Embed Size (px)
DESCRIPTION
Citation preview

Mycobacterium tuberculosis

Mycobacterium: Slender rods that sometimes show branching
filamentous forms resembling fungal mycelium. In liquid cultures they form a mold-like pellicle~
hence the name ‘mycobacterium’ = Fungus like bacteria.
They are acid-fast, aerobic, non-motile, non-capsulated and non-sporing, obligate parasites, opportunistic pathogens and saprophytes.
Robert Koch in 1882, isolated the mammalian strain and proved its causative role in Tuberculosis.
Mycobacterium has many bacilli, most common of them are M. tuberculosis and M. lepra.

Mycobacterium tuberculosis
Straight or slightly curved rod of about 3µm x 0.3µm
Occurs either in pairs or small clumps. Gram Positive; but they resist decolorisation after
being stained with basic dyes ~ but they resist decolorisation with 20% Sulphuric acid and absolute alcohol when treated with acid fast stains.

Cultural Characteristics
O Colonies appear in about 2 weeks & sometimes may take up to 8 weeks.
O OPTIMUM TEMPERATURE is 37º C; Growth doesn’t occur above 40ºC or below 25ºC.
O OPTIMUM pH is 6.4 to 7O M. tuberculosis are
eugonic.O The organisms are highly
susceptible even to traces of toxic substances present in the media.
O Koch originally grew the bacilli on heat coagulated bovine serum.
O SOLID MEDIA:CONTAINING EGG * Lowenstein-Jensen * Petragnini * DorsetCONTAINING BLOOD,SERUM * Tarshis * LoefflerCONTAINING POTATO *Pawlowsky
O LIQUID MEDIA: * Dubos * Middlebrooks * Proskauer & Beck’s * Sula & Sauton’s

Cultural Differences of Liquid & Solid Media
Growth in Liquid Media Growth in Solid Media
O Growth begins at the bottom, without dispersing the agents.
O The organisms creeps up the sides and forms a prominent surface pellicle which extends along the side of the medium.
O Diffuse growth is observed in Dubos’ medium.
O Virulent strains form long serpentine cords while a-virulent strains grow in a dispersed manner.
O Forms dry, rough, raised, irregular colonies with a wrinkled surface.
O They are creamy-white, becoming yellowish or buff colored on further incubation.
O They are tenacious and not easily emulsified.

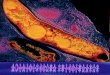
M. Tuberculosis as seen on Lowenstein-Jensen Medium

Lifecycle of M. tuberculosis in Human Tuberculosis spreads through the air when a person with untreated
pulmonary TB coughs or sneezes. Once in the body, the tuberculosis bacilli has about 5 stages in its life cycle:
Stage 1: OnsetBacteria is inhaled through the air and typically engulfed by alveolar macrophages. At this instant, disease progression depends on the virulence of the inhaled strain and the anti mycobacterial capabilities of the macrophage in question. In some cases, the bacteria are able to reproduce and initiate the infection. Tuberculosis begins when the inhaled mycobacterial nuclei reach aveolar machrophages Stage 2: Symbiosis If the initial macrophage does not succeed in killing the bacteria, the bacteria will replicate until the macrophage bursts. The bacteria are now engulfed by other alveolar macrophages and non activated macrophages. The macrophages that arrive from the bloodstream engulf the exposed bacteria in a symbiotic manner—neither the host nor the bacteria is harmed

Contd
Stage 3: Initial Caseous Necrosis The next stage of disease development begins when bacterial reproduction slows. Growth slows because as the bacteria reproduce, they kill all the surrounding non activated macrophages and run out of cells to divide within. In addition, the increased number of bacteria produces anoxic conditions and reduces the local pH The bacteria can no longer reproduce in this tubercule, but can remain alive for long periods of time at this state. The host kills its own tissues to prevent the spread of the bacteria. Also at this stage, the host will test positive for tuberculin.
Stage 4: Interplay of Tissue-Damaging and Macrophage Activating Immune Response Macrohpages surround the tubercule, some of which may be inactivate. M. tuberculosis uses the inactive macrophages to reproduce, causing the tubercule to grow. The tubercule may break off or spread into the bronchus, and then other parts of the lung. If the tubercules reach the blood stream, the patient can develop tuberculosis outside of the lungs, which is known as milliary tuberculosis. Secondary lesion can develop almost anywhere within the body, but are commonly found in the bones, joints, lymph nodes, and genitourinary system.
Stage 5: Liquefaction and Cavity FormationAt some point the centres of the tubercles may liquefy, which produces a very conducive environment for the bacteria and rapid spread of the disease. Only a very small % of infected individuals will progress to this stage.

Resistance of M. tuberculosis
Heat Labile ~ Killed at 60ºC in 15 – 20 minutes. Cultures are killed by exposure to sunlight for 2 hours . Cultures remain viable at RT for 6 – 8 months and can stored
up to 2 years at -20ºC. Bacilli in sputum remain alive for 20 to 30 hours
in droplet nuclei are viable for 8 to 10 days. Bacilli are resistant to ~ Chemical disinfectants, 5% phenols,
15% Sulphuric acid, 3% nitric acid, 5% Oxalic acid. But they are very sensitive to ~ Formaldehyde and
Gluteraldehyde. They are destroyed by tincture of Iodine in 5 minutes & by 80% ethanol in 2 to 10 minutes.

LABORATORY DIAGNOSIS:
o Demonstrating the bacilli in the lesion by microscopy
o Isolating the bacilli in the culture
o Transmitting the infection to experimental animals
o Demonstrating hypersensitivity to tuberculoprotein

PROPHYLAXIS: EARLY DETECTION AND TREATMENT ~ IMMUNOPROPHYLAXIS
Immunoprophylaxis
* By Intradermal Injections of live attenuated vaccine developed by Calmette and Guerin in 1921, called BCG - Bacille Calmette Guerin .* Injection of BCG in animals induces self limited infection with production of small tubercles, thereby giving rise to delayed hypersensitivity and immunity.* BCG also has many complications : Local: Abscess, Indolent ulcer, Tuberculoids, Confluent and lupoid lesions. Regional: Enlargement and Suppulation of draining Lymph nodes. General: Fever, Mediastinal adenitis, Erythema nodosum, tendency to keloid formation and rarely non-fatal meningitis.
In TB endemic countries such as India, BCG vaccines are administered to babies by intradermal injections immediately after birth or as early as possible after that , but before age of 12 months.
Babies born to AFB +ve mothers should be given BCG vaccine ONLY AFTER a course of preventive chemotherapy.
















![[Micro] mycobacterium tuberculosis](https://img.pdfslide.net/doc/110x75/55d6fc67bb61ebfa2a8b47ea/micro-mycobacterium-tuberculosis.jpg)







