Embed Size (px)
Citation preview


How Old is HBV?
• HBV associated with humans for >1,000 years but no definitive evidence
• Recent evidence establishes ≥500 years
• Naturally mummified body of a Korean child found virtually intact
• Laparoscopy: Large organ in RUQ and biopsies sent for pathology and HBV DNA testing
– HBV DNA genotype C isolated from the liver
– Pathology: Appeared to be normal liver
Klein A, et al. 58th AASLD; Boston, MA; November 2-6, 2007. Poster 925.

Viral Characteristics
HIV HBV HCV
Virus type RNA Retrovirus DNA Hepadenovirus RNA Flavivirus
Eradication possible with therapy? No—Latent reservoirs No-cccDNA
Yes—Sustained virologic response (cure)
Viral targets Mainly CD4+ cells Hepatocytes Hepatocytes
Variants HIV 1 and 2 8 genotypes A-H 6 genotypes 1-6
Pathogenesis Damage to host immune system
Host immune response
Host immune response
Hepatitis B is 50 to 100 times more infectious than HIVUnlike HIV, it can live outside the body in dried blood for longer than a week
World Health Organization. Hepatitis B. http://www.who.int/mediacentre/factsheets/fs204/en/. Accessed November 7, 2007; Block TM, et al. Clin Liver Dis. 2007;11:685-706; Krogstad P. Semin Pediatr Infect Dis. 2003;14:258-268;
Penin F. Clin Liver Dis. 2003;7:1-21; Lauer GM, Walker BD. N Engl J Med. 2001;345:41-52.
World Health Organization. Hepatitis B. http://www.who.int/mediacentre/factsheets/fs204/en/. Accessed November 7, 2007; Block TM, et al. Clin Liver Dis. 2007;11:685-706; Krogstad P. Semin Pediatr Infect Dis. 2003;14:258-268;
Penin F. Clin Liver Dis. 2003;7:1-21; Lauer GM, Walker BD. N Engl J Med. 2001;345:41-52.

Nucleoside Analogues in HBV
HBV- Global health problem 250m people worldwideMax prevalence in Asia Pacific and Subsaharan
AfricaHBV: Vaccination : 179 countries
Chronic carriers at risk

Normal Aminotransferase Levels and Risk of Mortality from Liver Diseases
Kim HC et al. Kim HC et al. BMJBMJ 2004; 328:983 2004; 328:983
1.01.0
2.92.9
9.59.5
19.219.2
30.030.0
59.059.0
NormalNormal
ElevatedElevated
Korea Medical Insurance Corporation 94,533 men; 47,522 women
35-59 yrs old Relative risk for liver mortality compared with AST and ALT <20 IU/l

7 Taiwanese townships aged 30–65 years
(n=89,293)
Baseline HBsAg+(n=9800)
Baseline HBV DNA(n=3851)
Follow-up analysisfor cirrhosis/HCC
(n=3774)
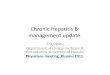
Viral Load Predicts Disease Progression:The REVEAL Study
Risk Evaluation of Viremia Elevation & Associated Liver Disease
Prospective, multicenter, observational cohort study
Chen CJ. JAMA. 2006;295:65-73.
1991-19921991-1992RecruitmentRecruitment
June 2004: June 2004: 43,993 PYs follow-up43,993 PYs follow-up
• 24% PCR neg
• 85% HBeAg(-)
• 94% ALT<45 IU/L
• 98% non-cirrhotic (on Ultrasound)


00.0
0.1
0.2
0.3
0.4
0.5
0.6
1 2 3 4 5 6 7 8 9 10Year of follow-up
Cum
ulati
ve H
azar
d of
Liv
er
Dis
ease
HBeAg(+) HBV DNA ≥104
HBeAg(-) HBV DNA ≥104
HBeAg(-) HBV DNA <104
Progression from Chronic Hepatitis to Cirrhosis with normal ALT
Chen JD, et al. 43rd EASL; Milan, Italy; April 23-27, 2008. Abstract 644.

