Embed Size (px)
Citation preview
Each patient ought to feel somewhat the better after the physician's visit, irrespective of the nature of the illness. ~Warfield Theobald Longcope

Multiple Sclerosis: Diagnosis and Treatment
Monique Canonico DO
Assistant Clinical ProfessorJohn A. Burns School of Medicine
April 2015

Objectives
• 1. Learn the disease characteristics and demographics.
• 2. Discuss the pathophysiology.
• 3. Learn the clinical presentation.
• 4. Become familiar with MS therapeutics algorithms

It's not what you look at that matters, it's what you see.
-Henry David Thoreau
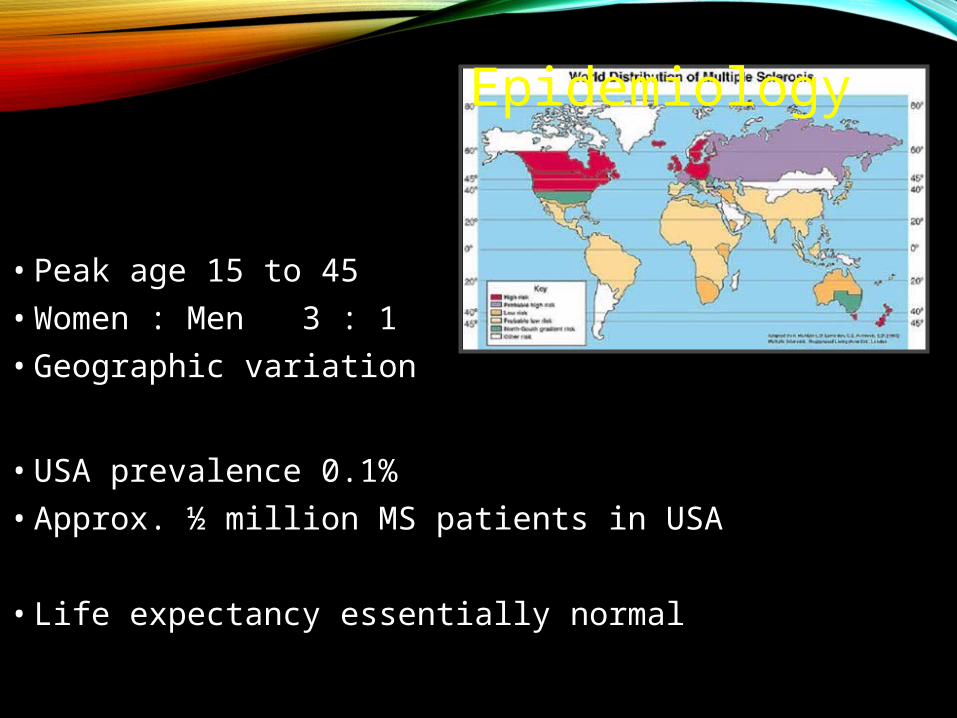
Epidemiology
• Peak age 15 to 45
• Women : Men 3 : 1
• Geographic variation
• USA prevalence 0.1%
• Approx. ½ million MS patients in USA
• Life expectancy essentially normal
-avg person US has 1/750 risk of MS (.1%)-risk in child or sibling of pt~ 4%-Monozygotic twins: 30%-over 159 genetic variations related to MS have been identified
GENETICS
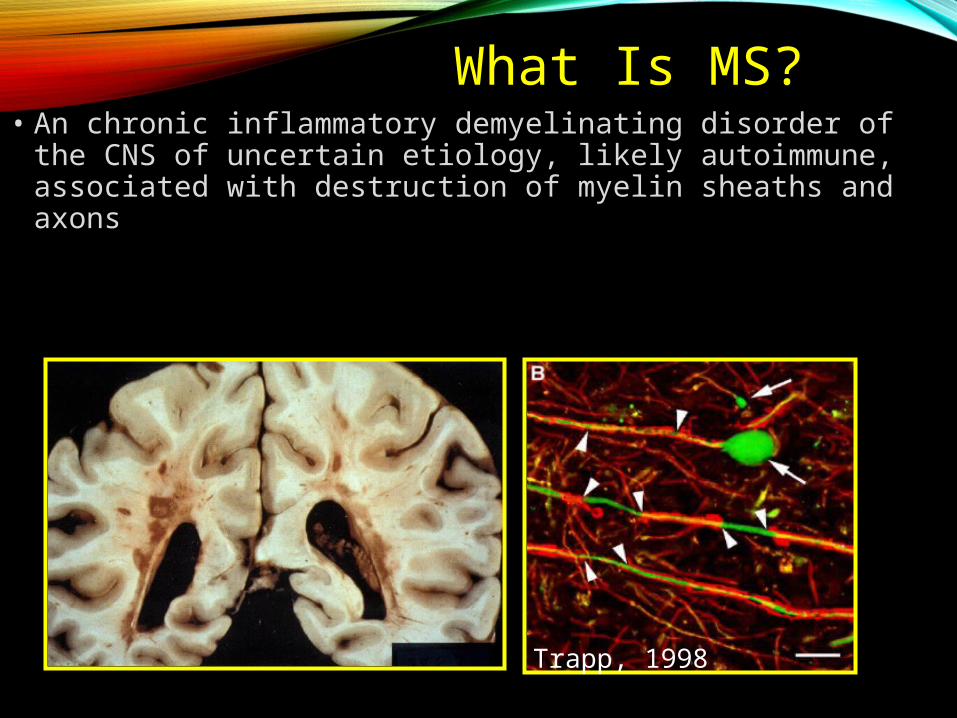
What Is MS?• An chronic inflammatory demyelinating disorder of the
CNS of uncertain etiology, likely autoimmune, associated with destruction of myelin sheaths and axons
Trapp, 1998

-Described in late 1800s by Dr. Charcot-Perivascular inflammation and demyelination-Plaques occur anywhere in the CNS
-Most frequent: optic nerve, brainstem, cerebellum, spinal cord-Above lesions correlate with clinical sxs
-Axon sparing within the plaques
Pathological Hallmarks
-Disruption of blood-brain barrier-Unknown if demyelination precedes or follows inflammation-Acute inflammatory response of lymphocytes, plasma cells, macrophages
-Macrophages contain myelin breakdown product-Lymphocytes: antibody- and cell-mediated immunity (direct), secretion of lymphokines or cytokines (indirect)
Plaque evolution

