Embed Size (px)
Citation preview

Prof Narendra Malhotra
President ISPAT
Prof Jaideep Malhotra
President elect ISPAT
An ISPAT initiativ
Micronutrients and Pregnancy
Effect of Suplementation and its
Outcomes &
Vitamen D 3 in women’s health

It is now widely accepted that the risks of a number of chronic diseases in adulthood such as diabetes mellitus, hypertension and coronary heart disease may have their origins before birth
Fetal origins of adult diseases
Ref:Effect of In Utero and Early-Life Conditions on Adult Health and Disease; Peter D. Gluckman et.al; N Engl J Med 2008;359:61-73.
The early life origins of asthma and related allergic disordersJ O WarnerCorrespondence to:Prof. J O WarnerProfessor of Child Health, Allergy & Inflammation Sciences, Division of Infection, Inflammation & Repair, School of Medicine,University of Southampton, UK; [email protected]

Early Programming and Fetal origins of adult diseases
Developmental plasticity: Ability of an organism to develop in various ways, depending on the particular environment or setting
Developmental programming is defined as the response by thedeveloping mammalian organism to a specific challenge during acritical time window that alters the trajectory of developmentwith resulting persistent effects on phenotype
Ref: Prenatal origins of adult disease; Current Opinion in Obstetrics and Gynecology 2008, 20:132–138
Peter D. Gluckman, et.al, N Engl J Med 2008;359:61-73

Fetal Origins of Adult Disease
Responses to adverse environments:1. Accelerated maturation
( G- corticoid level)1. Keeps nutrients
( growth & nutrition)3. Pregnancy termination
(abortion, prematurity)
MATERIAL ENVIRONMENT
+MATERIAL & PLACENTAL
PHYSIOLOGY
fetalEnvironment
IntrauterineEnvU –Placental
Unity
+ GENOME
Alterations:•fetal growth
•Interaction pre-and-post natal environments
FETAL ORIGIN OF DISEASE

Effects of undernutrition
Ref: Maternal nutrition: Effects on health in the next generation Caroline Fall; Indian J Med Res 130, November 2009, pp 593-599
Cortisol
Maternal diet
Uteroplacentralblood flow
Placentraltransfer
Fetal genome
Nutrient demand exceeds supplyFETAL UNDERNUTRITION
Brain sparing Down regulation of growth
Early Maturation
Altered body composition
Impaired development: bloodvessels,liver,kidneys,pancreas.
↓ Insulin/IGF-1Secretion and sensitivity
Centralobesity
Insulinresistance
HyperlipidaemiaHypertension
Type 2 diabetes and CHD
Muscle ↓

Conceptual frameworks for how maternal diet and micronutrients status may affect the development of chronic disease in the offspring
Ref: Stewart CP, J Nutr 2010 140(10): 437-445 PMID 20071652
Hormonal adaptationsFe,Zn,Ca
•Increased stress hormones•Decreased somatotrophic
hormones(GF,Insulin)
Epigenetic gene regulation
Folate ,Vitamin B-12
Restricted foetal growth and development
Maternal micronutrient deficiency
Renal functionFe, Zn,Vitami n A foalte•Impaired nephrogenesis/ Reduced nephronendowment•Reduced GFR•Increased sodium sensitivity
Cardiovascular functionFe,Zn,Viatmin A folate•Impairedvascularization•Malformations•Cardiac hpertrophy
Pancreas / β –cell function
Fe,Zn,folate,VitaminB-12
•Reduction in number and area of β - cell
Body compositionMg,Zn,folate,Vitamin
B-12•Reduced lean body mass•Altered fat deposition or metabolism•Sedentary behaviour•Altered appetite•regulation
Primary FunctionVitamin A,Vitamin D•Reduced bronchial branching & alveoli•Reduced elastin•Reduced VEGF•Chronic respiratory infections•Reduced lung capacity
HypertensionInsulin resistance
and β – celldysfunction
Cardio metabolic risk

Nutritional Programming of the Brain
Brain Development

Perinatal period is a “BrainTime”:A window of opportunity forNutritional optimization ofbrain development andfuture health and performance

Maternal Nutrition and Cognition in offspring
Permanent, largecognitive and
motoreffects of early nutrition – withstructural changes
in the brain

MRI Brain mappingSuggests cognitive effects of
early nutrition related to
multiple effects on brain
structure
Ref: Edmonds CJ et al. Pediatrics 2010;126:e1095–e1101

