Embed Size (px)
Citation preview
Management for locking compression plate/ dynamic
compression plate implant failure in non union osteoporotic
humerus shaft bone fracture

ww.sciencedirect.com
a p o l l o m e d i c i n e x x x ( 2 0 1 5 ) 1e4
Available online at w
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
Original Article
Management for locking compression plate/dynamic compression plate implant failure in nonunion osteoporotic humerus shaft bone fracture
Mohammed Iftekar Ali
Apollo Reach Hospital, Karimnagar, India
a r t i c l e i n f o
Article history:
Received 30 October 2014
Accepted 9 April 2015
Available online xxx
Keywords:
Humerus
Nonunion
Interlocking
Nail
Osteoporosis
E-mail address: [email protected]://dx.doi.org/10.1016/j.apme.2015.04.0010976-0016/Copyright © 2015, Indraprastha M
Please cite this article in press as: Ali Mfailure in non union osteoporotic hj.apme.2015.04.001
a b s t r a c t
Introduction: To introduce the experience of treating nonunion osteoporotic of humeral
fractures with interlocking nailing for failed surgical treatment by plating. Etiology for non-
union after failed surgical management of humeral shaft fractures is multi-factorial.
Following factors may play a role in nonunion e inadequate fracture fixation with poor
contact between the fracture segments, osteomalacia, osteoporosis, infection, devitaliza-
tion of bone and many more.
Materials and methods: A retrospective comparative study of twenty four patients who
had locking compression plate failure in osteoporotic humerus shaft fractures treated with
interlocking nail and iliac crest bone graft at Gandhi Hospital from 2007 to 2010.
Results: Twenty extremities had a return to nearly normal function within twelve weeks
after nailing. According to Rommens criteria excellent results seen in 79.2%, moderate
16.7%, poor 4.1%. The mean Constant-Murley score improved from pre operative 45.9 ± 17.6
to 79.1 ± 12.6 (p < 0.001) post operative.
Conclusion: Interlocking intramedullary nailing of the humerus provides immediate sta-
bility and can be accomplished with a closed technique, brief operative time, and mini-
mum morbidity, with a resultant early return of function to the extremity.
LEVEL OF EVIDENCE: iii retrospective cohort study.
Copyright © 2015, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
Osteoporotic humeral nonunion resulting after operative
intervention of plate fixation presents a different set of prob-
lems like broken or loosened implants, scarred tissues, avas-
cular bone ends and sometimes deep seated infection.1,2
Loosened screws cause osteolysis at the hole sites and loss
of local bone substance. The cortex underneath the plate
o.uk.
edical Corporation Ltd. A
I, Management for lockumerus shaft bone fr
becomes sclerotic and avascular. In such a complicated con-
dition replating becomes even more difficult and enough
stability may not be achieved. In addition, dissection and
periosteal damage further decreases the viability of the bone
ends and puts radial nerve at a high risk of injury. The major
technical problem the surgeon faces is the difficulty to pro-
duce secure fixation of the implant to the bone. The common
mode of failure of internal fixation in osteoporotic bone is
ll rights reserved.
ing compression plate/dynamic compression plate implantacture, Apollo Medicine (2015), http://dx.doi.org/10.1016/

Table 2 e Final results According to Rommen's criteria.
Result No. of cases %
Excellent 19 79.2
Moderate 4 16.7
Poor 1 4.1
a p o l l o m e d i c i n e x x x ( 2 0 1 5 ) 1e42
bone failure rather than implant breakage. Rosen has defined
a delay of 3e4months inbony healing as a delayed union and a
delay of 6e8 months as a non-union.3
The high rate of complications has encouraged extensive
research into the development of implants that improve the
bone-implant interface by preventing high bone strain and
distributing the force to the bone in a load-sharing rather than
load-bearing configuration. Intramedullary nails are load
sharing and provide relative stability. They seem to be the
most efficient method of reducing strain at the bone-implant
interface. Cancellous or corticocancellous bone autografts to
assist fracture healing are probably still the best.