Conduction block at site of lesionSlower conduction time along affected nerveIncreased subjective feeling of fatigue secondary to compensation for neurologic deficits
Results of Demyelination
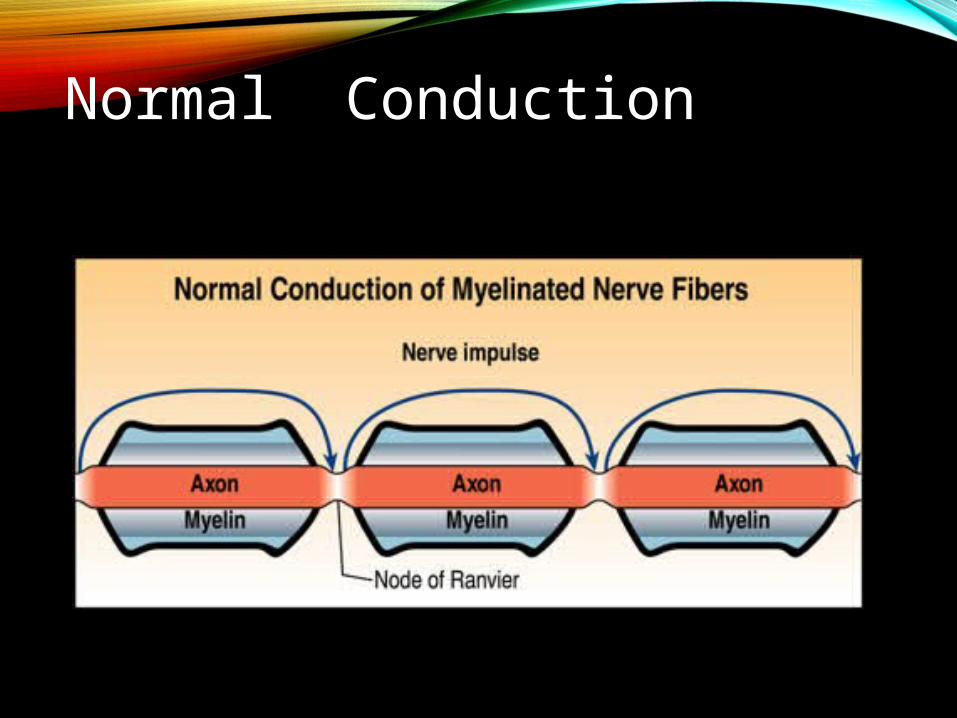
Normal Conduction
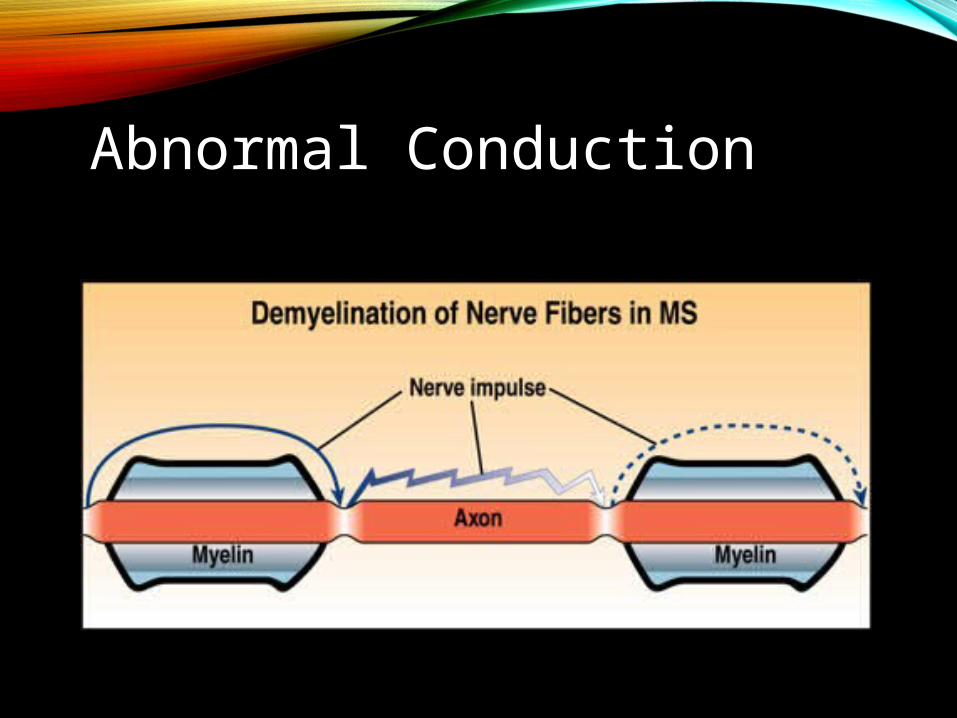
Abnormal Conduction
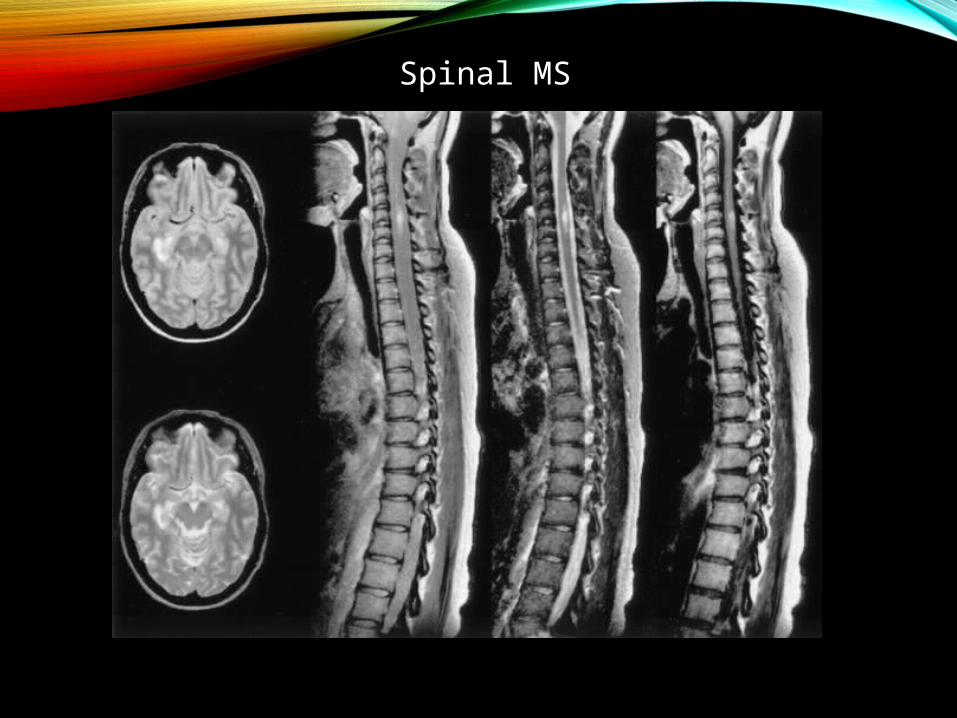
Spinal MS
CASE 2
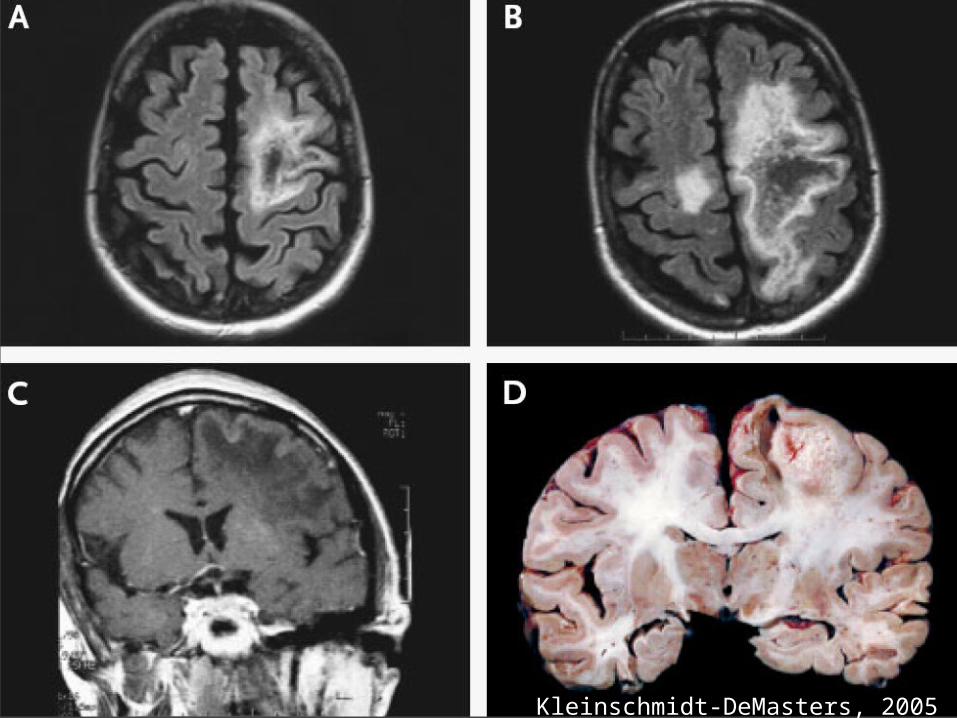
Kleinschmidt-DeMasters, 2005