Key cognitive educational performance & motor
skills influenced by early nutrition
Ref: Edmonds CJ et al. Pediatrics 2010;126:e1095–e1101

For each 1kg
reduction in birth weight
(compared to other
twin) there was a 13
Point loss in verbal IQ
Ref: Edmonds CJ et al. Pediatrics 2010;126:e1095–e1101

Programming for Diabetes: Undernutrition and Overnutrition
Type2 Diabetes

fetal undernutrition
Undernourished (small) mother
Postnatal under nutrition
Insulin resistance
Small baby (Thin-fat)
Altered fuels
Pregestationaland gestational hyperglycemia
Obesity and hyperglycemia
Macrosomia
fetal adiposity & islet dysfunction
Postnatal over nutrition (Urbanisation)
Dual - Teratogenesis
Undernutrition Overnutrition
Nutrient-mediatedteratogenesis
Fuel-mediated teratogeneis
Ref: Yajnik CS, Deshmukh U, 2009

12Y
6Y
Postnatal
Birth
Intrauterine
Preconception
Children & parents Size, bodyComposition IR CVD risk markers Cognition 690/722 (95%)
Children & parents Size, body Composition IR CVD risk markers698/723 (96%)
Growth every 6 months 743
Size Phenotype 770
Maternal Size Nutrition Metabolism Paternal size Metabolic variables fetal growth (USG) 814
Maternal Size Hemoglobin 2675
19
93
19
94
-96
20
00
-03
20
06
-08
Pune Maternal Nutrition Study
Ref: Indian J Med Res 130, Caroline Fall ,November 2009, pp 593-599

The nutritional status of pregnant women in
India

Current scenario in India
• 18% of pregnant women consumed < 50% of calories
• 34% of pregnant women consumed <50% of protein
• 85% of pregnant women consumed <50% iron
• 57% of pregnant women consumed <50% b-caroten - relative to their RDA(recommended dietary allowance)Ref: Indian Pediatrics 1999; 36: 991-998

Pregnancy Diet – 4 Pillars of development

CONTENTS OF THIS PRESENTATION
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Introduction
Micronutrient is the umbrella term used to represent essential vitamins and minerals required from the diet
to sustain virtually all normal cellular and molecular functions
Cell signaling, motility, proliferation, differentiation and apoptosis that regulate tissue growth, function
and homeostasis
Ann Nutr Metab 2015;66(suppl 2):22–33Nat Rev Endocrinol 2016; 12(5): 274–289

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Prevalence of Multiple Micronutrient Deficiencies
• Globally, approximately two billionpeople, the majority women andyoung children, are affected, bymicronutrient deficiencies, with evenhigher rates during pregnancy
• Concurrent deficiencies of morethan one or two micronutrients arewell documented among youngpregnant women, (and youngchildren), especially in Low- andMiddle-Income Countries
Nutrients 2015, 7

Prevalence of Multiple Micronutrient Deficiencies
Pe
rce
nta
ge o
f P
regn
ant
Wo
me
n D
efic
ien
t Community based cross sectional
survey To assess the prevalence of
multiple micronutrient deficiencies amongst pregnant
women
1Indian J Pediatr 2004 ;71(11):1007-142Indian J Endocr Metab 2014; 18:486-90
73.5
2.7
43.6
73.4
26.3
37
0
10
20
30
40
50
60
70
80

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Risk Factors for Micronutrient Deficiency in Pregnancy
Poor Quality Diets High Fertility RatesRepeated
Pregnancies
Short inter-pregnancy Intervals
Increased Physiological
Needs
Nutrients 2015, 7, 1744-1768
Increased Additional Demand During Pregnancy

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Nat. Rev. Endocrinol. doi:10.1038/nrendo.2016.37
Function and Timing of Micronutrients that Affect Outcomes in Offspring
Short-term Long-term
Miscarriage
Stillbirth
Birth defects
Small size for gestational age
Preterm birth
Death
Altered growth, body composition
Compromised cardiometabolic,
pulmonary and immune function
Poor neurodevelopment and cognition
Adverse health outcomes of gestational micronutrient deficiency

