Embed Size (px)
Citation preview

Clinical Research
Five-Year Longitudinal Assessment of the Prognosisof Apical MicrosurgeryThomas von Arx, DMD,* Simon S. Jensen, DDS,*† Stefan H€anni, DMD,‡
and Shimon Friedman, DMD§
Abstract
Introduction: Apical surgery is an important treatmentoption for teeth with post-treatment apical periodon-titis. Knowledge of the long-term prognosis is necessarywhen weighing apical surgery against alternative treat-ments. This study assessed the 5-year outcome of apicalsurgery and its predictors in a cohort for which the1-year outcome was previously reported. Methods:Apical microsurgery procedures were uniformly per-formed using SuperEBA (Staident International, Staines,UK) or mineral trioxide aggregate (MTA) (ProRoot MTA;Dentsply Tulsa Dental Specialties, Tulsa, OK) root-endfillings or alternatively Retroplast capping (RetroplastTrading, Rorvig, Denmark). Subjects examined at1 year (n = 191) were invited for the 5-year clinicaland radiographic examination. Based on blinded, in-dependent assessment by 3 calibrated examiners, thedichotomous outcome (healed or nonhealed) was deter-mined and associated with patient-, tooth-, andtreatment-related variables using logistic regression.Results: At the 5-year follow-up, 9 of 191 teeth wereunavailable, 12 of 191 teeth were extracted, and 170of 191 teeth were examined (87.6% recall rate). A totalof 129 of 170 teeth were healed (75.9%) compared with83.8% at 1 year, and 85.3% were asymptomatic. Twosignificant outcome predictors were identified: themesial-distal bone level at #3 mm versus >3 mmfrom the cementoenamel junction (78.2% vs 52.9%healed, respectively; odds ratio = 5.10; confidenceinterval, 1.67-16.21; P < .02) and root-end fillingswith ProRoot MTA versus SuperEBA (86.4% vs. 67.3%healed, respectively; odds ratio = 7.65; confidenceinterval, 2.60-25.27; P < .004). Conclusions: This studysuggested that the 5-year prognosis after apical micro-surgery was 8% poorer than assessed at 1 year. Italso suggested that the prognosis was significantlyimpacted by the interproximal bone levels at thetreated tooth and by the type of root-end filling materialused. (J Endod 2012;38:570–579)From the *Department of Oral Surgery and Stomatology, SchooSurgery, Copenhagen University Hospital, Copenhagen, Denmark; ‡PToronto, Toronto, Ontario, Canada.
Address requests for reprints to Dr Thomas von Arx, DepartmentCH-3010 Bern, Switzerland. E-mail address: [email protected]/$ - see front matter
Copyright ª 2012 American Association of Endodontists.doi:10.1016/j.joen.2012.02.002
570 von Arx et al.
Key WordsApical surgery, long-term study, outcome, predictors, prognostic factors
Apical surgery is an important endodontic treatment modality intended to curepersistent apical periodontitis (AP) after orthograde root canal treatment.
Post-treatment AP has been shown to affect up to 65% of root-filled teeth in differentpopulations (1). This highly prevalent condition is preferably treated by orthograde(nonsurgical) retreatment; however, specific benefit-risk analysis or patientpreference may favor apical surgery as the treatment of choice (2). As an alternativeto nonsurgical or surgical retreatment, the tooth can be extracted and replaced withan implant-supported restoration, with a tooth-borne fixed prosthesis, or with aremovable prosthesis (3). Thus, for teeth with post-treatment AP, patients currentlycan select from 3 contrasting treatment options. A critical consideration in thischallenging decision juncture is the prognosis, as suggested by the current bestevidence for each treatment option. This study addressed the outcome of apicalsurgery.
Over the years, over 75 studies have reported a very wide range of data on theprognosis of apical surgery using a variety of root-end filling materials and surgicaltechniques (4). Attempts to narrow the range of the reported outcomes by selectingstudies based on methodological rigor and to identify significant outcome predictorshave been reported (4, 5). In a recent systematic review and meta-analysis, Setzeret al (6) concluded that the prognosis of ‘‘endodontic microsurgery’’ including theuse of high-power illumination and magnification (microscope or endoscope);ultrasonic tips for root-end cavity preparation; and mineral trioxide aggregate(MTA), intermediate restorative material, or SuperEBA for root-end filling is signif-icantly better than that of the ‘‘traditional root-end surgery’’ performed in many ofthe studies. The reviewers suggest a 94% chance to cure post-treatment AP afterendodontic microsurgery (6); however, this conclusion is supported exclusivelyby short-term (1 or 2 years) outcome reports. Considering the 5% to 25% riskof regression to AP reported beyond 3 or more years after apical surgery(7–12), the short-term data supporting the current systematic review’s conclusions(6) may overestimate the long-term prognosis of endodontic microsurgery (4).Similarly, the assessment of significant outcome predictors requires long-termobservations as reported in only 4 studies (12–15), none of which focused onendodontic microsurgery. By reviewing the contrasting results of these 4 studiesand the recent reviews, the potential significant predictors of healing after apicalsurgery may be patient related (patient’s age over 45 years), tooth related (theabsence of preoperative signs and symptoms, adequate root filling density,
l of Dental Medicine, University of Bern, Bern, Switzerland; †Department of Oral and Maxillofacialrivate Practice, Bern, Switzerland; and §Discipline of Endodontics, Faculty of Dentistry, University of
of Oral Surgery and Stomatology, School of Dental Medicine, University of Bern, Freiburgstrasse 7,ibe.ch
JOE — Volume 38, Number 5, May 2012

Clinical Research
inadequate root filling length, a small periapical lesion of #5 mm,and the absence of a post), and treatment related (use of themicrosurgical technique) (5, 12–15).To further elucidate the prognosis of apical microsurgery and theoutcome predictors, the purpose of this prospective longitudinal studywas to provide evidence for the 5-year outcome of apical microsurgeryin a cohort of patients for whom we previously reported the 1-yearoutcome (16). Furthermore, patient-, tooth-, and treatment-relatedvariables were investigated for their outcome-predicting value toprovide clinicians with the ability to project the particular prognosisfor specific patients who consider apical microsurgery versus alterna-tive options.
