Embed Size (px)
Citation preview

Molecular Biology & Targeted Therapy in
Lung Cancer Dr. Rikin Hasnani

Introduction & History• Lung cancer is the most common cause of cancer-related death in
men and women worldwide, responsible for over 1 million deaths annually.• Although 1-year survival has improved over the past few decades,
overall 5-year survival has remained relatively unchanged at 12% to 16% over the past 30 years.• A key discovery in the past decade has been that some lung cancers
harbor specific mutations that are essential for malignant growth, which lead to gain of function of oncogenes or loss of function of tumor suppressor genes .

• Historically, nonsmall cell lung cancer (NSCLC) has been classified histologically as squamous cell carcinoma, adenocarcinoma, and large cell carcinoma, and various chemotherapeutic regimens have been used to treat different histological subtypes. • It is now realized that NSCLC is a collection of diseases that are identifiable by
specific molecular abnormalities, personalized therapy became a goal for patients with NSCLC. • Between 1980 and 2000, NSCLC driver lesions that were investigated included
mutations in the Kirsten rat sarcoma viral oncogene homolog (KRAS) and protein 53 (p53) genes, loss of specific chromosomal loci, loss of heterozygosity, and DNA methylation of TSGs. • In 2004, driver mutations in the epidermal growth factor receptor (EGFR) gene, a
membrane-bound receptor tyrosine kinase (RTK) that regulates cell growth, were discovered in NSCLC, especially in adenocarcinomas• In 2007, the existence of the echinoderm microtubule-associated protein-like 4
(EML4) translocation to the anaplastic lymphoma kinase (ALK) gene resulting in an EML4-ALK fusion gene was discovered in NSCLC.

REGULATION OF CELL GROWTH AND SURVIVAL• MEMBRANE-BOUND RECEPTOR TYROSINE KINASES• INTRACELLULAR KINASES AND TARGETS: RAS/RAF/MEK/ERK PATHWAY• CELL CYCLE REGULATION

MEMBRANE-BOUND RECEPTOR TYROSINE KINASES• Membrane-bound RTKs share a common general structure composed of an
extracellular region that contains a ligand-binding domain, an extracellular juxtamembrane region, a hydrophobic transmembrane domain, a cytoplasmic TK domain, and a cytoplasmic tail with tyrosine residues that serve as sites for receptor phosphorylation.• Driver lesions in the membrane-bound RTKs result in deregulated signaling
or in a effector that cannot be shut off. • RTK activation in cancer may occur via overexpression of wild-type receptor
due to gene amplification (resulting in excess signaling), excess ligand production, ligand overstimulation, activating mutations, translocations resulting in activated fusion proteins, or reduced receptor downregulation.


• The prototypical RTKs involved in lung cancer are members of the ErbB family. • The ErbB family of RTKs includes ErbB1 (EGFR; HER1), ErbB2
(HER2/Neu), ErbB3 (HER3), and ErbB4 (HER4). • In the lung, these RTKs are expressed by the pulmonary epithelium
(e.g., alveolar type II cells and bronchial cells) and fibroblasts.• Members of the epidermal growth factor (EGF) family of peptide
hormones serve as ligands for ErbB RTKs, and include EGF, transforming growth factor-α, betacellulin, and epiregulin for ErbB1; and the neuregulins for ErbB3 and ErbB4.

INTRACELLULAR KINASES AND TARGETS: RAS/RAF/MEK/ERK PATHWAY• Downstream of membrane-
bound RTKs is the RAS/RAF/MEK/ERK pathway, which is a pivotal intracellular signaling pathway that transmits RTK signals to the nucleus via a cascade of specific protein phosphorylation.

RAS
• The RAS family of oncogenes includes neuroblastoma RAS viral oncogene homolog (NRAS), KRAS, and Harvey rat sarcoma viral oncogene homolog (HRAS).
• KRAS is the gene that is most commonly involved in lung cancer
• Approximately 20% to 30% of NSCLC harbor activating point mutations in RAS genes.
• Mutations occur most frequently in the KRAS gene (90%), specifically in codons 12, 13, and 61

• RAF• RAF is a family of serine–threonine kinases that includes A-RAF, B-RAF,
and C-RAF.• Although RAF is activated by RAS, activation can also occur
independently of RAS through other activators such as Src, c-Jun NH2-terminal kinase, interferon-β, protein kinase C-α (PKC-α), or through dimerization between RAF isoforms. • Activating mutations of the B-RAF gene have been reported in up to
3% of NSCLC tumors, most of which are adenocarcinoma

CELL CYCLE REGULATION• In nontransformed pulmonary epithelial
cells, cell division is a tightly regulated process with multiple checkpoints that assess extracellular growth signals, cell size, and DNA integrity. • Cyclins and their associated cyclin-
dependent kinases (CDKs) are the central machinery that control cell cycle progression. • Alterations in these proteins may lead to
a bypass of the checkpoints that assess a cell’s readiness to divide.


