Embed Size (px)
DESCRIPTION
Citation preview

ObesityObesity
Dr Aftab AsifAssociate Professor
Psychiatry Dept Fatima Jinnah Medical College Sir Ganga Ram Hospital Lahore
Obesity DefinitionObesity Definition
bull A condition in which excessive body fat may put a person at health risk
bull A metabolic disorder that is primarily induced and sustained by an over consumption or underutilization of caloric substrate
Storage of fat Storage of fat
bull Fat is stored as triglycrides in adipose tissues and the distributed mainly under skin inndash Abdomenndash Breastndash Buttocksndash Thighs
Obesity measureament toolsObesity measureament tools
bull Ideal body wt (IBW)
bull Body mass index (BMI)ndash weight in Kg height (m) 2
Obesity ClassificationObesity ClassificationStandards (BMI)
Research
Under weight
lt 20 lt 185
Normal 20 ndash 25 185 ndash 275
Over weight 25 ndash 30 275 ndash 30
Obese 30 ndash 40 gt 30
Severely obese
gt 40
bull Moderate obesity ndash Associated with
increase in cell size
bull Sever obesityndash Associated with
increase in no of fat cells
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
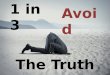
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
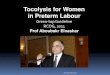
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Obesity DefinitionObesity Definition
bull A condition in which excessive body fat may put a person at health risk
bull A metabolic disorder that is primarily induced and sustained by an over consumption or underutilization of caloric substrate
Storage of fat Storage of fat
bull Fat is stored as triglycrides in adipose tissues and the distributed mainly under skin inndash Abdomenndash Breastndash Buttocksndash Thighs
Obesity measureament toolsObesity measureament tools
bull Ideal body wt (IBW)
bull Body mass index (BMI)ndash weight in Kg height (m) 2
Obesity ClassificationObesity ClassificationStandards (BMI)
Research
Under weight
lt 20 lt 185
Normal 20 ndash 25 185 ndash 275
Over weight 25 ndash 30 275 ndash 30
Obese 30 ndash 40 gt 30
Severely obese
gt 40
bull Moderate obesity ndash Associated with
increase in cell size
bull Sever obesityndash Associated with
increase in no of fat cells
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Storage of fat Storage of fat
bull Fat is stored as triglycrides in adipose tissues and the distributed mainly under skin inndash Abdomenndash Breastndash Buttocksndash Thighs
Obesity measureament toolsObesity measureament tools
bull Ideal body wt (IBW)
bull Body mass index (BMI)ndash weight in Kg height (m) 2
Obesity ClassificationObesity ClassificationStandards (BMI)
Research
Under weight
lt 20 lt 185
Normal 20 ndash 25 185 ndash 275
Over weight 25 ndash 30 275 ndash 30
Obese 30 ndash 40 gt 30
Severely obese
gt 40
bull Moderate obesity ndash Associated with
increase in cell size
bull Sever obesityndash Associated with
increase in no of fat cells
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Obesity measureament toolsObesity measureament tools
bull Ideal body wt (IBW)
bull Body mass index (BMI)ndash weight in Kg height (m) 2
Obesity ClassificationObesity ClassificationStandards (BMI)
Research
Under weight
lt 20 lt 185
Normal 20 ndash 25 185 ndash 275
Over weight 25 ndash 30 275 ndash 30
Obese 30 ndash 40 gt 30
Severely obese
gt 40
bull Moderate obesity ndash Associated with
increase in cell size
bull Sever obesityndash Associated with
increase in no of fat cells
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Obesity ClassificationObesity ClassificationStandards (BMI)
Research
Under weight
lt 20 lt 185
Normal 20 ndash 25 185 ndash 275
Over weight 25 ndash 30 275 ndash 30
Obese 30 ndash 40 gt 30
Severely obese
gt 40
bull Moderate obesity ndash Associated with
increase in cell size
bull Sever obesityndash Associated with
increase in no of fat cells
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

bull Moderate obesity ndash Associated with
increase in cell size
bull Sever obesityndash Associated with
increase in no of fat cells
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Obesity Trends Among Obesity Trends Among US AdultsUS AdultsObesity BMI ge30 kgm2 or ~ ge14 kg overweight for 163 cm person
1998
No Data lt10 10ndash14 15ndash19 ge20
2000
No Data lt10 10ndash14 15ndash19 ge20
2002
No Data lt10 10ndash14 15ndash19 20ndash24 ge25No Data lt10 10ndash14 15ndash19 20ndash24 ge25
2004
Data from CDC Behavioral Risk Factor Surveillance System
Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Causes of ObesityCauses of Obesity
Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Causes of ObesityCauses of Obesity
bull Complex and multifactorialndash Genetic predispositionndash Endocrine disordersndash Socializationndash Agendash Sexndash Race
ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

ndash Economic statusndash Psychologicalndash Culturalndash Emotionalndash Environmental factorsndash Cessation of smoking
Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Genetic PredispositionGenetic Predisposition
offspring chanceof being obese
80
150
1020304050607080
2 obeseparents
2 normalparents
Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Multi-Hormonal Control of Body WeightMulti-Hormonal Control of Body WeightRole Of Fat- Gut- And Islet-derived SignalsRole Of Fat- Gut- And Islet-derived Signals
Amylin
GI tractAdipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman MK and Flier JS Science 2005 307 1909-1914
LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

