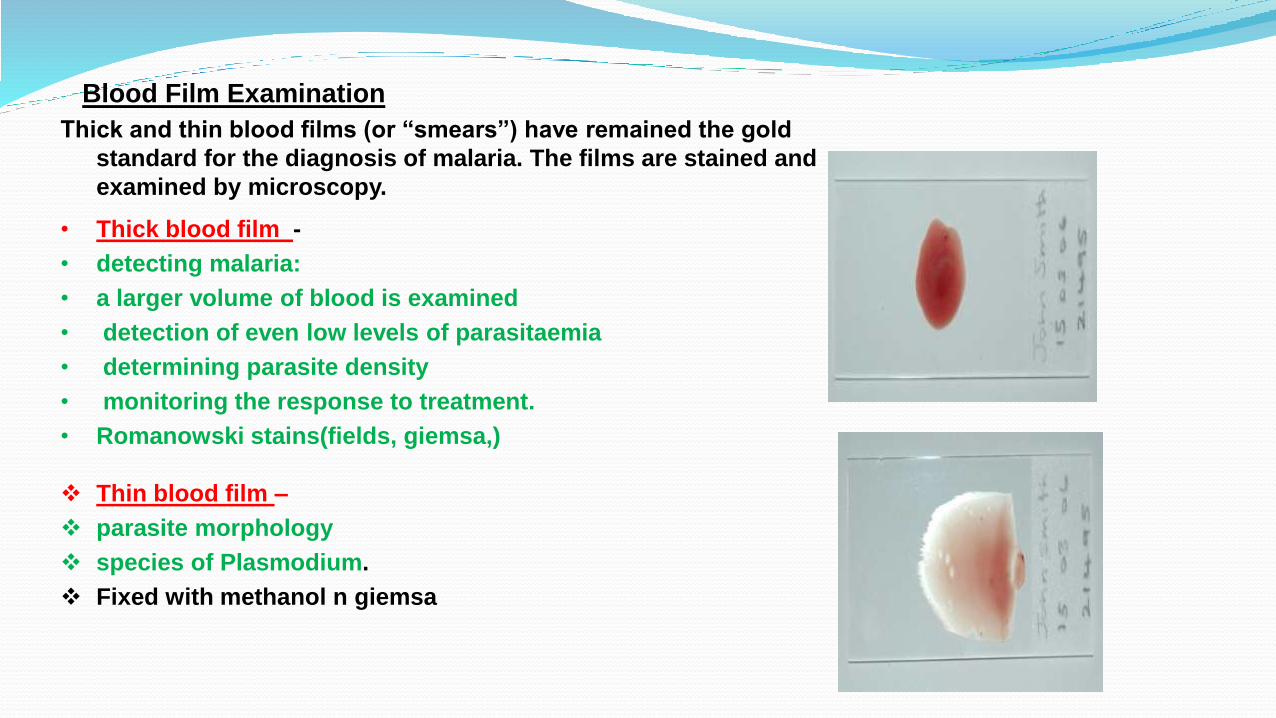
Blood Film Examination
Thick and thin blood films (or “smears”) have remained the gold
standard for the diagnosis of malaria. The films are stained and
examined by microscopy.
• Thick blood film -
• detecting malaria:
• a larger volume of blood is examined
• detection of even low levels of parasitaemia
• determining parasite density
• monitoring the response to treatment.
• Romanowski stains(fields, giemsa,)
Thin blood film –
parasite morphology
species of Plasmodium.
Fixed with methanol n giemsa
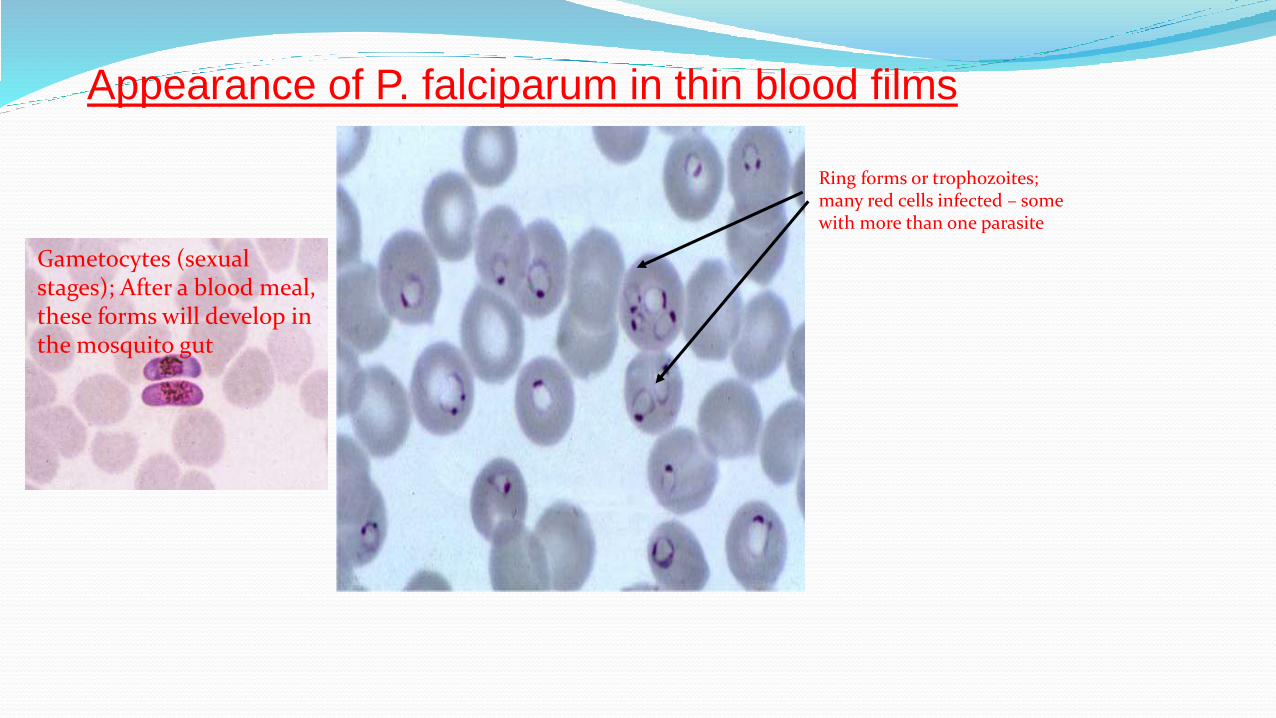
Appearance of P. falciparum in thin blood films
Ring forms or trophozoites; many red cells infected – some with more than one parasite
Gametocytes (sexual stages); After a blood meal, these forms will develop in the mosquito gut
Other methods of diagnosis of malaria
Quantitative Buffy coat test:-
It involves staining of the centrifuged & compressed red cell layer
with acridine orange & its examination under UV light source.
Fast, easy & more sensitive than thick smear examination, abt
60microlitres of blood from a finger, ear, or heel puncture is
sufficient.
The parasites contain DNA which takes up acridine orange stain,
fluorescing parasites can be observed at the RBC/WBC interface
using standard white light microscope
Rapid diagnostic tests:-
Detects malarial antigens (PfHRP2/PMA/pLDH) from asexual &/or sexual forms of
the parasite.
Detected by colour changes on the antibody coated lines on the strip test such as