Materials and MethodsThe study cohort and interventions were characterized previously
(16); however, key characteristics and details not provided previouslyare described herein to satisfy the requirement of adequate reporting.
Study CohortSubjects were recruited from among 251 patients who received
apical surgery at the Department of Oral Surgery and Stomatology,School of Dental Medicine, University of Bern, Bern, Switzerland,from January 2000 to December 2003. A total of 194 teeth in thesame number of subjects met the inclusion criteria (16) and wereenrolled in the study. This cohort is characterized for key patient-and tooth-related preoperative variables in Table 1.
InterventionOne oral surgeon (T.v.A.) who has extensive experience in per-
forming apical microsurgery provided all treatments. The surgicaltechnique was previously described in detail (16). Briefly, local anes-thesia was administered; full-thickness mucoperiosteal flap elevated;osteotomy performed; the apical 3 mm of the root resected with noor minimal bevel; the pathological tissue curetted; hemostasis estab-lished; and the root end inspected with a rigid endoscope for accessorycanals, isthmus, and cracks. Two methods of root-end managementwere used without randomized allocation: (1) a root-end cavity wasprepared with sonic microtips (Kavo Dental, Biberach, Germany)and filled with either SuperEBA (Staident International, Staines, UK)in 55 subjects (28.4%) or with ProRoot MTA (Dentsply Tulsa DentalSpecialities, Tulsa, OK) in 53 subjects (27.3%) and (2) a shallowconcavity was drilled into the root end and sealed with a resincomposite (Retroplast; Retroplast Trading, Rorvig, Denmark) bondedwith Gluma (Heraeus Kulzer, Dormagen, Germany) in the remaining 86subjects (44.3%). Flaps were secured with interrupted sutures (Sera-lon; Serrag-Wiessner, Nalla, Germany). Nonsteroidal analgesics anda 0.12% chlorhexidine-digluconate mouthwash were prescribedroutinely, whereas prophylactic antibiotics were prescribed for 61%of subjects. The main indications for antimicrobial prophylaxisincluded a history of acute infection, the presence of clinical signsand symptoms at the preoperative examination, and an anticipatedduration of surgery longer than 1 hour.
Follow-up ExaminationAt the 1-year follow-up examination, subjects were advised that
they would be contacted 4 years later for an additional clinicaland radiographic examination of the surgically treated teeth. With3 subjects lost to follow-up at the 1-year examination (16), a total of191 subjects were invited by letter to attend the 5-year examination.Those subjects who did not respond were contacted by telephoneand encouraged to attend without an offer of reimbursement.
JOE — Volume 38, Number 5, May 2012
The entire cohort of 191 subjects attending the 1-year examinationwas accounted for at the 5-year juncture. Teeth that had been extractedwere recorded along with the diagnosis at the time of extraction. Allsubjects who did not respond, declined examination, or could not bereached were considered lost to follow-up.
The treatment provider performed all follow-up examinations. Tominimize bias, the examination and data entry were performed blindedof the subject’s pre- and postoperative data. Subjects were askedto report occurrences of pain. The clinical examination recorded thepresence or absence of swelling and sinus tract and the response topercussion and palpation. Radiographs were exposed using theparalleling technique with the use of the XCP Rinn film holder (DentsplyRinn, Elgin, IL) to assess the periapical status.
Outcome AssessmentOutcome was assessed based on clinical and radiographic
measures. Radiographs were interpreted independently by 2examiners (S.H. and S.S.J.) and by the treatment provider who wereall previously calibrated for use of the healing classification describedby Molven et al (17). Calibration included the radiographic assessmentof sample cases using the schematic depiction of the healing categories(17). Intra- and interexaminer agreement was assessed using the Cohenkappa statistics.
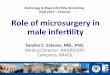
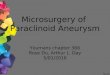
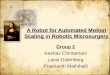
The radiographic evidence of periapical healing was classifiedas complete (Fig. 1), incomplete (scar tissue formation, Fig. 2),uncertain (Fig. 3), or unsatisfactory (Fig. 4) in strict adherence towell-established universal criteria (17, 18). Interpretation conflictswere resolved by reaching consensus among the 3 examiners. Toascertain that all allocations to the ‘‘incomplete healing’’ categorywere appropriate, the teeth in this category underwent additionalindependent scrutiny by a fourth examiner (S.F.).