LeptinLeptin
bull Released from fat tissues bull Interact with
ndash Hypothalamusndash Adipose tissue
bull Inhibits neuropeptide Y and Aguoti-related peptide (AGRP) in CNS
bull Binds to central melanocortin receptorsbull Decreases food intakebull Increases energy expenditure
How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

How leptin causes obesityHow leptin causes obesity
bull Primary decrease of leptin (low leptin)bull Leptin receptor resistance (high leptin)
bull So increase neuropeptide Y and AGRP increase in food intake and low energy expenditure sever obesity
InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

InsulinInsulin
uarr Insulin inhibit Hormone Sensitive lipase (HSL)
Dec break down of fat uarr body fat
Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Insulin Insulin
uarr insulin stimulation of lipoprotien lipase uarr storage of triglycrides in fat cells uarr total body fat
Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Which fat depletes more Which fat depletes more abdominal or glutealabdominal or gluteal
bull Abdominal (hyperplastic adipose tissue )
Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Which fat depletion site causes Which fat depletion site causes metabolic abnormalitiesmetabolic abnormalities
bull Abdominal
bull Responding to hypocaloric dite more and cause metabolic abnormalities
Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Feeding centerFeeding center
bull Hypothalamusndash Ventromedial hypothalamus (inhibits feeding)ndash Lateral hypothalamus (stimulates feeding)
bull Oraxin hyperphagiandash Arcuate nucleus neuropeptide Y (increses
appitite)
Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Diseases Linked to ObesityDiseases Linked to Obesity
bull Diabetesbull Coronary Heart
Diseasebull High Blood Pressurebull Strokebull Arthritis
bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

bull Gastroesophageal refluxbull Cancerbull High cholesterolbull Endocrine disease
bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

bull Hypertrophic Cardiomyopathybull Infertilitybull Depressionbull Obstructive sleep apneabull Gallstonesbull Fatty liverbull Stress incontinencebull Venous ulcersbull Sudden death
What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

What About the Role of SerotoninWhat About the Role of Serotonin
bull Theory that low serotonin levels leads to ldquocarbohydrate cravingrdquo and plays a major role in the development of obesity
Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Psychological ComplicationsPsychological Complicationsof Obesityof Obesity
bull Emotional distress
bull Discrimination
bull Social stigmatization
Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Cardiovascular Cardiovascular PathophysiologyPathophysiology
bull Excess body massndash uarr metabolic demand rarr uarr CO2
bull uarr workloadbull LVH (left ventricular hypertrophy)bull uarr pulmonary blood flow
ndash Pulmonary HTN rarr cor pulmonale rarr right heart failure
Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Volume ReplacementVolume Replacement
bull Adult total body water percentage is 60 to 65
bull Severely obese total body water is 40
bull Estimated blood volume in obese patient is 45 to 55 mLkg ndash 70 mLkg for the non-obese
Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Selected Medications That Can Selected Medications That Can Cause Weight GainCause Weight Gain
bull Psychotropic medications
ndash Tricyclic antidepressants
ndash Monoamine oxidase inhibitors
ndash Specific SSRIs
ndash Atypical antipsychotics
ndash Lithium
ndash Specific anticonvulsants
-adrenergic receptor blockers
SSRI=selective serotonin reuptake inhibitor
Diabetes medicationsndash Insulinndash Sulfonylureas (glipizide
glucotrol)ndash Thiazolidinediones
(pioglitazone )
Tamoxifen (anti-estrogen)
Steroid hormonesndash Glucocorticoids
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Calories chartCalories chart
Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Calories chartCalories chart
Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Calories chartCalories chart
TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

