Embed Size (px)
DESCRIPTION
coração
Citation preview

part of
RESEARCH ARTICLE
10.2217/17435889.2.3.333 © 2007 Future Medicine Ltd ISSN 1743-5889 Nanomedicine (2007) 2(3), 333–344 333
Vitamin E TPGS-emulsified poly(lactic-co-glycolic acid) nanoparticles for cardiovascular restenosis treatmentSi-Shen Feng1,2,3†, Wutao Zeng1,7, Yean Teng Lim5,6, Lingyun Zhao1, Khin Yin Win1, Reida Oakley5, Swee Hin Teoh4, Ronald Chi Hang Lee6 & Shirong Pan7
†Author for correspondence1Department of Chemical & Biomolecular Engineering, National University of Singapore, Block E5, 02–11, 4 Engineering Drive 4, 117576 SingaporeTel.: +65 6516 3835;Fax: +65 6779 1936;E-mail: [email protected] of Bioengineering, National University of Singapore, Singapore3Nanoscience & Nanoengineering Initiative (NUSNNI), National University of Singapore, Singapore4Department of Mechanical Engineering, National University of Singapore, Singapore5Department of Surgery, National University of Singapore, Singapore6Cardiac Department, National University Hospital, Singapore7Division of Cardiology, Cardiovascular Medical Department, The First Affiliated Hospital, Zhongshan University Medical School, Guangzhou, China
Keywords: cardiovascular stents, nanobiotechnology, nanomedicine, paclitaxel, percutaneous transluminal coronary angioplasty, sirolimus
Aims: Paclitaxel is one of the most effective antiproliferative agents and it has been applied in the development of drug-eluting stents. There are difficulties, however, in using paclitaxel in clinical applications owing to its poor solubility and side effects. We have synthesized nanoparticles of biodegradable polymers for the effective and sustainable delivery of paclitaxel and other antiproliferative agents for restenosis treatment. Methods & results: Paclitaxel-loaded poly(lactic-co-glycolic acid) (PLGA) nanoparticles were prepared by a modified solvent extraction/evaporation method with D-α-tocopheryl polyethylene glycol 1000 succinate (TPGS) or polyvinyl alcohol (PVA) as an emulsifier. Drug-loaded nanoparticles were characterized for size and size distribution, surface morphology, surface charge, drug-encapsulation efficiency and in vitro drug-release kinetics. Cellular uptake of fluorescent nanoparticles was investigated in vitro in coronary artery smooth muscle cells and in vivo in the carotid arteries of rabbits. The antiproliferative effects of the nanoparticle formulations were assessed in vitro in close comparison with Taxol®. Both the PVA- and TPGS-emulsified nanoparticles have similar size and size distribution, surface morphology and dispersion stability and showed great advantages over paclitaxel in in vitro cellular uptake and cytotoxicity than Taxol. The TPGS-emulsified nanoparticle formulation has higher drug-encapsulation efficiency, cellular uptake and cytotoxicity than the PVA-emulsified nanoparticle formulation. IC50 in 24-h culture with coronary artery smooth muscle cells is 748 ng/ml for paclitaxel, 708 ng/ml for PVA-emulsified nanoparticles and 474 ng/ml for TPGS-emulsified nanoparticles, respectively. Conclusion: TPGS-emulsified PLGA nanoparticles have great potential for the effective and sustainable delivery of antiproliferative agents and for the development of nanoparticle-coated stents, which may become the third generation of cardiovascular stents.
Coronary atherosclerosis and heart attack are theleading causes of mortality in the world. The mostcommon treatments so far include percutaneoustransluminal coronary angioplasty (PTCA) withor without intracoronary stents. However,30–50% of patients experience restenosis within3–6 months of PTCA treatment [1]. There are twokinds of treatment for restenosis currently:mechanical treatment and drug therapy. Theformer is stenting [2]. Although popular, stentingdoes not solve the problem becasue 10–15% ofthe patents will suffer from restenosis again within6 months. The latter treatment type includes thetreatment by antiproliferative/antiplatelet/anti-coagulant agents, calcium channel antagonists,inhibitors of angiotensin-converting enzyme, cor-ticosteroids or a fish-oil diet [3]. Nevertheless, drugtherapy is not that effective owing to the purepharmaceutical properties and the multidrugresistance (MDR) effects of the antiproliferativeagents, such as paclitaxel and sirolimus. Researchis thus focused on more effective drug-deliverydevices, such as nanoparticles of biodegradable
polymers, for local delivery and a combination ofdrug therapy and devices, such as drug-elutingstents; for example, the Cypher® stent, whichreleases sirolimus, and the TAXUS® stent, whichreleases paclitaxel.
Paclitaxel (Taxol®) is one of the best anti-neoplastic drugs that has been found from naturein recent decades. It has excellent therapeuticeffects against a wide spectrum of cancers [4]. Itwas approved by the US FDA for ovarian cancerin 1992, for advanced breast cancer in 1994 andfor early-stage breast cancer in 1999. The mech-anism of its anticancer effects has been inten-sively investigated. It inhibits mitosis in tumorcells by binding to microtubules. Paclitaxel aidspolymerization of tubulin dimers to form micro-tubules and thus stabilizes the microtubules,leading to cell death [5–7]. Paclitaxel is thus anantiproliferative drug that could be beneficial formany other diseases caused by a loss of control ofcell proliferation. Among them is cardiovascularrestenosis. Due to its difficulty in clinical admin-istration and MDR, various dosage forms of
For reprint orders, please contact:[email protected]

RESEARCH ARTICLE – Feng, Zeng, Lim et al.
334 Nanomedicine (2007) 2(3) future science groupfuture science group
paclitaxel have been under intensive investiga-tion. The dosage form used most often is Taxol,which is formulated in Cremophor EL. Thisadjuvant is responsible for serious side effects,including hypersensitivity reactions, nephro-toxicity, neurotoxicity and cardiotoxicity. Someof the side effects are serious, even life-threaten-ing [8–13]. A better dosage form, docetaxol (Taxo-tere®), was developed later. Although it achievesa higher survival rate (SR), the side effects arestill a problem and are probably caused by theadjuvant polysobate.
Our research here has investigated the feasibil-ity of the formulation of antiproliferative agentsby biodegradable poly(lactic-co-glycolic acid)(PLGA) nanoparticles, which are prepared by thesolvent extraction/evaporation method by usingamphiphilic poly(vinyl alcohol) (PVA) orD-α-tocopheryl polyethylene glycol 1000 succi-nate (TPGS) as an emulsifier for the treatmentand prevention of restenosis. The drug-loadednanoparticles were then characterized by varioustechniques, such as laser light scattering fornanoparticle size and size distribution, field-emission scanning electron spectroscopy(FESEM) and atomic force microscopy (AFM)for surface morphology and zeta-potential forsurface charge. High-performance liquid chro-matography (HPLC) was employed to measurethe drug-encapsulation efficiency (EE) and thein vitro drug-release kinetics. Cellular uptake offluorescent nanoparticles was investigatedin vitro in coronary artery smooth muscle cells(CASMCs) and in vivo in carotid arteries of rab-bits, which was visualized by confocal laser scan-ning spectroscopy (CLSM). The antiproliferativeeffects of the nanoparticle formulations wereassessed in vitro by the MTS assay and analyzedwith consideration of the drug-release kinetics inclose comparison with Taxol.
