Embed Size (px)
Citation preview

MalnutritionMalnutrition

WHO definitionWHO definition
““The cellular imbalance between The cellular imbalance between supply of nutrients and energy and supply of nutrients and energy and the body's demand for them to the body's demand for them to ensure growth, maintenance, and ensure growth, maintenance, and specific functions." specific functions."

Malnutrition (“hypotrophy” in Russian-Malnutrition (“hypotrophy” in Russian-language literature) is a part of larger language literature) is a part of larger group of disorders, chronic disorders group of disorders, chronic disorders
of nutrition (CDN). This group includes of nutrition (CDN). This group includes malnutrition and adiposity. The current malnutrition and adiposity. The current
lecture is only devoted to the first lecture is only devoted to the first disorder, malnutrition. disorder, malnutrition.

ClassificationClassification
Weight deficit classification: Weight deficit classification: 11stst degree – weight deficit 10-20% degree – weight deficit 10-20% 22ndnd degree – weight deficit 20-30% degree – weight deficit 20-30% 33rdrd degree - weight deficit degree - weight deficit > > 30%30%

The 3The 3rdrd degreedegree malnutrition includes malnutrition includes two conditions, two conditions,
kkwashiorkor and marasmus.washiorkor and marasmus.

ClassificationClassification
acute acute ((weight is primarily affectedweight is primarily affected)) chronicchronic ((proportionate reduction in proportionate reduction in
weight and height) weight and height)

ClassificationClassification
Primary (inadequate food intake)Primary (inadequate food intake) Secondary (increased nutrient Secondary (increased nutrient
needs, decreased nutrient needs, decreased nutrient absorption, and/or increased absorption, and/or increased nutrient losses)nutrient losses)

ClassificationClassification
Height deficit classification: Height deficit classification: 11stst degree – height deficit 5-10%, degree – height deficit 5-10%, 22ndnd degree – height deficit 10-15% degree – height deficit 10-15% 33rdrd degree – height deficit degree – height deficit > 15> 15%%

The main, most often seen variant The main, most often seen variant of 3of 3rdrd degree malnutrition is protein degree malnutrition is protein--energy malnutrition (PEM).energy malnutrition (PEM).
As a rule, concurrent deficiency ofAs a rule, concurrent deficiency of iron, iodine, zinc, and vitamin Airon, iodine, zinc, and vitamin A is is also seen.also seen.

Kwashiorkor vs. marasmusKwashiorkor vs. marasmus
edematous edematous nonedematousnonedematous
fair-to-normal calorie fair-to-normal calorie intake with inadequate intake with inadequate protein intakeprotein intake
inadequate intake of inadequate intake of protein and caloriesprotein and calories
dysadaptation to dysadaptation to starvationstarvation
adaptation to adaptation to starvationstarvation
marasmicmarasmic kwashiorkorkwashiorkor

EtiologyEtiology
1) Alimentary factors1) Alimentary factors: : quantitative undernutrition (hypogalactia, quantitative undernutrition (hypogalactia,
administration of insufficient quantity of administration of insufficient quantity of mixtures) mixtures)
qualitative undernutrition (insufficiency of qualitative undernutrition (insufficiency of proteins, vitamins, trace elements).proteins, vitamins, trace elements).
Poverty and ignorancePoverty and ignorance , feeding habits, , feeding habits, early early cessation of breastfeeding…cessation of breastfeeding…

EtiologyEtiology
2) Infections (greater demands, protein loss, 2) Infections (greater demands, protein loss, food restriction):food restriction):
diarrheadiarrhea malaria, measles, etc.malaria, measles, etc. sepsis, pyelonephritis and urinary tract sepsis, pyelonephritis and urinary tract
infections, other foci of infectioninfections, other foci of infection

EtiologyEtiology
Chronic illnesses: Chronic illnesses: – Children with chronic illnesses frequently have Children with chronic illnesses frequently have
anorexia, which leads to inadequate food anorexia, which leads to inadequate food intake. intake.
– Increased inflammatory burden and increased Increased inflammatory burden and increased metabolic demands can increase caloric need. metabolic demands can increase caloric need.
– Any chronic illness that involves the liver or Any chronic illness that involves the liver or small bowel affects nutrition adversely by small bowel affects nutrition adversely by impairing digestive and absorptive functions. impairing digestive and absorptive functions.

