Embed Size (px)
Citation preview

New Advancements in the Treatment of Prostate Cancer
Simon Treissman MD FRCSCRoyal Inland Hospital
Department of Surgery
Kamloops RotaryHilton Doubletree Kamloops
November 27, 2013
New Advancements in the Treatment of prostate Cancer
“Movember” MadnessStarted in 2003 in Melbourne Australia by 30 “MO Bros”
Has Now spread to 45 countries and raised $447 million

New Advancements in the Treatment of prostate Cancer
Discussion:– Structure and Function of the normal prostate gland– What can go wrong with the prostate?– The problem of prostate cancer– Historical Perspectives– Traditional therapies– New advancements– The future

What is the prostate gland?
• What does a normal prostate gland look like?
Bladder
Prostate
Urethra
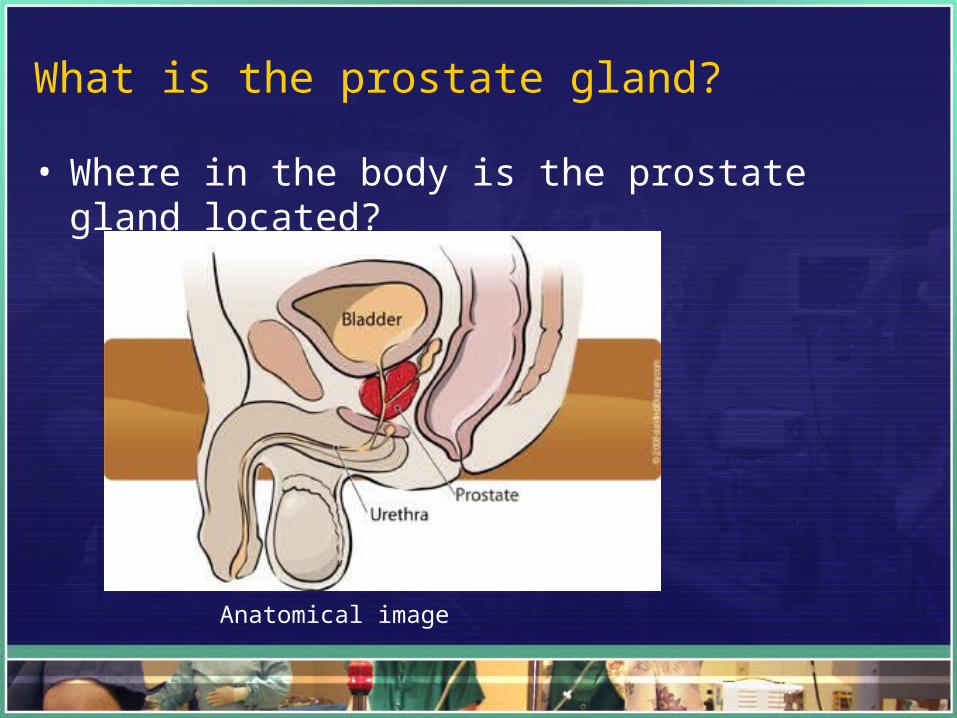
The prostate is located at the base of the bladder. Urine must pass through it on its way to the toilet.
Schematic
What is the prostate gland?
• Where in the body is the prostate gland located?
Anatomical image

What is the prostate gland?
• What does the normal prostate gland do?– Largest, most active male sex gland– Located at the base of the male pelvis– Lies “astride” the male urethra– Produces most of the ejaculate by volume– Ranges in size from 10 – 25 grams– Healthy function is necessary for successful fertilization.

The Abnormal Prostate Gland (pathology)
• What can go wrong with the prostate gland?– Postatitis– Benign Prostate Hyperplasia (BPH)– Prostate Cancer (ACP)
Anatomical Schematic

The Abnormal Prostate Gland: Prostate Cancer
• What can go wrong with the prostate gland?– Age dependant– Immortal “Clone” of malignant cells– Originates within the “peripheral zone”– Can “invade” and “metastasize”
Prostate cancer
Schematic

The Abnormal Prostate Gland: Prostate Cancer
• What can go wrong with the prostate gland?– ACP anatomical images