The drug-loaded PLGA nanoparticles can beused either for local delivery by balloon catheteror for the development of a novel type of cardio-vascular stent – the nanoparticle-coated stent[101]. Why do we prefer the nanoparticle formula-tion? This is because pure paclitaxel is not bio-adhesive to the cell membrane owing to its poorpharmaceutical properties, including the MDReffects. Our pioneering research on the nano-particle formulation of paclitaxel has demon-strated that nanoparticles are more adhesive to,and thus easier to be taken up by, cancer cells,such as Caco-2 cells and HT-29 cells, than themicroparticle formulation and the free drug itself[14–16]. The nanoparticle-coated stents may
become a new (the third) generation of cardiovas-cular stents, which will solve the problems of thesecond-generation stents – the drug-eluting stents[101]. Although successful, these drug-elutingstents have some problems, such as low drug-load-ing ability, slow and incomplete drug release, inef-ficient uptake by vascular smooth muscle cells(VSMCs) [17–20], late angiographic stent thrombo-sis (LAST) [21] and issues of long-term safety andefficacy, which have raised the cost–effectivenessproblem [22,23].
PLGA nanoparticle formulation of anti-proliferative drugs for the treatment of cardio-vascular restenosis has had a history of more than10 years [24–31]. However, the reports of a PLGAnanoparticle formulation of paclitaxel for resten-osis treatment are few in the literature [32,33],although this drug has been used widely in drug-eluting stents. The idea of TPGS-emulsifiedPLGA nanoparticles for restenosis treatment isnovel, coming from our research on TPGS usedas an effective emulsifier or as a component of thenovel PLA–TPGS copolymer in the nanoparticleformulation of anticancer drugs, which resultedin high drug EE, high cellular uptake of thenanoparticles by cancer cells, long half-life in cir-culation and high therapeutic effects demon-strated by high area-under-the-curve (AUC) ofthe in vivo pharmacokinetic measurement [16].
Materials & methodsPLGA with L:G molar ratio of 50:50 and Mw of40,000–75,000, PVA with Mw of30,000–70,000, fluorescence marker cou-marin-6, phosphate-buffered saline (PBS), mini-mum essential medium, penicillin–streptomycinsolution, trypsin–EDTA solution, Triton® X-100, Hank’s balanced salt solution (HBSS) and3-(4,5-dimethylthiazol-2-yl)-5-(3-carboxymeth-oxyphenyl)-2-(4-sulfonyl)-2H-tetrazoliumn(MTS) were purchased from Sigma (St Louis,MO, USA). Paclitaxel was purchased from Yun-nan Hande Biotechnology Inc (China). Taxolwas from Bristol-Myers Squibb Caribbean Com-pany (USA). Vitamin E D-α-tocopheryl polyeth-ylene glycol 1000 succinate (vitamin E TPGS orsimply TPGS) was obtained from EastmanChemical Company (USA). Dichloromethane(DCM, analytical grade) was from Merck(Darmstadt, Germany) and acetonitrile (HPLCgrade) was from Fisher Scientific (NJ, USA).Fetal bovine serum (FBS) was received fromGibco (Life Technologies, AG, Switzerland).Ultrapure water (Millipore, Bedford, MA, USA)was used throughout the experiment.

Nanoparticles of biodegradable polymers for restenosis treatment – RESEARCH ARTICLE
335future science groupfuture science group www.futuremedicine.com
Preparation of nanoparticlesPLGA nanoparticles loaded with paclitaxel orfluorescent marker (0.5% coumarin-6) wereprepared by a modified solvent extraction/evap-oration method (single emulsion) by using PVAor TPGS as the emulsifier [34,35]. In brief, 8 mlof dichloromethane (DCM) solution of110 mg PLGA and 11 mg paclitaxel was addeddrop by drop to a 120 ml aqueous phase, inwhich PVA 600 mg or TPGS 36 mg wasadded. The solution was then emulsified for120 s using a microtip probe sonicator(XL2000, Misonix Incorporated, NY, USA) at50 W in pulse mode. The formed oil in water(o/w) emulsion was stirred gently at room tem-perature (22°C) by a magnetic stirrer overnightto evaporate the organic solvent. The resultingsample was collected by centrifugation(12,000 rpm, 15 min, 16°C; Eppendorf model5810R, Eppendorf, Hamburg, Germany) andwashed three times with ultrapure water. Theproduct was freeze-dried (Alpha-2, MartinChrist Freeze Dryers, Germany) to obtain afine powder of nanoparticles, which was kept ina vacuum dessicator. We did not use any cryo-protectant in the freeze-dry process because allthe materials, including paclitaxel and TPGS,are stable in lyophilization.
Characterization of nanoparticlesSize & size distributionNanoparticle size and size distribution weredetermined by laser light scattering with a par-ticle size analyzer (90 Plus, Brookhaven Insti-tute, Huntsville, NY, USA) at a fixed angle of90° at 25°C. In brief, the dried nanoparticleswere suspended in filtered deionized water andsonicated to prevent particle aggregation andto help form a uniform dispersion of nano-particles. The size distribution was given bythe polydispersity index.
Surface morphologyMorphology of the drug-loaded nanoparticleswas observed by FESEM (JSM-6700F,JEOL.LED, Japan), which requires an ioncoating with platinum by a sputter coater(JFC-1300, Jeol, Tokyo) for 40 s in a vacuumat a current intensity of 40 mA after preparingthe sample on metallic studs with double-sidedconductive tape. AFM was conducted withNanoscope IIIa in the tapping mode. Beforeobservation, the nanoparticles were fixed on adouble-sided sticky tape that was stuck to thestandard sample stud.
Drug EEThe amount of drug encapsulated in the nano-particles was determined in triplicates by HPLC(Agilent LC 1100 series). 3 mg of nanoparticleswere dissolved in 1 ml of DCM, and 3 ml ofacetonitrile-water (50:50) was then added. Anitrogen stream was introduced to evaporatethe DCM until a clear solution was obtained.The solution was put into vials to detect thepaclitaxel concentration by HPLC. For HPLCanalysis, a reverse phase Inertsil® ODS-3 col-umn (150 x 4.6 mm i.d., pore size 5 µm, GLScience, Tokyo, Japan) was used and the mobilephase was delivered at a rate of 1 ml/min by apump (HP 1100 High Pressure GradientPump). 50 µl of sample was injected by an autosampler (HP 1100 Autosampler) and the col-umn effluent was detected at 227 nm with avariable wavelength detector (HP 1100 VWD).The calibration curve was prepared for thequantification of drug in the nanoparticles andit was linear over the range of 50–10,000 ng/mlwith a correlation factor of r2 = 0.9999. Themeasurement was performed in triplicate. Thedrug EE was obtained as the mass ratio betweenthe amount of paclitaxel incorporated in thenanoparticles and that used in the nanoparticlepreparation process [34,35].