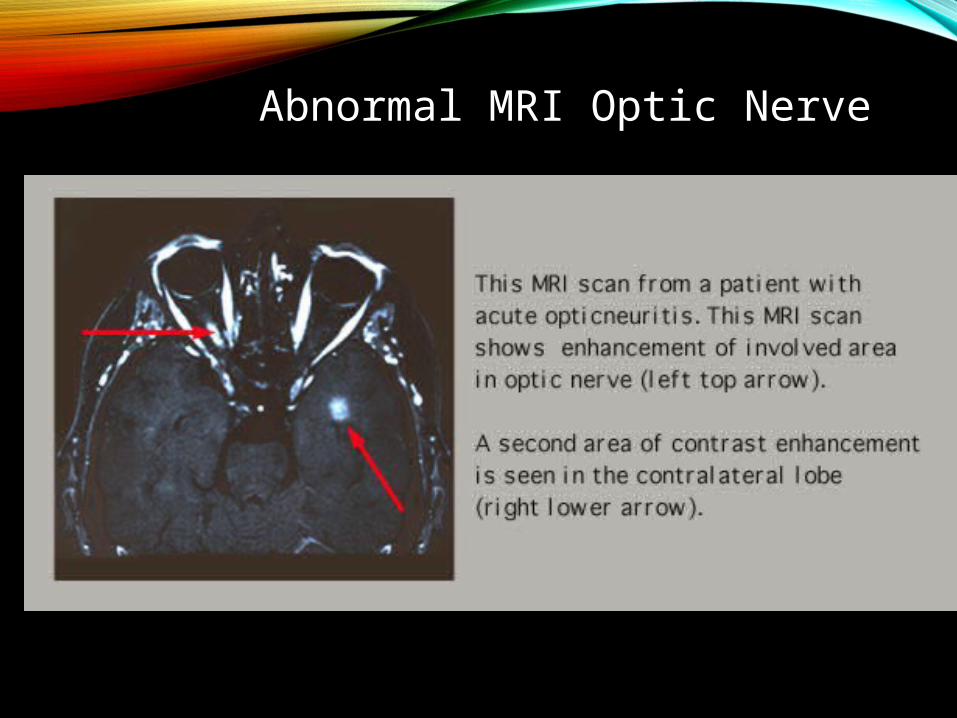
Abnormal MRI Optic Nerve
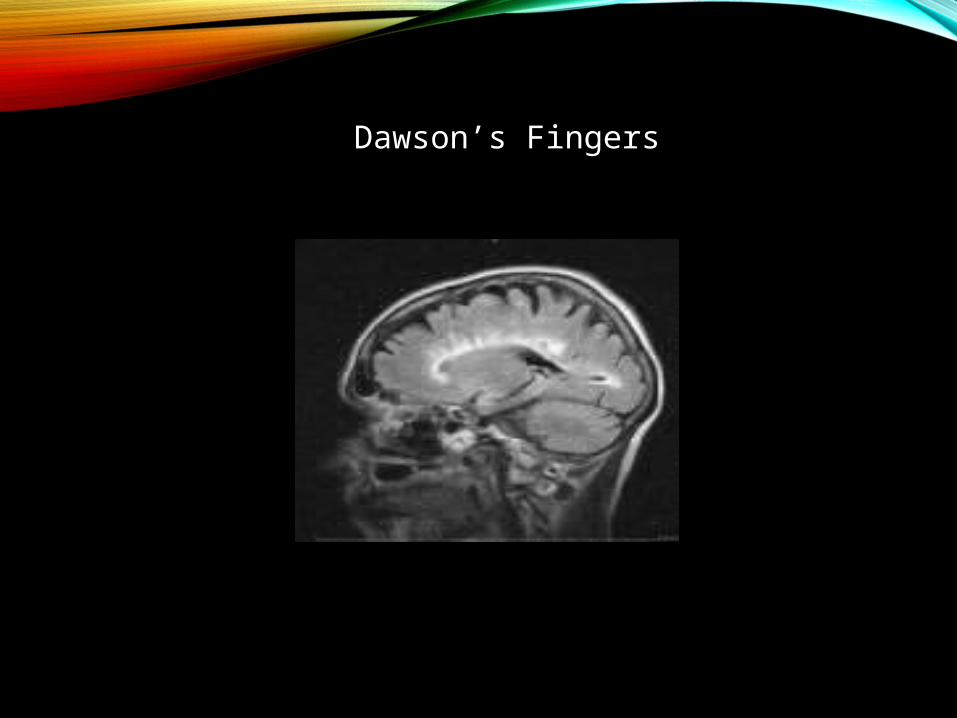
Dawson’s Fingers
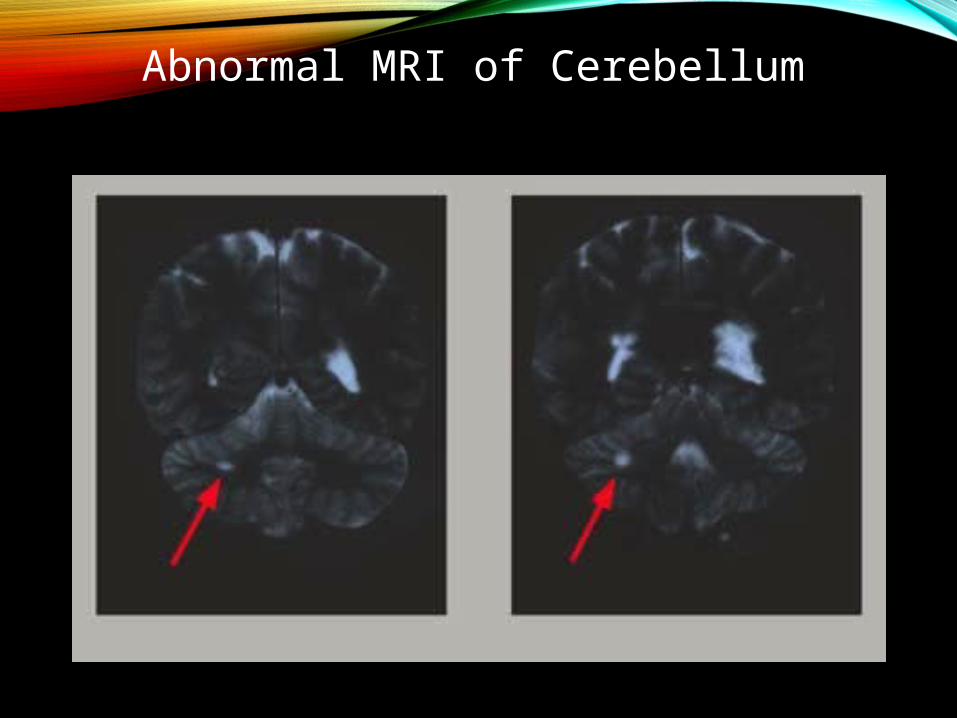
Abnormal MRI of Cerebellum
Symptoms are the body's mother tongue; signs are in a foreign language. ~John Brown
-Episodes of neurologic dysfunction followed by stabilization/remission-Relapses can be rapid or gradual onset-May persist or resolve over weeks to months-Relapsing-remitting pattern is most common in MS
Clinical Presentation