Chronic HBV
• Primary aim of treatment : progression of disease progression to cirrhosis, decompensation and HCC
• HBV DNA: Strongest predictor of HCCReveal study
Hongkong study: 8 yrs follow up
HCC risk calculators

GuidelineHBeAg + HBeAg-
HBV DNA
copies/mL
ALT
U/L
HBV DNA
copies/mL
ALT
U/L
US Algorithm 2008* ≥105>ULN or
(+) biopsy≥104
>ULN or
(+) biopsy
EASL 2008/9 ≥104 > ULN ≥104 > ULN
APASL 2008 ≥105 >2x ULN ≥105 >2x ULN
AASLD 2007/9 ≥105>2x ULN or
(+) biopsy≥105
>2x ULN or
(+) biopsy
Treatment Criteria for Chronic Hepatitis B

Chronic HBV Treatment:Simplified Flow Chart
Keeffe EB, et al. Clin Gastroenterol Hepatol. 2006;4:936-962.
HBeAg Positive
Treat
Monitor
HBeAg Negative
HBV DNA >20,000 IU/mL HBV DNA >2,000 IU/mL
Normal ALT
Liver Biopsy
Abnormal Histology
Elevated ALT
ALT Evaluation
IU/mL to copies/mL conversion: Versant HBV DNA 3.0 (bDNA): 1 IU/mL=5.2 copies/mL. Cobas Amplicor HBV monitor: 1 IU/mL=5.6 copies/mL.
Cobas TaqMman 48 HBV: 1 IU/mL=5.8 copies/mL.

Indications of treatment
• Moderate to severe liver disease- h/p ALT/HBV DNA levels
• AASLD/ EASL/APASL guidelines• But
• Advanced age,• Extrahepatic manifestations,• Family history of cirrhosis• HBV treatment with help of biomarkers• Fiborscan

Antiviral agents
1982
HBV Vaccine
1985
INF
2005
Peg INF
Enticavir
2006
Telbivudine
2008
Tenofovir

Oral Drugs with Anti-HBV Activity - 2015
Nucleoside Analogs: Lamivudine
EntecavirTelbivudineEmtricitabine
Nucleotide Analogs Adefovir DipivoxilTenofovir Disoproxil
‡

First Line Treatment Options Have The Lowest Resistance Rates
Lowest Rate of
Resistance
Lamivudine 65% to 70% at 4 to 5 years
Telbivudine 25% in HBeAg-positive patients11% in HBeAg-negative patients
at 2 years
Adefovir dipivoxil29% at 5 years
Entecavir*in the absence of prior lamivudine resistance
(1.25% at 5 years)
*Patients with LAM resistance have a 51% rate of novel mutations after 5 years of entecavir therapy
Tenofovir DFin treatment
naïve patients (0% at 2 years)
Highest Rate of
Resistance
US Treatment Algorithm – Resistance Profile
Keeffe, E, et al. Clinical Gastroenterology and Hepatology 2008;doi: 10.1016/j.cgh.2008.08.021 (e-pub).


New Preferred First-Line Treatment Options
• Based on superior efficacy, tolerability, and favorable resistance, the new preferred Oral first-line treatments are: – Tenofovir DF*
– Entecavir
US Treatment Algorithm and EASL Guidelines - Treatment Options
+Tenofovir DF should replace adefovir dipivoxil as a first-line drug in previously untreated patients with HBeAg-positive and HBeAg -negative disease
Keeffe, E, et al. Clinical Gastroenterology and Hepatology 2008;doi: 10.1016/j.cgh.2008.08.021 (e-pub).EASL Clinical Practice Guidelines (update, in press); access: www.easl.ch/PDF/cpg/EASL_HBV_CPGs.pdf, 11.14.08

Mechanisms of action of NUCS
• Suppress HBV DNA by targeting the HBV DNA polymerase (a reverse transcriptase) and thus intervene the replication of HBV DNA