• Rb• The product of the retinoblastoma susceptibility gene, Rb, plays a central role in
the G1-S transition, and Rb is considered a tumor suppressor gene. • Therefore, loss of normal function of this gene removes its suppressor effect
leading to cellular transformation.• p53• p53 is a transcription factor that can activate the transcription of numerous
genes, including the CDK inhibitor p21. • Mutation of the p53 gene results in a protein that fails to bind DNA effectively.
Therefore, expression of the CDK inhibitor p21 gene is decreased, and p21 protein production is decreased. • p21 protein is not available to stop the entry of the cell into S phase, again
resulting in unregulated cell cycle progression. • Mutations of the p53 gene occur in nearly 50% of NSCLC and abnormalities of p53
protein may play an important role in the tumorigenesis of lung epithelial cells.


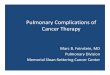
Targeted Therapy• EGFR • EGFR gene mutations are much more commonly found in female
never smokers of East Asian origin with adenocarcinoma histology. • Whereas the incidence of EGFR mutations in Asians is 25% to 35%,
the incidence in North American and Western European patients is approximately 15%. • However, the strongest predictor of EGFR mutation status appears to
be absent or low smoking history.

EGFR Mutations

• Erlotinib, Geftinib, Crizotinib are TK inhibitors.• A large number of retrospective series have demonstrated that the
response rate of EGFR mutation-positive patients to EGFR TKIs exceeds 60%.• Another strategy to block EGFR kinase function in patients with NSCLC
focuses on the use of monoclonal antibodies directed against EGFR.• Cetuximab, matuzumab, necitumumab and panitumumab are
monoclonal Ab against EGFR.

Erlotinib • Dose 150mg per day, orally• It is metabolized by Liver.• FDA approved erlotinib in 2013 in pt with locally advanced and metastatic
NSCLC who has failed atleast one prior chemotherapy regimen.• Side effects : • Rash - The Journal of Clinical Oncology reported in 2004 that "cutaneous
[skin] rash seems to be a surrogate marker of clinical benefit, but this finding should be confirmed in ongoing and future studies.• Interstitial pneumonitis, diarrhea, ingrown hairs are common • GI perforation, SJ syndrome, BOOP, pulmonary fibrosis are rare side effects

Gefitinib • On July 13, 2015, the FDA approved gefitinib as a first-line treatment
for metastatic NSCLC , which are positive for EGFR gene mutation.• Dose 250mg per day orally , till progression of disease of
unacceptable side effects• Side effects• Rash, acne, diarrhea, stomatitis, paronychia, asymptomatic elevation
of liver enzymes• Rare side effects – interstitial lung disease, corneal erosions

TKI Resistance• Virtually all patients who initially respond to EGFR TKI therapy will develop resistance
and suffer a clinical relapse. • Approximately 50% of the cases of acquired TKI resistance are attributed to a
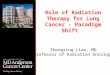
secondary EGFR gene mutation, the threonine to methionine point mutation at amino acid 790 (T790M) in exon 20.• Afatinib is the Drug Of Choice.• The LUX-Lung 3 trial investigated the efficacy and safety of afatinib compared with
pemetrexed/cisplatin in patients with EGFR mutation-positive stage IIIB/IV lung adenocarcinoma. • Treatment with afatinib led to a significantly prolonged PFS versus
pemetrexed/cisplatin (median 11.1 vs. 6.9 months).• Sequential blockade is another approach to treat TKI Resisitance.

Lux Lung 3 Trial

• EML4-ALK• In 2007, Soda et al. reported a new molecular abnormality involving the
fusion of ALK with EML4 in lung adenocarcinoma. • The fusion protein results from an inversion in the short arm of
chromosome 2 that fuses the N-terminal domain of EML4 to the intracellular kinase domain of ALK, leading to constitutive activation of the ALK kinase. • In the original report by Soda and colleagues, 6.7% of unselected NSCLC
patients had the EML4-ALK fusion protein.• Characteristic of pt.• Mutually excludes RAS, EGFR• Patients with EML4-ALK-positive stage III or IV NSCLC treated with
crizotinib, competitive inhibitor targeted to the ATP-binding pocket of the ALK TK , demonstrated an overall response rate of 60.8%.

• KRAS• 20 – 40 % of pt with NSCLC has RAS mutation.• 90% are KRAS• More common in smokers, Adenocarcinoma • Associated with worse prognosis.• Current therapeutic approaches targeting RAS fall into three major
categories: • inhibition of RAS protein synthesis, • alteration of RAS membrane localization - Salirasib • inhibition of effector molecules downstream of mutant RAS –
Sorafenib,AZD6244

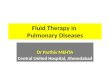
TKI in Squamous Cell Carcinoma
Comprehensive genomic characterization of squamous cell lung cancersThe Cancer Genome Atlas Research Network*



Erlotinib, Geftinib ,Afatinib Salirasib
AZD6244
SORAFENIB
EVEROLIMUS
CETUXIMAB, MATUZUMAB

Thank You