MS Signs and Symptoms
• Fatigue
• Heat intolerance
• Visual symptoms
• Numbness, tingling, loss of sensation
• Weakness
• Imbalance
• Urinary and sexual dysfunction
• Cognitive deficits
-Ascending numbness starting in feet-Bilateral hand numbness-Hemiparesthesia/dysesthesia-Generalized heat intolerance-Dorsal column signs
-Loss of vibration/proprioception-L’hermitte’s sign
Sensory Symptoms

-Unilateral or bilateral partial/complete internuclear ophthalmoplegia-CN VI paresis-Optic neuritis
-Central scotoma, headache, change in color perception, retro orbital pain with eye movement)
Visual Disturbances

-Weakness (mono-, para-, hemi- or quadriparesis)-Increased spasticity-Pathologic signs (Babinski, Chaddock, Hoffman)-Dysarthria
Motor Disturbance
-Urinary incontinence, incomplete emptying -Set up for UTI’s
-Cognitive dysfunction-Fatigue-Sexual dysfunction
Other Symptoms
Pain
• Trigeminal neuralgia in 2 percent
• L'hirmitte's sign in 9 percent
• Dysesthetic pain in 18 percent
• Back pain in 16 percent
• Visceral pain in 3 percent
• Painful tonic spasms in 11 percent
Anxiety and Depression
• Anxiety most prevalent
• 2/3 may have depression
• Euphoria
• Dysphoria
• Depression may severely impact the already present cognitive dysfunction that is associated with MS
Signs
• L’hirmitte’s Sign
• Uhtoff’s phenomenon
Neuro Exam
• Afferent pupillary defect
• Internuclear ophthalmoplegia
• Weakness
• Dysmetria
• Dysdiadochokinesia
• Increased reflexes
• Upgoing toe
Differential Diagnosis• Metabolic: SCD (B12 def),
Adrenomyeloneuropathy
• Connective Tissue Diseases: Sjogren’s, SLE
• Infectious: HIV, HTLV1, Lyme disease, Syphilis
• Structural: Chiari malformation, spinal cord compression
• Genetic: ataxias, paraplegias, mitochondrial
• Neoplastic: CNS lymphoma, paraneoplastic
• “MS variants”: ON, TM, ADEM, NMO
• Other: Neurosarcoidosis, CNS vasculitis
• Psychiatric

MS DIAGNOSIS “DISSEMINATION IN SPACE AND
TIME”

DIAGNOSTIC WORK UP• History & Physical Exam• Brain and Spinal Cord MRI• Labs: rule out mimics of MS
• Connective tissue diseases, infections, metabolic disorders
• Cerebrospinal Fluid (when clinical and MRI evidence inconclusive)
• Evoked Potentials: • Identify damage to visual, auditory, & touch perception
systems• Less sensitive than MRI or cerebrospinal fluid