With the tooth considered as the evaluated unit and mul-tirooted teeth classified according to the worst-appearing root, theoutcome was defined by combining the clinical and radiographicmeasures (19). Teeth were classified as ‘‘healed’’ when presentingwith complete or incomplete healing without clinical signs andsymptoms. Teeth were classified as ‘‘not healed’’ when presentingwith uncertain or unsatisfactory healing or with clinical signs or symp-toms regardless of the radiographic appearance. In addition to thehealing outcome, teeth were classified as ‘‘functional’’ based on theabsence of clinical signs and symptoms regardless of the radiographicappearance.
Statistical AnalysisPercent frequencies were generated to characterize the study
material in regards to 14 independent variables: patient related(ie, age, sex, and smoking), tooth related (ie, tooth type, pain, clinicalsigns/symptoms [tenderness to palpation or percussion, swelling, andsinus tract], size of periapical lesion, interproximal bone level, apicalextent of root canal filling, post, and previous apical surgery), and treat-ment related (ie, antibiotic prescription, root-end filling material, andinitial postoperative healing).
Interexaminer agreement was assessed with the Cohen weightedkappa statistics. All statistical analyses were performed with the softwareR version 2.12.2 (The R Foundation for Statistical Computing, Vienna,Austria). The dependent variable, the dichotomous outcome (healed vsnonhealed), was assessed for associations with all 14 measured in-dependent variables using multivariate analysis. Logistic regressionmodels were constructed to identify significant outcome predictorswhile accounting for confounding associations and extraneous vari-ables. Significance was established at the 5% level. Because of the
5-Year Outcome of Apical Surgery 571

TABLE 1. Preoperative Characteristics of the Inception Cohort (n = 194) and the Healed Outcome at 1 Year (n = 191) and 5 Years (n = 170) after ApicalMicrosurgery Related to Potential Outcome Predictors
Variable
Inceptioncohort 1-year follow-up 5-year follow-up
n % n n Healed % healed n Healed % healed
Total 194 100 191 160 83.8 170 129 75.9Age<45 years 60 30.9 60 54 90.0 56 44 78.6$45 years 134 69.1 131 106 80.9 114 85 74.6
SexMale 86 44.3 85 68 80.0 76 54 71.1Female 108 55.7 106 92 86.8 94 75 79.8
SmokingNo 141 72.7 139 116 83.5 123 97 78.9Yes 53 27.3 52 44 84.6 47 32 68.1
TeethMaxilla anteriors 55 28.4 54 46 85.2 52 43 82.7Premolars 43 22.2 42 35 83.3 34 27 79.4Molars 25 12.9 24 22 91.7 23 16 69.6Mandible anteriors 6 3.1 6 6 100 2 1 50.0Premolars 13 6.7 13 10 76.9 12 10 83.3Molars 52 26.8 52 41 78.8 47 32 68.1
PainAbsent 111 57.2 109 97 89.0 98 76 77.6Present 83 42.8 82 63 76.8 72 53 73.6
SignsAbsent 116 59.8 114 101 88.6 103 77 74.8Tender to percussion 30 15.5 30 25 83.3 23 19 82.6Swelling, sinus tract 48 24.7 47 34 72.3 44 33 75.0
Lesion sizeNo lesion 17 8.8 17 16 94.1 16 14 87.5#5 mm 106 54.6 104 90 86.5 91 74 81.3>5 mm 71 36.6 70 54 77.1 63 41 65.1
Crestal bone level*Mesial and distal #3 mm 150 77.3 148 123 83.1 133 104 78.2Mesial or distal >3 mm 24 12.4 24 21 87.5 20 16 80.0Mesial and distal >3 mm 20 10.3 19 16 84.2 17 9 52.9
Apical extent of root canal filling0-2 mm short of apex 126 64.9 123 103 83.7 108 84 77.8>2 mm short of apex 44 22.7 44 39 88.6 41 30 73.2Beyond the apex 24 12.4 24 18 75.0 21 15 71.4
PostAbsent 64 33.0 63 53 84.1 53 41 77.4Present 130 67.0 128 107 83.6 117 88 75.2
Previous surgeryNo 176 90.7 173 146 84.4 154 118 76.6Yes 18 9.3 18 14 77.8 16 11 68.8
AntibioticsNot prescribed 72 64 88.9 62 51 82.3Prescribed 119 96 80.7 108 78 72.2
Root-end fillingSuperEBA 55 42 76.4 49 33 67.3ProRoot MTA 51 46 90.2 44 38 86.4Retroplast 85 72 84.7 77 58 75.3
Postoperative healingUneventful 174 148 85.1 156 120 76.9Complication 17 12 70.6 14 9 64.3
*Measured on radiographs from the cementoenamel junction or, if not visible, from the margin of a crown or filling.
Clinical Research
exploratory type of the study, no P value correction for multiplecomparisons was performed.
ResultsAttrition of the cohort at the 5-year follow-up examination is
summarized in Table 2. A total of 170 of 194 subjects (87.6%) withthe same number of treated teeth were available for re-examination after5 years. Information was available for an additional 12 teeth (6.2%) thatwere extracted because of fracture or prosthetic considerations
572 von Arx et al.
unrelated to the surgical treatment performed. Three subjects (1.5%)could not be reached, 6 subjects (3.1%) did not respond, and 3subjects (1.5%) did not attend the 1-year examination. The total lossto follow-up from baseline to 5 years was 24 subjects (12.4%) includingthe extracted teeth.
