Embed Size (px)
Citation preview
OCD in pregnant and postpartum women
Mohamed sedky
Psychiatric specialistQMHH
May 2015
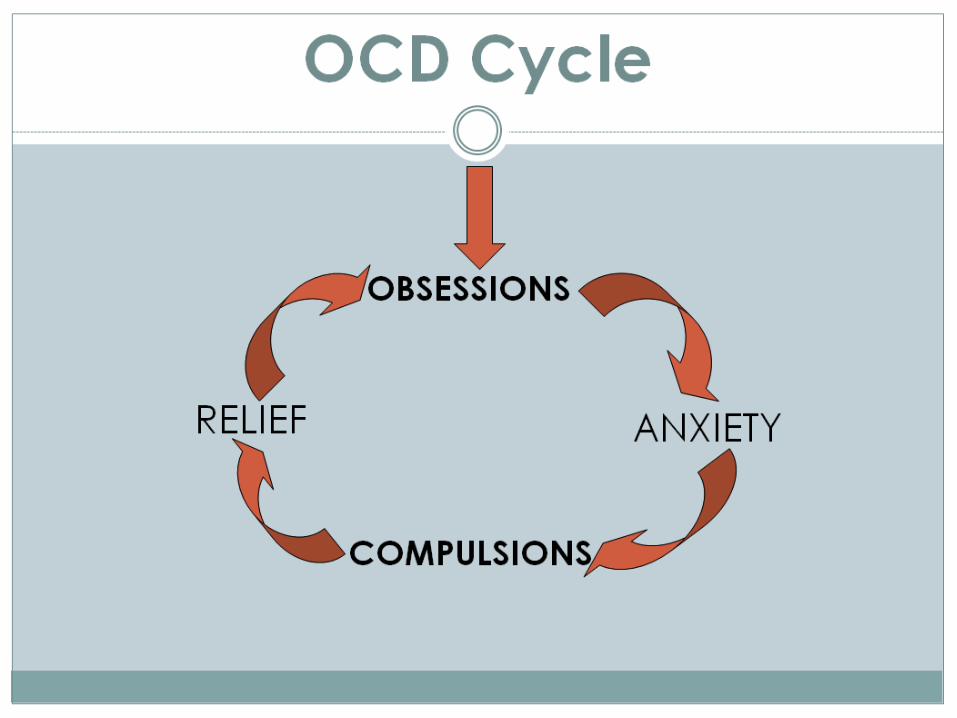
Obsessive Compulsive Disorder (OCD)
OCD is characterized by intrusive, troubling thoughts (obsessions), and repetitive, ritualistic behaviours (compulsions) which are time consuming, significantly impair functioning and cause distress.
Obsessions
Recurrent and persistent thoughts, impulses, or images that are experienced, at some time during the disturbance, as intrusive and inappropriate and that cause marked anxiety or distress.
They are not simply excessive worries about real life problems.
The person attempts to ignore or suppress them, or to neutralize them with some other thought or action.
The person recognizes that the obsessive thoughts, impulses, or images are a product of his or her own mind (not imposed from outside).
Common Obsessions in OCD
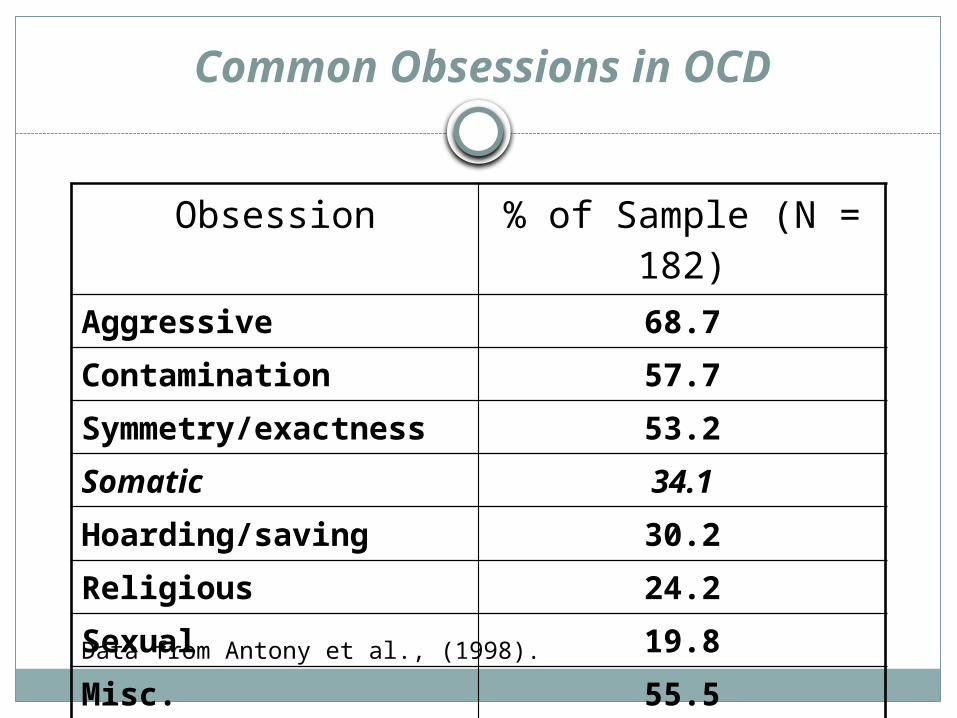
Obsession % of Sample (N = 182)Aggressive 68.7
Contamination 57.7
Symmetry/exactness 53.2
Somatic 34.1
Hoarding/saving 30.2
Religious 24.2
Sexual 19.8
Misc. 55.5
Data from Antony et al., (1998).
