Embed Size (px)
DESCRIPTION
In spite of greater economic convergence globally, as low-income countries grow into middle-income country economies, intra-country inequalities – economic, social, and health status – risk being exacerbated. To expand access to high quality healthcare at low cost at point of care, guidance is needed to identify effective performance measures to gauge progress. Is is increasing access to the current healthcare package to new users, is it adding more or better healthcare for current beneficiaries, or is healthcare expansion to be understood as lower prices and greater protection from out-of-pocket spending on health services? Results are presented from a 2012 pilot of two equity measures that set out to determine whether either of the measures was more practical to implement at lower cost and easily understood by social protection program managers. Recommendations are made for integrating these measures into existing programs.
Citation preview

Measuring to Manage Progress toward Universal Health CoverageBen BellowsOn behalf of the Social Franchise Metrics Working GroupNHIS 10th Anniversary International Conference on UHCAccra

UHC is multidimensional & aspirational
Access: Expand coverage to wider population
Scope: Improve quality & quantity of health services offered
Financial protection: Improve size of subsidies or reduce informal charges
3
How universal can vouchers really be?
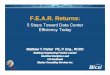
Despite growing evidence for vouchers’ impressive impact in terms of equity, financial protection and quality of care, they remain for now a specific tool to enable underserved groups to access priority services. However the WHO’s ‘cube’ frames progress towards UHC in terms of the share of people, services and costs covered, with a focus on growing these three dimensions as far as possible
xi. Given this
understanding of UHC, how important can
vouchers’ contribution to UHC really be?
The first point to remember is that vouchers do not have to be targeted. For example, all families were eligible for the wildly successful family planning voucher programmes in Korea and Taiwan in the 60s-90s. Even among targeted voucher programmes, some are being operated on a huge scale: the Chiranjeevi Yohana scheme in Gujarat, India, which is targeted to the poor, is a case in point. Vouchers don’t have to be targeted to specific services either: vouchers for migrant farm workers in the US cover all types of services with a maximum reimbursement level
xii. This sort of voucher
programme illustrates very clearly how vouchers and insurance are actually on the same spectrum, as noted by Gorter et al (2013)
xiii. A voucher scheme in Tanzania is
located even further along that spectrum: vouchers distributed to pregnant women entitle the mother and her baby to full health insurance during the baby’s infancy, while the rest of the family gains entitlement to
partial health insurancexiv
.
However, most voucher schemes do target particular groups, and/or provide entitlement to only a few services. Far from being contradictory to UHC, targeting vouchers both in terms of services and population groups could actually help even well-established UHC systems avoid common
pitfalls.
Pitfall 1: Social Health Insurance can emphasise curative care at the expense of
public health and preventative care
Because the first aim of Social Health Insurance is to prevent catastrophic health expenditure, some fledgling insurance schemes start by covering expensive inpatient services only, excluding outpatient, primary and preventative services from the benefit package (e.g. India, Kenya, Philippines)
xv. In addition, individuals in any
system (whether SHI or input-based) may under-consume public and preventative health care if left to their own devices. This is because some of the risks of not seeking care, such as infecting others, as well as the future costs of illness, are borne by others. In either of those situations, vouchers can serve as a useful addition to the prevailing health financing approach, thereby ensuring that preventive services are appropriately emphasised. Vouchers are often used for preventive services, most notably for family planning, but also for immunisation (Cambodia and Armenia), and cervical and breast cancer screening (Nicaragua,
Vietnam)xvi
.
Figure 1: WHO's Universal Health Coverage 'Cube'

Access is far from universal in 54 LMIC
• Of 12 MNH interventions in a review of public data across 54 countries, family planning was the third most inequitable
*Barros, A. J. D., Ronsmans, C., et al. (2012). “Equity in maternal, newborn, and child health interventions in Countdown to 2015: a retrospective review of survey data from 54 countries”. Lancet, 379(9822), 1225-33.