Interexaminer AgreementKappa values of pair-wise comparisons among the 3
examiners with regard to radiographic healing classification ranged
JOE — Volume 38, Number 5, May 2012

Figure 1. Mandibular first molar radiographically assessed as ‘‘complete healing’’ 5 years after apical microsurgery with ProRoot MTA root-end filling. (A) Preop-erative and (B) postoperative: in the mesial root, both canals and the isthmus were prepared and filled, whereas in the distal root 1 canal was prepared and filled.(C) The 1-year follow-up and (D) the 5-year follow-up.
Clinical Research
from 0.59 to 0.74, indicating fair to good agreement. A good to excellentagreement was observed between each examiner’s classificationand the consensus classification, with kappa values ranging from0.74 to 0.92.
OutcomeFive years after apical microsurgery, 129 of 170 teeth (75.9%)
were classified as healed compared with 83.8% at 1 year after treatment.Taking into account the absence of clinical signs or symptoms, 145 of170 teeth (85.3%) were classified as ‘‘functional’’ 5 years after apicalsurgery. Distribution of the radiographic classification categories forthe 170 teeth examined at 5 years is summarized in Table 3. Of 141 teethclassified as complete/incomplete healing at 1 year, 125 teeth (88.7%)remained so at 5 years, whereas 16 teeth (11.3%) regressed to uncer-tain /unsatisfactory healing at 5 years. Conversely, of 29 teeth classifiedas uncertain/unsatisfactory healing at 1 year, 5 teeth (17.2%) pro-gressed to complete/incomplete healing. On balance, the number ofteeth classified as complete/incomplete healing decreased from 141teeth at 1 year to 130 teeth at 5 years after treatment, a reductionof 7.8%. With regard to root-end filling materials, regression to
JOE — Volume 38, Number 5, May 2012
uncertain/unsatisfactory healing was lowest in teeth treated withProRoot MTA.
Outcome PredictorsThe following variables were associated with healed rate dif-
ferences of 10% or larger (considered clinically meaningful) at 5 years:
1. Patient related: smoking status2. Tooth related: the type of tooth, the size of the lesion, and the crestal
bone level3. Treatment related: the type of root-end filling material, antibiotic
treatment, and the postoperative healing course
The final logistic regression model revealed 1 tooth-related and 1treatment-related statistically significant predictor of a healed outcome:mesial-distal crestal bone level at #3 mm versus >3 mm from thecementoenamel junction (78.2% vs 52.9% healed, respectively; oddsratio = 5.10; confidence interval, 1.67–16.21; P < .02) and root-endfillings with ProRoot MTA versus SuperEBA (86.4% vs 67.3% healed,respectively; odds ratio = 7.65; confidence interval, 2.60–25.27;P < .004; Tables 1 and 4).
5-Year Outcome of Apical Surgery 573

Figure 2. The maxillary lateral incisor radiographically assessed as ‘‘incomplete healing’’ 5 years after apical microsurgery with ProRoot MTA root-end filling.(A) Preoperative, (B) postoperative, (C) 1-year follow-up, and (D) 5-year follow-up.
Clinical Research
DiscussionThis prospective longitudinal study evaluated the 5-year prognosis
of apical microsurgery in a cohort for whom the 1-year data have beenreported previously (16). The study design was consistent with themethodology requirements for the assessment of prognosis at a highlevel of evidence. The study cohort was recruited, treated, andfollowed-up prospectively, with data reported for subjects attendingboth the 1-year (16) and 5-year examinations. The roughly 12% attri-tion of the inception cohort was lower than the 22% to 49% loss to
574 von Arx et al.
follow-up reported in other relatively current apical surgery studieswith comparable observation periods (8, 10–12, 14, 15, 20). The88% recall rate achieved was consistent with the requirement forthe second highest level of evidence (1b) for the assessment ofprognosis (21). Only 1 tooth per subject was included and consideredthe unit of evaluation, and teeth presenting with through-and-through orapicomarginal lesions were excluded to ascertain uniformity of thecohort and to avoid potential confounding of the results. Patient- andtooth-related data collection followed a detailed protocol; however,
JOE — Volume 38, Number 5, May 2012

Figure 3. The mandibular first molar radiographically assessed as ‘‘uncertain healing’’ 5 years after apical microsurgery with Retroplast root-end capping.(A) Preoperative and (B) postoperative: both resected root faces were sealed including an isthmus in the mesial root. (C) The 1-year follow-up and (D) the5-year follow-up.
Clinical Research
the inception cohort was not characterized in regards to AP persistingafter the initial treatment only or after retreatment as would have beendesired (4). Although the prognosis of apical surgery was better whenAP persisted after retreatment than after initial treatment in 1 study (22),this variable was not a significant outcome predictor in anotherstudy (15).
To standardize interventions, 1 provider treated all subjects, andall teeth were root-end filled following a uniform surgical protocol.Because the root-end filling techniques were not randomly allocated,the level of evidence for comparing their effectiveness was lower(2b) than would be provided by a randomized controlled trial (21).
To ascertain objective outcome assessment, 2 independent exam-iners and the treatment provider interpreted the radiographic imagesblinded to the preoperative appearance. Blinding of root-end fillingmaterials was not entirely possible because of the different radiographicappearance of the 3 materials used. Stents were not manufactured tofacilitate reproducible radiographic exposures, as was the case in themajority of apical surgery outcome studies; nevertheless, radiographswere positioned with a film holder, and the paralleling exposuretechnique was used to reduce distortion.