2. Materials & methods
A retrospective study of Twenty four cases of failure fixation
in non union osteoporotic fracture shaft humerus, were sta-
bilised with the interlocking nail and iliac crest bone
graft.1,2,4e7 Therewere 10male {41.66%) and 14 female (58.33%)
patients. All patients (Table 2) had atrophic nonunion of the
humerus except two. The right side was affected in 14 cases
[58.3%], and left 10 cases [41.7%]. The nonunion was in the
upper third of the humerus diaphysis in four cases (16.6%),
middle third in 18 cases [75%), and lower third in two cases
(8.3%). The original fracture was close in 20 cases (83.3% and
open in 4 cases (16.7%). In 4 cases (16.7%), there was history of
infection after the index surgery, however, active infection
was controlled by debridement and antibiotics. Autogenous
Iliac crest bone graft (ICBG) was performed in all cases. Our
inclusion criteria are all patient older than 50 year with failed
surgical fixation. Our exclusion criteria are fresh fracture and
young patient. All surgery were performed by single surgeon.
Average duration of surgery is one hour. All women and men
older than 50 years with low energy fracture were subjected to
BMD testing. The gold standard method is DEXA scan {dual
energy X-ray absorptiometry}.In our study hip, spine, forearm
were evaluated. In our study average mean T-score is �2.5,
serum vitaminD3 level is <50 nmol/L (<20 ng/mL) at 1st sur-
gery (Table 3).
2.1. Operative procedure: interlocking nail
The previous operative scar was used to approach the fracture
site. Implant removal is done. Debridement of non union site
is done followed by trimming and decortications of bone ends
were done.1,2,4 A longitudinal skin incision is made from the
most lateral point of the acromion. Using the small curved
Table 1 e Postoperative complications.
Complication No. of cases % (in comparison to all cases)
Immediate
Superficial
Infection 1 4.1
Delayed
Shoulder 4 16.6
Dysfunction
Non Union 1 4.1
Please cite this article in press as: Ali MI, Management for lockfailure in non union osteoporotic humerus shaft bone frj.apme.2015.04.001
awl, the entry portal is established, Interloking nail is inserted,
proximal and distal lockingwas done. Anterior iliac crest bone
grafts were used in all cases.
Post Operative Care.
� Antibiotics i.v for 3 days
� Universal shoulder immobiliser is given
� Suture removal on 10th day
� Assisted active ROM exercises for wrist & hand from 1st
post operative day
� Active assisted shoulder & elbow exercises started after 2
weeks
� 5 mg Zoledronic acid infusion was given two weeks after
surgery followed by yearly once for three years with
maintenance calcium citrate 500 mg once a day. It should
be given two weeks after surgery because delay dosing
would potentially increase the quantity of zoledronic acid
binding to the target area, leading to a greater anti catabolic
effect with the same dose. Second delayed administration
would allow the initial endogenous anabolic and catabolic
response to establish themselves before dose administra-
tion. Zoledronic acid administered as a 5 mg intravenous
infusion annually increases bone mineral density in the
lumbar spine and femoral neck by 6.7% and 5.1% respec-
tively and reduces the incidence of new vertebral and hip