labs
• ANA
• ACE
• Lyme
• Anticardiolipin ab
• ESR
• HIV
• Syphilis IgG
• SSA, SSB
• Neuromyelitis optica antibody(AQP4 ab)
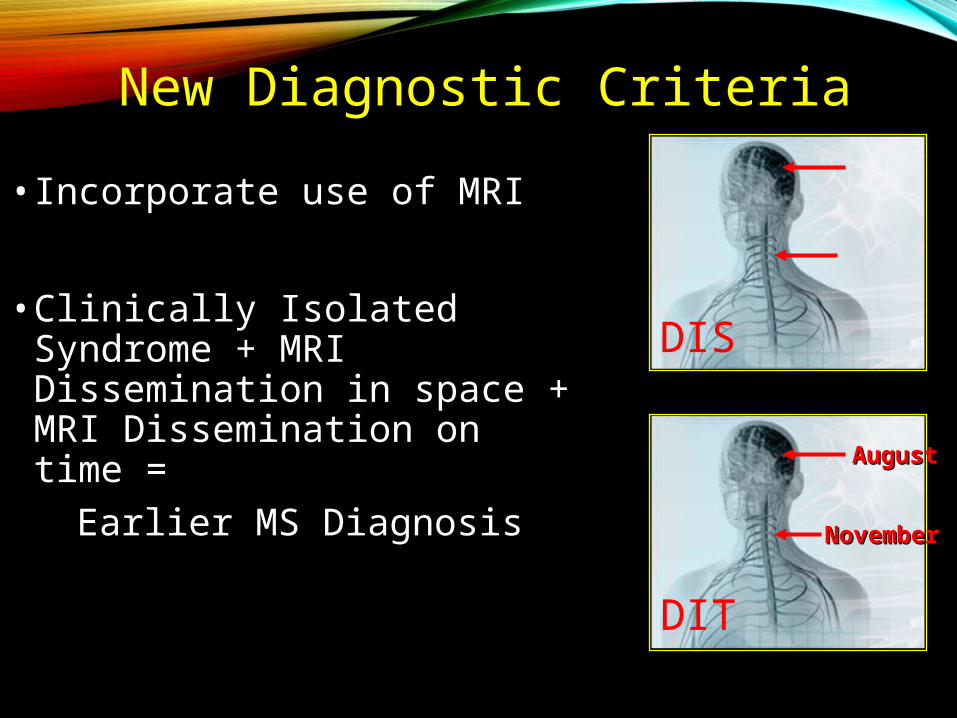
New Diagnostic Criteria
• Incorporate use of MRI
• Clinically Isolated Syndrome + MRI Dissemination in space + MRI Dissemination on time =
Earlier MS Diagnosis AugustAugust
NovemberNovember
DIS
DIT
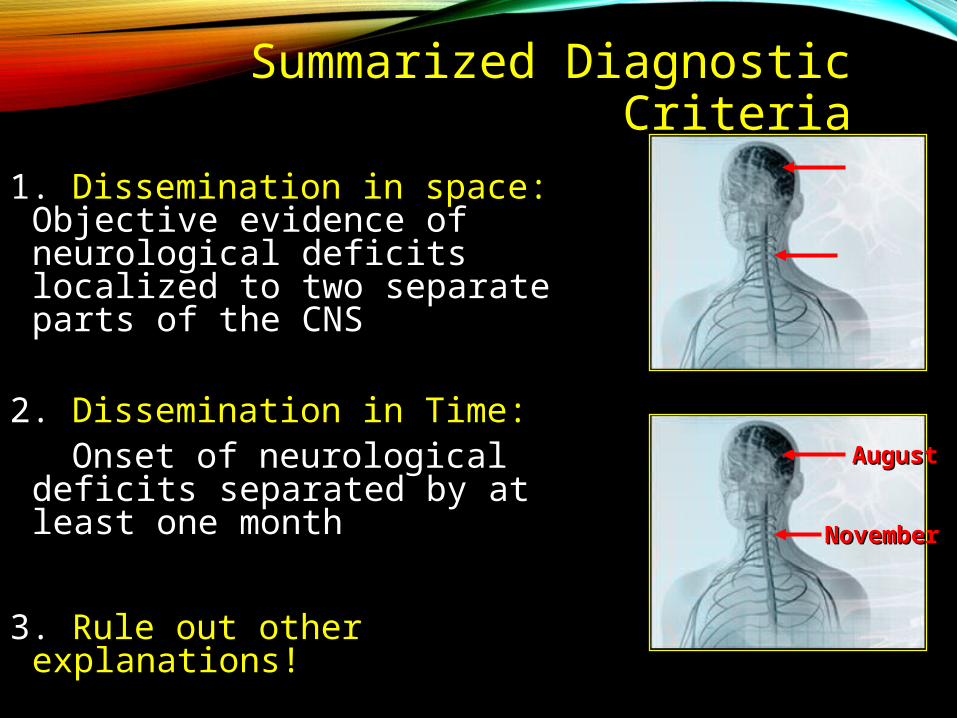
Summarized Diagnostic Criteria
1. Dissemination in space: Objective evidence of neurological deficits localized to two separate parts of the CNS
2. Dissemination in Time: Onset of neurological
deficits separated by at least one month
3. Rule out other explanations!
AugustAugust
NovemberNovember
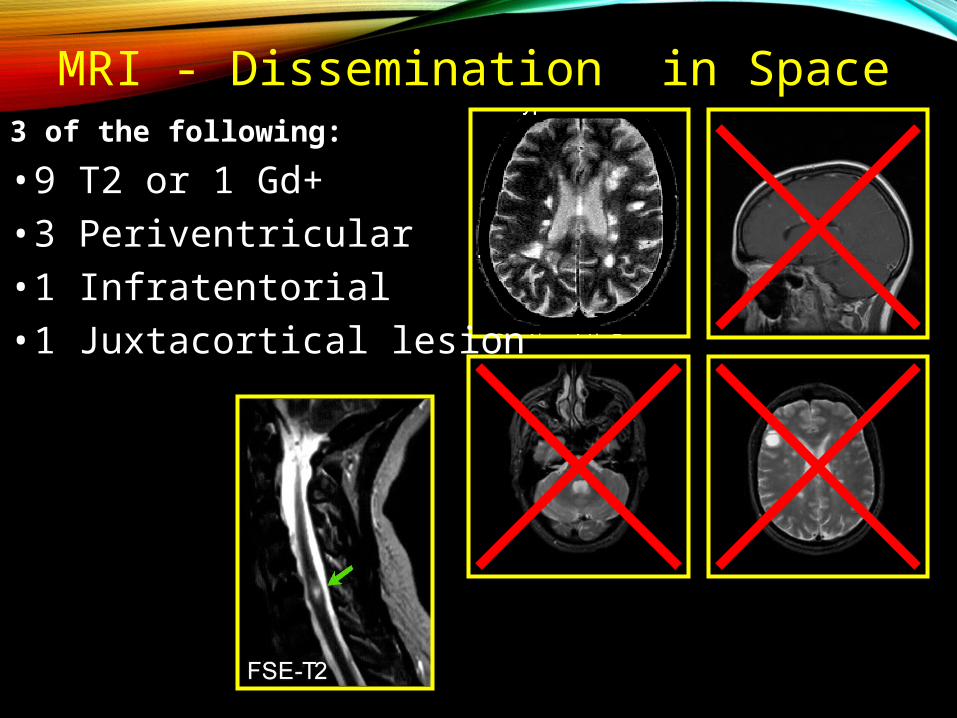
3 of the following:
• 9 T2 or 1 Gd+ • 3 Periventricular • 1 Infratentorial• 1 Juxtacortical lesion
MRI - Dissemination in Space

T2
MRI - Dissemination in Time
CIS> 1 month > 1 month
Gd
> 3 months
Polman, 2005
Gd
T2

