Embed Size (px)
DESCRIPTION
details of mitral valve repair
Citation preview

MITRAL VALVE REPAIR AND RELATED ASPECTS
Dr Dheeraj sharma M.Ch (CTVS) Resident

History of mitral valve repair
Sir Thomas Lauder Brunton, a Scottish physician, first introduced the concept of surgical repair of the mitral valve in 1902.
Elliot Cutler ,Professor of Surgery at the Peter Bent Brigham Hospital in Boston, performed the world’s first successful mitral valve operation in 1923 by carrying out a transventricular commissurotomy with a neurosurgical tenotomy knife.
Henry Souttar of England performed a single successful transatrial finger commissurotomy in 1925.
Surgical treatment of mitral regurgitation for prolapse was first introduced in the 1950s.

History
Harold and kay obliterated the commisures using sequence of mattress sutures.
Paneth and devega did the annuloplasty by taking the circumferential sutures around the annulus.
In 1960 McGoon proposed the resection of part of leaflets with ruptured chordae as a part of repair.
Carpentier and Duran started the use of prosthetic rings to remodel the mitral valve annulus.



Ethiology
Organic
• Degenerative• Barlow’s• Dystrophic• Marfan’s• Other
• Endocarditis• Rheumatic• Post-traumatic
Functional
• Ischemic• DCM• Secondary to
AS

Indications of intervention in MR
RECOMMENDATION COR LOE
MV surgery is recommended for symptomatic patients with chronic severe primary MR (stage D) and LVEF >30%
I B
MV surgery is recommended for asymptomatic patients with chronic severe primary MR and LV dysfunction (LVEF 30%–60% and/or LVESD ≥40 mm, stage C2)
I B
MV repair is recommended in preference to MVR when surgical treatment is indicated for patients with chronic severe primary MR limited to the posterior leaflet
I B
MV repair is recommended in preference to MVR when surgical treatment is indicated for patients with chronic severe primary MR involving the anterior leaflet or both leaflets when a successful and durable repair can be accomplished
I B
Concomitant MV repair or replacement is indicated in patients with chronic severe primary MR undergoing cardiac surgery for other indications .
I B

MV repair is reasonable in asymptomatic patients with chronic severe primary MR (stage C1) with preserved LV function (LVEF >60% and LVESD <40 mm) in whom the likelihood of a successful and durable repair without residual MR is >95% with an expected mortality rate of <1% when performed at a Heart Valve Center of Excellence
IIA B
MV repair is reasonable for asymptomatic patients with chronic severe nonrheumatic primary MR (stage C1) and preserved LV function in whom there is a high likelihood of a successful and durable repair with 1) new onset of AF or 2) resting pulmonary hypertension (PA systolic arterial pressure >50 mm Hg)
IIA B
Concomitant MV repair is reasonable in patients with chronic moderate primary MR (stage B) undergoing cardiac surgery for other indications
IIA C
MV surgery may be considered in symptomatic patients with chronic severe primary MR and LVEF 30% (stage D)
IIB C
MV repair may be considered in patients with rheumatic mitral valve disease when surgical treatment is indicated if a durable and successful repair is likely or if the reliability of long-term anticoagulation management is questionable
IIB B
Transcatheter MV repair may be considered for severely symptomatic patients (NYHA class III/IV) with chronic severe primary MR (stage D) who have a reasonable life expectancy but a prohibitive surgical risk because of severe comorbidities
IIB B
MVR should not be performed for treatment of isolated severe primary MR limited to less than one half of the posterior leaflet unless MV repair has been attempted and was unsuccessful
III B

Indication for intervention in MS


Treatment options
1. mitral valve replacement. 2. mitral valve repair

MV repair is superior to MVR
• Better preservation of LV function• Avoidance of prosthesis related events(hazards of
anticoagulation, stroke, endocarditis, short life span of bioprosthesis, poor patient compliance)
• Reduced hospital mortality• Reduced morbidity and LOS• Improved long term survival
Thourani et al, Circulation 2003; 108:298-304Zaho et al, JTCVS 2007;1257-1263Shuhaiber J et al, EJCTS 2007; 31:267-275Perrier P et al, Circulation 1984;70:187Akins CW, et al. ATS 1994; 58:668-676

General principles of mitral valve repair
1. create apposition of anterior and posterior leaflet in systole.
2. increase the valve mobility 3. prevent valve stenosis 4. reduce the annular dilatation 5. remodel the annulus 6. remove all the infective foci in case of
endocarditis.