Compulsions
Repetitive behaviors that the person feels driven to perform in response to an obsession, according to rules that must be applied rigidly.
Aimed at reducing distress or preventing some dreaded event or situation; however, these behaviors or mental acts either are not connected in a realistic way with the obsession or are clearly excessive.
Common Compulsions in OCD
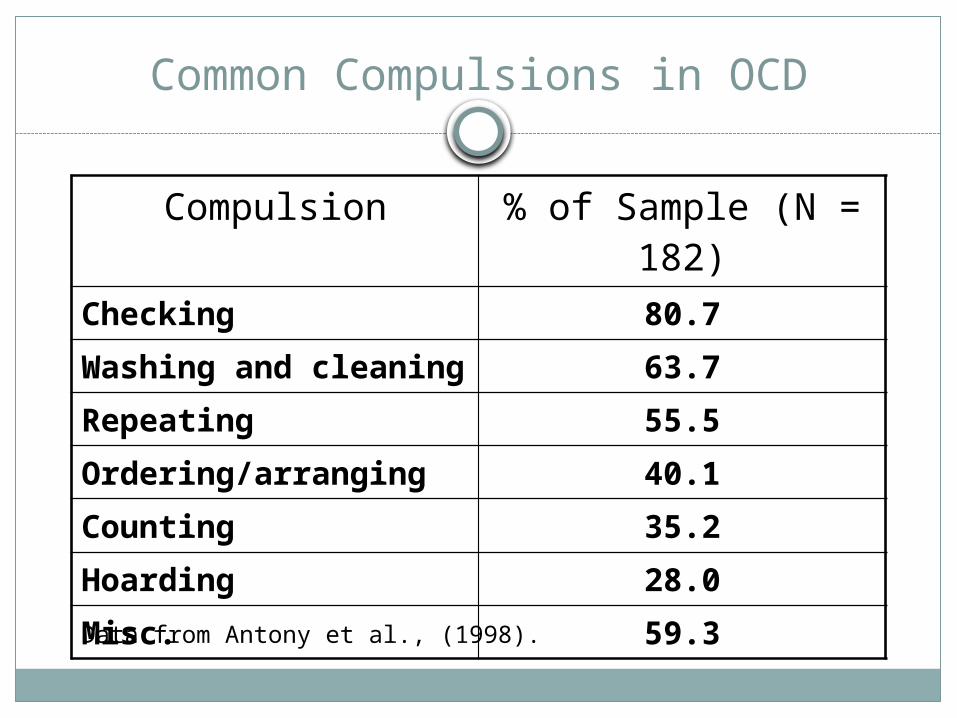
Compulsion % of Sample (N = 182)
Checking 80.7
Washing and cleaning 63.7
Repeating 55.5
Ordering/arranging 40.1
Counting 35.2
Hoarding 28.0
Misc. 59.3
Data from Antony et al., (1998).
prognosis
OCD is an often-disabling illness that is frequently difficult to treat.
30% show significant improvement 40% show moderate improvement 30% show no improvement.
OCD during pregnancy and postpartum
While the significance of depression and psychosis during pregnancy or postpartum have been widely recognized, OCD has not received as much attention.