optiMAL assay and para sight F test are being increasingly employed.
optiMAL:- immunochromographic test that can be performed with a drop of finger
stick blood,
Detects LDH (parasite glycolytic enzyme) produced by all species of metabolizing
plasmodium parasites
The detection limit of test is >100-200 parasites/ microL for P.falciparum & P.vivax
Positive test indicates presence of viable parasitemia.
Polymerase chain reaction:-
Highly sensitive and specific test for detecting all species of malaria,
particularly in cases of low level parasitemia and mixed infections
10 fold more sensitive than microscopy
Other investigations:-
Complete blood counts
Blood levels of glucose
Bilirubin
Urea
Creatinine
Transaminases
prothrombin time
urine analysis may be done as required.
DIFFERENTIAL DIAGNOSIS
EARLY PHASE :
Typhoid fever
Non icteric
hepatitis
Septicemia
PAROXYSMAL
PHASE :
U.T.I.
Gm. –Ve
Septicemia
Liver abscess
CEREBRAL MALARIA:
Meningitis
Encephalitis
Lead encephalopathy
Heat stroke
GASTROINTESTINAL ILLNESS:
Non specific gastroenteritis
Cholera
E. coli diarrhoea
Abdominal emergencies
ALGID MALARIA:
Shock due to septicaemia
CHRONIC MALARIAL FEVER WITH SPLENOMEGALY:
Tuberculosis
Kala azar
Leukemia

TREATMENT
Uncomplicated P. vivax malaria
CHLOROQUINE:
10mg/kg stat followed by 10mg/kg 24, 5 mg/kg at 48 hrs total 25mg/kg
PRIMAQUINE :
o.25mg/kg 14 days
(relapse prevention)
• Frequent relapse: 0.5-0.75mg/kg primaquine
• No role with quinine/ sp regimen
uncomplicated P. falciparum malaria
No role for chloroquine
ACT THERAPY - RX OF CHOICE.