Myxomatous mitral valve
Myxomatous mitral valve disease is most common indication of mitral valve surgery .
90% of the mitral valves are amneble to surgical repair.
Features of myxomatous mitral valve:1. Dilated annulus2. Elongated redundant leaflets3. Chordae may be thin or thick, ruptured
or elongated

Surgical indications
Symptomatic patients with mitral valve disease and 3+ and 4+ regurgitation.
Asymptomatic patients with 3+ or 4+ regurgitation and evidence of decreased LV function demonstrated by LV dilatation and decreased EF and new onset atrial fibrillation.

Myxomatous mitral valve disease
Principles of repair includes:1. Apposition of anterior and posterior
leaflet in systole.2. Reducing the height of posterior
leaflet(most critical step).3. Stabilizing the AML (by repair or
replacement of chordae).4. Remodelling the annulus by prosthetic
ring.

In case of the myxomatous mitral valve disease in around 80% of cases it is the PML which is involved (especially p2) and in 20% cases pathology involves AML.
if we deal with the PML and annulus effectively ,AML can be left intact . Repair of AML is required in specific situations.

Posterior leaflet prolapse/flail
Quadrangular resection
Sliding plasty(leaflet advancement technique)
Chordal replacement Anterior leaflet
commissuroplasty Folding plasty

1. Quadrangular resection
This technique is used when posterior leaflet is markedly elongated specifically P2 sgment.
Here we perform a limited resection of the involved segment removing minimal number of adjascent chordae and much of the supporting structures. This effectively reduce the height of PML.
The area is excised in trapezoid or quadrangular shape with narrowest portion of trapezoid at the annulus.

After resection the remaining parts of the leaflet are brought together by suturing the leaflet to annulus and to each other directly.
First the two annular stitches are brought together by running sutures followed by approximating the leaflet parts from tip to annulus.
Disadvantage: 1. Distortion of annulus if the involved
segment is large.


2. Leaflet advancement technique(sliding plasty)
With this technique one incorporates excess tissue from remaining segments of posterior leaflet, bringing the remaining segments together and at same time preserving as many chordae .
Here after quadrangular resection the incision given along the annulus in remaining leaflet tissue upto both the commissure followed by gradual reattachmentof leaflet to annulus by advancing the remaining leaflet in space vacated by resected tissue.

This technique allows remodeling of tissue which can be easily adjusted to residual tissue and height of leaflet.
Pledgeted sutures are not used as they cause scarring and provide a site for potential thrombus formation.
Running sutures along the annulus margin are important as they help to reduce the height of posterior leaflet.
Any annular distortion is taken care by annuloplasty ring.

Placing annuloplasty ring is final step of basic mitral valve repair.
Most important aspect of ring selection is to find exact size and shape .
To exactly size the ring there are two methods:
1. Intertrigonal distance2. The height of anterior leaflet.


To mark the two trigones we first place U stitches at the two trigones . These stitches help to stabilize the intertrigonal area for exact sizing.
Rings can be implanted by running sutures but most commonly deep intraventricular annular mattress sutures are placed.
9-11 sutures are usually sufficient to completely encircle even the most dilated valves.

For myxomatous mitral valve disease it is better to upsize the ring rather than downsizing so as to minimizing the possibility of development of SAM.



3. Anterior leaflet commissuroplasty
This technique is used when the commissural part of the posterior leaflet is prolapsed .
Here we take a suture from diseased segment of posterior leaflet and pass it through the normal opposite leaflet tissue and tying the knot on the surface of leaflet thus obliterating the prolapsed segment.


4. Folding plasty technique

Anterior and Bileaflet disease
Chordal replacement Alfieri / E2E Chordal transfer Papillary muscle
repositioning Triangular resection Flip over technique Durans technique

1. Chordal replacement
Also known as artificial chordal implantation. Technique: This technique involves placing a mattress
suture with a pledget on the papillary muscle to which the redundant or ruptured chord has beenattached. The two ends of the double-armed PTFE are the brought up through the edge of the leaflet that needs to be lowered. The critical part of this technique is determining the degree to which the leaflet is lowered and hence how tightly the stitch is tied down.

Artificial chordae with PTFE is the technique that is perhaps the most popular current technique for AML pathology.
Originally described by Frater and Zussa. Duran has devised a method for more
precise measurement of the correct height for these new chordal structures.


Gillinov, JTCVS 2008
ADVANTAGES
DISADVANTAGES
Anatomical reconstruction
No resection needed
Difficult sizing

2.The edge-to-edge technique
Also known as alfereri technique.
First case performed in 1991
Technically simple and reproducible

Edge to edge repair
Indication: 1. Compromised LV with very less EF.2. Ruptured anterior leaflet.3. Hemodynamic compromised patient
where urgent intervention is required . Where we cannot prolong the pump time. This procedure serves as bailout procedure.