EtiologyEtiology
– Cystic fibrosis Cystic fibrosis – Chronic renal failure Chronic renal failure – Childhood malignancies Childhood malignancies – Congenital heart disease Congenital heart disease – Neuromuscular diseases Neuromuscular diseases – Chronic inflammatory bowel diseases Chronic inflammatory bowel diseases

EtiologyEtiology
Anorexia because of perinatal or other Anorexia because of perinatal or other brain diseases, unfavorable factors of brain diseases, unfavorable factors of surroundings, neuroses.surroundings, neuroses.
Malformations of mouth, gastrointestinal Malformations of mouth, gastrointestinal tract such as ileus, pylorostenosis etc.tract such as ileus, pylorostenosis etc.
Syndrome of "short bowel" after extensive Syndrome of "short bowel" after extensive intestinal resections.intestinal resections.

EtiologyEtiology
Syndromes of malabsorption (intolerance of Syndromes of malabsorption (intolerance of lactose, saccharose, glucose, protein of cow or lactose, saccharose, glucose, protein of cow or soya milk; celiac disease, cystic fibrosis of soya milk; celiac disease, cystic fibrosis of pancreas, exudative enteropathy, enteropathic pancreas, exudative enteropathy, enteropathic acrodermatitis, atrophy of villi of small intestine.acrodermatitis, atrophy of villi of small intestine.
Hereditary anomalies of metabolism Hereditary anomalies of metabolism (galactosemia, leucinosis, fructosemia, diseases (galactosemia, leucinosis, fructosemia, diseases of Niman-Pick, Tey-Saks), immunodeficiencies of Niman-Pick, Tey-Saks), immunodeficiencies (predominantly of T-system).(predominantly of T-system).

Pathophysiology:Pathophysiology:
Inadequate intakes Inadequate intakes →→ decreased activity decreased activity and energy expenditureand energy expenditure →→ However, fat However, fat stores are mobilized stores are mobilized →→ protein catabolism. protein catabolism.
Activation of sympatho-adrenal system Activation of sympatho-adrenal system (chronic stress).(chronic stress).
Hypoproteinemia, hypoglycemia, acidosis, Hypoproteinemia, hypoglycemia, acidosis, hypokalemia, hyponatremia,hypocalcemia, hypokalemia, hyponatremia,hypocalcemia, hypophosphatemia.hypophosphatemia.

Pathophysiology:Pathophysiology:
Immune system: Immune system: Loss of delayed hypersensitivity;Loss of delayed hypersensitivity; Impaired lymphocyte response;Impaired lymphocyte response; Impaired phagocytosis (secondary to decreased Impaired phagocytosis (secondary to decreased
complement and certain cytokines);complement and certain cytokines); Decreased secretory immunoglobulin A (IgA);Decreased secretory immunoglobulin A (IgA); Mimic AIDS Mimic AIDS (deficit of T-helpers, activity of T-(deficit of T-helpers, activity of T-
suppressors is normal or slightly decreased).suppressors is normal or slightly decreased).

Pathophysiology:Pathophysiology:
Brain development:Brain development: slowed rate of growth of the brain, slowed rate of growth of the brain, lower brain weight, lower brain weight, thinner cerebral cortex, thinner cerebral cortex, decreased number of neurons, decreased number of neurons, insufficient myelinization, insufficient myelinization, changes in the dendritic spines.changes in the dendritic spines.