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Micronutrients During Pregnancy & LactationAre we Neglecting Few Micronutrients.......
Today in practice most of theattention has been given only tofew micronutrients, for exampleiron, folate, Vit B, Calcium and Vit-D3
Some micronutrients deserveattention as studies have shown thelinks between deficiency states andpoor pregnancy outcome. EgIodine, zinc, copper, Mangnese,magnesium .
Am J Clin Nutr May 2005 ; vol. 81 no. 5 1206S-1212S

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

A Pregnant with Iodine DeficiencyThe Consequences
In General Population
Hypothyroidism
Goitre
Pregnancy
Abortion
Still Birth
Pregnancy and Fetal Health
IQ and Neuropsychological
Brain damage
Mental retardation
Psychomotor defects Indian J Endocrinol Metab. 2015 Sep-Oct; 19(5): 602–607. Thyroid. 2009 May;19(5):511-9.Nutrient requirements and recommended dietary allowances for indians .ICMR 2009 ReportIndian J Endocr Metab 2014;18:486-90
Prevention: Iodized Salt
PreventionAdditional Iodine Supplementation

Even with use of iodized salt & eating seafood, awoman’s daily iodine intake would be in the orderof 100–150 mcg per day approximately half theamount recently recommended during pregnancyand lactation (i.e 220 -290 mcg)
International Journal of Gynecology and Obstetrics 131 S4 (2015) S213–S253
FIGO recommends that all pregnant and Lactating women should take adequate supplementation of Iodine

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Calcium and Vitamin D Status in India
• Indian RDA for non-pregnant women- 600 mg/day.• Over 50% of women, are not meeting this number• There is evidence of calcium depletion, measured by bone
mineral density, particularly in women after repeated pregnancy and lactation
• Vitamin D deficiency exists in Indian adults-based on 25 hydroxy Vitamin D2
• Vit D status of children - very low in both urban and rural populations
• Pregnant women and their new born had low vitamin D status• Dietary calcium supplementation had positive effect on 25(OH)D
levels
Ref: JAPI, 2009; (57):40-48

Calcium & Vitamin DMust for Pregnancy and Fetal Bone Development
Calcium Carbonate Higher Elemental CalciumHigher BioavailabilityEconomical and Safe
Vitamin DOptimal serum 25(OH)D level in pregnancy should be at least 20
ng/mL (50 nmol/L)

CALCIUM METABOLISM IN PREGNANCY

increased1,25(OH)2D
ProlactinPlacental Lactogen
Increased intestinal calcium absorption
CALCIUM METABOLISM IN PREGNANCY (Contd..)

VITAMIN D METABOLISM

NON-SKELETAL FUNCTIONS OF VITAMIN D
ROLE OF VITAMIN D

25(OH)D LEVELS URBAN INDIAN ADULTS
1. Goswami R, Gupta N, Goswami D, Marwaha RK, Tandon N, Kochupillai N. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am J Clin Nutr. 2000;72(2):472-5. 2. Arya V, Bhambri R,Godbole MM, Mithal A. Vitamin D status and its relationship with bone mineral density in healthy Asian Indians.Osteoporos Int. 2004;15(1):56-61. 3. Tandon N, Marwaha RK, Kalra S, Gupta N, Dudha A, Kochupillai N. Bone mineralparameters in healthy young Indian adults with optimal vitamin D availability. Natl Med J India. 2003;16(6):298-302.4. Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D. Vitamin D status in Andhra Pradesh : a population basedstudy. Indian J Med Res. 2008;127(3):211-8. 5. Marwaha RK, Tandon N, Reddy DR, Aggarwal R, Singh R, Sawhney RC,et al. Vitamin D and bone mineral density status of healthy schoolchildren in northern India. Am J Clin Nutr.2005;82(2):477-82.
Categories of patients Vitamin D levels
Physicians and nurses1 3.19 ng/ml (winter) ; 7.18 ng/ml (summer)
Pregnant women1 8.76 ng/ml
Hospital staff2 66% had <15 ng/ml; 20.6% had <5 ng/ml; 78% had <20 ng/ml
Para-military forces3 18.4 ng/ml (winter); 25.3 ng/ml (summer)
Urban children4 Male: 15.57+/-1.21 ng/ml; Female: 18.5+/-1.66 ng/ml
Urban adult4 Male: 18.54+/-0.8 ng/ml; Female: 15.5+/-0.3 ng/ml
Urban children withsocioeconomic status (SES)5
35.7% children had <9 ng/ml (42.3% in lower SES and 27% in upper SES)
PREVALENCE OF VITAMIN D DEFICIENCY