Surface chargeZeta-potential is an indicator of surface charge,which determines particle stability in the dis-persion and redispersabliity of the nano-particles. Zeta-potential of nanoparticles wasdetermined by a zeta-potential analyzer (ZetaPlus, Brookhaven Instruments, Huntsville,NY, USA) by dipping a palladium electrode inthe sonicated particle suspension. The meanvalue of ten readings is reported.
In vitro drug-release kinetics 5 mg of the drug-loaded nanoparticles were putin a centrifuge tube containing 10 ml PBS(pH 7.4) with 0.1% tween 80. After dispersionby a vortex mixer (S0100–230V, Labnet Interna-tional Inc., USA), the tube was placed in anorbital shaker water bath at 37°C. The well-redispersed status of the nanoparticles for con-tinuous release measurement can be confirmedby the laser light-scattering measurement. Atdesignated time intervals, the tube was taken outand centrifuged at 11,500 rpm for 15 min. Thesupernatant was removed and extracted with5 ml DCM to determine the amount of drugreleased inside it. The pellets were resuspended

RESEARCH ARTICLE – Feng, Zeng, Lim et al.
336 Nanomedicine (2007) 2(3) future science groupfuture science group
in 10 ml of fresh PBS with 0.1% tween 80 forcontinuous release measurement. The analysisprocedure was the same as described in thedetermination of the EE [34,35].
Cell cultureIn the present study, CASMCs were provided byCambrex Bio Science Walkersville Inc, USA andpassages between five and ten were used.CASMCs were cultured in Dulbecco’s modifiedEagle’s medium (DMEM) supplemented with20% FBS (vol/vol %) and 1% penicillin–strep-tomycin solution. The cells were seeded at4.3 × 104 cells/cm2 in 96-well black plates withtransparent bases (Costar, IL, USA) for quantita-tive measurement of the cellular uptake of thefluorescent nanoparticles and cytotoxicity meas-urement of the drug-loaded nanoparticles or onthe Lab-Tek® chambered cover glasses (NagleNunc International, Naperville, IL, USA) forconfocal microscopy. The cell monolayer wascultured at 37°C in a humidified atmospherecontaining 5% CO2 and the medium wasreplaced every two days [34–36].
Uptake of nanoparticles by CASMCsQuantitative study: microplate reader analysisCASMCs were seeded in 96-well black platesand were incubated for 48 h. Cultural mediumwas then replaced by transport buffer HBSS andpre-incubated at 37°C for 1 h. After equilibra-tion, cellular uptake of fluorescent nanoparticleswas initiated by exchanging the transportmedium with 100 µl of the specific nanoparticlesuspension and incubated the cells for approxi-mately 1–6 h. The experiment was terminatedby washing the cell monolayer three times withPBS to eliminate excess nanoparticles that werenot entrapped by the cells. The cell membranewas permeated with Triton X-100 solution toexpose the internalized nanoparticles for quanti-tative measurement. Cellular uptake of the fluo-rescent nanoparticles was quantified byanalyzing the cell lysate in a Genios microplatereader. Uptake was expressed as the percentage ofthe fluorescence associated with the cells versusthat present in the feed solution [36].
Qualitative study: CLSMCASMCs were seeded on Lab-Tek® chamberedcover glasses (Nagle Nunc International, Naper-ville, IL, USA) and incubated at 37°C in a 95%air and 5% CO2 environment. On the day ofthe experiment, the growth medium wasreplaced by HBSS (pH 7.4). After equilibration
with HBSS for 30 min, the buffer was replacedwith a nanoparticle suspension (250 µg/ml inHBSS) and the monolayers were further incu-bated for 4 h. The monolayers were then washedthree times with fresh prewarmed transportbuffer to eliminate excess nanoparticles. Thecells were fixed with 70% ethanol and the nucleiwere stained by propidium iodide (PI). Thesamples were mounted in the fluorescentmounting medium (Dako, CA, USA) untilexamination was performed by the CLSM (ZeissLSM 410, Germany) equipped with an imagingsoftware, Fluoview FV300.
In vitro antiproliferative effects of drug-loaded nanoparticles The antiproliferative effects of the paclitaxel-loaded PLGA nanoparticles were investigatedin vitro by culturing CASMCs with the nano-particle formulation of paclitaxel in close com-parison with Taxol at the same paclitaxelconcentration. The cell viability (survival rate)was determined by the MTS assay, which is acolorimetric method to determine the number ofviable cells that are proliferating. It is composedof a solution of tetrazolium, which is bioreducedby metabolically active cells into a soluble forma-zan product in the culture medium. Its absorb-ance can be measured at 490 nm by a microplatereader (Genios, Tecan, Männedorf, Switzerland).The quantity of formazan is directly proportionalto the number of living cells. After cells wereseeded in a 96-well plate (Costar, IL, USA) andequilibrated with the DMEM medium (withoutFBS) for 1 h, the medium was removed and thenanoparticle suspension in DMEM with 10%FBS was added. After incubation for a scheduledtime, 20 µl of MTS inner salt was added to eachwell of a 96-well assay plate containing the sam-ples in 100 µl of culture medium. The plate wasincubated for 4 h at 37°C in a humidified atmos-phere containing 5% CO2 [34,35,37]. The cellmortality (death rate) is defined as 100% viabil-ity. It should be noted that it is the cell mortality,but not the cell viability, that should be propor-tional to the area-under-the-curve of the drugconcentration versus time.
Animal protocolsThe animal protocol was approved by the Insti-tutional Animal Care and Use Committees(IACUC, Protocol #: 802/05), Office of Life Sci-ence, National University of Singapore. Alto-gether, we used ten New Zealand white rabbitsfor the in vivo infusion experiment.

N anoparticles o f b iodegradable polym ers for restenosis treatm ent – R E S E A R C H A R T I C L E
337future science groupfuture science group www.futuremedicine.com
Rabbit anesthesia2.0–3.0 kg male New Zealand white rabbits wereanesthetized using Ketamine/Xylazine at a dos-age of 35 mg/kg/5 mg/kg subcutaneously fol-lowed by tracheal incubation and weremaintained with 1.0–2.0 vol% isoflurance, 70%N2O and 30 vol% oxygen.
Artery isolationCarotid arteries (averaging 3–4 cm in length)were isolated with all side branches being ligated.
Arteries injured by balloon catheterThe distal vessel was punctured by a 18 G trochar.The needle was withdrawn and the cannula was leftin the vessel. A balloon catheter (2.5 × 10–20 mm)was introduced and advanced in a retrograde fash-ion into the isolated artery segment via the cannuladistal in the vessel. Once positioned proximally, theballoon was inflated with saline to achieve visualoverstretch of the vessel and then withdrawn a dis-tance of 2 cm. The process was repeated twoadditional times. The catheter was then removed.
Infusion of nanoparticlesThe proximal portion was clamped by a non-crushing vascular clamp. The nanoparticle suspen-sion was injected at the distal end of the segment,which was connected to a pressure pump via thecannula. The arterial lumen was filled with thenanoparticle suspension at 1 atm pressure for 60 sand the vessel was harvested and the nanoparticlesflushed out by 0.9% saline water.