JOE — Volume 38, Number 5, May 2012
Different patient-, tooth-, and treatment-related variables wereexplored for association with the outcome, and significant outcomepredictors were identified using a multivariate analysis. Because thisstudy followed up the cohort for whom the 1-year data were available,no sample size calculation was performed, and no specific sample sizetarget was set.
The overall 5-year healed rate of 76% (129/170 subjects)compared well with the 4- to 10-year healed rate of 74% reported inthe Toronto Study (15). In that study, not all subjects were treated usingthe apical microsurgical technique, and 84% of teeth were root-endfilled with ProRoot MTA, intermediate restorative material, or SuperEBAwithout a significant difference in outcome (15). In current years, onlya few apical surgery studies assessed the outcomes of 4 years or longer(10–15, 20, 22, 23), whereas there have been many short-term studies(4). Especially in the past decade, many studies have reported onthe outcome of apical microsurgery (6), albeit with only short-term(#2 years) follow-up. Short-term observation after apical surgerymay overestimate the prognosis (4) because 5% to 25% of teeth re-corded as healed at the short-term have been reported to regresswhen observed 3 years or longer after surgery (7–12). In the
5-Year Outcome of Apical Surgery 575

Figure 4. The mandibular first molar radiographically assessed as ‘‘unsatisfactory healing’’ 5 years after apical microsurgery with Retroplast root-end capping. (A)Preoperative and (B) postoperative: the resected root face of the mesial root was sealed including the isthmus. (C) The 1-year follow-up and (D) the 5-year follow-up.
Clinical Research
present apical microsurgery study, regression occurred inapproximately 11% of teeth assessed as healed at 1 year. Thisregression was partially offset by fewer teeth that were healed at 5years but not at 1 year. The overall healed rate 5 years after apicalmicrosurgery was 8% lower than it was after 1 year, underlining theoverestimated prognosis suggested by short-term studies on apicalmicrosurgery (4).
One tooth-related variable was identified as an outcomepredictor for which the prospective study design provided a high levelof evidence (1b). Teeth that presented with no or minor interprox-imal bone loss both mesially and distally had a higher healed ratethan teeth with greater interproximal bone loss (78% vs 53%, respec-tively). This finding corroborated the previously reported adverseeffect of compromised bone support on the prognosis after apicalsurgery (4, 24, 25). The risk, especially in the longer-term, is thatan apicomarginal bacterial pathway may develop over time whenthe crestal bone level is already compromised at the time of apicalmicrosurgery (24). Such communication may not only compromiseperiapical healing, but it can also lead to a significant loss of peri-odontal attachment in the long-term, as observed in teeth that didnot heal after apical microsurgery (26). Therefore, from the clinical
576 von Arx et al.
perspective, the supporting bone level should be assessed preopera-tively and carefully considered before the tooth is subjected to apicalmicrosurgery (24).
Although not a randomized controlled trial, this 5-year studyoffered an opportunity to examine the effectiveness of the 3 root-endfilling materials; ProRoot MTA (86% healed) was shown to be superiorto SuperEBA (67% healed). Several shorter-term apical microsurgerystudies have reported high success rates using ProRoot MTA rangingfrom 89% to 97% (16, 20, 24, 25, 27–30). Three of these studies(24, 27, 29) contributed to the conclusion in the recent systematicreview that the success rate of apical microsurgery was 94.5% (6).In the present study, ProRoot MTA-treated teeth showed the leastregression at 5 years (just under 4%), suggesting the most effectiveseal over the longer observation period. Of the teeth treated withProRoot MTA, 86% were healed at 5 years. In the absence of any othercomparable long-term studies, our results suggested that, at best, thechance of teeth to heal in the longer-term after apical microsurgeryusing ProRoot MTA would be 86%, which is lower than the 94% sug-gested in the recent systematic review (6). This suggested prognosisis far better than that reported in previous 4-year or longer studieson apical surgery performed with other root-end filling materials and
JOE — Volume 38, Number 5, May 2012

TABLE 2. Distribution of the Study from Inception to the 5-Year Follow-up
Population Subjects Status
Inception cohort 194 Received treatmentLost to follow-up at
1-year examination3 Did not attend
Eligible for 5-yearfollow-up
191 Invited for examination
Lost to follow-upat 5 years
9 1 deceased2 left country6 did not respond
Teeth extracted 12 11 vertical fracture1 prosthetic considerations
Attended 5-yearexamination
170 Teeth examined
Clinical Research
without emphasis on themicrosurgical technique (8, 9, 11, 12, 13, 23).Nevertheless, additional long-term, methodologically sound studies arerequired to augment the evidence for the prognosis after apical micro-surgery using ProRoot MTA.