Edge to edge repair
Technique: it is simple , we approximate anterior and posterior leaflets at same level to create a figure of 8 mitral valve orifice.
Disadvantage: there are chances of mitral valve stenosis. To ensure the adequacy of each orifice created by the edge-to-edge technique, we also measure the diameter of each orifice and confirm that it is at least 2 cm in diameter.
If the orifices are less than 2 cm in diameter, the technique is abandoned.


When employed to correct the anterior leaflet prolapse , a suture affixes the free edge of a segment of normal posterior leaflet to free edge of prolapsing segment of anterior leaflet.
The nomal posterior leaflet with its intact chordae serves to anchor the anterior leaflet and restricts its motion.

3.Papillary muscle repositioning
Also known as chordal shortening and is originally described by Carpentier for leaflet prolapse due to elongated chordae .
The elongated chordae are burried in the trench of papillary muscle to effectively reduce the size of chordae and thus reducing the prolapse of leaflet.
Disadvantage: there are high chances of recurrence. The scissoring motion of papillary muscle causing erosion and rupture.

One of the first techniques developed by Carpentier of chordal shortening involves incising the papillary muscle, placing the redundant anterior leaflet chords within the muscle, and then sewing the papillary muscle over the chord, thus entrapping the chordae and shortening it.


4. Flip over technique
In this technique we cut the healthy leaflet segment from posterior leaflet with attached chordae just opposite to the involved anterior leaflet segment and implant this healthy segment on diseased leaflet segment.
The advantage is that it is not necessary to precisely measure the chordal length as natural chordae are of adequate length.


5. Duran’s repair
In this technique we excise a oval portion from mid and basal part of redundant anterior leaflet . All the chordae attached to the ventricular surface of the excised part are separated and are reapplied to the remaining leaflet after the defect in the remaining leaflet is approximated by suturing the two parts.


6. Triangular resection
The technique is similar to the triangular resection of PML.
To be used when only a small part of the leaflet is involved.
Annulus distortion can occur if the involved area is large.


Results
Using these techniques upto 90% of degenerative mitral valves can be repaired.
Hospital mortality is less than 1%. Overall 10 yr freedom from reoperation is
around 93%. Echocardiographic assessment results in
98% 10 yr and 97% 20 yr freedom from reoperation.
Risk of repair failure is increased by anterior leaflet prolapse, chordal shortening and failure to use annuloplasty ring.

Repair in Rheumatic mitral valve disease
Pathology of rheumatic heart disease produces varying degrees of regurgitation, stenosis or mixed lesions.
Acute rheumatic valvulitis produces leaflet prolapse and MR.
Patients with RHD has components of restricted leaflet motion producing stenosis or mixed lesions.
Restricted leaflet motion is caused by thickening of subvalvular apparatus, thickening of leaflets and chordae and commissural fusion. There may be calcification of valve.

Surgical indications
Symptomatic MS is indication of surgery. A new onset atrial fibrillation A patient with pliable leaflets , no
calcification, normal chordae can be considered for repair.
If the valve is severely distorted , leaflets are heavily calcified and there is extreme subvalvar fibrosis and shortening the valve should be replaced.

Repair techniques
In patients with primary stenosis and limited calcification and subvalvar thickening open mitral commissurotomy is a good option.
Commissurotomy should extend 2mm from annulus. More extensive commissurotomy causes MR.
If MR occurs after commissurotomy annuloplasty is done with ring.
Patients with combined lesions are best served by replacement.


Results
10 yr freedom from reoperation in patients with repaired rheumatic mitral valve is around 72%.
Open mitral commissurotomy provides 78-91% 10 yr freedom from reoperation.
Durability of repair in RHD is limited with as many as 50 % developing MR in 5 yrs.

Repair of endocarditis of mitral valve
All the principles of repair are similar except that all the infected material must be removed and placement of any prosthetic material should be avoided.
There are 2 challenges:1. Removing all infection and leaving
sufficient tissue for repair of valve.2. Remodeling the annulus with autologus
material without implanting the prosthetic ring.

Endocarditis
Pathologic findings include:1. Chordal rupture(70%)2. Vegetations (62%)3. Leaflet perforation (53%)4. Abscess (7%)

Surgical indications
1. Heart failure nonresponsive to medical therapy
2. Multiple embolic events3. Uncontrolled sepsis4. Extension of infection to surrounding
structures5. Early operation is indicated for fungal
and staphylococcal infections.