Histological examination of nanoparticle-infused arteriesNanoparticles loaded with the fluorescent markercoumarin-6 were used in this study. Each arterialsegment after nanoparticle infusion was flushed toremove the nanoparticles not taken up byCASMCs by 0.9% saline water and then frozen bydry ice with an OCT (Mile, Inc, Elkhart, IN,USA)-embedding compound. Cross sections of10 µm thickness were cut using a cryomicrotomeand mounted on the glass slides. The slides wereobserved under a confocal microscope.
Statistical analysisResults of the experiments are expressed asmean ± SD. In the nanoparticle cellular uptakeexperiment, the student unpaired t-test wasadopted for the comparison between the PVA-and TPGS-emulsified PLGA nanoparticles.The cytotoxicity study was tested by ANOVA.Probability values of p < 0.05 and p < 0.01were considered to be significant and highlysignificant, respectively.
Results & discussionsPhysicochemical properties of nanoparticlesSize, EE & surface charge of the drug-loaded nanoparticles The data reported in Table 1 represent the averageof five measurements. The emulsifier concentra-tion needed to form the nanoparticles was5.0% w/v (emulsifier weight/water phase vol-ume) for the PVA-emulsified nanoparticles and0.3% w/v for the TPGS-emulsified nano-particles. This means that TPGS was 16.7-timesmore effective than PVA as an emulsifier for usein the emulsification process, that is, to make thesame amount of nanoparticles, the requiredamount of TPGS could be 16.7-times less thanthat of PVA. A more effective recipe was alsoreported [16]. This is a significant advantage ofTPGS over PVA. Also from Table 1, the mean sizewith 10% drug loading was 257 ± 10.2 nm forthe PVA-emulsified nanoparticles and288 ± 11.7 nm for the TPGS-emulsified nano-particles. The light-scattering measurement ofthe particle size agrees well with that given by theSmile View software from the FESEM images.
The TPGS-emulsified nanoparticles achievedmuch higher EE (92.6 ± 10.0%) than the PVA-emulsified nanoparticles (55.8 ± 4.98%). It isclear that TPGS has an advantage over PVA,resulting in much higher EE and, therefore, inmuch higher drug loading in the nanoparticles.We mentioned earlier that 110 mg PLGA and11 mg paclitaxel were added in the organic sol-vent. The theoretical drug-loading ratio shouldhave been 10%. However, owing to incomplete
Table 1. The size and size distribution, drug-encapsulation efficiency and Zeta-potential of paclitaxel-loaded, PVA- or TPGS-emulsified PLGA nanoparticles.
Emulsifier Size (nm) Polydispersity EE (%) Zeta-potential (mv)
PVA (5.0% w/v) 257 ± 10.2 0.031 55.8 ± 4.98 -13.74 ± 1.94
TPGS (0.3 w/v) 288 ± 11.7 0.028 92.6 ± 10.0 -21.5 ± 3.57
EE: Encapsulation efficiency; PLGA: Poly(lactic-co-glycolic acid); PVA: Polyvinyl alcohol; TPGS: D-α-tocopheryl polyethylene glycol 1000 succinate.

RESEARCH ARTICLE – Feng, Zeng, Lim et al.
338 Nanomedicine (2007) 2(3) future science groupfuture science group
encapsulation, that is, less than 100% EE, theactual drug-loading ratio was modified by theEE values, which is thus 5.58% for the PVA-emulsified nanoparticles and 9.26% for theTPGS-emulsified nanoparticles.
Both types of drug-loaded nanoparticleswere stable in their dispersion, possessing neg-ative surface charges with high absolute valuesof zeta-potential (Table 1), which are-13.74 ± 1.94 mV for the PVA-emulsifiednanoparticles and -21.5 ± 3.57 mV for theTPGS-emulsified nanoparticles. The surfacecharge determines stability of the nanoparticlesuspension and resuspensability of the nano-particles. TPGS-emulsified nanoparticles thushave advantages over PVA-emulsified nano-particles in their suspension stability andresuspensability. This finding is in agreementwith that of our earlier research of nanoparti-cle formulation of paclitaxel for cancertreatment [37].
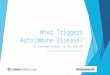
Morphology of nanoparticlesFigure 1 shows the FESEM images of PVA-(Figure 1A) and TPGS-emulsified (Figure 1B)
PLGA nanoparticles of 10% drug loading,which reveals their regular spherical shape andsmooth surface without any noticeable pinholesor cracks within the instrument resolution. Thesize distribution of all nanoparticles was unimo-dal, with a range of 150–500 nm and a meandiameter of 200–300 nm, as confirmed by thelaser light-scattering measurement. Figure 2 showsAFM images of paclitaxel-loaded, TPGS-emulsi-fied PLGA nanoparticles and a magnified imageof the nanoparticle surface, from which wrinklesand a small hole can be observed. The advantageof AFM is that it can reveal the true structurewith much higher resolution than SEM since theimage is obtained by direct contact or tapping ofthe AFM tip on or over the particle surface.
In vitro drug-release kineticsThe in vitro release profiles of paclitaxel from thePVA- or TPGS-emulsified PLGA nanoparticlesis shown in Figure 3, from which the effect of sur-face coating on the in vitro drug-release behaviorcan be observed. The drug-release kineticsexhibit a biphasic pattern characterized by a fastinitial burst during the first 5 days, followed by aslow, sustained release. An initial burst duringthe first 5 days of 67.9% for the PVA-emulsifiednanoparticles and 51.2% for the TPGS-emulsi-fied nanoparticles was followed by a first orderrelease with a reduced rate afterwards. Approxi-mately 81.2% of the PVA-emulsified nano-particles and 66.2% of the TPGS-emulsifiednanoparticles were released in 30 days. Pleasenote the release for the first 72 h is 58.6% for thePVA-emulsified nanoparticles and 43.4% for theTPGS-emulsified nanoparticles. These data willbe used later to interpret the cellular mortality ofthe drug formulated in the nanoparticles. Itseems that the drug release from the nano-particles is much faster (∼1 month) than therelease of drugs from drug-eluting stents(∼6 months), which represent two differenttreatments of restenosis: local drug delivery anddevice plus drug; each has advantages and disad-vantages. For local drug delivery, the nanoparti-cles are the reservoir of the drug after adsorptionby the CASMCs. The 1 month (or even faster)drug-release period may be appropriate for thetreatment. For drug-eluting stents, the stentsthemselves are the reservoir of the drug and alonger period would result in long-term treat-ment. Unfortunately, one of the major problems
Figure 1. Scanning electron microscopy images of paclitaxel-loaded nanoparticles.
FESEM Images of (A) polyvinyl alcohol- or (B) D-α-tocopheryl polyethylene glycol 1000 succinate-emulsified, drug-loaded poly(lactic-co-glycolic acid) nanoparticles of 10% drug loading.
Figure 2. Atomic force microscopy images of paclitaxel-loaded nanoparticles.
(A) Atomic force microscopy image of paclitaxel-loaded, D-α-tocopheryl polyethylene glycol 1000 succinate-emulsified poly(lactic-co-glycolic acid) nanoparticles and (B) magnified image of the nanoparticle surface.