TreatmentTreatment
Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Aim of treatmentAim of treatment
To achieve a modest weight loss that is also maintained long term
Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Impact of Weight Loss Impact of Weight Loss
~5Weight Loss
5-10Weight Loss
HbA1c
Blood Pressure
Total Cholesterol
HDL Cholesterol
Triglycerides
1 Wing RR et al Arch Intern Med 19871471749-17532 Mertens IL Van Gaal LF Obes Res 20008270-2783 Blackburn G Obes Res 19953 (Suppl 2)211S-216S4 Ditschunheit HH et al Eur J Clin Nutr 200256264-270
1
2
3
3
1
2
3
3
4
Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Obesity Treatment PyramidObesity Treatment Pyramid
DietDiet Physical ActivityPhysical Activity
Lifestyle ModificationLifestyle Modification
PharmacotherapyPharmacotherapy
SurgerySurgery
Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Guide for Selecting Obesity TreatmentGuide for Selecting Obesity Treatment
The Practical Guide Identification Evaluation and Treatment of Overweight and Obesity in Adults October 2000 NIH Pub No00-4084
Treatment 25-269 27-299 30-349 35-399 gt40
Diet Exercise Behavior Tx
+ + + + +
Pharmaco-therapy
With co-morbidities + + +
Surgery With co-morbidities +
BMI Category (kgmBMI Category (kgm22))
Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Treatment of ObesityTreatment of Obesitybull Goal of treatment 10 weight lossbull Caloric restriction -500 kcaldaybull Moderate physical activity
ndash 30 minutes dailybull Behavioral modificationbull Drug therapy
National Institutes of Health Obes Res 1998 6 (suppl 2) 51Sndash209S
DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

DietDiet
bull Reduce fatty dietsbull Increase fiber dietbull Take calories according to requirements(1000 to 1500 Kcal)bull Stop bing eating
ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

ExerciseExercise
bull Take 30 min daily for physical activity
Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Benefits of Physical Activity forBenefits of Physical Activity forHealth and Weight ControlHealth and Weight Control
bull 1048708 Improves cardiovascular health independent of weight loss
bull 1048708 Improves mood and energy level
bull 1048708 Increase weight loss compared with diet alone
bull 1048708 Spares loss of fat-free mass during weight loss
Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Behavior TherapyBehavior Therapy
Eating and physical activity patterns are learned behaviors and can be modified
bull 1048708 Behavior Modification Techniquesndash 1048708 Self Monitoringndash 1048708 Stimulus Controlndash 1048708 Behavioral Contractingndash 1048708 Cognitive Restructuringndash 1048708 Stress Managementndash 1048708 Relapse Preventionndash 1048708 Social Support
bull Hyder et al Behavior Modification in the treatment of Obesity Practical Approaches for Family Physicians Clinics in Family Practice June 20022
Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Drug treatment inDrug treatment inadultsadults
bull Record initial weight
bull Discuss decision to start drug treatment choice potential benefit and limitations adverse effect and monitoring requirement with patient
bull Review regularly to monitor compliance effectiveness adverse effect
bull Reinforce lifestyle advice
The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

The Regulation of Prescription The Regulation of Prescription Weight-Loss Drugs Weight-Loss Drugs
bull Part I 1947 to 1973Approval of the amphetamines and the amphetamine
congeners
bull Part II 1974 to 1995Short-term treatment
bull Part III 1996 to presentLong-term treatment
Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Drugs Approved by FDA for Drugs Approved by FDA for Treating ObesityTreating Obesity
Generic NameTrade Names
Approved Use
Year Approved
Orlistat Xenical Long-term 1999
Sibutramine Reductil Meridia Long-term 1997
Diethylpropion Tenulate Short-term 1973
Phentermine Adipex lonamin Short-term 1973
Phendimetrazine Bontril Prelu-2 Short-term 1961
Benzphetamine Didrex Short-term 1960
Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Anti-obesity drugsAnti-obesity drugsDrug name Orlistat Sibutramine
Brand name Xenical Reductil trim fast
Primary indication Obesity Obesity
Use Long-term Long-term
Mechanism of action GI lipase inhibitor CNS monoamine reuptake inhibitor
Dosing 120 mg TID 5-15 mg OD
Side Effects Steatorrhea Insomnia
Oily spottingIncontinence
Dry mouthIncreased BP
SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

SURGICAL THERAPY SURGICAL THERAPY
bull Only Recommended in Selected Adult Patients
BMI gt 40 or with Co-morbid
Conditions
bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

bull Liposuction
bull Abdomeno plasty
bull Restrictive bariatric proceduresndash Bandingndash Stapling
Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Roux-en-Y GBPRoux-en-Y GBP
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Adjustable gastric bandingAdjustable gastric banding
Current Status of Medical and Surgical Therapy for ObesityCurrent Status of Medical and Surgical Therapy for ObesityGastroenterology Vol120 No3Gastroenterology Vol120 No3
Restrictive bariatric procedures
ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

ConclusionConclusionbull Lifestyle changes such as diet and exercise are still the
mainstay of obesity management
bull Aim of treatment should be modest weight loss maintained in the long term
bull Add anti-obesity drugs only if above fails
bull Consider the risk vs benefit of prescribing these drugs
Thank youThank you

Thank youThank you