OCD may also occur during these periods and poses unique clinical challenges: May affect the bond between mother and her infant. OCD is often a very comorbid disorder with depression, being usually
OCD the antecedent. Mothers with obsessions related to their children (e.g., aggressive
intrusions) usually hide or minimize these symptoms for fear of being stigmatized, which results in less treatment demands (underdiagnosis), and in a higher risk for the disorder to become chronic.
Epidemiology
There are several case reports showing that pregnancy and postpartum period are associated with the onset of OCD more frequently than other life events.
prevalence of OCD in the general population 1.08 % in pregnant women 2.07 % in postpartum women 2.43 %
Incidence of OCD in pregnant women 2.1-13.7% in postpartum women 2.3-15.2%
Epidemiology
Also, the perinatal period is a stage that increases the risk of exacerbation preexisting of OCD, particularly in the puerperium.
exacerbation of OCD in pregnant women 8 - 34.1% in postpartum women 29 - 50%
Pathogenesis
OCD is a brain-based neurobiological disorder, but more specific knowledge about its etiology is limited.
Theories of Pathogenesis include: The Neuroendocrine theory The sociobiological theory The Cognitive-behavioural model
Pathogenesis
Neuroendocrine theory:A serotonergic dysregulation is postulated due to
fluctuations in female gonadal steroids during the perinatal period.
fluctuations in estrogen and progesterone
Serotonin dysregulation
OCD symptoms
Pathogenesis
The sociobiological theory:Maintains that the genesis of perinatal OCD lies in a
greater reactivity or dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis as a response to stressful life events.
Stressful life events
HPA dysregulation
OCD symptoms
Pathogenesis
Cognitive-behavioural model: the presence of intrusive thoughts during pregnancy and puerperium is a
relatively common phenomenon, with 49-69% of women being affected in the perinatal period.
The role of hyper-responsibility and overestimation of threat or danger is highlighted as intrapsychic factors that contribute to an inappropriate interpretation of normative intrusions in people exposed to a new life event as parenthood.
hyper-responsibility
inappropriate interpretation of normative intrusions
OCD symptoms
Risk Factors
Risk factors associated with pregnancy onset OCD: Primiparity Second or third trimester of gestation Number of gestations and live birth Miscarriage Gestational complication Positive family history of OCD
Risk Factors
Risk factors associated with postpartum onset OCD: Primiparity (6.57% vs 1.81% multiparous ones) The first 4 weeks of postnatal period Higher levels of anxiety Obsessive-compulsive personality disorder Avoidant personality disorder Personal history of major depression The existence of OCD related dysfunctional belief
Clinical manifestations
The obsessional thinking and compulsive behaviors of perinatal OCD often focus on the pregnancy or baby
During pregnancy, obsessions are often about fears of fetal death or contamination.
Clinical manifestations
Examples of obsessions during pregnancy:Fear of fetal deathMother's belief that she is infected and if she holds her
baby the infection will spread to the baby as well (eg. herpes or AIDS).
Intrusive thoughts of accidentally harming the foetus by exposure to medications, chemicals, vaccinations, or certain foods.
Aggressive obsessions towards fetus.
Clinical manifestations
Examples of compulsions during pregnancy:
Excessive checking for fetal movements.
The mother's repeated requests for ultrasounds to check fetal wellbeing prior to birth.
Avoidance of certain foods or medications for fear of harming the foetus.
Clinical manifestations
Examples of obsessions during postpartum:Excessive fears of contamination of the babyExcessive fear of accidentally harming a child through
carelessnessIntrusive thoughts of dropping the baby onto the floorIntrusive thoughts of throwing the baby out the windowIntrusive thoughts of stabbing the newborn babyIntrusive thoughts of suffocating or drowning the newborn babyThe idea that the baby could die while sleepingAn image of the baby choking and not being able to save himAn image of the baby dead
Clinical manifestations
Examples of compulsions during postpartum:Avoidance of feeding the baby for fear of accidental poisoningAvoidance of bathing the infantStaying physically isolated from the babyIsolating the baby from other people out of fear they might
contaminate the babyHiding or throwing out knives, scissors, and other sharp objectsCompulsive checking of the infant (eg, at night)Excessive washing of baby clothing or bottlesExcessive washing of other family members clothing
Clinical manifestations
Patients with OCD often have insight into their obsessions, recognizing them as intrusive and inappropriate, though their degree of insight can vary.
When severe obsessive thoughts persist over a long period of time, they can resemble fixed delusional thinking.