Advantage of repair in endocarditis
Includes:1. Preservation of native , living valve
apparatus which is resistant to infection and concomitant avoidance of prosthetic material.

Repair technique
All the infected material is removed from leaflet . Leaflets are completely detached from the annulus and the annulus is debrided if endocarditis involve the annulus and are covered with pericardial lining before reattaching the leaflets.
Local treatment with iodine solution is recommended.

Repair techniques
In case of ruptured chordae to posterior leaflet quadrangular resection is performed.
Anterior chordal rupture is repaired with standard techniques.
Anterior leaflet perforation are repaired with autologus pericardial patch.
Abscess cavities are debrided and excluded with pericardial patch.
Pericardial annuloplasty is done with both active and chronic endocarditis.

Results
Around 80% of mitral valves with endocarditis are amnable to repair.
Hospital mortality is around 1-7%. Recurrent endocarditis is rare after mitral
valve repair. When compared with replacement ,repair
of infected mitral valve results in greater freedom from recurrent infection and higher early and late survival.

Repair of mitral valve in special situations
1. clefts in posterior leaflet 2. with annular calcifications 3. systolic anterior motion 4. Repair of ischemic MR.

Clefts in posterior leaflet
Clefts when present in posterior leaflet gets accentuated after the repair
Treatment is approximation of clefts using the mattress suture by prolene 4-0.

Repair of PML with subannular calcification
Seen mostly in elderly patients and in patients with long standing disease.
There are two sinarios:a) If annulus is not affected by calcification
and calcification is only subannular: only partial resection of calcification is required.
b) When there is extreme calcification of annular and subannular tissue: separate atria from ventricle and enblock resection of calcium is done followed by reapproximation of atria and ventricle

Systolic anterior motion
SAM occurs due use of rigid annuloplasty rings and when the height of the PML is inadequately reduced for repair.
In both of the situations the redundant PML pushes the AML towards the septum in systole and it results in approximation of AML to septum which is enhanced in mid and late systole due to venturi effect leading to LVOTO.


SAM occurs in about 5-10 % cases of repair.
In patients at risk SAM is potentiated by hypovolemia, vasodiatation and use of inotropes.
More events of SAM are seen after quadrangular resection and is minimised by use of sliding plasty.

Systolic anterior motion
Treatment of SAM: 1. Reresect the PML to reduce the height.2. Upsize the annuloplasty ring.

Repair of ischemic MR
Mechanism of development of MR can be derived from Carpentier’s functional classification.
According to it ischemic MR can result from type I, II, IIIB dysfunctions.
Carpentier’s IIIB dysfunction is most common and significant form of ischemic MR.

Mechanism of regurgitation functional classification
« Surgeons are not basically concerned with lesions. We care more about function. Therefore one may define the aim of a valve reconstuction as restoring normal leaflet function rather than normal valve anatomy »
A. Carpentier, the French Correction 1984

Development of type IIIB dysfunction results due to :
1. Changes in ventricular wall: RWMA, increased sphericity
2. Subvalvar changes includes fibrosis and rupture of papillary muscles, teethering of papillary muscles, apical and posterolateral displcement of papillary muscle leading to restriction of leaflet motion.
3. Annular dilatation and distortion due to alteration in geometry of post infarction LV.

Mechanism of ischemic MR
Mechanism can be divided into 3 catagories.
1. Ruptured papillary muscles2. Infarcted but unruptured papillary
muscle lads to fibrosis and chordal elongation.
3. Functional MR:a. Left ventricular dysfunction and
dilatationb. Annular dilatationc. Both LV dilatation and annular dilatation.

Surgical indication in ischemic MR
1. Severe ischemic MR 2. Mild to moderate ischemic MR:
Controversial
A patient with ischemic MR of grade 2+ onwards require mitral valve repair concomitant with revascularization.

Surgical approach
1. Median sternotomy is surgical approach of choice.
2. Right lateral thoracotomy may be used in patients with prior CABG and functioning grafts. Here we perform right anterolateral thoracotomy through 4th ICS.
3. Right thoracotomy is C/I inpatients with previous right thoracic surgeries, COPD, severe AR.

Repair
Mitral valve repair is standard treatment for ischemic mitral regurgitation.
Here the anterior paracommissural scallop (P1 ) constitutes the referance point.
Mitral annulus is then examined to access the dilatation.
It is the P2 & P3 segments of posterior leaflet which are most commonly involved as they are attached to posterior papillary muscle which has single blood supply.