BA
1 µm 1 µm
0.3 V
0.1 V
0.0 V
0.15
0.15
0.10
0.10
0.05
0.050
0 µmµm0.1 0.2 0.3
BA

Nanoparticles of biodegradable polymers for restenosis treatment – RESEARCH ARTICLE
339future science groupfuture science group www.futuremedicine.com
for drug-eluting stents is that the drug coated onthe stent surface cannot be completely released.An ideal solution is thus to combine the twotherapies, that is, to develop nanoparticle-coatedstents [101].
It should be pointed out that, although thesurfactant molecules are supposed to be washedaway after formulation, incomplete washing willresult in some residues remaining on the nano-particle surface, which will affect the drug release.Moreover, the release medium also plays a deci-sive role in determining the drug-release kinetics.The in vivo release could thus be much fasterthan the in vitro release owing to the interactionsbetween the plasma proteins and the drug. Thishas been confirmed by the in vitro measurementof drug release in plasma (data not shown).
Cellular uptake of nanoparticlesQualitative studyFigure 4 shows confocal microscopic images ofCASMCs after 4-h incubation with coumarin-6-loaded, PVA- (Figure 4A) or TPGS-emulsified(Figure 4B) PLGA nanoparticles at 37°C. Thenuclei were stained by PI (red), and the cou-marin-6-loaded nanoparticles (green) in thecytoplasm were visualized by overlaying imagesthat were obtained by fluorescein isothio-cyanate (FITC) filter and PI filter. The imagesshow that most of the internalized nano-particles are located in the cytoplasm. Somemay have penetrated into the nuclei.
It should be pointed out that the washingprocedure may not be able to wash theadhered nanoparticles out of the cell surface
and the residues would affect the cellularuptake measurement of the fluorescent nano-particles. The residues, however, would notaffect the CLSM images because CLSM has asectioning function.
Quantitative studyFigure 5 shows the effects of the incubation timeon the cellular uptake of the fluorescent PVA-or TPGS-emulsified PLGA nanoparticles. Thenanoparticle concentration used for incubationwith the CASMCs was 500 µg/ml. The signifi-cance of the TPGS-emulsified versus PVA-emulsified nanoparticles is p < 0.01. Figure 4
demonstrates that the cellular uptake of nano-particles increased with the incubation time.At each designated time, the TPGS-emulsifiednanoparticles could achieve much higher cellu-lar uptake than the PVA-emulsified nano-particles. After incubation for 6 h, theCASMC uptake was 38% for the TPGS-emul-sified nanoparticles versus 21% for thePVA-emulsified nanoparticles.
Figure 6 shows the effects of the nanoparticleconcentration on the cellular uptake of the flu-orescent PVA- or TPGS-emulsified PLGAnanoparticles after 4 h incubation. We can seefrom this figure that the cellular uptake ofnanoparticles increased with the nanoparticleconcentration and, at each designated nano-particle concentration of 100, 250 500 µg/ml,the TPGS-emulsified nanoparticles showedgreat advantages over the PVA-emulsifiednanoparticles in cellular uptake. For example,at the 500 µg/ml nanoparticle concentration,the cellular uptake was 33% for the TPGS-emulsified nanoparticles versus 13.5% for thePVA-emulsified nanoparticles. This advantageis significant (p < 0.01). The quantitativestudy confirmed the results observed from thequalitative study, showing that the TPGS-emulsified nanoparticles have advantagesresulting in higher cellular internalization thanthe PVA-emulsified nanoparticles. Althoughthe detailed mechanism is unknown,vitamin E facilitates cellular uptake of drugs.
It may be concerning that the fluorescentcoumarin-6 markers formulated in the nano-particles could leak, which may affect the resultof the cellular uptake measurement. To addressthis problem, we have conducted an experi-ment to measure the in vitro release of cou-marin-6 from the nanoparticles and our resultsshowed that the leakage, in up to 24 days, wasless than 5% and thus negligible [36].
Figure 3. In vitro drug releases of PVA- or TPGS-emulsified, paclitaxel-loaded PLGA nanoparticles of 10% drug loading.
Each point represents mean ± SD (n = 3).NP: Nanoparticle; PLGA: Poly(lactic-co-glycolic acid); PVA: Polyvinyl alcohol; TPGS: D-α-tocopheryl polyethylene glycol 1000 succinate.
0102030405060708090
0 5 10 15 20 25 30 35Time (day)
Cu
lmu
lati
ve r
elea
se (
%)
Vitamin E TPGS-emulsified NPsPVA-emulsified NPs

RESEARCH ARTICLE – Feng, Zeng, Lim et al.
340 Nanomedicine (2007) 2(3) future science groupfuture science group
In vitro antiproliferative effects of drug-loaded nanoparticlesWe first tested the cytotoxicity of the placeboPVA- or TPGS-emulsified PLGA nanoparticles,that is, the nanoparticles with no drug encapsu-lated. Figure 7 show the cytotoxicity of the placeboPVA- or TPGS-emulsified PLGA nanoparticles atnanoparticle concentrations of 2.5, 25 and100 µg/ml after 72 h incubation with the
CASMCs. Data represent the mean ± SD withn = 6. There was no significant decease in the cellviability for the two types of PLGA nanoparticlescompared with the control (p < 0.05), althoughthe placebo PVA-emulsified PLGA nanoparticlesshowed a slightly larger decrease in cell viabilityand such a decease becomes more significant athigh nanoparticle concentrations. This meansthat the TPGS-emulsified nanoparticles aremore biocompatible than the PVA-emulsifiednanoparticles. This is another advantage ofTPGS versus PVA as an emulsifier.
Figure 8 shows the effects of the drug concen-tration on CASMC viability after 72 h incuba-tion with the paclitaxel-loaded, PVA- or TPGS-emulsified PLGA nanoparticle suspension ver-sus Taxol. The table in the figure shows themeasured CASMC mortality (viability + mor-tality = 1) as well as that after the correctionmade by considering the 72 h drug releasefound from the drug-release profiles (Figure 3).The data represent mean ± SD of n = 6. Thesignificance of the TPGS-emulsified nanoparti-cles versus PVA-emulsified nanoparticles isp < 0.01 at 25 ng/ml drug concentration andp < 0.05 at 250 and 500 ng/ml drug concentra-tions. From the table it can be seen that the via-bility (the percentage of the CASMCs thatsurvived) after 72 h culture at 25 ng/ml paclit-axel concentration is 80.5% for Taxol, 79.1%for the PVA-emulsified nanoparticle formula-tion and 78.2% for the TPGS-emulsified nano-particle formulation. The mortality (thepercentage of the CASMCs killed) after 72 hculture at 25 ng/ml paclitaxel concentration isthus 19.5% for Taxol, 20.9% for the PVA-emulsified nanoparticle formulation and 21.8%for the TPGS-emulsified nanoparticle formula-tion, which means that the PVA- and theTPGS-emulsified nanoparticle formulations ofpaclitaxel have 1.07- and 1.12-times higherantiproliferative effects than the Taxol after 72 htreatment. Such advantages of the nanoparticleformulations versus the free drug should havebeen even more significant if the sustainabledrug-release manner of the nanoparticle formula-tion were further considered [16]. The drug releasefrom the nanoparticles for the first 72 h wasfound to be 58.6% for the PVA-emulsified nano-particles and 43.4% for the TPGS-emulsifiednanoparticles, respectively (Figure 3). Moreover,the drug release is from 0% at t = 0 to 58.6 or43.4% when Taxol was 100% immediately avail-able to the cells. The corrected mortality after72 h culture at 25 ng/ml paclitaxel concentration
Figure 4. Confocal microscopic images of coronary artery smooth muscle cells cultured with fluorescent nanoparticles.