fractures by 70% and 41%. Most common side effects are
post-dose fever, flu-like symptoms, myalgia, arthralgia,
and headache which usually occur in the first 3 days after
infusion and are self-limited. Rare adverse effects include
renal dysfunction, hypocalcemia, atrial fibrillation, and
osteonecrosis of the jaw.
3. Results
There were 24 cases with mean age of 63.29 years.
The mean time of radiological bone healing was 4.2
months (range three to seven months). Sound bone healing
was achieved in all cases except one (4.1%). Result of case1
was shown in Fig. 1a, b, c.The number of cases available for
follow up is twenty four and duration of follow up is eighteen
months. According to the to Rommen's Criteria, the functional
outcome was excellent in 19cases (79.2%), moderate in four
cases (16.7%), poor in one case [4.1%] which was treated by
Ilizarov ring fixator. Therewere no cases of iatrogenic nerve or
vascular injury due to surgery. There was good relief of pain
within two weeks after nailing procedures and excellent relief
after five weeks. All patients had improvement in the func-
tional use of the extremity after fixation. No patient noted any
limitation of motion of the elbow. The range of motion of the
shoulder was documented numerically for eleven patients,
who had a mean of 101� (range, 55e180�) of abduction and 98�
ing compression plate/dynamic compression plate implantacture, Apollo Medicine (2015), http://dx.doi.org/10.1016/
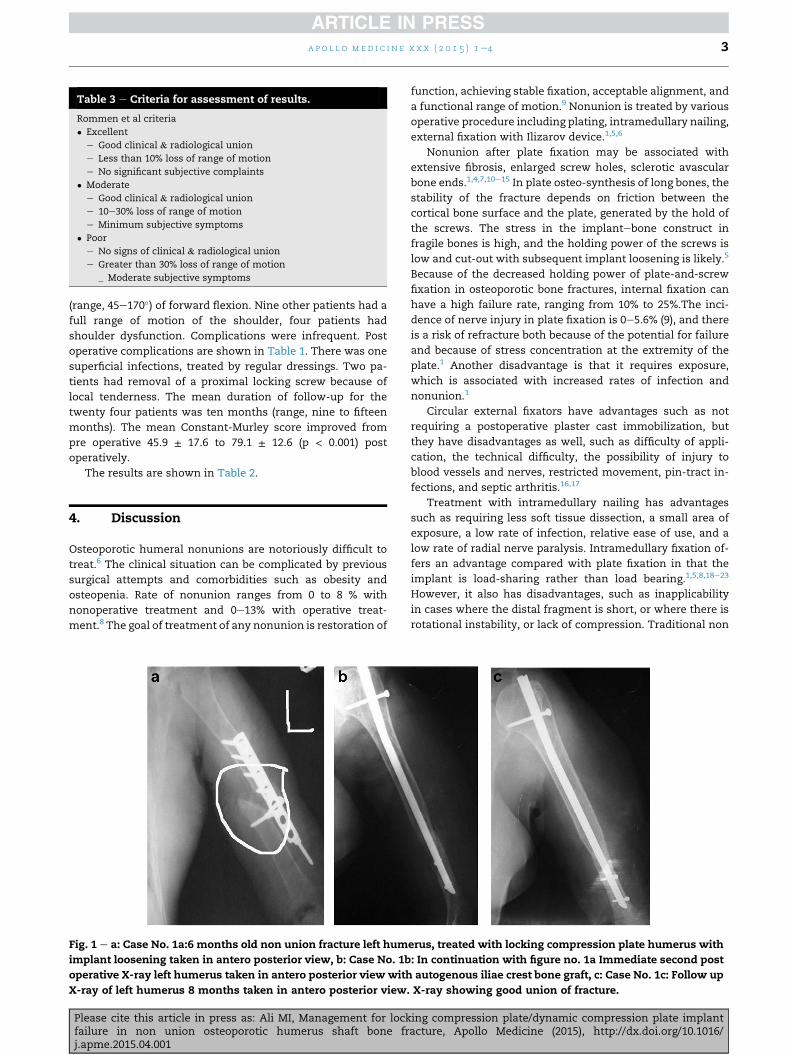
Table 3 e Criteria for assessment of results.
Rommen et al criteria
� Excellent
e Good clinical & radiological union
e Less than 10% loss of range of motion
e No significant subjective complaints
� Moderate
e Good clinical & radiological union
e 10e30% loss of range of motion
e Minimum subjective symptoms
� Poor
e No signs of clinical & radiological union
e Greater than 30% loss of range of motion
_ Moderate subjective symptoms
a p o l l o m e d i c i n e x x x ( 2 0 1 5 ) 1e4 3
(range, 45e170�) of forward flexion. Nine other patients had a
full range of motion of the shoulder, four patients had
shoulder dysfunction. Complications were infrequent. Post
operative complications are shown in Table 1. There was one
superficial infections, treated by regular dressings. Two pa-
tients had removal of a proximal locking screw because of
local tenderness. The mean duration of follow-up for the
twenty four patients was ten months (range, nine to fifteen
months). The mean Constant-Murley score improved from
pre operative 45.9 ± 17.6 to 79.1 ± 12.6 (p < 0.001) post
operatively.
The results are shown in Table 2.
4. Discussion
Osteoporotic humeral nonunions are notoriously difficult to
treat.6 The clinical situation can be complicated by previous
surgical attempts and comorbidities such as obesity and
osteopenia. Rate of nonunion ranges from 0 to 8 % with
nonoperative treatment and 0e13% with operative treat-
ment.8 The goal of treatment of any nonunion is restoration of
Fig. 1 e a: Case No. 1a:6 months old non union fracture left hum
implant loosening taken in antero posterior view, b: Case No. 1b
operative X-ray left humerus taken in antero posterior view with
X-ray of left humerus 8 months taken in antero posterior view.