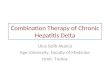
0102030405060708090
PEG-INF LAM ADV ETV LdT TDF
Rates of Undetectable HBV DNA and Normal ALT in HBeAg+ Patients
0
1020
30
40
5060
70
80
PEG-INF LAM ADV ETV LdT TDF
24%
39%
21%
67%60%
74%
39%
66%
48%
68% 69%77%
Undetectable HBV DNA Normal Range ALT
Rates of undetectable HBV DNA and normal range ALT at one year of therapy with:pegylated interferon alpha 21 (PEG_INF), lamivudine (LAM), adefovir (ADV), entecavir (ETV),
and tenofovir DF (TDF) in HBeAg positive patients with CHB in randomized clinical trails. These trials used different HBV DNA assays and they were not head-to-head comparisons for all the drugs.
EASL Clinical Practice Guidelines (update, in press); access: www.easl.ch/PDF/cpg/EASL_HBV_CPGs.pdf, 11.14.08

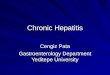
Rates of Undetectable HBV DNA and Normal ALT in HBeAg– Patients
0
20
40
60
80
100
PEG-INF LAM ADV ETV LdT TDF0
102030405060708090
PEG-INF LAM ADV ETV LdT TDF
63%72%
51%
90% 88% 91%
38%
74% 72%78%
74% 77%
Undetectable HBV DNA Normal Range ALT
Rates of undetectable HBV DNA and normal range ALT at one year of therapy with:pegylated interferon alpha 21 (PEG_INF), lamivudine (LAM), adefovir (ADV), entecavir (ETV),
and tenofovir DF (TDF) in HBeAg negative patients with CHB in randomized clinical trails. These trials used different HBV DNA assays and they were not head-to-head comparisons for all the drugs.
EASL Clinical Practice Guidelines (update, in press); access: www.easl.ch/PDF/cpg/EASL_HBV_CPGs.pdf, 11.14.08


Summary: AASLD Guidelines for Management of Antiviral-Resistant HBV
Resistance Rescue Therapy
LamivudineTelbivudine
Add adefovir or tenofovir DFSwitch to: Emtricitabine + tenofovir DF (fixed-dose combination) Entecavir (risk of entecavir resistance)
Adefovir Add lamivudineSwitch to: Emtricitabine + tenofovir DF (fixed-dose combination) Entecavir (if no prior lamivudine resistance)
Entecavir Add adefovir or tenofovir DF
Multidrug Multidrug resistance to lamivudine + adefovir: Consider emtricitabine + tenofovir DF (fixed-dose combination), tenofovir DF, entecavirMultidrug resistance to lamivudine + entecavir: Consider tenofovir DF or emtricitabine + tenofovir DF (fixed-dose combination)
Lok AS, et al. Hepatology. 2007;46:254-265.

Durability of response
LAM: HBeAg –VE : 50% relapse with 6m of cessation of treatment
ADV: 46% relapse with 5 years
ETV : 29% to 53% after cessation of treatment
50% - sustained HBeAg seroconversion off treatment

Role of quantitative HBsAg
• HBsAg quantitative correlates with CCC DNA only in HBeAg +ve patients and not in HBeAg –ve patients
• True inactive carriers HBV DNA <2000IU/ml with HBsAg quantitative <1000IU/ml
• HBeAg –ve patient HBV DNA 2000 IU/ml and HBsAg <100 IU/ml.
• Good chance of spontaneous clearance

GS-103: HBsAg Loss/seroconversion Occurred only in HBV Genotypes A + D
• At week 48, HBsAg loss occurred in 3.2% with TDF and 0% with ADV (p=0.02)
• 14 patients (6%) lost HBsAg by year 2 on TDF– 9 TDF-TDF and 5 ADV-TDF– 11/14 HBsAb seroconversion
• TDF induced loss of HBsAg in Caucasian patients infected with genotype A or D virus
GenotypeHBsAg Clearance at
Year 2 n/N (%)
A 8/67 (12%)
B 0/35 (0%)
C 0/69 (0%)
D 6/90 (7%)
Heathcote EJ, et al. 44th EASL; Copenhagen, Denmark; April 22-26, 2009; Abst. 909.