Pathophysiology:Pathophysiology:
Degeneration of the liver and heartDegeneration of the liver and heart Atrophy of the small bowelAtrophy of the small bowel Decreased intravascular volume leading to Decreased intravascular volume leading to
secondary hyperaldosteronism. secondary hyperaldosteronism. AnemiaAnemia Decreased activity of gastric, intestine, Decreased activity of gastric, intestine,
pancreatic enzymespancreatic enzymes

Frequency:Frequency:
In the US: In the US: Total - Total - <<1%. 1%. Highest risk group (children in shelters for Highest risk group (children in shelters for
the homeless) the homeless) << 10%, 10%, Children in rural areas - 10% of. Children in rural areas - 10% of. Hospitalized children - ¼ acute PEM and Hospitalized children - ¼ acute PEM and
27% chronic PEM. 27% chronic PEM.

Frequency:Frequency:
20-30% of infants in developing countries 20-30% of infants in developing countries have PEM have PEM
More than half of young children in South More than half of young children in South Asia have PEM, Asia have PEM,
In sub-Saharan Africa, 30% of children have In sub-Saharan Africa, 30% of children have PEM. PEM.

Mortality:Mortality:
Malnutrition is directly responsible for Malnutrition is directly responsible for 300,000 deaths per year in children younger 300,000 deaths per year in children younger than 5 years in developing countries and than 5 years in developing countries and contributes indirectly to over half the deaths contributes indirectly to over half the deaths in childhood worldwide. in childhood worldwide.

Risk of sudden deathRisk of sudden death
HypothermiaHypothermia HypoglycemiaHypoglycemia DyselectrolytemiaDyselectrolytemia Diarrhea and dehydrationDiarrhea and dehydration Congestive cardiac failureCongestive cardiac failure InfectionsInfections

Clinical ManifestationsClinical Manifestations
11stst degree degree 22ndnd degree degree 33rdrd degree degree
Weight Weight deficitdeficit
10-20%10-20% 20-30%20-30% >30%>30%
CNSCNS IrritationIrritation SlowdownSlowdown Severe Severe slowdownslowdown
AppetiteAppetite ↑↑or or ↓↓ ↓↓ AnorexiaAnorexia
GI enzymes GI enzymes Slightly Slightly ↓↓ ↓↓ Severely Severely ↓↓
SkinSkin Pale Pale Pale, dryPale, dry Flaccid, dryFlaccid, dry

Clinical Manifestations Clinical Manifestations (continued)(continued)
11stst degree degree 22ndnd degree degree 33rdrd degree degree
S/c fatS/c fat Absent on Absent on abdomenabdomen
Absent on Absent on extremitiesextremities
Absent on Absent on faceface
TurgorTurgor Decreased Decreased Severely Severely decreaseddecreased
Absent Absent
ImmunityImmunity Preserved Preserved Impaired Impaired Severely Severely impairedimpaired
Weight Weight gaingain
Slowed downSlowed down Almost Almost absentabsent
Weight Weight lossloss

Clinical ManifestationsClinical Manifestations
Marasmus:Marasmus: Failure to gain weight and irritability Failure to gain weight and irritability →→weight loss weight loss
and listlessness and listlessness → → emaciation. emaciation. Skin turgor loss (extremitiesSkin turgor loss (extremities→trunk→face) →trunk→face) Distended or flat abdomen with the intestinal Distended or flat abdomen with the intestinal
pattern.pattern. Muscle atrophy Muscle atrophy →→ hypotonia. hypotonia. Subnormal temperature and slow pulse. Subnormal temperature and slow pulse. Constipation or starvation diarrhea (frequent small Constipation or starvation diarrhea (frequent small
stools with mucus).stools with mucus).

Clinical ManifestationsClinical Manifestations
KwashiorkorKwashiorkor initially lethargy, apathy, or irritability. initially lethargy, apathy, or irritability. inadequate growth, loss of muscle tissue, inadequate growth, loss of muscle tissue,
increased susceptibility to infections, increased susceptibility to infections, vomiting, diarrhea, anorexia, flabby vomiting, diarrhea, anorexia, flabby subcutaneous tissues, subcutaneous tissues,
Edema (internal organs Edema (internal organs → → in the face and in the face and limbs),limbs),

Clinical ManifestationsClinical Manifestations
Kwashiorkor (continued)Kwashiorkor (continued) Dermatitis (darkening of the skin in irritated Dermatitis (darkening of the skin in irritated
areas but not in areas exposed to sunlight, areas but not in areas exposed to sunlight, depigmentation depigmentation
Sparse and thin hair.Sparse and thin hair. Enlarged liver (edema and fatty infiltration)Enlarged liver (edema and fatty infiltration) Eventually Eventually →→ stupor, coma, and death. stupor, coma, and death.