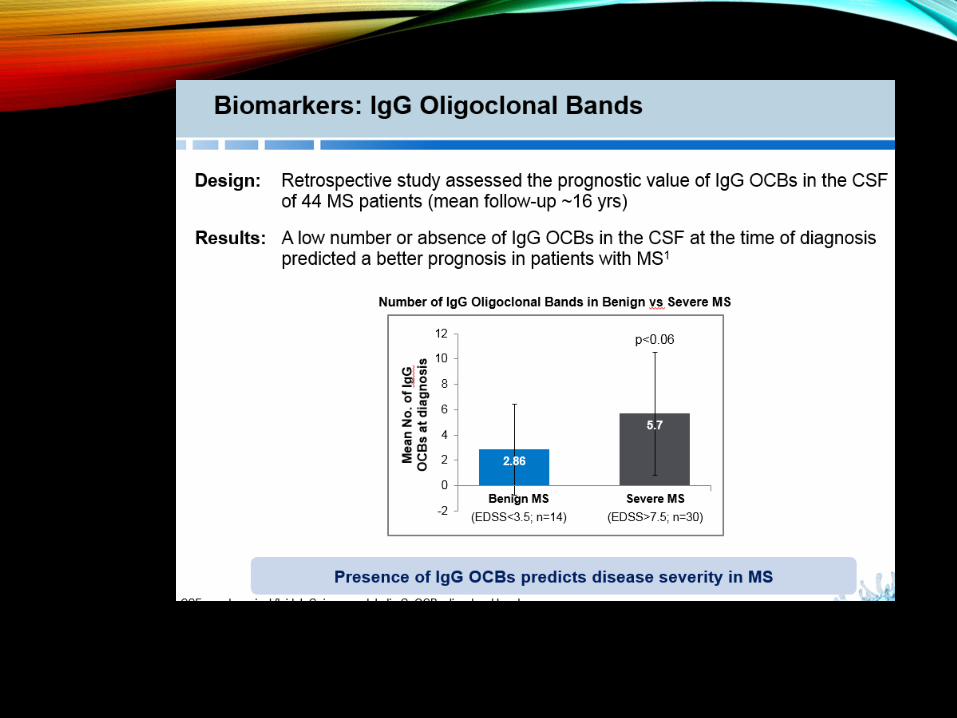
CSF Analysis
• Elevated IgG Index >0.7 • Increased CNS IgG synthesis,
with normal serum IgG consistent with MS
• Oligoclonal Bands • Presence of 2 distinct
bands in CSF is consistent with MS
• Most helpful for suggesting an alternative Dx-high protein, marked pleocytosis, PMNs
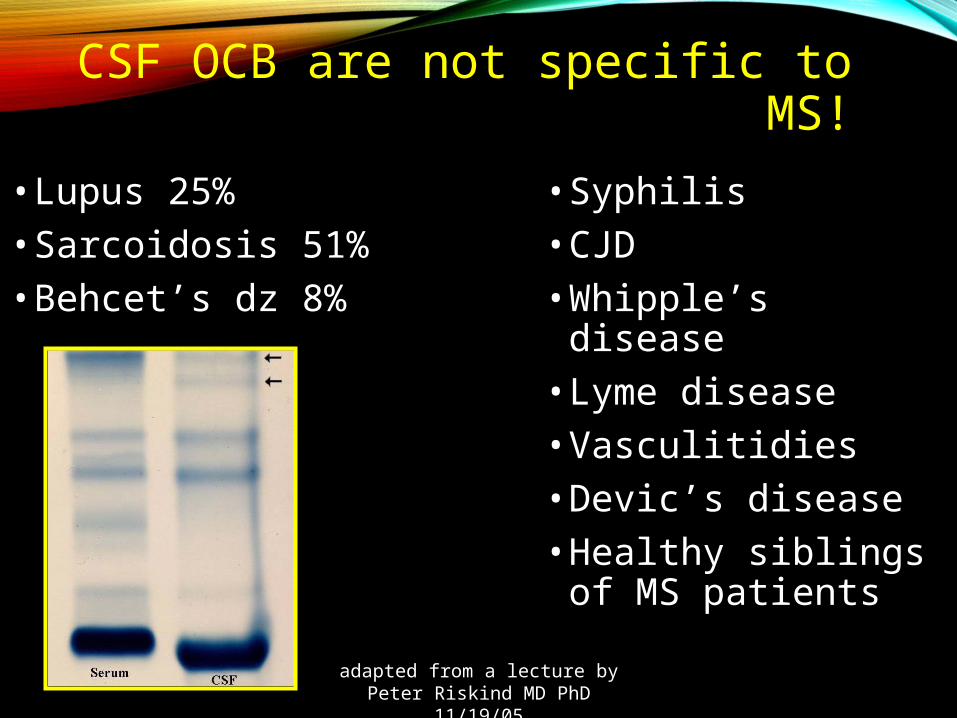
CSF OCB are not specific to MS!
• Lupus 25%• Sarcoidosis 51%• Behcet’s dz 8%
• Syphilis• CJD• Whipple’s disease• Lyme disease• Vasculitidies• Devic’s disease• Healthy siblings of
MS patients
adapted from a lecture by Peter Riskind MD PhD 11/19/05

TREATMENTACUTE
Steroids
IVIG
Plasma exchange
DISEASE MODIFYING
11 treatments
CAM
Recent evidence based guide lines published by the American Academy of Neurology
HOW TO IDENTIFY A RELAPSE?
• CRITICAL, compare with previous examinations (history and examination), when ever possible
• Relapses can be precipitated by infections and fever• Check U/A for occult UTI
TREATMENT OF RELAPSE
• INPATIENT• Severe deficits• Risk of fall or other injury • Poor social support
• OUTPATIENT• All other relapses

TREATMENT OF RELAPSE:
• IV methylprednisolone one gram daily for 5 days
• Severe cases: up to 2 grams daily x 7d
• Oral Prednisone for special circumstances• poor veins, insurance issues, travel, etc…

TREATMENT OF RELAPSE: PLASMAPHERESIS
• Severe relapses not responding to steroids
• 5 to 7 courses done on alternate days for 2 weeks
• One course takes place over 3 to 4 hours
Nonpharmacologic Management
• Exercise (avoid overheating)
• Physical / occupational therapy
• Nutrition (avoid extremes of weight)
• Avoid excess heat exposure or elevated core temperature
• Prompt tx of fever with antipyretics• Cool environment / cool bath

PHARMACOLOGICMGT
• MANY OPTIONS NOW

FDA-Approved Disease-Modifying AgentsAubagio (teriflunomide) Avonex (interferon beta-1a) Betaseron (interferon beta-1b) Copaxone (glatiramer acetate) Extavia (interferon beta-1b) Gilenya (fingolimod) Novantrone (mitoxantrone) Rebif (interferon beta-1a) Tecfidera (dimethyl fumarate) Tysabri (natalizumab)Lemtrada (alemtuzumab)


The Big GunsTysabri (natulizumab)Gilenya (fingolimod)
Lemtrada (alemtuzumab)

Generic Copaxone is Here
• Data presented at the ACTRIMS/ECTRIMS mtg Sept 14
Randomized study comparing Copaxone with a generic version of glatimer acetate in 735 pts and vs placebo
-The GATE study found NO SUCH DIFFERENCES
-The numbers of enhancing MRI lesions were the same over 7-9 mos (the primary endpoint)
-Both groups showed superiority over placebo
-Adverse effects similar
Stem Cell Therapy
• Mesenchymal stem cell therapy for MS passed safety and feasibility in a Phase I study at the Mellen Center for MS
• This paves the way for larger studies
• The strategy is REPAIR of damaged tissues
• 24 patients (14 secondary progressive and 10 with relapsing remitting
• Tx was with autologous adult mesenchymal stem cells from the bone marrow

Neuropsychiatric Symptoms : MS
• Prozac/Paxil for depression
• Venlafaxine or mirtazapine for depression
• Can add methylphenidate if needed
• ECT is OK in MS (but carries risk of relapse)
• Anxiety is the most common MS symptomCognitive Behavioral Therapy is helpful
• Bipolar disease is twice as common in MS tx with valproate or Li or antipsychotics

AGENTAGENT MECHANISMMECHANISM ROUTEROUTE PHASEPHASE
RituximabRituximab Anti CD20Anti CD20 IV (2 x year)IV (2 x year) Phase IIPhase II
CampathCampath Anti CD52Anti CD52 IV (1 x year)IV (1 x year) Phase IIPhase II
DaclizumabDaclizumab Anti CD25Anti CD25 IV or SC (q mo)IV or SC (q mo) Phase IIPhase II
Anti IL-12Anti IL-12 Anti IL-12Anti IL-12 SC (qw or qow)SC (qw or qow) Phase IIPhase II
Statins Statins immunomodulatorimmunomodulator oraloral Phase IIPhase II
TeriflunomideTeriflunomide immunomodulatorimmunomodulator oraloral Phase IIIPhase III
Anti VLA-4Anti VLA-4 SAM inhibitorSAM inhibitor oraloral Phase IIIPhase III
FTY 720FTY 720 immunomodulatorimmunomodulator oraloral Phase IIIPhase III
Oral CladribineOral Cladribine immunosuppressanimmunosuppressantt
oraloral Phase IIIPhase III
MinocyclineMinocycline immunomodulatorimmunomodulator oraloral Phase IIPhase II
EstriolEstriol immunomodulatorimmunomodulator oraloral Phase IIPhase II
MBP 8292MBP 8292 immunomodulatorimmunomodulator IV (q month)IV (q month) Phase IIIPhase III
Therapeutic Agents Under InvestigationTherapeutic Agents Under Investigation
We cannot become what we need to be by remaining what we are.
-Max De Pree

