Embed Size (px)
DESCRIPTION
Author: Abdulaziz Rajeh Alanzi
Citation preview

Management & Complications of stroke
Mr.Abdulaziz R. Alanzi
Medical Student, Al-Imam University
Riyadh – Saudi Arabia

References
UpToDate Electronic Medical Database
Harrison's Principles of Internal Medicine Book,18e, Dan L. Longo, Anthony S. Fauci, Dennis L. Kasper, Stephen L. Hauser, J. Larry Jameson, Joseph Loscalzo, Eds.

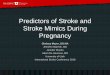
Management
Medical management of stroke and TIA. Rounded boxes are diagnoses; rectangles are interventions. Numbers are percentages of stroke overall. ABCs, airway, breathing, circulation; BP, blood pressure; CEA, carotid endarterectomy; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage; TIA, transient ischemic attack.

Management: Acute Ischemic Strokefalls within six categories
(1) Medical support: optimize cerebral perfusion in the surrounding ischemic penumbra
(2) IV thrombolysis: recombinant tPA
(3) Endovascular techniques: Intraarterial administration of a thrombolytic agent
(4) Antithrombotic treatment: Platelet Inhibition & Anticoagulation
(5) Neuroprotection: providing a treatment that prolongs the brain's tolerance to ischemia
(6) Stroke centers and rehabilitation

Management: Acute Ischemic Stroke
Medical support:
if blood pressure is >185/110 mm Hg –-< B1-adrenergic blocker (esmolol)
Fever –-< antipyretics and surface cooling
Serum glucose <6.1 mmol/L (110 mg/dL) –-< insulin infusion
Cerebral Edema –-< Water restriction and IV mannitol
Feeding –-< NGT
Sphincters –-< Foleys Catheter

Management: Acute Ischemic Stroke
IV thrombolysis:
Administration of rtPA Intravenous access with two peripheral IV lines (avoid arterial or central line placement)Review eligibility for rtPAAdminister 0.9 mg/kg IV (maximum 90 mg) IV as 10% of total dose by bolus, followed by remainder of total dose over 1 hFrequent cuff blood pressure monitoringNo other antithrombotic treatment for 24 hFor decline in neurologic status or uncontrolled blood pressure, stop infusion, give cryoprecipitate, and reimage brain emergentlyAvoid urethral catheterization for 2 h


Management: Acute Ischemic Stroke
Endovascular techniques :

Management: Acute Ischemic Stroke
Antithrombotic treatment:- Platelet inhibition: Aspirin is the only antiplatelet agent that has been proven
effective for the acute treatment of ischemic stroke; there are several antiplatelet agents proven for the secondary prevention of stroke.
- Anticoagulation: Trials generally have shown an excess risk of brain and systemic hemorrhage with acute anticoagulation. Therefore, trials do not support the routine use of heparin or other anticoagulants for patients with atherothrombotic stroke.
Neuroprotection: Drugs that block the excitatory amino acid pathways have been shown to protect neurons and glia in animals. Hypothermia is a powerful neuroprotective treatment in patients with cardiac arrest and is neuroprotective in animal models of stroke, but it has not been adequately studied in patients with ischemic stroke.

Management: Acute Ischemic Stroke
Stroke centers and rehabilitation:Proper rehabilitation of the stroke patient includes early physical, occupational, and speech therapy. It is directed toward educating the patient and family about the patient's neurologic deficit, preventing the complications of immobility (e.g., pneumonia, DVT and pulmonary embolism, pressure sores of the skin, and muscle contractures).
The goal of rehabilitation is to return the patient to home and to maximize recovery by providing a safe, progressive regimen suited to the individual patient. Additionally, the use of restraint therapy (immobilizing the unaffected side) has been shown to improve hemiparesis following stroke.

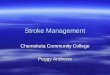
Complication PercentFalls 25Urinary tract infection 24Chest infection 22Pressure sores 21Depression 16Shoulder pain 9Deep venous thrombosis 2Pulmonary embolism 1
Medical complications of stroke were frequent in a prospective multicenter study of 311 patients followed weekly through hospital discharge and again at 6, 18, and 30 months after stroke.Data from: Langhorne, P, Stott, DJ, Robertson, L, et al. Medical complications after stroke: a multicenter study. Stroke 2000; 31:1223.
Complications of strokeCommon medical complications of stroke

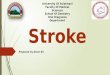
Complications of strokeSerious medical complications of stroke
In a prospective study that analyzed the placebo group of the RANTTAS database (n = 279), at least one serious medical complication (defined as prolonged, immediately life threatening, or resulting in hospitalization or death) occurred in 24 percent of patients.Data from: Johnston, KC, Li, JY, Lyden, PD, et al. Medical and neurological complications of ischemic stroke: experience from the RANTTAS trial. RANTTAS Investigators. Stroke 1998; 29:447.
Complication Percent
All pneumonias 5
Aspiration pneumonia alone 3
Heart failure 3
Gastrointestinal bleeding 3
Cardiac arrest 2
Angina/MI/cardiac ischemia 1
Deep venous thrombosis 1
Pulmonary embolism 1
Hypoxia 1
Urinary tract infection 1
Sepsis 1
Cellulitis 1
Peripheral vascular disorder 1
Dyspnea 1
Pulmonary edema 1
Dehydration 1