25(OH)D LEVELS: RURAL DATA
1. Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V. High prevalence of vitamin D deficiency amongpregnant women and their newborns in northern India. Am J Clin Nutr. 2005;8:1060–4. 2. Harinarayan CV,Ramalakshmi T, Prasad UV, Sudhakar D. Vitamin D status in Andhra Pradesh : a population based study. Indian J MedRes. 2008;127(3):211-8.
Categories Vitamin D levels
Adolescent girls1 88.6% had <20 ng/ml
Pregnant women1 74% had <20 ng/ml
Weather-wise1 Levels in summer [22 ng/ml ] > in winter [12ng/ml]
During winter1 Levels in boys [~25 ng/ml] > female siblings [~12 ng/ml]
Rural children2 Male: 17 +/- 1.3 ng/ml; Female: 19+/- 1.59 ng/ml
Rural adult2 Male: 23.73 +/- 0.8 ng/ml; Female: 19+/- 0.89 ng/ml

25 (OH)D LEVELS: ELDERLY INDIANS IN DELHI
Marwaha RK, Tandon N, Garg MK, Kanwar R, Narang A, Sastry A, et al. Bone health in healthy Indianpopulation aged 50 years and above. Osteoporos Int. 2011;22(11):2829-36.
Severity All (1346) Male Female
25(OH)D Levels (ng/dl) 9.79±7.61 9.81±6.79 9.78±8.30
Severe (<5 ng/ml) 376 (27.9%) 166 (25.8%) 210 (29.9%)
Moderate (5-<10 ng/ml) 457 (34.0%) 220 (34.2%) 237 (33.7%)
Mild (10-<20 ng/ml) 395 (29.4%) 201 (31.3%) 194 (27.6%)
VDI (20-<30 ng/ml) 92 (6.8%) 47 (7.3%) 45 (6.4%)

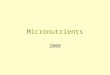
VITAMIN D DEFICIENCY IN INDIAN HEALTH PROFESSIONALS
Beloyartseva M, Mithal A, Kaur P, Kalra S, Baruah MP, Mukhopadhyay S, et al. Widespread vitamin D deficiency among Indian health care professionals. Arch Osteoporos. 2012;7(1-2):187-92.
Aurangabad
Bangalore
Bhopal
Chennai
Kolkata
Lucknow
Vapi
JaipurJodhpur
Chandigarh
Hyderabad
Cochin
Madurai
Ahmedabad
Mumbai
Vitamin D deficiency
Vitamin D insufficiency
Vitamin D sufficiency

VITAMIN D STATUS IN ADULTS (>18 YEARS)
Wahl DA, Cooper C, Ebeling PR, Eggersdorfer M, Hilger J, Hoffmann K, et al. A global representation ofvitamin D status in healthy populations. Arch Osteoporos. 2012;7(1-2):155-72.

REASONS FOR WIDESPREAD DEFICIENCY
Latitude, season, time of the day
Cloud cover and atmospheric pollution
Time spent outdoors
Customary dress and sunscreen use
Skin pigmentation and age
Prentice A. Vitamin D deficiency: a global perspective. Nutr Rev. 2008;66(10 Suppl 2):S153-64.

SKIN COLOUR IS IMPORTANT
Skin type
Sun history Example
I Always burns easily, never tans, extremely sensitive skin
Red-headed, freckled, Celtic, Irish-Scots
II Always burns easily, tans minimally, very sensitive skin
Fair-skinned, fair-haired, blue-eyed Caucasians
III Sometimes burns, tans gradually to light brown, sun-sensitive skin
Average-skinned Caucasians, light-skinned Asians
IV Burns minimally, always tans to moderate brown, minimally sun-sensitive
Mediterranean-type Caucasians
V Rarely burns, tans well, sun-insensitive skin
Middle Easterners, some Hispanics, some African-Americans
VI Never burns, deeply pigmented, sun-insensitive skin
African-Americans
Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80(6):1678S-88S.
Indians have skin type V

PCOS Inverse association between 25(OH)D levels and insulin resistance,
features of hyperandrogenism, and circulating androgens in women with PCOS.
Normalisation of menstrual cycles with vitamin D and calcium supplementation over 6 months.
Dietary supplementation with vitamin D or an analog improves
• insulin sensitivity
• Circulating testosterone
• Parameters of ovarian folliculogenesis and ovulation
Luk J, Torrealday S, Neal Perry G, Pal L. Relevance of vitamin D in reproduction. Hum Reprod. 2012;27(10):3015-27.
IMPORTANCE OF VITAMIN D IN WOMEN