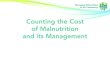
Kwashiorkor in a 2 yr old boyKwashiorkor in a 2 yr old boy
Generalized edema, Generalized edema,
Typical skin lesions, Typical skin lesions,
State of prostration. State of prostration.

Clinical ManifestationsClinical Manifestations
Behavioral changes : Behavioral changes : o Irritability, Irritability, oapathy, apathy, odecreased social responsiveness, decreased social responsiveness, oanxiety, anxiety, oattention deficits attention deficits

Clinical ManifestationsClinical Manifestations
– IronIron - Fatigue, anemia, decreased cognitive - Fatigue, anemia, decreased cognitive function, headache, glossitis, and nail changes function, headache, glossitis, and nail changes
– IodineIodine - Goiter, developmental delay, and - Goiter, developmental delay, and mental retardation mental retardation
– Vitamin DVitamin D - Poor growth, rickets, and - Poor growth, rickets, and hypocalcemia hypocalcemia
– Vitamin AVitamin A - Night blindness, xerophthalmia, - Night blindness, xerophthalmia, poor growth, and hair changes poor growth, and hair changes

Clinical ManifestationsClinical Manifestations
– FolateFolate - Glossitis, anemia (megaloblastic), and - Glossitis, anemia (megaloblastic), and neural tube defects (in fetuses of women neural tube defects (in fetuses of women without folate supplementation) without folate supplementation)
– ZincZinc - Anemia, dwarfism, hepatosplenomegaly, - Anemia, dwarfism, hepatosplenomegaly, hyperpigmentation and hypogonadism, hyperpigmentation and hypogonadism, acrodermatitis enteropathica, diminished acrodermatitis enteropathica, diminished immune response, poor wound healing immune response, poor wound healing

Lab StudiesLab Studies
o Complete blood count (CBC) – anemia, ESR, Complete blood count (CBC) – anemia, ESR, WBC. WBC.
o Serum electrolytes, Serum electrolytes, o Urinalysis and culture. Urinalysis and culture. o Stool specimens Stool specimens o Protein nutritional status - serum albumin, Protein nutritional status - serum albumin,
creatinine, and BUN levels. creatinine, and BUN levels. o Retinol-binding protein, prealbumin, and Retinol-binding protein, prealbumin, and
transferrin have short half-life.transferrin have short half-life.

Additional Additional Lab StudiesLab Studies
Thyroid functions or sweat chloride testsThyroid functions or sweat chloride tests Evaluation of renal functionEvaluation of renal function Celiac serology (IgA and IgG to gluten) Celiac serology (IgA and IgG to gluten) Chest X-rayChest X-ray ECG (ECG (ST depression, T waves inversion - ST depression, T waves inversion -
potassium deficit)potassium deficit) Other cultures (blood, throat, nasopharynx)Other cultures (blood, throat, nasopharynx)

ManagementManagement
Appropriate diet is crucial Appropriate diet is crucial 1st grade – at home,1st grade – at home, 22ndnd and 3 and 3rdrd grade – hospitalization. grade – hospitalization. Finding and managing the cause!Finding and managing the cause! ““Younger” food.Younger” food.

ManagementManagement
Frequency of feeding: Frequency of feeding: 11stst degree – 7 times / day; degree – 7 times / day; 22ndnd degree – 8 times / day; degree – 8 times / day; 33rdrd degree – 10 times / day. degree – 10 times / day.