CAM
• AAN guideline Feb 2014
• Knowledgeable advice should be given
• Counseling is part of the evaluation and mgt
• ( part of “Cognitive care” )• -CPT code 99201 (new)• -CPT code 99241 (est)

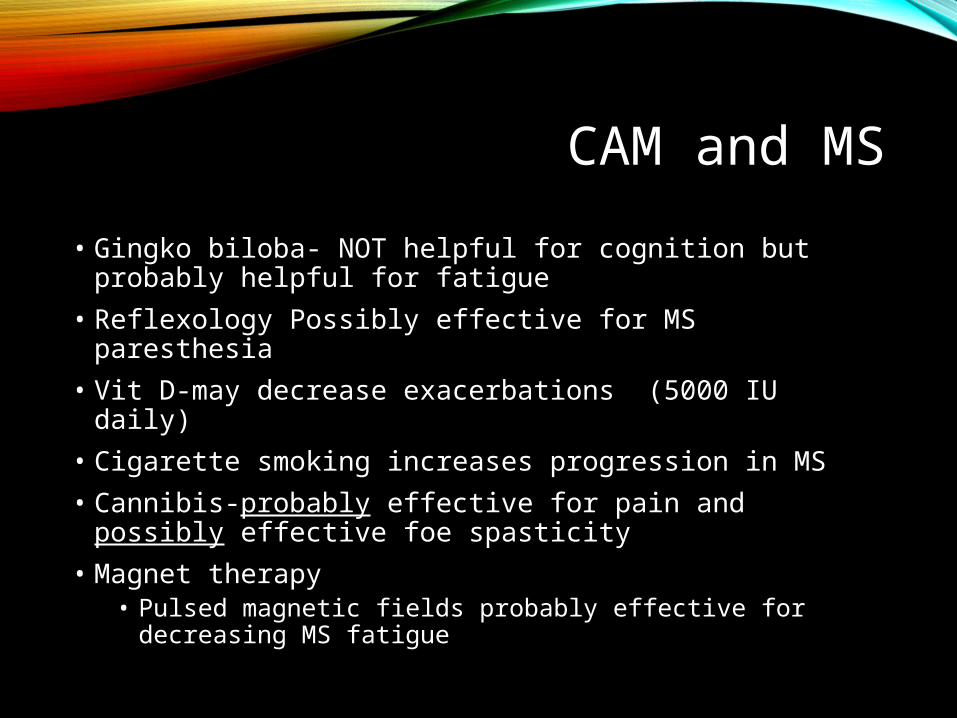
CAM and MS
• Gingko biloba- NOT helpful for cognition but probably helpful for fatigue
• Reflexology Possibly effective for MS paresthesia
• Vit D-may decrease exacerbations (5000 IU daily)
• Cigarette smoking increases progression in MS
• Cannibis-probably effective for pain and possibly effective foe spasticity
• Magnet therapy• Pulsed magnetic fields probably effective for
decreasing MS fatigue

Pulsed magnetic Field Therapymay help with MS fatigue

CAM in MS: SLeep
•No melatonin!•Theanine Serene (oral supplement)