On very rare occasions, these thoughts can progress to psychosis, where the patient believes the ideas/thoughts are real.
Course
Women who have new onset of OCD in the perinatal period tend to have a milder course than preexisting disorder, with more favourable prognosis for pregnancy-onset OCD than postpartum-onset OCD.
women with preexisting OCD, earlier onset and greater severity tends to be associated with a more severe course during pregnancy or postpartum. These patients typically experience their usual obsessions and compulsions with the addition of those that are baby-centered.
Screening
It is suggest that obstetricians or primary care clinicians administer a one-question screening in the course of prenatal and postpartum care. Two illustrative screening questions include:
●"It's not uncommon for new mothers to experience intrusive, unwanted thoughts that they might harm their baby. Have any such thoughts occurred to you?".
●"Have you had any scary thoughts, for example, that you might accidentally harm the baby? Many women experience such thoughts, but are afraid to mention them."
Assessment
Patients who screen positive should receive a thorough psychiatric assessment that includes a diagnostic evaluation for OCD and considers possible alternative diagnoses.
Assessment
In evaluating the patients’ mental status, it is important to distinguish the obsessional thoughts of OCD from psychotic thoughts or ideas.
The interviewer should explore whether the patient has insight into the false ideas and related behaviors (obsessions and compulsions) or if she believes they are real (psychosis). Particularly when the patient lacks insight into her illness, assessment should rule out the presence of accompanying psychotic symptoms (eg, hallucinations) that are characteristic of a psychotic disorder rather than OCD.
Patients should be asked if they have intent or desire to harm the baby, others, or themselves. Patients should be evaluated for comorbid disorders, including depression and generalized anxiety disorder.
Assessment
Whenever possible, assessment for OCD should include secondary sources of information, such as the patient's partner or a close family member.
Women with OCD are often secretive about their symptoms and may be reluctant to disclose them to a clinician due to stigma, shame, or fear that disclosure would lead to the baby being taken away.
Sometimes the symptoms may come to clinical attention only when the partner or other family caregiver has to return to work and is concerned about the mother's ability to care for the child on her own.
Risk of harm
Risk factors for harm include: the stated intent to cause harm psychotic thoughts poor insight poor impulse control Accompanying severe depression low levels of family support Baby with more than usual needs
o Avoidance of the baby carries a risk for neglect, with the potential for severe harm or even death.
Management
OCD is a challenging disorder to treat; only 30% of patients show significant improvement.
Treatment of the illness in pregnant and postpartum women can be more complex, with additional risk factors to consider and little data available to inform treatment.
Management
When the patient's illness is accompanied by factors suggesting a risk of harm to mother or baby, safety should be the foremost consideration. Interventions should be based on the likelihood of harm.
In lower-risk situations, outpatient interventions may be sufficient, such as a partner or family members who will provide support, child care, and ensure the patient is not alone with the baby.
In higher-risk circumstances, the mother may require hospitalization.
Management
PsychotherapyCognitive-Behavioural therapy( CBT ) has been suggested as a first-line treatment of OCD in pregnant and breastfeeding women.
Other techniques that can be used: Filial therapy Psychoeducation exposure and response prevention
Management
Symptoms suggesting the possible utility of this approach include the mother avoiding the infant, being intrusive, or being excessively clingy.Although evaluated for numerous populations, filial therapy has not been studied specifically for OCD.
filial therapyFilial therapy trains the mother through instruction, demonstration play, and supervision to create positive interactions with the baby, recognizing and responding to his or her emotions in an accepting environment.
Management
Medication
Medications shown to be effective for treatment of OCD in the general population include the serotonergic antidepressants and, for refractory cases, augmentation with atypical antipsychotic medication.
Management
Deciding whether or not to prescribe one of these medications for a pregnant or nursing woman should be based, as it is for all patients, on a careful weighing of the benefits and risks of treatment, including:
The severity and chronicity of the obsessions and compulsions, and the degree to which they impair patient and family functioning.
The risks that untreated illness present to the mother and baby (eg, avoidance, neglect, suicidality, or homicidality).
The risks the medications present to the baby through exposure either in utero or during breast feeding.