GYNECOLOGICAL DISORDERS ASSOCIATED WITH VITAMIN D DEFICIENCY
Disorder Strength of association
Recommendation for testing
Recommendation for supplementation
Polycystic Ovary Syndrome
+++ Routine 25(OH)Dtesting not recommended
60k once a month
Premenstrual Syndrome
+ As for normal population
Uterine Fibroid + As for normal population
Endometriosis + As for normal population
IVF +- As for normal population

It is prudent to optimize Vitamin D status in
women with polycystic ovary syndrome (PCOS)
and in women planning pregnancy.

PREVALENCE OF VITAMIN D DEFICIENCY IN PREGNANT INDIAN WOMEN
1. Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V. High prevalence of vitamin D deficiency amongpregnant women and their newborns in northern India. Am J Clin Nutr. 2005;8:1060–4. 2. Sahu M, Bhatia V, AggarwalA, Rawat V, Saxena P, Pandey A, et al. Vitamin D deficiency in rural girls and pregnant women despite abundantsunshine in northern India. Clin Endocrinol (Oxf). 2009;70(5):680-4. 3. Marwaha RK, Tandon N, Chopra S, Agarwal N,Garg MK, Sharma B, et al. Vitamin D status in pregnant Indian women across trimesters and different seasons and itscorrelation with neonatal serum 25-hydroxyvitamin D levels. Br J Nutr. 2011;106(9):1383-9.
25 (OH) D levels Prevalence
Less than 22.5 ng/ml 84% pregnant women1
Less than 20 ng/ml74% rural pregnant women2
96.5% pregnant women3
99.7% lactating women3

MATERNAL SERUM VITAMIN D3 AND NEONATAL OUTCOMES
Insufficient serum levels of 25-OHD were associated with
• Gestational Diabetes (pooled odds ratio 1.49, 95% confidence interval 1.18 to 1.89),
• Pre-eclampsia (1.79, 1.25 to 2.58), and
• Small For Gestational Age Infants (1.85, 1.52 to 2.26).
Pregnant women with low serum 25-OHD levels had an increased risk of
• bacterial vaginosis and
• low birth weight infants
• but not delivery by caesarean section.
Aghajafari F, Nagulesapillai T, Ronksley PE, Tough SC, O'Beirne M, Rabi DM. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: systematic review and meta-analysis of observationalstudies. BMJ. 2013;346:f1169.
EFFECTS OF VITAMIN D DEFICIENCY IN PREGNANCY

NEONATAL OUTCOMES
Maternal and cord blood levels of 25(OH)D closely correlate
Maternal vitamin D deficiency may affect femoral bone development as early as 19 week (Mahon et al 2010)
Lower bone mineral density (Javaid et al 02006)
Neonatal birth weight (Ert et al 2012)

VITAMIN D DEFICIENCY IN PREGNANCY IS ASSOCIATED WITH..
Maternal Disorders Strength of association
Preecclampsia +++
Gestational Diabetes +
Bacterial Vaginosis ++
Neonatal Disorders Strength of association
Small for Gestational Age (SGA) +++

WHAT CUT-OFF TO BE USED IN PREGNANCY?
For birth variables: 15 ng/ml (37.5nmol/l)
Rise in PTH: 22.5 ng/ml (56.25nmol/l)
For pregnancy outcomes: 30 ng/ml (75nmol/l)
25(OH)D less than 20ng/ml or 50 nmol/l: Deficient
25(OH)D between 20-30ng/ml or 50-75 nmol/l : insufficient
Rabi et al, BMJ 2013; Sachan et al, AJCN, 2005

VITAMIN D3 CONCENTRATION IN MOTHERS AND INFANTS
Mean serum 25(OH)D of 8.2 ng/mL at enrollment.
Cholecalciferol 400 units vs 2000 units vs 4000 units per day
The percent who achieved 25(OH)D greater than 32 ng/mL and greaterthan 20 ng/mL concentrations in mothers and infants was highest in 4000IU/d group.
No adverse event related to vitamin D supplementation.
Hollis BW, Wagner CL. Clinical review: The role of the parent compound vitamin D with respect to metabolism andfunction: Why clinical dose intervals can affect clinical outcomes. J Clin Endocrinol Metab. 2013;98(12):4619-28.
HOW TO SUPPLEMENT VITAMIN D DURING PREGNANCY