The Abnormal Prostate Gland: Prostate Cancer
• Local “invasion”• Prostatism (LUTS)• Bladder outlet obstruction• Hydronephrosis• Renal Insufficiency• Obstructive Renal Failure
The Abnormal Prostate Gland: Prostate Cancer
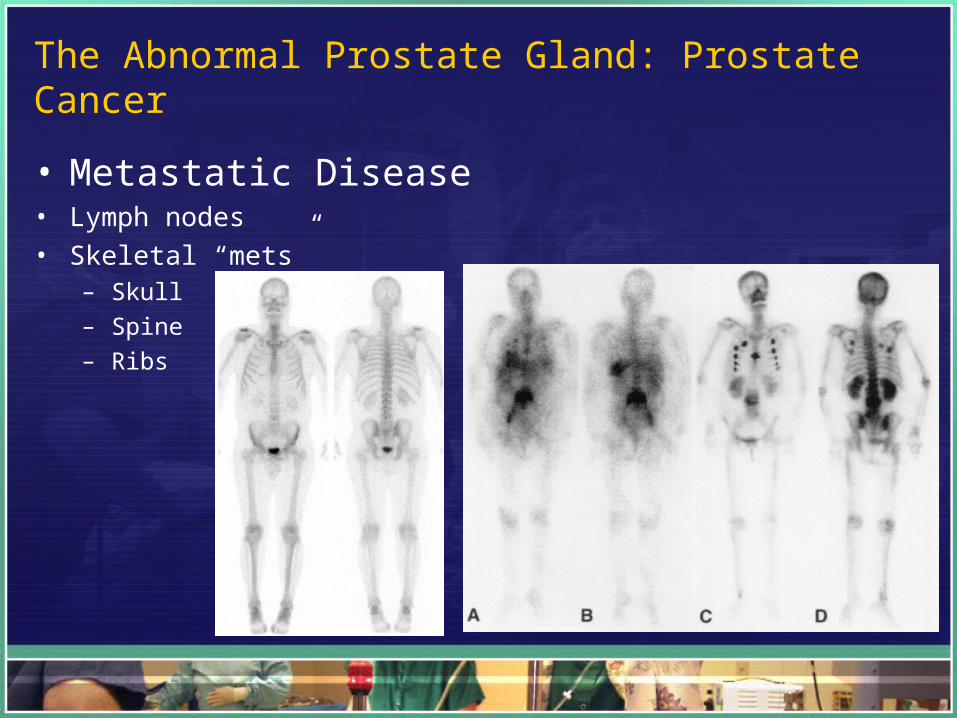
• Metastatic Disease• Lymph nodes• Skeletal “mets”
– Skull– Spine– Ribs

The Abnormal Prostate Gland: Prostate Cancer
• What can go wrong with the prostate?– ACP metastatic disease

The abnormal Prostate Gland: Prostate Cancer
• Incidence of prostate cancer by age:
0102030405060708090
10 20 30 40 50 60 70 80 90
Averagenumber ofcases per year(100's)
Average Number of new cases per yr UK – 2008 – 20102.
ACP is age dependent

Consider the Human Male: Historical PerspectiveEvolutionary considerations
• Primitive / Modern
Survive
Procreate
Evade predators / seat beltHunt wooly mammoth / jobFind suitable shelter / mortgage
Harem / Marriage

Consider the primitive Human Male:
• Primitive Man (3 million years)
– Life is tough• No running water / sanitation, unsatisfactory housing, inadequate
food, no textiles• Predators, microbial illnesses, viral illnesses, no vaccination
– Life is short• Life Expectancy at Birth (LEB) = early forties

Consider the modern Human Male:
• Modern Man ( 200,000 - 50,000 years)
– Life is good!• Lots of carbohydrates, protein, foods out of season• Better living conditions• Relative freedom from predators / pathogens
This happy Canadian fellow can expect to live to 80!

New Advancements in the Treatment of prostate Cancer
• “Rectangularization” of the survival curve
Survivors out of 100,000 born alive by age, Canada1
100
50
25
10 20 30 40 50 60 70 80 90
1981 -
1951 -
1921 -

New Advancements in the Treatment of prostate Cancer
• Primitive man VS Modern man
LEB = 40 years LEB = 80 years
Life has changed but procreation hasn’t

New Advancements in the Treatment of prostate Cancer
• Combination of age related incidence and growing life expectancy -

New Advancements in the Treatment of prostate Cancer
• “Traditional” Treatments for prostate cancer– Surgery– Irradiation (XRT / EBRT)– Hormonal manipulation (ADT)

New Advancements in the Treatment of prostate CancerTraditional Therapy
• Surgery– Radical Retropubic Prostatectomy (RRP)
Terence Millin (1940’s)– “Anatomical” RRP Patrick Walsh (1980’s)
“Bzzzzzzzz zzzzzzzz”

New Advancements in the Treatment of prostate CancerTraditional Therapy
Irradiation (XRT)
Radium (1920’s)X-ray therapy (1930’s)Cobalt 60 (1940’s - p)Linear accelerator (1950’s – p)“Brachy” therapy (1960’s - p)