Impact of HBV Genotype on treatment response
• No relation with HBeAg seroconversion or HBV DNA decline respond.

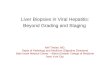
Oral Antivirals Reduce the Incidence of HCC in Patients with HBV-related Liver Cirrhosis
Eun, J. et al, AASLD 2007, Abstract #961.
Control, n=111
Treated, n=111
Mean follow-up 4.4 for treated, 5.4 for untreated
Annual incidence rate of 1.02% Tx. vs. 6.0% non-Tx. patients/year
* (Log-rank, p=0.003)
5%*
33%

Impact of NA treatment on HCC
• Well documented for LAM /ADV only
• Prospective study: LAM vs Placebo 651 CHB patients
• Results 3.9% Vs 74% (LJAM etal. NEJM 2004)
• Enticavir/ TDF: Regression of fiborsis/ cirrhosis/ documented ? HCC reduction

Impact of NA treatment on hepatic decompensation
Lam : 32M : 50% reduction in rate of hepatic decompensation
A significant proportion of patients taken off OLT list

NA treatment after LT
• Entecavir monotherapy 91% HBsAg loss
98.8% undetectable HBV DNA after LT after a mean follow up of 53 months
Fung et al AJ Gastroentrol 2013

NA on Immunosuppresed State and Immune restoration
• Reactivation of HBV replication and decompensation reported in 20-50% of CHB patients
• Poor outcome on those with high viral load and underlying established cirrhosis

Pregnancy Category
Tenofovir DF Category B
Telbivudine Category B
Lamivudine Category C
Entecavir Category C
Adefovir Category C
• There is a considerable body of safety data in pregnant HIV-positive women who have received TDF and/or LAM or FTC
US Treatment Algorithm and EASL Guidelines - Treatment Options
Keeffe, E, et al. Clinical Gastroenterology and Hepatology 2008;doi: 10.1016/j.cgh.2008.08.021 (e-pub).EASL Clinical Practice Guidelines (update, in press); access: www.easl.ch/PDF/cpg/EASL_HBV_CPGs.pdf, 11.14.08

Strategies to improve treatment efficacy – Denovo combination treatment
• TDF + ETV better than either along if HBVDNA > 108 IU/ml in HBeAg +ve patients
Lok AS(Gastroenterol 2012)
• Road Map therapy -only for TDV patients

NEWER NAS
• Prodrug of Tenofovir better lymphoid distribution
• Lesser renal and bone toxicities
• Besifovir : Acyclic nucleotide phosphonate : as good as ETV/ TDF
Tenofovir Alafenamide 25mg

Future NA development
• Viral entry inhibitors• Acylated peptides derived from the large HBV
envelop protein block viral entry• Use preS1 peptides• Small interfering RNA produce strong and
persistent antiHBV activity• Block interaction between HBeAg and HBsAg• Some HBV Gerome Oligonuclitides induce Robust
expression of INF by plasmocytosed cells.

Conclusion
• NAS- New era of HBV treatment• Reduce hepatic decompensation and HCC• Infrequent side effects/ ease administration• 1st Generation : Viral resistance• 2nd Generation: ETV : 1.2% ( 5 years)
TDF: 0% ( 6 years)• Combination treatment for HBV DNA>10 8 log• ? What to do for suboptimal responders• ?RGT

Future Perspectives
• Indefinite treatment : major drawback
• ? Peg INF + TDF – RCT on
• ? Peg INF after HBeAg seroconversion
• Tenofovir Alafenamide, Besifovir : Newer NAS/entry inhibitors/smrnas

39
HBsAg