Confocal microscopic images of coronary artery smooth muscle cells after 4 h incubation with coumarin-6-loaded, (A) polyvinyl alcohol- or (B) D-α-tocopheryl polyethylene glycol 1000 succinate-emulsified poly(lactic-co-glycolic acid) nanoparticles at 37°C. The nuclei were stained by propidium iodide (PI) (red), and the cellular uptake of fluorescent coumarin-6-loaded nanoparticles (green) in the cytoplasm were visualized by overlaying images obtained by a fluorescein isothiocyanate filter and a PI filter. The cells look unhealthy because they were being killed by the drug-loaded nanoparticles.
Figure 5. Effects of the incubation time on the cellular uptake of the fluorescent PVA- or TPGS-emulsified PLGA nanoparticles.
The nanoparticle concentration was 500 µg/ml. Each point represents mean ± SD (n = 4). The significance of the TPGS-emulsified versus PVA-emulsified nanoparticles is p < 0.01. CASMC: Coronary artery smooth muscle cell; PLGA: Poly(lactic-co-glycolic acid); PVA: Polyvinyl alcohol; TPGS: D-α-tocopheryl polyethylene glycol 1000 succinate.
50 µm 20 µm
BA
0
10
20
30
40
50
1 2 4 6
Incubation time (h)
CA
SM
C u
pta
ke o
f n
ano
par
ticl
es (
%)
PVA
TPGS

Nanoparticles of biodegradable polymers for restenosis treatment – RESEARCH ARTICLE
341future science groupfuture science group www.futuremedicine.com
should thus be 0.209/0.586/0.5 = 0.713 for thePVA-emulsified nanoparticle formulation and0.218/0.434/0.5 = 1.005 for the TPGS-emulsi-fied nanoparticle formulation, which meansthat the PVA- and the TPGS-emulsified nano-particle formulations of paclitaxel should actu-ally have 3.66- and 5.15-times higherantiproliferative effects than Taxol after the72 h treatment.
As can be seen from the table in Figure 8, thedifference in the measured mortality of theCASMCs after 72 h culture with the PVA- orTPGS-emulsified PLGA nanoparticles at thesame 25, 250, 500 ng/ml paclitaxel concentra-tions is not significant before corrected by drugrelease, which is 20.9, 33.9 and 38.1% for thePVA-emulsified nanoparticles versus 21.8,38.8 and 48.7% for the TPGS-emulsifiednanoparticles. Nevertheless, the cellular uptakeof the nanoparticles after 6 h culture wasfound before to be 21% for the PVA-emulsi-fied nanoparticles compared with 38% for theTPGS-emulsified nanoparticles (Figure 5).These two results seem to conflict. A fair expla-nation, however, can be found from the drug-release kinetics. The 72 h drug release is 55%for the PVA-emulsified nanoparticles, which ismuch higher than the 24% for the TPGS-emulsified nanoparticles. The effects of thehigher cellular uptake of the TPGS-emulsifiednanoparticles might have been balanced bythat of the lower drug-release rate.
Another way to evaluate the antiproliferativeeffectiveness of the drug in the various formula-tions is to measure their IC50, which is definedas the drug concentration needed to kill 50% ofthe CASMCs at a given period, say in 24 h.This can be obtained by finding the inter-section of the viability versus the drug concen-tration curve with a horizontal line of viabilityat 50%. By extrapolation, we can find fromFigure 8 that the IC50 in 24 h would be748 ng/ml for Taxol, 708 ng/ml for the PVA-emulsified nanoparticle formulation and474 ng/ml for the TPGS-emulsified nano-particle formulation, which implies that thePVA-emulsified nanoparticle formulation is5.35% more effective than Taxol and theTPGS-emulsified nanoparticle formulation is36.6% more effective than Taxol and 33.1%more effective than the PVA-emulsified nano-particle formulation in 24 h treatment. Consid-ering the sustainable-release manner of thenanoparticle formulations, their advantage overthe free drug should be even greater. If we usedthe corrected data in Figure 8, the IC50 wouldhave been 748 ng/ml for Taxol, 209 ng/ml for
Figure 6. Effects of the nanoparticle concentration on the cellular uptake of the fluorescent PVA- or TPGS-emulsified PLGA nanoparticles after 4 h incubation.
The significance of the TPGS-emulsified nanoparticles versus PVA-emulsified is p < 0.01. PLGA: Poly(lactic-co-glycolic acid); PVA: Polyvinyl alcohol; TPGS: D-α-tocopheryl polyethylene glycol 1000 succinate.
0
10
20
30
40
100 250 500Nanoparticle concentration (µg/ml)
Cel
l up
take
(%
)PVA
TPGS
Figure 7. Cytotoxicity of the placebo PVA- or TPGS-emulsified PLGA nanoparticles (with no drug encapsulated inside the nanoparticles) at various nanoparticle concentrations after 72 h incubation with CASMCs.
Data represent mean ± SD with n = 6. There were no significant changes in cell viability between PLGA nanoparticles and the control (p < 0.05), although the PVA-emulsified PLGA nanoparticles showed a slight decrease in cell viability at high nanoparticle concentration.CASMC: Coronary artery smooth muscle cell; PLGA: Poly(lactic-co-glycolic acid); PVA: Polyvinyl alcohol; TPGS: D-α-tocopheryl polyethylene glycol 1000 succinate.
0
20
40
60
80
100
120
2.5 25 100Nanoparticle concentration (µg/ml)
Per
cen
tag
e o
f co
ntr
ol
PVATPGS

RESEARCH ARTICLE – Feng, Zeng, Lim et al.
342 Nanomedicine (2007) 2(3) future science groupfuture science group
the PVA-emulsified nanoparticle formulationand 160 ng/ml for the TPGS-emulsifiednanoparticle formulation.
These in vitro experiments, of course, are justa preliminary evaluation of toxicity or therapeu-tic activity of the nanoparticle formulation. Fur-ther in vivo study will determine if theformulation can be used for clinical trials beforeit can become a commercial product.
Arterial uptake of nanoparticles Figure 9 shows confocal microscopic images ofcross sections of the carotid arteries of rabbitsthat were injured by balloon catheter and theninfused by the fluorescent nanoparticle suspen-sion. We can observe the carotid arterial uptake
of the fluorescent nanoparticles from these fig-ures: Figure 9A is the control, Figure 9B is thePVA-emulsified PLGA nanoparticles, Figure 9C
is the TPGS-emulsified nanoparticles andFigure 9D is the TPGS-emulsified nanoparticlesat 100-times higher resolution. We can see littlefluorescence in the control carotid artery wall(Figure 9A). After the fluorescent nanoparticleinfusion, fluorescence could be clearly observedin the carotid arteries walls (Figure 9B). TheTPGS-emulsified nanoparticles showed advan-tages in cellular uptake compared with thePVA-emulsified nanoparticles (Figure 9C & D).