Of the Retroplast-treated teeth in this study, about 75% werehealed after 5 years. This finding corroborated the 6- to 9-year 78%success rate reported by Yazdi et al (12). This long-term prognosis ispoorer than the 73% to 92% reported in the short-term after usingRetroplast (16, 31–35), suggesting regression over time. Indeed, ofthe 85% Retroplast-treated teeth that were healed after 1 year in ourprevious study (16), over 9% showed regression after 5 years in thecurrent study, whereas 6% regression was reported in another long-term study (12). Although conceptually apical capping with a dentin-bonded material is expected to seal potential bacterial pathways
TABLE 3. Radiographic Classification of Healing at 5 Years (n = 170) after ApicaMaterial Used
Healing classification
1 year 5 years
Category n* Category n %S
Complete 130 Complete 114 87.7Incomplete 2 1.5Uncertain 7 5.4Unsatisfactory 7 5.4Subtotal
Incomplete 11 Complete 2 18.2Incomplete 7 63.6Uncertain 1 9.1Unsatisfactory 1 9.1Subtotal
Uncertain 22 Complete 3 13.6Incomplete 1 4.6Uncertain 10 45.5Unsatisfactory 8 36.4Subtotal
Unsatisfactory 7 Complete 1 14.3Incomplete 0 –Uncertain 0 –Unsatisfactory 6 85.7Subtotal
Total (n) 170 Complete 120 70.6Incomplete 10 5.9Uncertain 18 10.6Unsatisfactory 22 12.9
Total of healed cases after 5 years (129/170, Table 1) differs from the total number of cases with com
radiographic healing presented with clinical symptoms.
%S, proportion of subtotal filled with given material.
Healing classification according to Molven et al.17
*n excludes 21 subjects lost to follow-up.
JOE — Volume 38, Number 5, May 2012
between the root canal and periapical tissues (31), the application ofRetroplast is highly technique sensitive. Possibly, contamination ofthe resected root surface or trimming of excess material in some casesmay compromise the seal and the prognosis.
Teeth root ends filled with SuperEBA showed the lowest healedrate (ie, 67%) 5 years after apical microsurgery, which is significantlylower than for ProRoot MTA-treated teeth. This 5-year prognosis was10% better than reported in a previous 3-year study (36) but about20% poorer than reported in 2 other long-term studies using SuperEBA(23, 37). However, methodological issues, such as the use of the root asthe evaluated unit in both studies (23, 37) and a large loss to follow-up(37), precluded direct comparisons of our results with those of theprevious studies (4). Of the 76% SuperEBA-treated teeth that werehealed after 1 year in our previous study (16), 9% showed regressionafter 5 years in the current study, which is similar to the 8.5% regressionreported 5 to 7 years after apical microsurgery (10). Again, the highshort-term success rates of up to 97% reported using SuperEBA(6, 16, 37, 20–22, 24) misrepresents the longer-term prognosis.
Taking into account the absence of clinical signs or symptoms,85% (145/170) of the teeth were ‘‘functional’’ 5 years after apicalmicrosurgery although only 76% were healed. The difference of 9%between these 2 outcome measures was lower than the 20% difference(94% and 74%, respectively) reported in the Toronto Study (15).Nevertheless, these findings underlined the frequent absence of clinicalsigns and symptoms associated with post-treatment apical periodontitis(4, 14, 15) and the importance of radiographic examination tocomprehensively assess the outcome of treatment. According toBarone et al (15), patients weighing different treatment alternativesfor teeth with post-treatment apical periodontitis should be informed
l Microsurgery Related to Classification at 1 Year and the Root-end Filling
Root-end filling material
SuperEBA ProRoot MTA Retroplast
n %S n %S n %S
28 84.8 31 91.2 55 87.31 3.0 1 2.9 0 –3 9.1 1 2.9 3 4.81 3.0 1 2.9 5 7.9
33 34 631 20.0 1 20.0 0 –3 60.0 3 60.0 1 1001 20.0 0 – 0 –0 – 1 20.0 0 –5 5 11 12.5 1 33.3 1 9.10 – 1 33.3 0 –3 37.5 1 33.3 6 54.54 50.0 0 – 4 36.48 3 110 – 0 – 1 50.00 – 0 – 0 –0 – 0 – 0 –3 100 2 100 1 50.03 2 2
30 61.2 33 75.0 57 74.04 8.2 5 11.4 1 1.37 14.3 2 4.5 9 11.78 16.3 4 9.1 10 13.0
plete and incomplete radiographic healing after 5 years (130/170) because 1 case with complete
5-Year Outcome of Apical Surgery 577

TABLE 4. The Final Logistic Regression Model Identifying 2 SignificantPredictors of the Healed Outcome 5 Years after Apical Microsurgery
VariableOddsratio
Confidenceinterval
Pvalue
Crestal bone level*(0 = >3 mm,1 = #3 mm) 5.10 1.67-16.21 .017
Root-end filling(0 = SuperEBA,1 = ProRoot MTA)
7.65 2.60-25.27 .003
All other variables listed in Table 1 were rejected in the series of logistic regression models
constructed.
*Measured on radiographs from the cementoenamel junction or, if not visible, from the margin of a
crown or filling.
Clinical Research
about the high probability of retaining asymptomatic function 5 yearsafter apical microsurgery even if radiographs do not suggest the teethto be healed. Such information can assist the patients, especiallythose experiencing preoperative symptoms, in relating the pro-jected outcomes to their individual values and in setting specificgoals they hope to achieve by having the teeth treated by apical micro-surgery.
As highlighted earlier, this longitudinal study provided insightinto the dynamics of healing and its regression beyond the firstyear after apical microsurgery, suggesting overestimation of the prog-nosis by short-term assessment. In previous longitudinal studies inwhich treatment was not consistent with apical microsurgery (6),the 1-year assessment predicted the 5-year prognosis with an accu-racy of 91% (7) and 95% (8), which is similar to the 95% predictiveaccuracy reported in a current 6- to 9-year study (12) and the 90%predictive accuracy reported herein. In the longer-term, regressionfrom healed to nonhealed in some teeth (16 in the present study)is partially offset by continued healing of fewer teeth (5 in the presentstudy) that are not healed in the short-term. Thus, the short-termoutcomes of apical microsurgery cannot be taken as reportedbecause they overestimate the long-term prognosis, but they canbe extrapolated to project the long-term prognosis at roughly 90%to 95%.