Limited financial protection is common in 51 LMIC*
• 13–32% of household expenditures over 4 weeks went to healthcare
• 25% poor households incurred potentially catastrophic healthcare expenses
• >40% of households used savings, borrowed money, or sold assets to pay for care
• 41-56% of households spent 100% of health care expenditures on medicines
*Wagner, Graves, Reiss, LeCates, Zhang, Ross-Degnan. 2011. “Access to care and medicines, burden of health care expenditures, and risk protection: Results from the World Health Survey” Health Policy. 100(2-3):151-158

Selected constructs and metrics for UHC measurement
Quality of care:• Donabedian framework (structure, process, outcomes)• Investment in facility infrastructure
Financial protection:• Out-of-pocket spending on health paid for by the patient at
the point of service • Proportion of household consumption that is spent on
healthcare
Equitable access:• Geographic proximity• Above or below a poverty line • Member of a wealth quintile

Preferred characteristics in a UHC equity measure
• Program Managers
• Quick, inexpensive to
collect
• Easy to interpret by
managers and field staff
• Agency Headquarters
• Standardized &
comparable nationally
• Easy to explain to policy
makers
• Other Stakeholders
• Comparable internationally
• Clients• Transparent, trustwort
hy, quick application process
• Time-delimited membership
• Recognition of solidarity
• Recourse for appeal

Pilot study: Find a good routine, monitoring equity indicator
• MPI dismissed: not feasible to collect
• PPI and Wealth Index piloted in 5 countries in 2012 as part of franchise client exit interviews
• Results compared against selection criteria
Progress out of Poverty Index
(PPI)
Wealth Index (WI)
Multi-dimensional
Poverty Index (MPI)

PPI tools

DHS questions

Quintile India Madag Benin DRC Mali
n=797 n=853 n=535 n=242 n=293
1 (Poorest) 27.9 2.1 3.4 0 0
2 (Poorer) 22.5 9.3 2.4 0 0
3 (Middle) 21.7 25.4 4.3 0 0.3
4 (Richer) 15.3 38.6 13.1 9.1 13.9
5 (Richest) 12.7 24.6 76.8 90.9 85.7
Results & indicator attributes
Wealth IndexRelative measure
Uses DHS data to compare client sample to national wealth quintiles
Low-cost because DHS data is publicly available
PPIAbsolute measure
Asset list gives likelihood that a client is under $1.25/day poverty threshold
Expensive: unique asset weights developed for each country
Only 6% of Benin franchise clients are from the bottom 40% of the population
Threshold Clients Benin Pakistan Philippines Vietnam
$1.25/day
Franchise 19% 17% 17% 8%
National 47% 21% 18% 17%
$2.50/day
Franchise 61% 72% 51% 51%
National 75% 60% 42% 43%
19% of Benin franchise clients living under the $1.25/day threshold vs. 47% of the national population

Selection criteria
Criteria PPI Wealth Index
Easy to Collect and Interpret
Easy to collect
Easy to calculate
Easy to interpret poverty threshold
Easy to collect
Difficult to calculate
Quintiles widely used/understood
Low Cost $20,000-$25,000 per country
Requires some upkeep costs
Inexpensive
Based on publicly-available DHS
Comparable to National Context
Percent of clients under poverty line easily
comparable to national poverty rate
Difficult/impossible subgroup analysis e.g.:
just urban, or just FP clients
Wealth quintiles accurate and validated
comparison to national distribution
Easy subgroup analysis
Comparable AcrossCountries
Percentage of clients under $1.25/day
standard across countries
Can discuss percentage of clients that fall
within bottom 40%, but measure is
relative to a country

Using Wealth Index routinely
• Randomly select NHIS facilities or enrollment centers
• Conduct exit surveys among clients• 20 questions about household characteristics• Adds approximately 10 minutes to each interview
• Centralized data analysis in M&E unit – takes about 8 hours
• Build capacity through a tool kit and standard syntax files
• Conduct surveys on quarterly or semi-annual basis

Uganda & Kenya: Equity targeting for program enrollment
• Uganda & Kenya voucher programs
• Every client identified in the community using a short targeting tool
• Voucher expires after a year and can only be used for one service package.

Respondents who had ever used the
HealthyBaby voucher in Uganda (2010-
2011)
0%
5%
10%
15%
20%
25%
30%
35%
Poorest quintile
Poorer quintile
Middle quintile
Richer quintile
Richest quintile

Does NHIS enrollment vary by wealth quintile?
0%
10%
20%
30%
40%
50%
Poorest Less poor Middle Less rich Richest
Women (DHS 2008)
All (SHINE, 2009)

Conclusions: Active equity targeting is key component of UHC
• Tools exist that can cost-effectively identifying the poor who, in the absence of active identification, would not have become NHI members
• Monitor samples of clients for reporting against performance targets
• Use for beneficiary identification and enrollment
• Consider: Are other exemptions as effective to achieve the same objective?

Thank you
Social Franchising Metrics Working Group• Bill & Melinda Gates Foundation• DKT• International Planned Parenthood Federation• Johns Hopkins• Marie Stopes International• Population Services International • Rockefeller Foundation • Population Council • University of California San Francisco • USAID• World Health Partners