Please cite this article in press as: Ali MI, Management for lockfailure in non union osteoporotic humerus shaft bone frj.apme.2015.04.001
function, achieving stable fixation, acceptable alignment, and
a functional range of motion.9 Nonunion is treated by various
operative procedure including plating, intramedullary nailing,
external fixation with Ilizarov device.1,5,6
Nonunion after plate fixation may be associated with
extensive fibrosis, enlarged screw holes, sclerotic avascular
bone ends.1,4,7,10e15 In plate osteo-synthesis of long bones, the
stability of the fracture depends on friction between the
cortical bone surface and the plate, generated by the hold of
the screws. The stress in the implantebone construct in
fragile bones is high, and the holding power of the screws is
low and cut-out with subsequent implant loosening is likely.5
Because of the decreased holding power of plate-and-screw
fixation in osteoporotic bone fractures, internal fixation can
have a high failure rate, ranging from 10% to 25%.The inci-
dence of nerve injury in plate fixation is 0e5.6% (9), and there
is a risk of refracture both because of the potential for failure
and because of stress concentration at the extremity of the
plate.1 Another disadvantage is that it requires exposure,
which is associated with increased rates of infection and
nonunion.1
Circular external fixators have advantages such as not
requiring a postoperative plaster cast immobilization, but
they have disadvantages as well, such as difficulty of appli-
cation, the technical difficulty, the possibility of injury to
blood vessels and nerves, restricted movement, pin-tract in-
fections, and septic arthritis.16,17
Treatment with intramedullary nailing has advantages
such as requiring less soft tissue dissection, a small area of
exposure, a low rate of infection, relative ease of use, and a
low rate of radial nerve paralysis. Intramedullary fixation of-
fers an advantage compared with plate fixation in that the
implant is load-sharing rather than load bearing.1,5,8,18e23
However, it also has disadvantages, such as inapplicability
in cases where the distal fragment is short, or where there is
rotational instability, or lack of compression. Traditional non
erus, treated with locking compression plate humerus with
: In continuation with figure no. 1a Immediate second post
autogenous iliae crest bone graft, c: Case No. 1c: Follow up
X-ray showing good union of fracture.
ing compression plate/dynamic compression plate implantacture, Apollo Medicine (2015), http://dx.doi.org/10.1016/

a p o l l o m e d i c i n e x x x ( 2 0 1 5 ) 1e44
reamed nails, such as Ender and Rush nails, and reamed
Kuntscher nails do not achieve sufficient stability, particularly
in rotation. Stability, rotational stability in particular, can be
achieved with locked intramedullary nails if the distal and
proximal screws are correctly inserted.24,25 Gupta et al ob-
tained good rotational stability with intramedullary nails,
with a functional improvement rate of 89%.26 Successful
outcome rates of 87.5e100% have been reported in non unions
treated with locked intramedullary nails.1,13 In our patients,
nails appropriate to the width of the medulla were locked at
the distal and proximal ends; rotational stability was achieved
in all patients, and complete consolidation in 96%.It is claimed
in the literature that compression is not achievedwhen locked
intramedullary nails are used in nonunions or primary frac-
tures, and hence that treatment may be unsuccessful.1
Nonetheless, 100% successful results have been reported
with the achievement of rotational stability.26 The rate of
nonunions caused by lack of compression may be reduced by
achieving sufficient contact between fracture fragments intra
operatively.
In conclusion, intramedullary nailing and autogenous bone
grafting increases the union rate provided that a nail with a
diameter appropriate to the width of the medulla is used and
that distal and proximal locking are performed correctly. In
addition, that the low infection rate, low risk of radial nerve
injury, and the need for only limited surgical exposure make
this a suitable choice in the treatment of nonunions.
Conflict of interest statement
The author has none to declare.
Ethical statement
The ethical statement as (1) the patients gave the informed
consent prior being included into the study; (2) the study was
authorized by the local ethical committee and was performed
in accordance with the Ethical standards of the 1964 Decla-
ration of Helsinki as revised in 2000.
r e f e r e n c e s
1. Wu CC, Shin CH. Treatment for nonunion of the shaft thehumerus: comparison of plates and Seidel interlocking nails.Can J Surg. 1992;35:661e665.
2. Rose SH, Milton LJ, Morrey BF. Epidemiologic features ofhumeral shaft fractures. Clin Orthop. 1982;168:24e30.
3. Rosen H. The treatment of nonunions and pseudoarthroses ofthe humeral shaft. Orthop Clin North Am. 1990;21:725e742.
4. Healy WL, White GM, Mick CA. Non union of the humeralshaft. Clin Orthop. 1987;219:206e213.
5. Stern PJ, Mattingly DA, Pomeroy DL. Intramedullary fixationof humeral shaft fractures. J Bone Joint Surg Am.1984;66:639e646.