PROGNOSIS
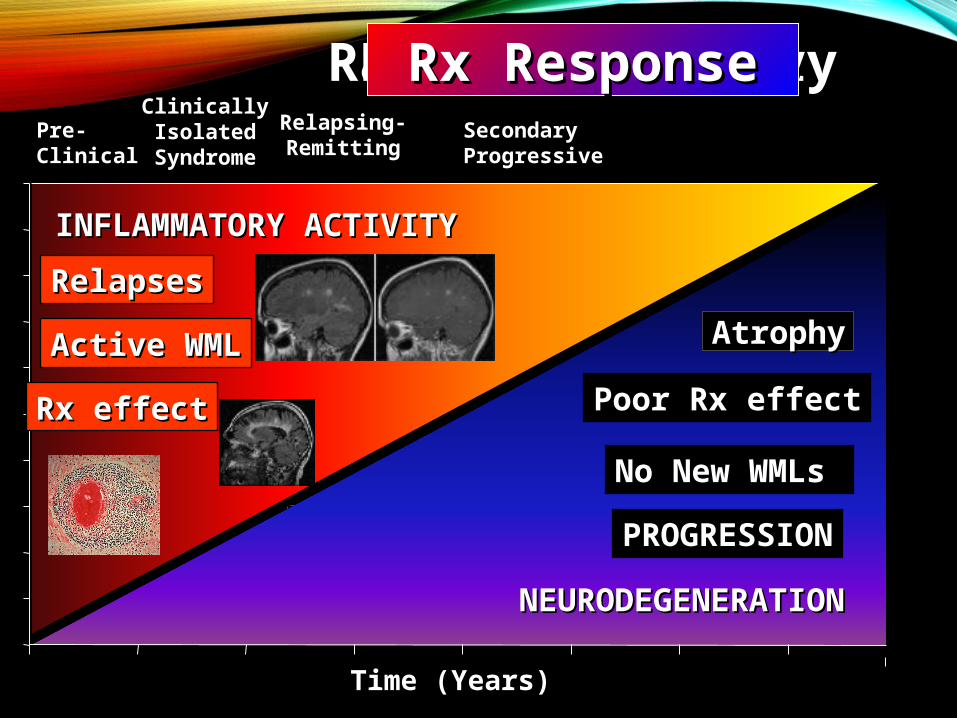
Time (Years)
Dis
ease
Par
amet
er
INFLAMMATORY ACTIVITYINFLAMMATORY ACTIVITY
NEURODEGENERATIONNEURODEGENERATION
PROGRESSIONPROGRESSION
RelapsesRelapses
Active WMLActive WML
Time (Years)
Pre-Pre-ClinicalClinical
ClinicallyClinicallyIsolatedIsolated
SyndromeSyndrome
Relapsing-Relapsing-RemittingRemitting
SecondarySecondaryProgressiveProgressive
Rx effectRx effect Poor Rx effectPoor Rx effect
No New WMLs No New WMLs
CLINICALLYCLINICALLYRadiographicallyRadiographicallyPathologicallyPathologicallyRx ResponseRx Response
AtrophyAtrophy
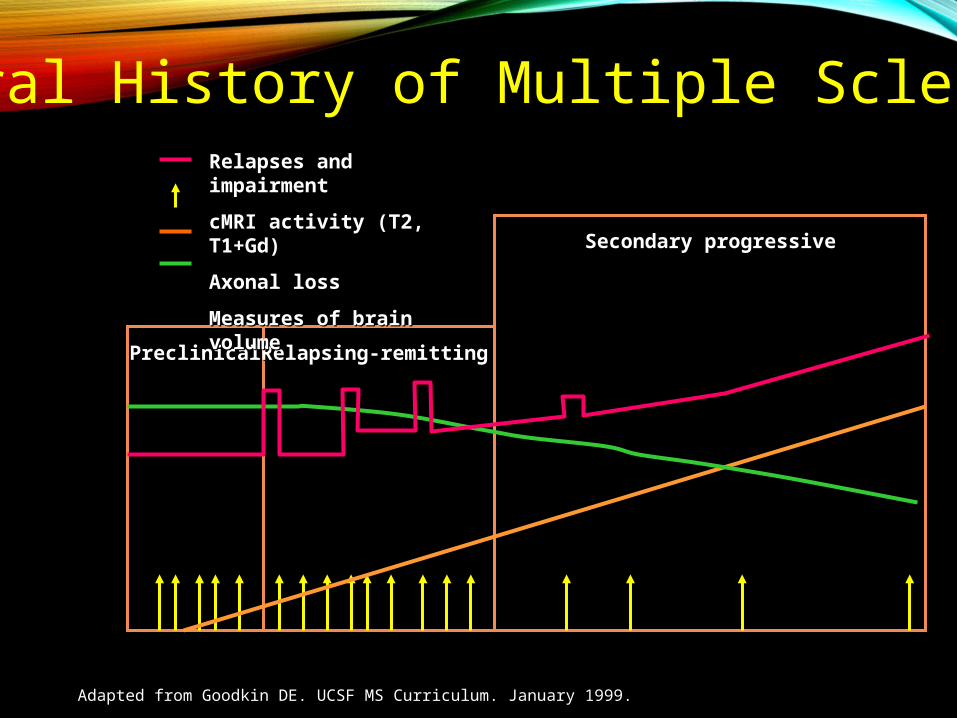
PreclinicalPreclinical Relapsing-remittingRelapsing-remitting
Secondary progressiveSecondary progressive
Adapted from Goodkin DE. UCSF MS Curriculum. January 1999.
Natural History of Multiple SclerosisRelapses and impairmentRelapses and impairment
cMRI activity (T2, T1+Gd)cMRI activity (T2, T1+Gd)
Axonal lossAxonal loss
Measures of brain volumeMeasures of brain volume
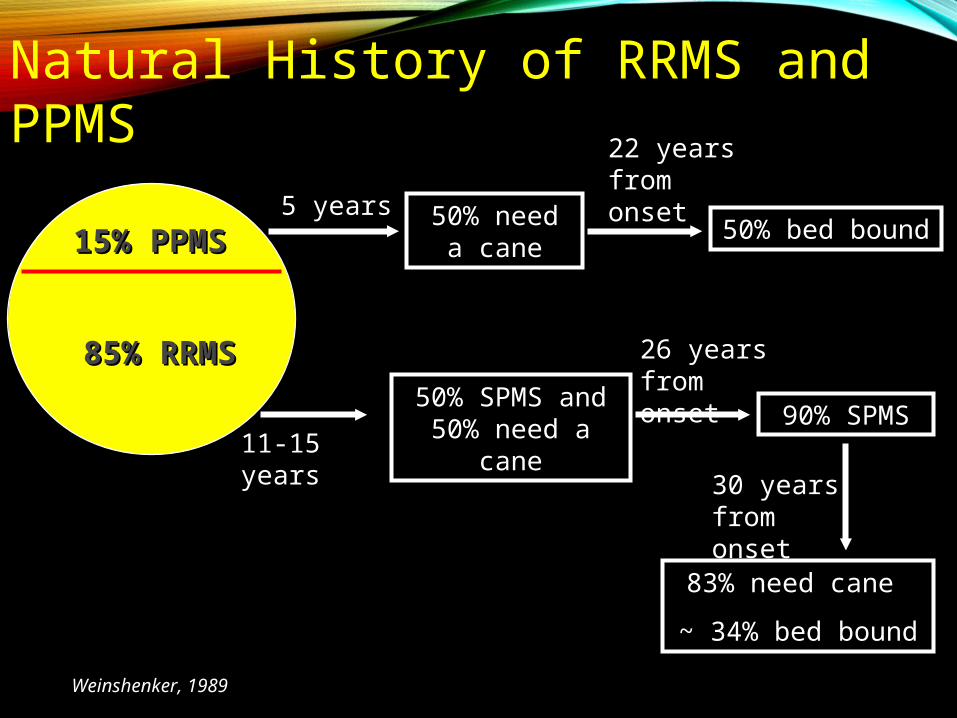
Weinshenker, 1989
15% PPMS15% PPMS
85% RRMS85% RRMS50% SPMS and
50% need a cane 90% SPMS11-15 years
26 years from onset
50% need a cane
5 years
Natural History of RRMS and PPMS
30 years from onset
83% need cane
~ 34% bed bound
22 years from onset
50% bed bound
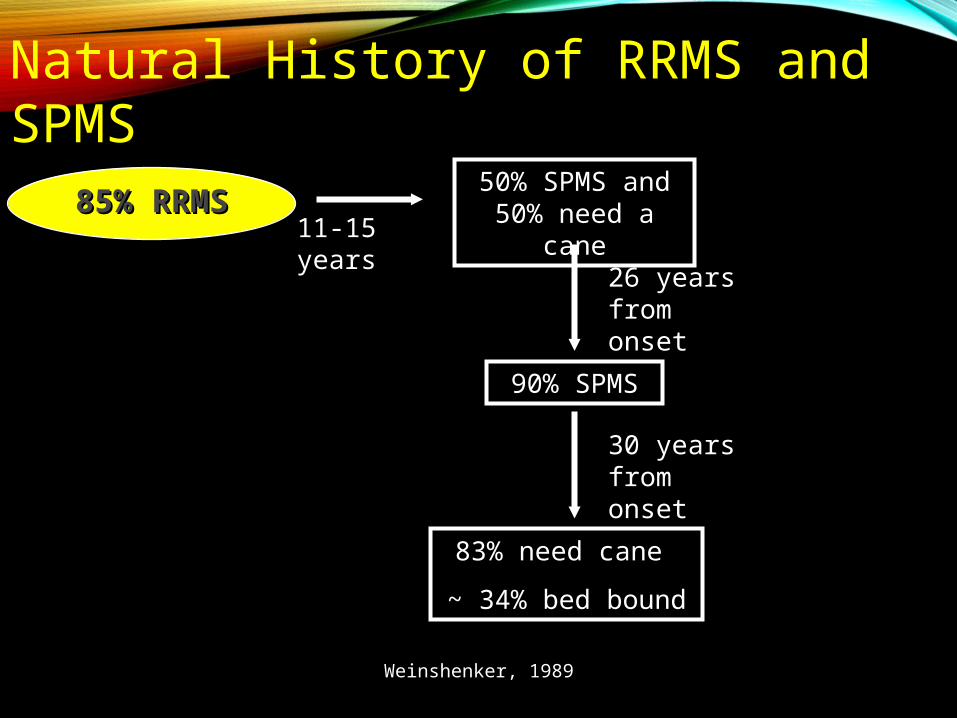
Weinshenker, 1989
85% RRMS85% RRMS50% SPMS and
50% need a cane
90% SPMS
11-15 years
26 years from onset
Natural History of RRMS and SPMS
30 years from onset
83% need cane
~ 34% bed bound

Summary
• Demographics
• Presentation
• Differential
• Evaluation
• Treatment


Have PAtients call the Hawaii MS SOciety
808 532 0811