ManagementManagement
Breast milk is the choice;Breast milk is the choice; Other choices – highly adapted milk Other choices – highly adapted milk
formulas, in cases of intolerance - formulas, in cases of intolerance - without lactase formulas or soy milk-without lactase formulas or soy milk-based formulas.based formulas.
Two stages of feeding – tolerance and Two stages of feeding – tolerance and high caloric feeding. high caloric feeding.

Diet for 1Diet for 1stst grade grade
Period of tolerance – 1-3 days;Period of tolerance – 1-3 days; Calculations of protein, carbohydrates, fat and Calculations of protein, carbohydrates, fat and
calories is made for the due body weight:calories is made for the due body weight:
ProteinProtein Carbohyd-Carbohyd-ratesrates
FatFat CaloriesCalories
2,5 – 3,5 2,5 – 3,5 g/kgg/kg
12 – 13 12 – 13 g/kgg/kg
5,5 – 6 g/kg5,5 – 6 g/kg 110 – 120 110 – 120 kcal/kgkcal/kg

Diet of 2Diet of 2ndnd grade grade
Period of tolerance – 1 week;Period of tolerance – 1 week; Calculations of protein and Calculations of protein and
carbohydrates is made for the due carbohydrates is made for the due body weight; calculation of fat is made body weight; calculation of fat is made for the real weight;for the real weight;
Volume of food starts from ½ of the Volume of food starts from ½ of the calculated amount.calculated amount.

Diet of 3Diet of 3rdrd grade grade
Period of tolerance – 2-3 weeks;Period of tolerance – 2-3 weeks; Calculations of protein and Calculations of protein and
carbohydrates is made for the real + carbohydrates is made for the real + 20% body weight; calculation of fat is 20% body weight; calculation of fat is made for the real weight;made for the real weight;
Volume of food starts from 1/3 of the Volume of food starts from 1/3 of the calculated amount.calculated amount.

ManagementManagement
11stst phase - 24-48 hr - stabilization phase - 24-48 hr - stabilization.. Dehydration is corrected (oral rehydration Dehydration is corrected (oral rehydration
therapy is preferred; 10% glucose; therapy is preferred; 10% glucose; Increased total body water and decreased Increased total body water and decreased trace minerals; intravascular dehydration);trace minerals; intravascular dehydration);
Antibiotic therapy is initiated if neededAntibiotic therapy is initiated if needed Magnezium, potassium, vitamins BMagnezium, potassium, vitamins B

ManagementManagement
22ndnd phase - week to 10 days – diet tolerance phase - week to 10 days – diet tolerance Continued antibiotic therapy Continued antibiotic therapy Diet (-75 cal/kg and ~1 g/kg/24hr of protein) Diet (-75 cal/kg and ~1 g/kg/24hr of protein) Electrolytes, trace minerals, and vitamins.Electrolytes, trace minerals, and vitamins. Nasogastric tube is preferred to parenteral Nasogastric tube is preferred to parenteral
route.route. Easily assimilated food, frequent meals. Easily assimilated food, frequent meals.

ManagementManagement
33rdrd phase - week to 10 days – high-caloric phase - week to 10 days – high-caloric dietdiet
Diet (up to 150 kcal/kg/24 hr and 4 g/kg/24 Diet (up to 150 kcal/kg/24 hr and 4 g/kg/24 hr of protein). After adjustment the child can hr of protein). After adjustment the child can be fed ad libitum. be fed ad libitum.
Iron therapy (otherwise free iron will bind Iron therapy (otherwise free iron will bind limited stores of transferrin and exacerbate limited stores of transferrin and exacerbate oxidant damage), oxidant damage),
Vitamins, zink.Vitamins, zink.

ManagementManagement
Care taker education;Care taker education; Psychological attention to child;Psychological attention to child; Warming of the child;Warming of the child; Massages and physical activity (except 3Massages and physical activity (except 3rdrd
grade);grade); Outdoors time;Outdoors time; Frequent follow-upFrequent follow-up

Prophylaxis is better!Prophylaxis is better!

Thank youThank you














![Malnutrition [Autosaved]](https://img.pdfslide.net/doc/110x75/577cd2051a28ab9e7895192c/malnutrition-autosaved.jpg)