Management
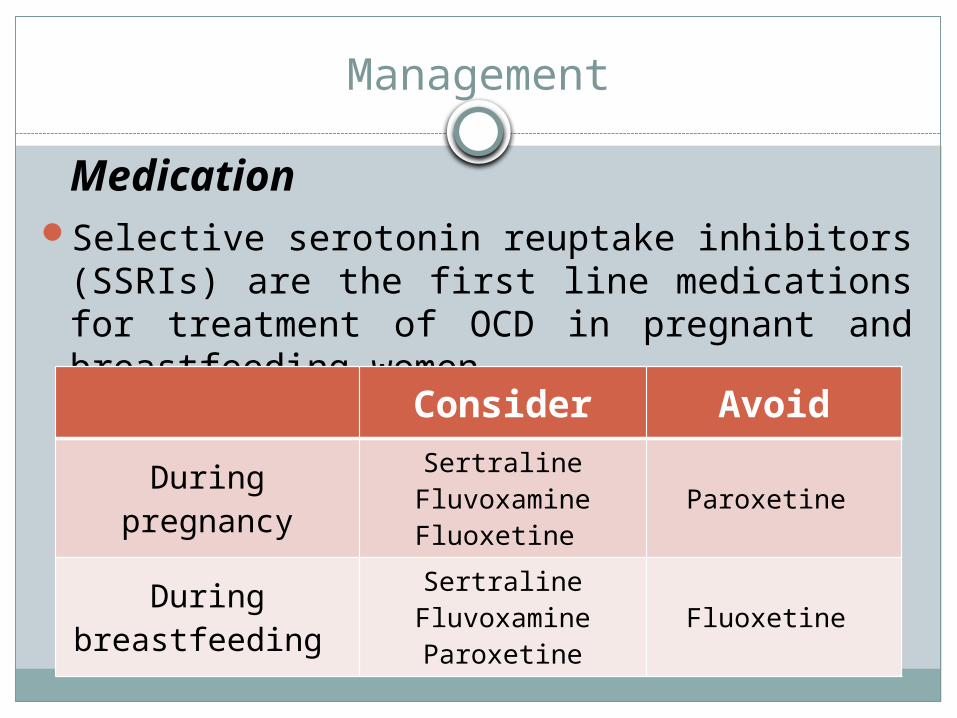
MedicationSelective serotonin reuptake inhibitors (SSRIs) are the
first line medications for treatment of OCD in pregnant and breastfeeding women.
Consider Avoid
During pregnancySertraline
FluvoxamineFluoxetine
Paroxetine
During breastfeeding Sertraline
FluvoxamineParoxetine
Fluoxetine
Management
Augmentation with atypical antipsychoticsReserved for refractory casesA single uncontrolled study examined Quetiapine
augmentation following an inadequate response to an SSRI in 17 postpartum women with OCD. After 12 weeks of treatment, 11 of the 17 women experienced a 50% or greater reduction in symptoms.
Summary And Recommendations
Estimates of the prevalence of (OCD) in pregnant and postpartum women appears to be approximately two times estimates of OCD prevalence in women in the general population.
Obsessional thoughts and compulsive behaviors in OCD during pregnancy or postpartum often concern the baby. Thoughts about contaminating or harming the baby are a common theme. Harmful behaviors are relatively rare but warrant careful assessment and intervention as needed to ensure safety.
OCD may go undetected during prenatal or postpartum care. Obstetricians and primary care clinicians should consider routine screening during pregnancy and for several months post-delivery.
For mild OCD without immediate risks to the mother or child, treatment with cognitive-behavioral therapy (CBT) is recommended. Adjunctive attachment therapy may be useful if an attachment or bonding issue is present.
Summary And Recommendations
Treatment with a serotonergic antidepressant is usually necessary for women with moderate to severe OCD. The decision to use psychotropic medication while pregnant or nursing requires informed consent via a careful discussion among the physician, the patient, and her partner of the potential risks of the medication versus the potential risks of the untreated illness.
When moderate-to-severe OCD is refractory to first-line treatment (serotonergic antidepressant), weigh the benefits and risks of the following options: augmentation with CBT, switching to a different class of serotonergic antidepressant, or augmentation with an atypical antipsychotic.
Attachment therapies may be useful in treating problems with attachment or bonding between mother and baby, although their use has not been studied for OCD.
Thank You







![The Incidence of Postpartum Hemorrhage in Pregnant … · between endometrial damage and uterine scarring and subsequent placenta previa [4]. Mean-while, the condition is frequently](https://img.pdfslide.net/doc/110x75/5ba8e78509d3f2f51d8b4ab9/the-incidence-of-postpartum-hemorrhage-in-pregnant-between-endometrial-damage.jpg)