Remodeling annuloplasty using undersized ring is the technique of choice in type IIIB dysfunction.
Most commonly braided 2-0 sutures are used to implant the ring.
The anterior commissure is the most difficult area to expose for suture placement and is generally approached last.
Downsizing the physio ring by 1 or 2 sizes or to use a true sized Mc Carthy-Carpentier IMR Etlogix ring is used for annuloplasty.

This IMR ring asymmetrically downsize the annulus .this ring downsizes the D3 dimension by 2 sizes and D2 dimension by 1 size. This makes it possible to select true size ring. Further more this ring contains titanium core which allows complete fixation of septolateral dimension during entire cardiac cycle.


Repair
Papillary muscle rupture is managed by mitral valve replacement with bioprosthesis.
Papillary muscle infarction without rupture is managed with repair techniques described with degenerative mitral valve disease and prolapse.
If the portion of posterior leaflet is affected quadrangular resection is indicated.
If there is anterior leaflet prolapse , chordal transfer and chordal replacement suffice.

Results
Hospital mortality after valve repair in ischemic MR is around 3-6%.
5 yr survival is around 58%. Patients with ruptured papillary muscle have
best long term survival , likely due to better preservation of LV function.
Patients with ischemic MR have more damaged LV and correspondingly a reduced longevity.
Because the long term survival is limited the durability of mitral valve repair in patients with ischemic MR is difficult to establish.

Types of ring
Rings can be: 1. Rigid / flexible/ semiflexible2. Complete/ incomplete/ asymmetric ring
Complete ring Incomplete ring
1. CE physio ring(titanium + velor decron)
2. Medtronic complete flexible ring(titanium core with silicon felt, 3 marks for referance.)
3. St jude semiflexible ring (AP angulation)
4. Carbomedics complete flexible ring
1.CE ring made of titanium core.2. Cogrove C shaped ring.3. Homemade ring with stainless steel wire.

Types of ring
Choice of ring:1. Degenerative diseases: rigid or flexible ring.2. RHD/ endocarditis/ congenital mitral disease:
rigid ring.3. Ischemic MR : rigid ring or asymmetric
ring(IMR ring by CE)4. Functional MR: geoform ring 5. If underlying myocardium is severely
diseased the choice is rigid ring and if only valve tissue is involved then incomplete ring is choice.

Rigid rings: there occur no change in diameter of ring in different parts of cardiac cycle. They may interfere with LV filling and functioning, LVOTO.
Incomplete rings: they are used when only annulus is dilated. No support to anterior part of valve .
Semiflexible rings: here the anterior portion is rigid, so no change occurs in transverse diameter. Posterior part is flexible so allows change in transverse diameter of valve.


Advantage of rings
1. Retain the shape and size of annulus.2. Keeps tension off the suture lines3. Increases leaflet coaptation4. Prevents recurrent dilatation of annulus.

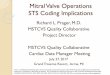
Hospital mortality for isolated first time elective MV repair is 2.5% (males) to 3.9% (females)
Operative risk is higher in elderly pts, associated CABG, NYHA III-IV, low EF and reoperation
Hospital mortality and repair rate STS National Adult Cardiac Database
Savage EB, et al Ann Thorac Surg 2003;75:820–5
1991
1993
1995
1997
1999
0%
20%
40%
60%
80%
100%
Replacement Repair

Older age is associated to Higher mortality
Higher morbidity
Longer LOS
2/3 of pts older than 70 years are denied surgery (Euroheart Survey)
Age and comorbidities
Mehta et al. Ann Thorac Surg 2002;74:1459-67

Very Long Term Survival for >20 years in 162 pts with Organic MR
Braunberger, et al Circulation. 2001;104[suppl I]:I-8-I-11.

Years
Su
rviv
al (
%)
100
80
20
00 2 4 6 8 10
60
40
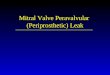
72%
EF 60%EF 50-60%
53%
P = 0.0001
EF < 50% 32%
Ejection Fraction
Enriquez-Sarano M et al. Circulation 1994; 90: 830 - 37
Preoperative LV Function Predicts Long Term Postoperative Survival

• If mitral repair is performed before the onset of severe symptoms (congestive heart failure, arrhythmias), life expectancy is restored
Preoperative Symptoms and Long Term Survival
David T et al, J Thorac Cardiovasc Surg 2003;125:1143-52

Durability: Freedom from Reoperation1072 patients with degenerative mitral regurgitation
operated upon at CCF between 1985 and 1997
Gillinov et alJ Thorac Cardiovasc Surg 1998;116:734-43

The Bad News….
Flameng W, et al. Circulation. 2003;107:1609-1613

Thank you