VITAMIN D REPLACEMENT IN RURAL NORTH INDIAN PREGNANT WOMEN
Pregnant women received
• no cholecalciferol (Group A) or
• 60000U (Group B) in the fifth month of gestation or
• 120000U each in the fifth and seventh gestational months (Group C).
Cholecalciferol in doses of 120 000 U each in fifth and seventh gestational months was effective in raising 25OHD at delivery.
Sahu M, Das V, Aggarwal A, Rawat V, Saxena P, Bhatia V. Vitamin D replacement in pregnant women in rural northIndia: a pilot study. Eur J Clin Nutr. 2009;63(9):1157-9.

VITAMIN D SUPPLEMENTATION IN PREGNANT INDIAN WOMEN
All pregnant women after 12 weeks
2000 units per day
4000 to 5000 units per day in those with high risk (with calciummonitoring)
• High risk for hypertension or preecclampsia
• High risk for GDM
• High risk for preterm delivery
• Clinical features of osteomalacia
• Previous baby with SGA/ rickets/ hypocalcemia

Vitamin D requirements during lactation: high-dose maternal supplementation as therapy to prevent hypovitaminosis D for both the mother and the
nursing infantBruce W Hollis and Carol L Wagner
A maternal intake of 4000 IU/d could achieve substantial progress towardimproving both maternal and neonatal nutritional vitamin D status.
Hollis BW, Wagner CL. Vitamin D requirements during lactation: high-dose maternal supplementation as therapy toprevent hypovitaminosis D for both the mother and the nursing infant. Am J Clin Nutr. 2004;80(6):1752S-8S.

VITAMIN D SUPPLEMENTATION IN LACTATING WOMEN
Cholecalciferol supplementation to all women
2000 units per day
4000 units
• in exclusively breast-fed infant
• if parents chose not to supplement the infant with vitamin D

CHALLENGES IN CURRENT CONVENTIONAL FORMULATION OF VITAMIN D3
Absorption of Vitamin D3 from conventional formulation is highly dependent on high-fat meal
Bioavailability of Vitamin D3 is dependent on bile secretions, micelle formation, and diffusion through unstirred-water layer
Compliance/ Convenience becomes a challenge as most Vitamin D3 preparations are to be administered along with milk or clarified butter
Raimundo FV, Faulhaber GA, Menegatti PK, Marques Lda S, Furlanetto TW. Effect of High- versus Low-Fat Meal on Serum 25-Hydroxyvitamin D Levels after a Single Oral Dose of Vitamin D: A Single-Blind, Parallel, Randomized Trial. Int J Endocrinol. 2011;2011:809069.

Absorption via 3 pathways (Paracellular, Transcellular and Persorption) is not fat-dependent and is unaffected by fed fast variation1
Bioavailability of nanoparticles is 3 times higher than conventional drugs as it penetrates the mucous layer easily2
Convenience of taking nanoparticle formulation is high as it does not require milk or clarified butter for absorption
VITAMIN D3 NANO PARTICLES – OVERCOMES THE CHALLENGE
1. McClements DJ. Edible lipid nanoparticles: Digestion, absorption, and potential toxicity. Progress in Lipid Research. 2013;52:409-23
2. Huang Q, Yu H, Ru Q. Bioavailability and delivery of nutraceuticals using nanotechnology. J Food Sci. 2010;75(1):50-7

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

METALLOENZYMES
There are more than 300 enzymes whose functions can beimpacted if diet is deficient on zinc, copper, manganese andmagnesium
They are important trace metals which are responsible for normalmetalloenzyme activity
All 4 play important role in maintaining maternal gestationalhealth and ensuring birth of healthy offspring
Some of the enzymes where zinc, copper, manganese magnesiumare linked are alcohol dehydrogenase, glucokinase, chymotrypsin,aldolases, triosephosphate isomerase, and pyruvate carboxylase...
J. Nutr. 2000; 130: 1437S—1446SComprehensive Reviews in Food Science and FoodSafety Vol.13,2014

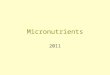
Zinc : A Necessary Micronutrient for Infantile Growth and development
Literature suggests abeneficial effect of maternalzinc supplement on
Infancy growth and developmental parameters
Neonatal immune system
Preventing infectious disease
Relationship between motherplasma zinc (Zn) and newbornlength in the supplemented group
Eur J Clin Nutr. 2004 Jan;58(1):52-9.