Although the long-term prognosis can be projected from short-term outcomes, the long-term outcome predictors were differentfrom those observed at 1 year. Preoperative pain was the sole outcomepredictor at 1 year (16), whereas 2 other predictors emerged at 5 years.This finding contested the ability of short-term studies to determineoutcome predictors of apical microsurgery, as observed in the superi-ority of ProRoot MTA over SuperEBA in the long-term (19% differencein healed rate) but not in the short-term (14% difference in healedrate).
Two previous long-term studies assessed the outcome predictorsof apical surgery using multivariate analysis (13, 15). In the 4- to10-year prospective Toronto Study (15), predictors of healing includedpatient age over 45 years, inadequate root canal filling, and crypt size of10 mm or less, whereas in the 4-year retrospective study by Rahbaranet al (13) predictors of healing included the absence of preoperativeradiolucency, the absence of a post, adequate coronal restoration,adequate quality of apical surgery, and placement of a root-end filling.Neither study found the root-end filling material significant (the inter-proximal bone level was not assessed), whereas the present study didnot support the 8 outcome predictors suggested by the 2 other studies(13, 15). This discord could be attributed to differences in treatmenttechniques. Although the apical microsurgery technique (6) wasused in the present study, it was not consistently used in the other 2studies (13, 15).
578 von Arx et al.
Several patient-, tooth-, and treatment-related variables (ie,smoking, tooth location, lesion size, 1-sided interproximal bone loss,antibiotic coverage, and postoperative healing course) were associatedwith 5-year healed rate differentials of 10% or greater, which areconsidered clinically meaningful. According to the multivariate analysis,these variables did not significantly impact the outcome. The lack ofsignificance might have been caused by uneven distributions of subsetsof the cohort across each variable, but it might also suggest thatthe differences might be random.
ConclusionsThis study provided a high level (1b) of evidence for the 5-year
prognosis after apical microsurgery, with 76% of the teeth healed.The healed rate was 8% lower than the reported 1-year rate for thesame cohort, with 16 teeth (12% of the cohort) regressing and 5 teeth(3% of the cohort) progressing from the first to fifth year after treat-ment. One tooth-related outcome predictor was identified: the healedrate was higher when the mesial and distal interproximal bone levelwas #3 mm from the cementoenamel junction (or restorationmargin). Another treatment-related outcome predictor was supportedby a lower level of evidence (2b): the healed rate was higher for root-end fillings with ProRootMTA (86%) than with SuperEBA (67%). Thereis an urgent need for additional prospective studies to augment theevidence for the long-term prognosis of apical microsurgery and toassess the root-end filling materials and other intervention aspects ofapical microsurgery at high-level evidence.
AcknowledgmentsThe authors thank Dr. J€urg H€usler and Kasper Stucki, Institute
of Mathematical Statistics and Actuarial Science, University ofBern, Bern, Switzerland, for the statistical analysis.
The authors deny any conflicts of interest related to this study.
References1. Eriksen HM, Kirkevang L-L, Petersson K. Endodontic epidemiology and treatment
outcome: general considerations. Endod Topics 2002;2:1–9.2. Friedman S. Considerations and concepts of case selection in the management of
post-treatment endodontic disease (treatment failure). Endod Topics 2002;1:54–78.3. Bigras BR, Johnson BR, BeGole EA, Wenckus CS. Differences in clinical decision
making: a comparison between specialists and general dentists. Oral SuSrg OralMed Oral Pathol Oral Radiol Endod 2008;106:139–44.
4. Friedman S. The prognosis and expected outcome of apical surgery. Endod Topics2005;11:219–61.
5. von Arx T, Penarrocha M, Jensen SS. Prognostic factors in apical surgery withroot-end filling: a meta-analysis. J Endod 2010;36:957–73.
6. Setzer FC, Shah SB, Kohli MR, Karabucak B, Kim S. Outcome of endodontic surgery:a meta-analysis of the literature—part 1: comparison of traditional root-endsurgery and endodontic microsurgery. J Endod 2010;36:1757–65.
7. Halse A, Molven O, Grung B. Follow-up after periapical surgery: the value of theone-year control. Endod Dent Traumatol 1991;7:246–50.
8. Jessl�en P, Zetterqvist L, Heimdahl A. Long-term results of amalgam versus glassionomer cement as apical sealant after apicectomy. Oral Surg Oral Med Oral PatholOral Radiol Endod 1995;79:101–3.
9. Kvist T, Reit C. Results of endodontic retreatment: a randomized clinical studycomparing surgical and nonsurgical procedures. J Endod 1999;25:814–7.
10. Rubinstein RA, Kim S. Long-term follow-up of cases considered healed one yearafter apical microsurgery. J Endod 2002;28:378–83.
11. Wesson CM, Gale TM. Molar apicectomy with amalgam root-end filling: results ofa prospective study in two district general hospitals. Br Dent J 2003;195:707–14.