Artesunate 4mg/kg oral for 3 days
+Sulfodoxine 25mg/kg& pyrimethamine 1.25mg/kg as single dose (or)
artemeether + lumefantrine ( 20mg& 120 mg) pre formulated tablets six tablets tice daily for 3
days according to weight
+
Single dose of primaquine (0.75mg/kg)
Multidrug resistant p. falciparum un compl.(
to CQ & SP) Quinine
10mg/kg orally 3 times a day for 7 days
+
• Tetra cycline (4mg /kg 4 times a day for 7 days) or
• doxycycline ( 3.5mg/kg once a dsay for 7 days) or
• Clindamycin( 20mg/kg /day two divided doses)
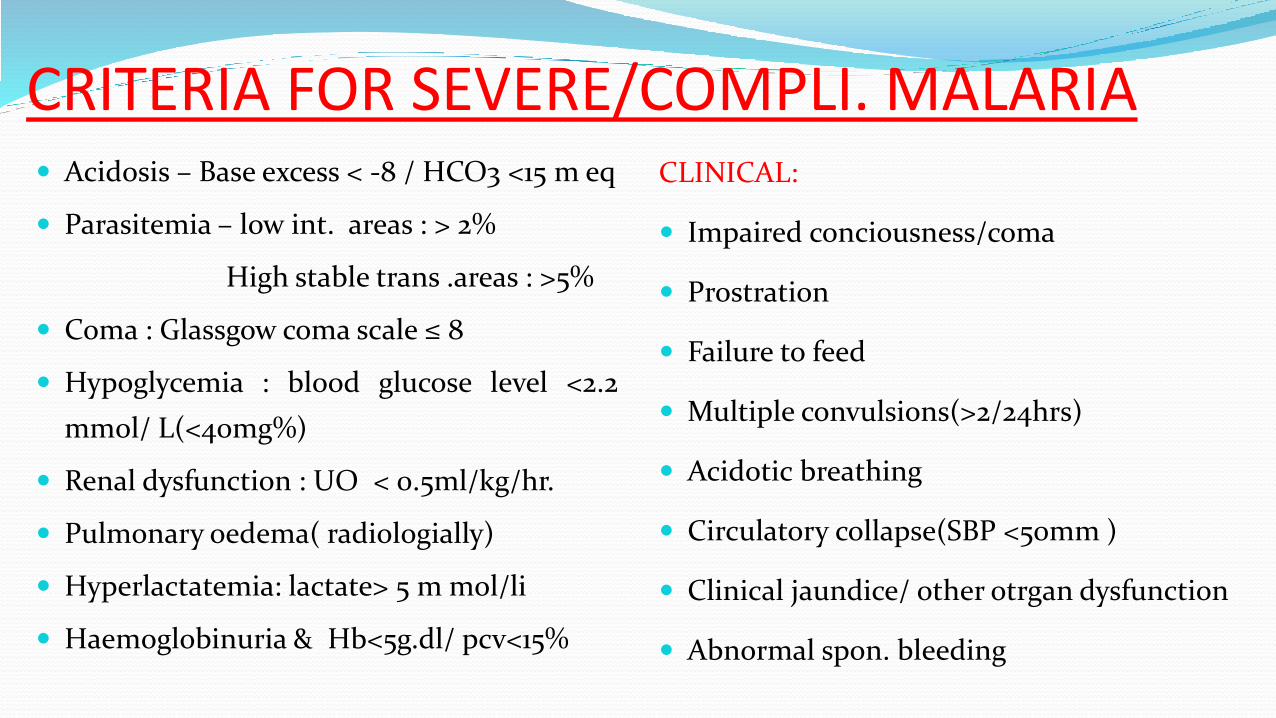
CRITERIA FOR SEVERE/COMPLI. MALARIA Acidosis – Base excess < -8 / HCO3 <15 m eq
Parasitemia – low int. areas : > 2%
High stable trans .areas : >5%
Coma : Glassgow coma scale ≤ 8
Hypoglycemia : blood glucose level <2.2
mmol/ L(<40mg%)
Renal dysfunction : UO < 0.5ml/kg/hr.
Pulmonary oedema( radiologially)
Hyperlactatemia: lactate> 5 m mol/li
Haemoglobinuria & Hb<5g.dl/ pcv<15%
CLINICAL:
Impaired conciousness/coma
Prostration
Failure to feed
Multiple convulsions(>2/24hrs)
Acidotic breathing
Circulatory collapse(SBP <50mm )
Clinical jaundice/ other otrgan dysfunction
Abnormal spon. bleeding
Complicated / severe malaria QUININE:
20mg/kg of quinine salt in 10 ml of dns/ isotonic sol. Over 4 hrs f/w
10mg/ kg over 2 hrs repeated 8th hrly til he takes orally then orally for 7 days.
(+) single dose of primaquine
ARTESUNATE:
2.4 mg/kg iv stat then 12 & 24hrs FOLLOWED by oral combination with
artemeether + lumefantrine for 7 days.
Supportive therapiesAntibiotics:- tetracycline, doxycycline etc..,
Anticonvulsants:-
should be administered for seizures lasting more than 5mins,
benzodiazepines-mostly used,
other anticonvulsants-paraldehyde, phenytoin, phenobarbitone, fosphenytoin, etc,
Blood transfusions is life saving in severe malarial anemia
Exchange transfusions has thought to benefit patients with high parasite count
rationale is to remove parasite burden,( >20%)
to reduce antigen load,
to remove parasite derived toxins and metabolites and
to correct anemia.
Dialysis:- indicated in case of acute renal failure due to severe falciparum malaria,
Rapidly raise of creatinine level-most sensitive indicator.
Inotropic support:- shock- algid malaria,
Dopamine is used
Send blood culture and start on iv antibiotics.
Hypoglycemia:-
any blood sugar <40mg/dL should be treated with 5ml/kg of 10% dextrose IV
Raised intracranial pressure:- mannitol
Ventilation:-
Prevention