Important role in pregnancy for the formationof a wide variety of enzymatic and otherprocesses within the developing foetus
Lower plasma concentrations of copper, werefound in cases of spontaneous abortion,threatened abortion, missed abortion andblighted ovum.
Copper Linked to Pregnancy and Placenta
Some authors suggest that serum copper levels can be used as avery sensitive indicator of certain pathological conditions andfurther possible course of pregnancy and placental functions
Serum copper decrease leads to a reduction of elastin andcollagen resulting in premature rupture of membranes
Srp Arh Celok Lek. 2012 J;140(1-2):42-46Placenta 2000; 21:773-81Proc Nutr Soc 2004; 63(4):553-62.

Serum manganese conc. during pregnancy is significantlylower than non-pregnant women
Manganese plays a role in bone formation, protein andenergy metabolism, metabolic regulation, and functions asa cofactor in a number of enzymatic reactions
Parameters Non-pregnant Pregnant Women P-Value
Serum Mn (nmol/l) 0.102±0.02 0.090±0.01*** 0.001
*** Significant differences at P≤0.001
Biosci., Biotech. Res. Asia 2013; 10(2), 837-841
Manganese: Also Called Mothering Nutrient

Magnesium levels low in pregnancy versus non-pregnant state.
Deficiency associated Pre-eclampsia Pre-term delivery Low birth weight Increases neonatal mortality and morbidity Leg cramps, fluid retention and restless legs during pregnancy
*Biosci., Biotech. Res. Asia; 2013: 10(2), 837-841 The Indian Journal of Pediatrics 2004; 71 (11) 1003-1005
Magnesium in Pregnancy
Parameters Non-pregnant Pregnant Women
P-Value
Serum Mg (nmol/l) 1.02±0.20 0.093±0.07* 0.05
Earlier supplementation trials during pregnancy have documentedan association with
Fewer maternal hospitalizations
Reduction in pre-term delivery
Less intrauterine growth retardation
Less frequent referral of the new born to the neonatalintensive care unit.

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Dietary Reference Values of Micronutrients in Pregnancy
Srp Arh Celok Lek. 2014;142(1-2):125-130

CONTENTS
Introduction
Prevalence of Multiple Micronutrient Deficiencies
Risk Factors for Micronutrient Deficiency in Pregnancy
Function and Timing of Micronutrients that Affect Outcomesin Offspring
Are We Neglecting Few Micronutrients
Iodine
Calcium, Vitamin D
Metalloenzymes: Zinc, Copper, Manganese and Magnesium
Dietary Reference Values of Micronutrients in Pregnancy
Conclusions

Diet• Starting a healthy diet before pregnancy
• Diet - Quantity and quality
• Basic and extra nutrients for
– Maintenance of maternal health
– Needs of growing fetus
– Strength and vitality required during labour
– Successful lactation
Ref: http://www.acog.org/publications/patient_education/bp001.cfmDutta D.C. Text book of obs, 2004

Planning healthy meals• Include all food groups in diet
– Vegetables & fruits
– Milk and dairy foods
– Cereals & Grains
– Meat, beans, and eggs
– Fats and oils

Gestation is a critical opportunity for future health
• Gestation is a most critical period for future maternal and infant health, wellbeing, performance and diseases.
• Maternal undernutrition/obesity increases risk for pregnancy complications, and future health.
• Transitional diets (i.e westernization) add risk of imbalance and deficiencies, especially vs. increased calorie-dense foods and the obesity epidemic.
• Multiparous women represent especially relevant target population for nutritional support.

Micronutrient deficiencies during pregnancy are a globalpublic health concern
Although evidence has rapidly accrued about roles ofantenatal micronutrients on the health of the offspring, gapsin our knowledge still remain
Micronutrient deficiencies have been linked to pregnancyloss, preterm delivery, small birth size, birth defects, and long-term metabolic disturbances
Global Guidelines & Voice from Scientific Bodies recommendsupplementation with micronutrients during pregnancy &lactation
CONCLUSIONS


NINE MONTHS ARE WINDOW OF OPPURTUNITY
Prevention, in order to be truly preventive, must be antenatal
J. W. Ballantyne, 1902
DailyWeeklys
Pt friendly and efective drugs and combinations should be chosen
Nano particles,micillisation etc