As mentioned previously, the infusion time ofthe fluorescent nanoparticle suspension in thearteries was 60 s. Such a short period wasapplied to address the concern of retention ofthe nanoparticles by the arteries in actual prac-tice of local delivery by catheter. It is clear thatnanoparticle-coated stents could have advan-tages compared with local delivery, which couldresult in higher nanoparticle retention. Thisshould be further investigated.
Discussion & future perspectiveAlthough our in vivo experiment showed effec-tive internalization of the paclitaxel-loaded,TPGS-emulsified PLGA nanoparticles, furtherexperiments are needed to show the advantagesof the nanoparticle formulation versus the origi-nal drug in resulting in better therapeuticeffects. This means that an in vivo restenosismodel should be developed by balloon inflationinjury, which should then be treated by the nan-oparticle formulation of paclitaxel in close com-parison with Taxol. We shall continue thisresearch as soon as possible.
Although the above research showed that thenanoparticle formulation of antiproliferativeagents could have advantages versus the originaldrug for cardiovascular restenosis treatment andthat the TPGS-emulsified PLGA nanoparticlesmay have even better effects than the traditionalPVA-emulsified PLGA nanoparticles, it is stillunclear whether the MDR effects are involved inthe CASMC treatment by paclitaxel, that is,whether CASMCs are rich in multidrug pumpproteins (P-glycoproteins). Paclitaxel-elutingstents are effective in reducing restenosis and onecould argue that the current issue of late stentthrombosis could be related to a continued signif-icant reduction in smooth muscle cell prolifera-tion as well as endothelial coverage of the stentstruts, certainly not lack of efficacy of the drugdelivery. From this point of view, the nanoparticle
Figure 8. Effects of the drug concentration on CASMC viability after 72 h incubation with the paclitaxel-loaded, PVA- or TPGS-emulsified PLGA nanoparticle suspension versus Taxol®.
The attached table shows the measured CASMC mortality (viability + mortality = 1) as well as that after the correction made by considering the 72 h drug release found from the drug-release profiles (Figure 3). The data represent mean ± SD of n = 6. The significance of the TPGS-emulsified nanoparticles versus PVA-emulsified nanoparticles is p < 0.01 at 25 ng/ml drug concentration and p < 0.05 at 250 and 500 ng/ml drug concentration.CASMC: Coronary artery smooth muscle cell; PLGA: Poly(lactic-co-glycolic acid); PVA: Polyvinyl alcohol; TPGS: D-α-tocopheryl polyethylene glycol 1000 succinate.
58.6% for PVA-emulsified nanoparticles 43.4 % for TPGS-emulsified nanoparticles
3.583.653.66
1.051.071.07
6.315.615.15
229.0177.9100.5130.1115.671.3
1.371.221.12
49.738.621.838.133.920.9
36.331.719.5
CA
SM
C c
ell v
iab
ility
(%
)
0
20
40
60
80
100Taxol®
PVA
TPGS
Mortality (%) 25 ng/ml 250 ng/ml 500 ng/ml
(1) Taxol(2) PVA
(3) TPGS(2)/(1)(3)/(1)
(4) 72 h drug release(5) PVA (Corr)(6) TPGS(Corr)(5)/(1)(6)/(1)

Nanoparticles of biodegradable polymers for restenosis treatment – RESEARCH ARTICLE
343future science groupfuture science group www.futuremedicine.com
formulation may be more useful for local drugdelivery for the treatment of cardiovascularrestenosis. Further investigations are needed.
ConclusionWe synthesized PVA- and TPGS-emulsifiedPLGA nanoparticles to formulate antiprolifera-tive agents with paclitaxel as a model drug for thetreatment and prevention of cardiovascular reste-nosis. We found that the nanoparticle formula-tions of paclitaxel can achieve much highercellular uptake and much better in vitro anti-proliferative effects than Taxol. The emulsifierused in the nanoparticle preparation processplays a key role in determining the drug EE,drug-release kinetics, cellular uptake and thusantiproliferative effectiveness of the formulateddrug. The TPGS-emulsified nanoparticles havegreat advantages versus the PVA-emulsifiednanoparticles for local delivery of antiprolifera-tive drugs, which can also be used in developingnanoparticle-coated stents.
AcknowledgementsThis research is supported by research grantsR-397–000–014–112 (SS Feng: PI), National Universityof Singapore (NUS). The authors are grateful of the review-ers for their thoughtful comments, without which this papercould not have reached its current status.
Figure 9. Confocal microscopic images of the uptake of the drug-loaded nanoparticles by carotid arteries of rabbits.
(A) Control. (B) Polyvinyl alcohol-emulsified poly(lactic-co-glycolic acid) nanoparticles. (C) D-α-tocopheryl polyethylene glycol 1000 succinate (TPGS)-emulsified nanoparticles. (D) TPGS-emulsified nanoparticles (magnification 100×).
BA
150 µm 150 µm
C D
150 µm 20 µm
Executive summary
• Paclitaxel is one of the most effective antiproliferative agents and has been used in drug-eluting stents; however, owing to its undesired physicochemical and pharmaceutical properties, it has difficulties in formulation and delivery. Nanoparticles of biodegradable polymers can help to solve these problems.
• In this study, we prepared paclitaxel-loaded poly(lactic-co-glycolic acid) (PLGA) nanoparticles by a modified solvent extraction/evaporation method with D-α-tocopheryl polyethylene glycol 1000 succinate (vitamin E TPGS or simply TPGS) as an emulsifier, which was meant to have advantages versus those prepared by traditional emulsifiers, such as polyvinyl alcohol (PVA).
• Cellular uptake of fluorescent nanoparticles can be visualized and measured in vitro in coronary artery smooth muscle cells (CASMCs) and in vivo in carotid arteries of rabbits. Both showed excellent effects of the TPGS-emulsified nanoparticles.
• The TPGS-emulsified nanoparticles had a higher drug-encapsulation efficiency, cellular uptake and cytotoxicity than PVA-emulsified nanoparticle formulations. The IC50 in 24 h culture with CASMCs is only 474 ng/ml for the TPGS-emulsified nanoparticles in comparison with 708 ng/ml for the PVA-emulsified nanoparticles and 748 ng/ml for Taxol®, respectively.
• TPGS-emulsified PLGA nanoparticles are of great potential for the effective and sustainable delivery of antiproliferative agents and for the development of nanoparticle-coated stents, which may become the third generation of cardiovascular stents.
Bibliography1. Popma JJ, Califf RM, Topol EJ: Clinical
trials of restenosis after coronary angioplasty. Circulation 84, 1426–1436 (1991).
2. Wilensky RL, March KL, Grudus-Pislo I, Spuedy AJ, Hathaway DR: Methods and devices for local-drug delivery in coronary and peripheral arteries. Trends Cardiovasc. Med. 3, 163–170 (1993).
3. Herrman JP, Hermans WR, Vos J, Serruys PW: Pharmacological approaches to the prevention of restenosis following angioplasty – the search for the holy-grail. Drugs 46, 18–52 (1993).