New Advancements in the Treatment of prostate CancerTraditional Therapy
• Hormonal manipulation– Charles Huggins– Born Halifax, Nova Scotia, 1901– BA Acadia 1920– MD Harvard 1924– Surgery (Urology) Chicago 1930 – University of Chicago 1930 – 1969– Nobel prize medicine– Chancellor Acadia 1972 - 1979

New Advancements in the Treatment of prostate CancerTraditional Therapy
New Advancements in the Treatment of prostate Cancer
• Advanced prostate cancer– “Huggins operation” Bilateral orchiectomy (castration)– Delivers remission of 18 months – 5 yrs!– Estrogens (stilbestrol)– Progestins (AndrocurR)– LHRH agonist antagonists– “non” steroidal androgen antagonists
New Advancements in the Treatment of prostate Cancer
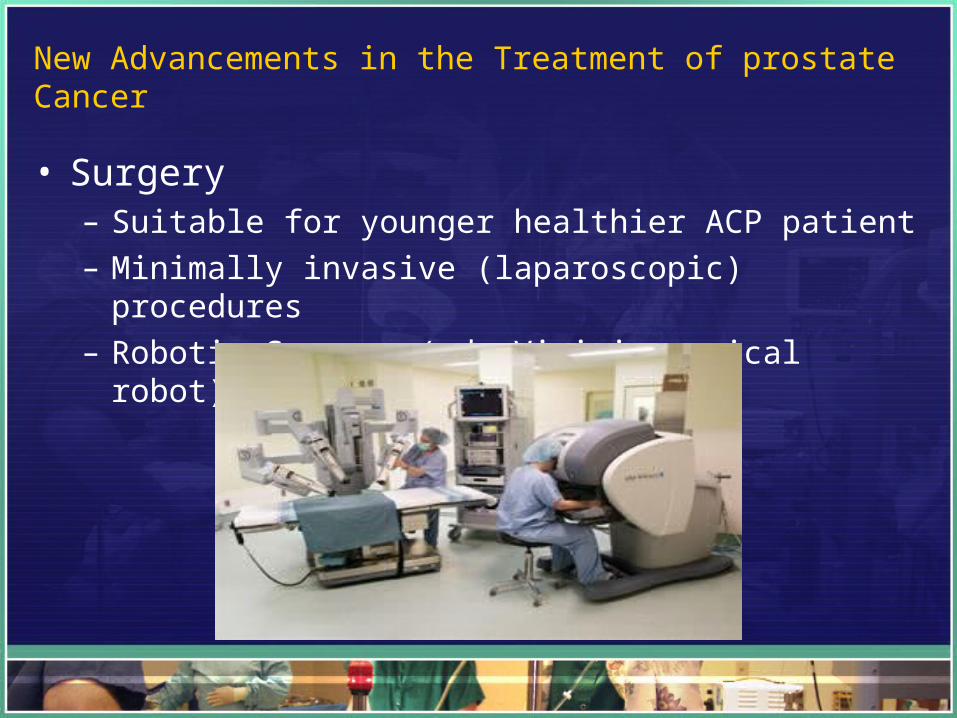
• Surgery– Suitable for younger healthier ACP patient– Minimally invasive (laparoscopic) procedures– Robotic Surgery ( da Vinici surgical robot)

New Advancements in the Treatment of prostate Cancer
• Irradiation– Brachytherapy
• 1960’s Au 98 (98Au)• 1990’s Iridium 192 (192Ir)• 2000’s Iodine 125 (125I)• High Intensity Focused Ultrasound (HIFU)
– Proton Therapy• Particle accelerator• Increased Dose intensity• Improved precision

New Advancements in the Treatment of prostate Cancer
• Hormonal Manipulation – Huggins operation– Estrogens– Progestins– LHrH’s– Non-steroidal agents
– Intracellular ADT therapy• Abiraterone (ZytingaR)• Enzalutamide (XtandiR)
abiraterone
“Abiraterone targets testosterone receptor inside the cell”

New Advancements in the Treatment of prostate Cancer
• Intra-cellular anti-androgens– Enzalutamide
• Reduces PSA by on average 89%• Extended survival by on average 5 months• Relatively non-toxic• FDA stopped trials in November 2011 – rushed to market
New Advancements in the Treatment of prostate Cancer
• RIH department of surgery– Established 1905– All major specialties represented– Major cases undertaken everyday – 24 / 7 / 365 coverage– Current OR completed 1962





