6. Palvanen M, Kannus P, Parkkari J. The injury mechanisms ofosteoporoticupper extremity fractures among older adults: a
Please cite this article in press as: Ali MI, Management for lockfailure in non union osteoporotic humerus shaft bone frj.apme.2015.04.001
controlled study of 287 consecutive patients and their 108controls. Osteoporos Int. 2000;11:822e831.
7. Pugh DM, McKee MD. Advances in the management ofhumeral nonunion. J Am Acad Orthop Surg. 2003;11:48e59.
8. Dalton JE, Salkeld S, Satterwhite YE, Cook SD. Abiomechanical comparison of intramedullary nailing systemsfor the humerus. J Orthop Trauma. 1993;7:367e374.
9. Flinkkil€a T, Hyv€onen P, Siira P, H€am€al€ainen M. Recovery ofshoulder joint function after humeral shaft fracture: acomparative study between antegrade intramedullary nailingand plate fixation. Arch Orthop Trauma Surg. 2004;124:537e541.
10. Zlotolow DA, Catalano 3rd LW, Barron OA, Glickel SZ. Surgicalexposures of the humerus. J Am Acad Orthop Surg.2006;14:754e765.
11. Livani B, Belangero W, Medina G, Pimenta C, Zogaib R,Mongon M. Anterior plating as a surgical alternative in thetreatment of humeral shaft non-union. Int Orthop.2010;34:1025e1031.
12. Loomer R, Kokan P. Non-union in fractures of the humeralshaft. Injury. 1976;7:274e278.
13. Corradi M, Petriccioli D, Panno B, Merenghi P. Seidel lockednailing for the treatment of unstable fractures and nonunionof the humerus. Chir Organi Mov. 1996;81:189e195.
14. Pietu G, Raymond G, Letenneur J. Treatment of delayed andnonunions of the humeral shaft using the Seidel locking nail:a preliminary report of five cases. J Orthop Trauma.1994;8:240e244.
15. Wu CC. Humeral shaft nonunion treated by a Seidelinterlocking nail with a supplementary staple. Clin Orthop.1996 May;326:203e208.
16. Lammens J, Bauduin G, Driesen R, et al. Treatment ofnonunion of the humerus using the Ilizarov external fixator.Clin Orthop. 1998;353:223e230.
17. Patel VR, Menon DK, Pool RD, Simonis RB. Nonunion of thehumerus after failure of surgical treatment managementusing the Ilizarov circular fixator. J Bone Joint Surg.2000;82:977e983.
18. Fenton P, Qureshi F, Bejjanki N, Potter D. Management of non-union of humeral fractures with the Stryker T2 compressionnail. Arch Orthop Trauma Surg. 2011;131:79e84.
19. Bosh U, Skutek M, Kasperczyk WJ, Tscherme H. Nonunion ofthe humeral diaphysis-operative and nonoperativetreatment. Chirurg. 1999;70:1202e1208.
20. Lin J, Hou SM, Inoue N, Chao EY, Hang YS. Anatomicconsiderations of locked humeral nailing. Clin Orthop at Res.1999;368:247e254.
21. Jinn L, Sheng M. Treatment of humeral shaft fractures byretrograde nailing. Clin Orthop. 1997;342:147e155.
22. Stannard JP, Harris HW, McGwin Jr G, Volgas DA, Alonso JE.Intramedullary nailing of humeral shaft fractures with alocking flexible nail. J Bone Joint Surg Am. 2003;85:2103e2110.
23. Ingman AM, Waters DA. Locked intramedullary nailing ofhumeral shaft fractures: implant design, surgical technique,and clinical results. J Bone Joint Surg. 1994;76:23e29.
24. Riemer BL, D'Ambrosia R. The risk of injury to the axillarynerve, artery, and vein from proximal locking screws ofhumeral interlocking nails. Orthopedics. 1992;15:697e699.
25. Prince EJ, Breien KM, Fehringer EV, Mormino MA. Therelationship of proximal locking screws to the axillary nerveduring antegrade humeral nail insertion of four commerciallyavailable implants. J Orthop Trauma. 2004;18:585e588.
26. Gupta RC, Gaur SC, Tiwari RC, Varma B, Gupta R. Treatmentof ununited fractures of the shaft of the humerus with bentnail. Injury. 1985;16:276e280.
ing compression plate/dynamic compression plate implantacture, Apollo Medicine (2015), http://dx.doi.org/10.1016/

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/