4. Wani MC, Taylor HL, Wall ME, Coggon P, McPhail AT: Plant antitumor agents. VI. The isolation and structure of taxol, a novel antileukemic and antitumor
agent from Taxus brevifolia. J. Am. Chem. Soc. 93, 2325–2327 (1971).
5. Lopes NM, Adams EG, Pitts TW, Bhuyan BK: Cell kill kinetics and cell cycle effects of Taxol on human and hamster ovarian cell line. Cancer Chemother. Pharmacol. 32, 235–242 (1993).

RESEARCH ARTICLE – Feng, Zeng, Lim et al.
344 Nanomedicine (2007) 2(3) future science groupfuture science group
6. Rowinsky EK, Cazenave LA, Donehower RC: Taxol: a novel investigational antimicrotubule agent. J. Natl Cancer Inst. 82, 1247–1259 (1990).
7. Donehower RC, Rowinsky EK, Grochow LB, Longnecker SM, Ettinger DS: Phase-I trial of Taxol in patients with advanced cancer. Cancer Treat. Res. 71, 1171–1177 (1987).
8. Weiss RB, Donehower RC, Wiernik PH et al.: Hypersensitivity reactions from Taxol. J. Clin. Oncol. 8, 1263–1268 (1990).
9. Rowinsky EK, Onetto N, Canetta RM, Arbuck SG: Taxol – the 1st of the taxanes, an important new class of antitumor agents. Semin. Oncol. 19, 646–662 (1992).
10. Webster L, Linsenmeyer M, Millward M, Morton C, Bishop J, Woodcock D: Measurement of cremophor EL following taxol: plasma levels sufficient to reverse drug exclusion mediated by the multidrug-resistant phenotype. J. Natl Cancer Inst. 85, 1685–1690 (1993).
11. Fjallskog ML, Frii L, Bergh J: Is cremophor, solvent for paclitaxel, cytotoxic? Lancet 342, 873 (1993).
12. Dorr RT: Pharmacology and toxicology of cremophor EL diluent. Ann. Pharmacother. 28, S11–S14 (1994).
13. Kongshaug L, Cheng S, Moan J, Rimington C: Interaction of cremophor-EL with human plasma. Int. J. Biochem. 23, 473–478 (1991).
14. Sanders E, Ashworth CT: A study of particulate intestinal absorption and hepatocellular uptake. Use of polystyrene latex particles. Exp. Cell Res. 22, 137–145 (1961).
15. Florence AT, Hillery AM, Hussain N, Jani PU: Factors affecting the oral uptake and translocation of polystyrene nanoparticles: histological and analytical evidence. J. Drug Target. 3, 65–70 (1995).
16. Feng SS: New-concept chemotherapy by nanoparticles of biodegradable polymers – where are we now? Nanomedicine 1, 297–309 (2006).
17. Haery C, Sachar R, Ellis SG: Drug-eluting stents: the beginning of the end of restenosis? Cleve. Clin. J. Med. 71, 815–824 (2004).
18. Raja SG: Drug-eluting stents and the future of coronary artery bypass surgery: facts and fiction. Ann. Thorac. Surg. 81, 1162–1171 (2006).
19. van der Hoeven BL, Pires NMM, Warda HM et al.: Drug-eluting stents: results, promises and problems. Intl J. Cardiol. 99, 9–17 (2005).
20. Thomas MK, Gupta YK: Drug-eluting stents: a pharmacoclinical perspective. Natl Med. J. India 19, 195–199 (2006).
21. Lee CH, Lim J, Low A, Tan HC, Lim YT: Late angiographic stent thrombosis of polymer based paclitaxel eluting stent. Heart 92, 551–553 (2006).
22. Eisenberg MJ: Drug-eluting stents: the price is not right. Circulation 114, 1745–1754 (2006).
23. Ryan J, Cohen DJ: Are drug-eluting stents cost-effective? It depends on whom you ask. Circulation 114, 1736–1744 (2006).
24. Lanza G, Winter P, Cyrus T et al.: Nanomedicine opportunities in cardiology. Ann. NY Acad. Sci. 1080, 451–465 (2006).
25. Banai S, Chorny M, Gertz SD et al.: Locally delivered nanoencapsulated tyrphostin (AGL-2043) reduces neointima formation in balloon-injured rat carotid and stented porcine coronary arteries. Biomaterials 26, 451–461 (2005).
26. Panyam J, Lof J, O’Leary E et al.: Efficiency of Dispatch® and Infiltrator® cardiac infusion catheters in arterial localization of nanoparticles in a porcine coronary model of restenosis. J. Drug Target. 10, 515–523 (2002).
27. Das GS, Rao GHR, Wilson RF et al.: Colchicine encapsulation within poly(ethylene glycol)-coated poly(lactic acid)/poly(ε-caprolactone) microspheres-controlled release studies. Drug Deliv. 7, 129–138 (2000).
28. Labhasetwar V, Song CX, Humphrey W et al.: Arterial uptake of biodegradable nanoparticles: effect of surface modifications. J. Pharm. Sci. 87, 1229–1234 (1998).
29. Humphrey WR, Erickson LA, Simmons CA et al.: The effect of intramural delivery of polymeric nanoparticles loaded with the antiproliferative 2-aminochromone U-
86983 on neointimal hyperplasia development in balloon-injured porcine coronary arteries. Adv. Drug Deliv. Rev. 24, 87–108 (1997).
30. Guzman LA, Labhasetwar V, Song CX et al.: Local intraluminal infusion of biodegradable polymeric nanoparticles: a novel approach for prolonged drug delivery after balloon angioplasty. Circulation 94, 1441–1448 (1996).
31. Gradus-Pizlo I, Wilensky RL, March KL et al.: Local delivery of biodegradable microparticles containing colchicine or a colchicine analogue: effects on restenosis and implications for catheter-based drug delivery. J. Am. Coll. Cardiol. 26, 1549–1557 (1995).
32. Kolodgie FD, John M, Khurana C et al.: Sustained reduction of in-stent neointimal growth with the use of a novel systemic nanoparticle paclitaxel. Circulation 106, 1195–1198 (2002).
33. Das GS, Rao GHR, Wilson RF et al.: Controlled delivery of taxol from poly(ethylene glycol)-coated poly(lactic acid) microspheres. J. Biomed. Mater. Res. 55, 96–103 (2001).
34. Feng SS: Nanoparticles of biodegradable polymers for new concept chemotherapy. Expert Rev. Med. Devices 1, 115–125 (2004).
35. Feng SS, Mu L, Win KY, Huang GF: Nanoparticles of biodegradable polymers for clinical administration of paclitaxel. Curr. Med. Chem. 11, 413–424 (2004).
36. Khin YW, Feng SS: Effects of particle size and surface coating on cellular uptake of polymeric nanoparticles for oral delivery of anticancer drugs. Biomaterials 26, 2713–2722 (2005).
37. Feng SS: In vitro and in vivo studies on vitamin E TPGS-emulsified poly(D,L-lactic-co-glycolic acid) nanoparticles for clinical administration of paclitaxel. Biomaterials 27, 2285–2291 (2006).
Patent101. United States Patent Application
Publications: Nanoparticle coating for drug delivery: US2006/0188543 A1 (2006).