12. Yazdi PM, Schou S, Jensen SS, Stoltze K, Kenrad B, Sewerin I. Dentine-bonded resincomposite (Retroplast) for root-end filling: a prospective clinical and radiographicstudy with a mean follow-up period of 8 years. Int Endod J 2007;40:493–503.
13. Rahbaran S, Gilthorpe MS, Harrison SD, Gulabivala K. Comparison of clinicaloutcome of periapical surgery in endodontic and oral surgery units of a teachingdental hospital: a retrospective study. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2001;91:700–9.
JOE — Volume 38, Number 5, May 2012

Clinical Research
14. Wang N, Dao TT, Knight K, Friedman S. Treatment outcome in endodontics: the Tor-onto Study. Phases I and II: apical surgery. J Endod 2004;30:751–61.15. Barone C, Dao TT, Basrani BB, Wang N, Friedman S. Treatment outcome in
endodontics: the Toronto study—phases 3, 4, and 5: apical surgery. J Endod2010;36:28–35.
16. von Arx T, Jensen SS, H€anni S. Clinical and radiographic assessment of variouspredictors for healing outcome one year after periapical surgery. J Endod 2007;33:123–8.
17. Molven O, Halse A, Grung B. Observer strategy and the radiographic classification ofhealing after endodontic surgery. Int J Oral Maxillofac Surg 1987;16:432–9.
18. Rud J, Andreasen JO, Jensen JE. Radiographic criteria for the assessment of healingafter endodontic surgery. Int J Oral Surg 1972;1:195–214.
19. Zuolo ML, Ferreira MO, Gutmann JL. Prognosis in periradicular surgery: a clinicalprospective study. Int Endod J 2000;33:91–8.
20. Song M, Shin S-J, Kim E. Outcomes of endodontic micro-resurgery: a prospectiveclinical study. J Endod 2011;37:316–20.
21. Oxford Centre for Evidence-based Medicine—Levels of Evidence. Available at:http://www.cebm.net/index.aspx?o=1025. Accessed November 25, 2011.
22. Taschieri S, Machtou P, Rosano G, Weinstein T, Del Fabbro M. The influence ofprevious non-surgical re-treatment on the outcome of endodontic surgery. MinervaStomatol 2010;59:625–32.
23. Gagliani MM, Gorni FGM, Strohmenger L. Periapical resurgery versus periapicalsurgery: a 5-year longitudinal comparison. Int Endod J 2005;38:320–7.
24. Kim E, Song JS, Jung IY, Lee SJ, Kim S. Prospective clinical study evaluatingendodontic microsurgery outcomes for cases with lesions of endodontic origincompared with cases with lesions of combined periodontal-endodontic origin.J Endod 2008;34:546–51.
25. Saunders WP. A prospective clinical study of periradicular surgery using mineraltrioxide aggregate as a root-end filling. J Endod 2008;34:660–5.
26. von Arx T, Al-Saeed M, Salvi GE. Five-year changes in periodontal parameters afterapical surgery. J Endod 2011;37:910–8.
JOE — Volume 38, Number 5, May 2012
27. Chong BS, Pitt Ford TR, Hudson MB. A prospective clinical study of mineral trioxideaggregate and IRM when used as root-end filling materials in endodontic surgery.Int Endod J 2003;36:520–6.
28. Lindeboom JAH, Frenken JWFH, Kroon FHM, van den Akker HP. A comparativeprospective randomized clinical study of MTA and IRM as root-end filling materialsin single-rooted teeth in endodontic surgery. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2005;100:495–500.
29. Christiansen R, Kirkevang L-L, Hørsted-Bindslev P, Wenzel A. Randomized clinicaltrial of root-end resection followed by root-end filling with mineral trioxide aggre-gate or smoothing of the orthograde gutta-percha root filling—1-year follow up. IntEndod J 2009;42:105–14.
30. von Arx T, H€anni S, Jensen SS. Clinical results with two different methods of root-endpreparation and filling in apical surgery: mineral trioxide aggregate and adhesiveresin composite. J Endod 2010;36:1122–9.
31. Rud J, Munksgaard EC, Andreasen JO, Rud V, Asmussen E. Retrograde root fillingwith composite and a dentin-bonding agent. 1. Endod Dent Traumatol 1991;7:118–25.
32. Rud J, Rud V, Munksgaard EC. Retrograde root filling with dentin-bonded modifiedresin composite. J Endod 1996;22:477–80.
33. Rud J, Rud V, Munksgaard EC. Effect of root canal contents on healing of teeth withdentin-bonded resin composite retrograde seal. J Endod 1997;23:535–41.
34. Rud J, Rud V, Munksgaard EC. Periapical healing of mandibular molars afterroot-end sealing with dentine-bonded composite. Int Endod J 2001;34:285–92.
35. Jensen SS, Nattestad A, Egdo P, Sewerin I, Munksgaard EC, Schou S. A prospective,randomized, comparative clinical study of resin composite and glass ionomercement for retrograde root filling. Clin Oral Investig 2002;6:236–43.
36. Pantschev A, Carlsson AP, Andersson L. Retrograde root filing with EBA cement oramalgam. Oral Surg Oral Med Oral Pathol 1994;78:101–4.
37. Rubinstein RA, Kim S. Short-term observation of the results of endodontic surgerywith the use of a surgical operation microscope and Super-EBA as root-end fillingmaterial. J Endod 1999;25:43–8.
5-Year Outcome of Apical Surgery 579